
Abstract
Benign cystic mesothelioma of the peritoneum (BCM) is an uncommon lesion with some 130 cases reported since the first case described by Smith and Mennenmeyer in 1979. It is a rare intra abdominal tumor occurring predominantly in women of reproductive age. Due to the rarity of this tumor, similarity of patient presentation, and comparable features on imaging, the diagnosis of this pathology is difficult, and is based on histological findings. This tumor is known for local recurrence. It's agreed that surgery is the only effective treatment, but there are no evidence-based treatment strategies for BCM.
Similar content being viewed by others

Introduction
Benign cystic mesothelioma of the peritoneum (BCM) is a rare intra abdominal tumor with a strong predilection for the peritoneum of pelvic organs. Symptoms are not specific, and the differential diagnosis is vast, including cystic lymphangioma, mucinous cystadenoma, cystic teratoma and pseudomyxoma retroperitonei. There are no evidence-based treatment strategies for BCM, and even if it is considered as a benign tumor, this tumor has a high local recurrence rate.
We report a new case of BCM, which appeared as a surgical emergency.
Case report
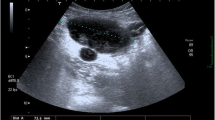
A 71 year-old woman presented to the emergency department complaining of history of abdominal pain since 2 days accompanied by diarrhea. Four months prior to presentation, she noticed an increase in abdominal girth. Moreover, she developed occasional abdominal discomfort, which slowly increased frequency. The patient also developed symptoms of constipation and severe reflux which were not improved by taking laxatives and a proton pump inhibitor. Our patient was hemodynamically stable with temperature at 37.9°C, and blood pressure was 130/80 mmHg. Abdominal examination was marked by diffuse abdominal distension, and tenderness. Computed tomography (CT) scanning showed a large spherical multi-loculated cystic mass in the abdomen which was not-communicating to any abdomen viscera, occupying nearly the entire abdominal cavity, displacing the hole bowel (Figure 1). Furthermore, on CT scan, there was a strong suspicion of central tumor necrosis (Figure 2). Therefore, our patient was taken to operating theatre. Laparotomy was done. Intraoperative examination showed a cystic mass extending from the pelvis inferiorly to the liver. There was a significant peritoneal thickening, and a peritoneal effusion, with many cystic lesions that makes dissection and resection very difficult. The mass and some of the free-floating cysts were carefully harvested and removed for histological examination. Benign cystic mesothelioma was revealed in the pathology report.

Large spherical multi-loculated cystic mass.

Suspicion of centro tumoral necrosis on CT scan.
Our patient made an excellent recovery, and she was discharged home after 6 days. Our patient was seen in out patient clinic at 1 month and 3 months. She had no functional complaints and kept a slight abdominal distension.
This study was performed according to the declaration of Helsinki and approved by the Local Ethical Committee.
Discussion
Benign cystic mesothelioma of the peritoneum (BCM) was described first by Mennenmeyer and Smith [1]. It’s a rare pathological entity with about 130 cases reported in the literature [2, 3] (Table 1). Several authors consider this tumor as benign [1, 4], and it’s prognosis is excellent [5]. There is only one reported death from BCM on the literature: Raafat and al. reported a case of a 14 years-old patient who had a subtotal resection of the abdominal mass, and died 12 years after refusing surgery for recurrence [6]. Indeed, BCM has a high local recurrence rate [7], and this recurrence rate is higher in women (40 – 50%) than in men (33%) [8]. The etiology remains unclear, but it is well known that many inciting factors may promote hyperplastic and neoplastic changes in mesothelial cells. The suggested provoking factors are foreign fibres and dusts, inflammatory mediators, and mechanical injuries [9]. Proliferation and inward migration of peripheral mesothelial cells, proliferation and metaplasia of underlying connective tissue cells, and surface attachment and differentiation of free-floating mononuclear cells all have been postulated as the mechanism of mesothelial cell proliferation in pathological conditions [9]. This peritoneal lesion is characterized by the formation of multiple multilocular thin-walled cysts, which may form large intraabdominal masses [1]. The BCM affects women in 80% of cases, with an average age of 34 years [3]. The clinical presentation is unspecific: it is usually abdominal pain, increased abdominal girth and constipation. Physical examination revealed abdominal distension, abdominal tenderness or a palpable mass [10]. Imaging modalities that can be used include abdominal ultrasound (US), CT scan, or magnetic resonance imaging (MRI). They allow to visualize the lesion, but not to differentiate it from other cystic lesions of the peritoneum [11], especially lymphangiomas [9]. Laparoscopy remains the best diagnostic tool because it enables to perform biopsies and to establish the definitive diagnosis [12]. There are no evidence-based treatment strategies for BCM, but surgery, with complete enucleation of the cyst to prevent recurrence and possible malignant transformation remains the mainstay of treatment. However, some researchers advocate aggressive surgery followed by heated intraperitoneal chemotherapy (HIPEC) [12]. Indeed, for a long time, the treatment consist of full excision of the lesions (debulking surgery) [7]. Currently, some teams recommend aggressive surgery (extended peritonectomy) followed by HIPEC [3, 13]. Two series are available on the results of extended peritonectomy followed by HIPEC. In the first one [13], 5 patients were asymptomatic, and 4 showed no recurrence with a follow up between 6 and 69 months. In the second series [14], 5 patients were asymptomatic, and 2 had got recurrence, with a follow up between 3 and 102 months.
Conclusion
Benign cystic mesothelioma of the peritoneum (BCM) is a rare tumor with a high local recurrence rate. It requires optimal care in a specialized center especially as there is no evidence-based treatment strategies.
Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images.
References
Mennemeyer R, Smith M: Multicystic, peritoneal mesothelioma: a report with electron microscopy of a case mimicking intra-abdominal cystic hygroma (lymphangioma). Cancer. 1979, 44: 692-698. 10.1002/1097-0142(197908)44:2<692::AID-CNCR2820440242>3.0.CO;2-6.
Safioleas MC, Constantinos K, Michael S, Konstantinos G, Constantinos S, Alkiviadis K: Benign multicystic peritoneal mesothelioma: a case report and review of the literature. World J Gastroenterol. 2006, 12 (35): 5739-5742.
González-Moreno S, Yan H, Alcorn KW, Sugarbaker PH: Malignant transformation of "benign" cystic mesothelioma of the peritoneum. J Surg Oncol. 2002, 79: 243-251. 10.1002/jso.10081.
Van Ruth S, Bronkhorst MWGA, Van Coeverden F, et al: Peritoneal benign cystic mesothelioma: a case report and review of literature. Eur J Surg Oncol. 2002, 28: 192-195. 10.1053/ejso.2000.1215.
Bhandarkar DS, Smith VJ, Evans DA, Taylor TV: Benign cystic peritoneal mesothelioma. J Clin Pathol. 1993, 46: 867-868. 10.1136/jcp.46.9.867.
Raafat F, Egan M: Benign cystic mesothelioma of peritoneum. Immunohistochemical and Ultrastructural features in a child. Paediatr Pathol. 1988, 8: 321-9. 10.3109/15513818809042975.
Schwartz AT, Peycru E, Tardat JP, Dufau J, Jarry F, Durand-Dastes : Le mésothéliome kystique péritonéal: bénin ou malin ?. J Chir. 2008, 145: 8-10.1016/S0021-7697(08)70550-7.
Canty MD, Williams J, Volpe RJ, et al: Benign cystic mesothelioma in a male. Am J Gastroenterol. 1990, 85: 311-15.
Pelosil G, Zannonil M, Caprioli F, Faccincani L, Battistoni MG, Balercia G, Bontempinil L: Benign multicystic mesothelial proliferation of the peritoneum: lmmunohistochemical and electron microscopical study of a case and review of the literature. Histol Histopath. 1991, 6: 575-583.
Vyas: Mesothelioma as a rapidly developing giant abdominal cyst. World J Surg Oncol. 2012, 10: 277-10.1186/1477-7819-10-277.
Yang DM, Jung DH, Kim H, Kim JH, Hwang HY, et al: Retroperitoneal cystic masses: CT, clinical, and pathologic findings and literature review. Radio Graphics. 2004, 24: 1353-1365.
Khuri SH, Assalia Y, Abboud A, Gilshtein W: Kluger benign cystic mesothelioma of the peritoneum: a rare case and review of the literature. Case Rep Oncol. 2012, 5: 667-670. 10.1159/000346187.
Sethna K: Peritoneal cystic mesothelioma: a case series. Tumori. 2003, 89: 31-35.
Baratti D, et al: Multicystic peritoneal mesothelioma treated by surgical cytoreduction and hyprerthermic intra peritoneal chemotherapy (HIPEC). vivo. 2008, 22: 137-157.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors declare that they have no competing interests.
Authors’ contributions
EBH and AB participated in writing the case report and revising the draft, OM, EB, AO, KM and KAT participated in the follow up. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Elbouhaddouti, H., Bouassria, A., Mouaqit, O. et al. Benign cystic mesothelioma of the peritoneum: a case report and literature review. World J Emerg Surg 8, 43 (2013). https://doi.org/10.1186/1749-7922-8-43
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1749-7922-8-43