
Abstract
Background
Effective implementation strategies are needed to optimize advancements in the fields of cancer diagnosis, treatment, survivorship, and end-of-life care. We conducted a review of systematic reviews to better understand the evidentiary base of implementation strategies in cancer control.
Methods
Using three databases, we conducted a search and identified English-language systematic reviews published between 2005 and 2010 that targeted consumer, professional, organizational, regulatory, or financial interventions, tested exclusively or partially in a cancer context (primary focus); generic or non-cancer-specific reviews were also considered. Data were extracted, appraised, and analyzed by members of the research team, and research ideas to advance the field were proposed.
Results
Thirty-four systematic reviews providing 41 summaries of evidence on 19 unique interventions comprised the evidence base. AMSTAR quality ratings ranged between 2 and 10. Team members rated most of the interventions as promising and in need of further research, and 64 research ideas were identified.
Conclusions
While many interventions show promise of effectiveness in the cancer-control context, few reviews were able to conclude definitively in favor of or against a specific intervention. We discuss the complexity of implementation research and offer suggestions to advance the science in this area.
Similar content being viewed by others


Background
Innovations in screening and early detection, development of effective treatment interventions, and strategies to improve quality of life have emerged from primary studies, and systematic reviews of these studies, in cancer control [1–9]. These advancements have the capacity to reduce mortality and morbidity from disease. However, optimizing these advancements requires their appropriate application, a goal that is often difficult to achieve [10, 11]. Understanding what are the most effective and promising interventions is warranted to ensure that the appropriate options are chosen and incorporated into implementation plans and prioritized for future research studies. The analysis of studies examining the effectiveness of implementation interventions is a key component to an overall knowledge translation (KT) research agenda [12].
The purpose of our study was to conduct a review of systematic reviews to better understand the evidentiary foundation regarding what is known about KT interventions. Specifically, we wanted to better understand the strengths and limitations of the field, to identify what interventions are ready for use now, and to identify research priorities and directions for the future. We were interested in studies conducted in the context of cancer control across the care continuum, from diagnoses to survivorship and end-of-life care, and across cancer diagnoses. We chose this scope given that "context" has been identified as an important consideration in the design and execution of implementation strategies and is a concept central to several KT models and research paradigms [12–15].
Methods
Overview
This project, Knowledge Translation to Improve Cancer Control in Canada, was funded by the Ontario Institute for Cancer Research and the Canadian Partnership Against Cancer. It received ethics approval from the Hamilton Health Sciences/Faculty of Health Sciences Research Ethics Board, McMaster University, Hamilton, Ontario, Canada. The design, execution, analysis, and reporting of the project was editorially independent from the funders.
To avoid duplication of effort, and to complete the study in the required time, we capitalized on available high-quality databases profiling systematic reviews of interventions to systematically search for, appraise, and evaluate the effectiveness of KT interventions that met our inclusion criteria. Aligning with existing categorical schemes (Canadian Agency for Drugs and Technologies in Health [CADTH] and Cochrane Collaboration's Effective Practice and Organisation of Care [EPOC] group), we sought interventions that targeted the groupings of consumers/patients/public (i.e., consumer interventions), clinicians and healthcare providers (i.e., professional interventions), organizational/managers/system leaders (i.e., organizational interventions), regulatory (i.e., new health service delivery regulation), and financial (i.e., incentives).
Search
To identify existing systematic reviews that met our inclusion criteria, we used three databases as our sources:
-
1.
Rx for Change (CADTH-EPOC Group Collaborative Initiative): http://www.cadth.ca/en/resources/rx-for-change/database
-
2.
Health Systems Evidence (formerly, Program in Policy Decision-Making), McMaster University: http://www.healthsystemsevidence.org/
-
3.
McMaster KT+, McMaster University: http://plus.mcmaster.ca/kt/Default.aspx
Eligibility criteria
Inclusion criteria
-
Study designs: Systematic reviews published between 2005 and 2010. While the methodology is still evolving, this interval was chosen to align with best evidence suggesting median survival time of a systematic review is approximately five years [16].
-
Outcomes: Systematic reviews that included at least one of the following outcomes: measurable clinical outcomes, observable behavior change, documented intention to behave, documented attitudes, documented knowledge uptake, or reported stakeholder satisfaction.
-
KT interventions: Interventions that focused on at least one of the following target groupings: consumer, professional, organization, regulatory, and financial, as outlined in the CADTH-EPOC framework.
-
Clinical scenarios:
-
○ Diagnosis: Interventions that were tested in cancer-specific environments (any cancer diagnosis). Reviews that included cancer as part of the clinical context or that were generic/nonspecific to clinical condition were also considered.
-
○ Stage of continuum of care: Diagnosis, treatment, follow-up, survivorship, end-of-life [17]a.
-
Exclusion criteria
-
Study designs: Any design other than systematic reviews.
-
Language: Non-English language due to cost and availability of translations.
Data extraction
Data were extracted from the systematic reviews meeting our eligibility criteria. For all reviews, data extracted included (i) intervention name/label; (ii) intervention definition and purpose; (iii) theories, frameworks, or models used to inform the design or execution of the intervention; (iv) key operational elements underpinning the execution of the intervention; (v) setting; (vi) geography (where the intervention was tested); (vii) stakeholder involvement (who and type of involvement); (viii) evaluation strategy; (ix) measurement instrument(s); (x) quality indicators and outcomes; (xi) recommendations and conclusions; (xii) cost information and/or information regarding sustainability of the intervention; and (xiii) AMSTAR quality appraisal (if available).
Quality control and critical appraisal
Title, abstract, and full-text screenings were done in duplicate (KG and LD). Disagreements were resolved by consensus or by a third party (JM). Data extraction and critical appraisal (if required) were conducted by one researcher and audited by a second. In circumstances where appraisal was not completed by the original source, the systematic reviews were appraised using AMSTAR [18], an 11-item evaluation tool assessing methodological standards, presentation, and critical appraisal in systematic reviews. AMSTAR ratings can range between 1 and 11, with 11 denoting highest quality.
Interpretation of systematic reviews' results and research priorities/direction
Data tables describing the systematic review study characteristics and results were circulated to subgroups of the research team (see Additional File 1). For each assigned systematic review and using a 7-point scale, members of the subgroups were asked to indicate their "assessment of effectiveness" for each intervention reviewed based on their interpretation of the data. A rubric was designed to guide these assessments and the interpretation of the rating scale. Interventions rated between 1 and 3 were considered ineffective, interventions rated 4 and 5 were considered promising and worth additional investigation, and interventions rated 6 or 7 were considered effective. Average scores of ratings were calculated for each systematic review. Investigators were then asked to identify any specific research priorities or research questions they thought relevant.
Results
Overall
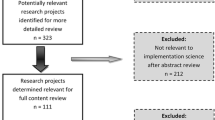
The initial search for systematic reviews yielded 591 reviews for consideration from the three source databases. Of these, a total of 38 reviews were originally considered and 31 retained [19]b. An additional three reviews were included post hoc, identified by members of the research team (see Additional File 2).
In total, 34 unique systematic review publications providing 41 evidence summaries on 19 unique interventions comprised the evidence base. Table 1 provides the definitions of the interventions considered. Some systematic reviews addressed more than one intervention or provided more than one evidence summary; in addition, more than one systematic review was available for some of the interventions. Additional File 2 provides the references for the included systematic reviews.
The overall quality of the systematic reviews, as measured by the AMSTAR tool [18], was moderate. The systematic reviews were most apt to target the treatment stage of the continuum and least likely to target survivorship (Table 2). Further, despite being a highly prevalent disease site, few systematic reviews targeted patients with lung cancer (Table 3). Some less prevalent diagnoses (head and neck, sarcoma, and melanoma) were rarely or never targeted. A significant number of reviews did not specify cancer diagnosis.
With respect to characteristics of the systematic reviews (Table 4), most did not specify whether a KT theory, model or framework was used to inform the design of the project or the intervention itself. Most of the reviews used a mixture of study designs as their primary evidentiary source, and only four reviews used non-randomized controlled trial (RCT) data exclusively as their primary evidence. Most systematic review authors reported poorly executed and poorly reported primary studies.
Common outcomes reported in the literature were measures of knowledge, satisfaction, and observed behavior and, to a lesser extent, clinical outcomes. Indeed, 7 of 17 consumer evidence summaries reported clinical outcomes, while 12 reported on knowledge, 10 reported on behavior observed, 9 reported on satisfaction, 8 reported on behavior intention, and 6 reported on attitude. For professional evidence summaries, 11 of 14 reported clinical outcomes, compared to knowledge (2), satisfaction (2), and behavior observed (10). Similarly, the most reported outcome for organizational evidence summaries were clinical outcomes (8), compared to behavior observed (7), satisfaction (7), knowledge (4), attitude (2), and behavior intention (1). However, when considering across the 41 evidence summaries in our sample, only 15 of 41 reported clinical outcomes.
With respect to intervention context (Table 5), clinicians were most often delivering the intervention, and a clinical environment (e.g., clinics, hospitals) was the most common setting for the intervention to take place. Interventions were most often delivered in person, by paper, or by phone. Technology-based modalities were used less often unless they defined the intervention itself (e.g., electronic medical record, clinical decision support systems).
The following sections, including the tables and additional files, provide an overview of the results by cluster of main intervention groupings. For more information on the complete raw data set, readers are asked to contact the corresponding author.
Interventions aimed at consumers (Additional File 3)
Sixteen publications addressing six unique consumer interventions provided 17 evidence summaries. Consumer interventions included education/information provision, decision-making aids, and interventions to support behavior change. Tables 4, 5, and 6 summarize characteristics of the systematic reviews; Table 7 summarizes the quality and efficacy appraisals of the interventions; and Table 8 summarizes the research suggestions made by members of the team.
The overall quality of the systematic reviews targeting consumer interventions was variable, ranging from poor to high. The average AMSTAR score was 7, with scores ranging from 3 to 10. Most of the systematic reviews did not include a meta-analysis or an empirical synthesis of findings. Evidence of effectiveness was most promising for patient education (e.g., improvements in patient knowledge and clinical outcomes); decision aids (e.g., improvements in patient knowledge and satisfaction, reduction in patient decisional conflict, and impact on decisions); and interactive health communication applications (e.g., improvements in knowledge, social support, behavior, and clinical outcomes). Most reviews within a given intervention type yielded significant variability with respect to effectiveness, and most authors were unable to provide definitive conclusions to their use.
Assessments by research team members on effectiveness yielded overall mean scores (across evidence summaries of similar interventions) ranging between 3.8 and 6.0 (see "Team Ratings" column of Table 7). Only one, interactive health communication applications, was rated as being effective. The remaining interventions were rated as promising and candidates for more study. Eight research ideas and three systematic review topics were identified by members of the research team (Table 8).
Interventions aimed at professionals (Additional File 4)
Twelve publications addressing seven unique professional interventions provided 14 evidence summaries. Professional interventions included education, audit and feedback, information technology (IT)/information management (IM)/informatics, clinical decision support systems, computerized physician order entry, reminders, local opinion leaders, tailored interventions, clinical pathways, guidelines, and discharge planning. Tables 4, 5, and 9 summarize characteristics of the systematic reviews; Table 10 summarizes the quality and efficacy appraisals for the interventions; and Table 11 summarizes the research suggestions made by members of the research team.
For these systematic reviews, the average AMSTAR score was 6, with scores ranging from 3 to 8. Trials that comprised the reviews included RCTs, clinical controlled trials, pre-/post studies, cluster RCTs, time series, observational, and trials labeled as "other." Of the 14 evidence summaries, 4 undertook quantitative pooling (i.e., meta-analysis).
Evidence of effectiveness was most promising for educational outreach and audit and feedback interventions (median improvement in clinical outcomes 5%); clinical decision support (improved clinical performance); computer order entry (reduction in medical errors); clinical pathways (reduction in complication rates); local opinion leaders (reduction in clinician noncompliance); and tailored interventions (improvement in some clinical outcomes). However, these benefits are contrasted against the concerns with the overall quality and lack of consistency across the systematic reviews. Moreover, the primary studies included in the systematic reviews are reported to be of poor quality, heterogeneous, and poorly reported with respect to the interventions, contexts, and measurements of outcomes. Together, this makes definitive conclusions about professional interventions very challenging.
Research team ratings of the interventions were assessed, and the overall mean scores (across evidence summaries of the same intervention) ranged between 4.3 and 5.0 all were within the "promising" category (see "Team Ratings" column in Table 10). Twenty-eight research ideas were recommended by members of the research team (see Table 11).
Interventions aimed at organizations (Additional File 5)
Nine reports addressing six unique organizational interventions provided 10 evidence summaries. The interventions included organizational/structural specific, continuity-of-care related, shared-care tactics, revisions of professional roles, and health information technology. Tables 4, 5, and 12 summarize characteristics of the systematic reviews; Table 13 summarizes the quality and efficacy appraisals of the interventions; and Table 14 summarizes the research suggestions made by members of the team.
Organizational interventions are those aimed at encouraging use and uptake of knowledge at the organizational level. The average AMSTAR score was 5, with scores ranging from 2 to 8, which indicates the range of very poor methodological quality to moderately high methodological quality. Overall, the reviews were not able to provide definite conclusions (e.g., statistically significant findings) to support the use of any of the specific interventions reviewed.
Two of the interventions, changing length of consultation time and shared-care tactic interventions, were rated by members of the research team as not effective (ratings of 3 and under). The remaining interventions fell between 4 and 5 on the scale, indicating promise and are candidates for further study (see Table 13). Twenty-eight research ideas were recommended by members of the research team (see Table 14).
Conclusion
We considered 34 unique systematic reviews providing 41 evidence summaries for 19 KT interventions. The quality of the execution of the systematic reviews varied significantly, with AMSTAR ratings ranging between 2 and 10. Primary evidence serving as the foundation for the systematic reviews included RCTs and nonrandomized trials. Systematic review authors describe the primary evidence as uneven with respect to quality, reporting, and outcomes.
While many interventions suggested promise of effectiveness, few reviews were able to conclude definitively in favor of or against a specific intervention. The interpretation of the evidence by members of the research team aligned with this analysis. The majority of the interventions were rated by the research team members as promising, but in need of additional study.
In considering KT in cancer control, one is struck by the complexity of the enterprise. While there are many studies being conducted, the quality is decidedly uneven and the impact on patient care or system performance is questionable. To that end, some key observations are noted and conclusions for the research enterprise can be drawn.
Overall, the approach to KT in cancer control appears patchy and unsystematic. While this may be due, in part, to the breadth, size, and scope of the research area, it is likely to be a major contributor to the hodgepodge of studies being conducted, the failure of the research community to consistently embrace high-quality research paradigms and standards, and the inability to create a common language and taxonomy in the field. Indeed, common across the systematic reviews considered here is that the studies that underpin them often fail to adequately describe all aspects of the KT intervention under investigation and (where relevant) the control group. This makes it very difficult to synthesize data, to improve the overall research enterprise, and to build from one study to another. Here, work by Cochrane's EPOC group and researchers such as Michie and others may assist in designing a common language, a common set of operational definitions, and common labels to facilitate the advancement of the KT field [20–22].
The complexity of the cancer field and the impact of that complexity to the KT research agenda cannot be underestimated. The numerous but unique diagnoses, the variety of providers involved in cancer care and control (i.e., public health, primary care, medical specialists, allied health providers, lay and peer providers), the various organizational settings in which care is offered, the risks associated with some care options, and the variability in decision-making styles by individuals affected by cancer are examples of this complexity. As it relates to the KT research enterprise, the role of context and individual differences must be stressed.
The design and execution of the primary studies fall below acceptable levels of quality. For example, we found that the systematic reviews often fail to measure meaningful end points because these data are not available in the primary literature that comprise the evidentiary base for synthesis. While measures of knowledge, satisfaction, and intention are important--and in fact, better studied--measures of intervention fidelity (or adherence to intervention), relevant clinical end points, and valid patient-centered outcomes are often lacking.
In addition, the design and execution of the systematic reviews in the KT field are uneven. For example, use of factorial designs, multilevel modeling techniques, and regression strategies could improve the precision by which we understand KT interventions. The application of these techniques is warranted. While this has been undertaken in some of the systematic reviews, it is not consistent, nor is it being done in the primary studies underpinning the existing reviews.
Thus, common principles of good scholarship and methodological rigor are required in systematic reviews of KT research and in the primary studies that underpin them. Namely, well-defined research questions, appropriate research design, patient-centered outcomes, analytic strategies to better understand the mechanisms associated with change, and completeness of reporting are necessary.
There are, however, limitations to our study. First, to manage scope and resource constraints of the project, we considered only systematic reviews available in databases of systematic reviews. While trying to avoid duplication, we acknowledge there may be other reviews that would have met our inclusion criteria that were not included in any of the three databases. Further, one review by Grimshaw (2006) [19] was found to be eligible during our search but was erroneously deleted and not included in our review. In addition, we acknowledge that there are likely primary studies not yet included in any of the systematic reviews we considered that would have been relevant to our question.
Second, this study was Canadian in focus with respect to members of the research team. While this conformed to the request for proposals criteria of the project's funders, it may be that a different composition of individuals would have yielded different conclusions. To advance the field, gathering a more international perspective may be warranted.
In summary, this project provides an overview of the evidence related to KT in cancer control. Given the current state of the evidence and the need for additional research in so many areas, we were not able to offer a definitive blueprint outlining a small manageable set of research priorities in this context. The field is open and considerable work is required. To ensure world-class research and research that will have a positive impact on people with cancer and on cancer system performance requires clarity and transparency of research scope and goals coupled with high expectations for the research community to achieve excellence in study design, execution, and reporting.
Endnotes
aInterventions to influence uptake of cancer screening were explored in a separate project and were not considered here [17]. Cancer prevention was out of scope for this project and the aforementioned project.
bOne eligible systematic review by Grimshaw et al. (2006) was inadvertently deleted from the systematic review sample [19]. It focused on guidance dissemination and implementation strategies. They found absolute improvement in performance of 14.1% for reminders, 8.1% for dissemination, 7.0% for audit and feedback, and 6% for multifaceted interventions. This review is not included in the summary statistics presented.
References
Mandel JS, Bond JH, Church TR, Snover DC, Bradley GM, Schuman LM, Ederer F: Reducing mortality from colorectal cancer by screening for fecal occult blood. N Engl J Med. 1993, 328: 1365-1371. 10.1056/NEJM199305133281901.
Hardcastle JD, Chamberlain JO, Robinson MH, Moss SM, Amar SS, Balfour TW, James PD, Mangham CM: Randomised controlled trial of faecal-occult-blood screening for colorectal cancer. Lancet. 1996, 348: 1472-1477. 10.1016/S0140-6736(96)03386-7.
Kronborg O, Fenger C, Olsen J, Jørgensen OD, Søndergaard O: Randomised study of screening for colorectal cancer with faecal-occult-blood test. Lancet. 1996, 348: 1467-1471. 10.1016/S0140-6736(96)03430-7.
Mandel JS, Church TR, Bond JH, Ederer F, Geisser MS, Mongin SJ, Snover DC, Schuman LM: The effect of fecal occult-blood screening on the incidence of colorectal cancer. N Engl J Med. 2000, 343: 1603-1607. 10.1056/NEJM200011303432203.
Verma S, Trudeau M, Pritchard K, Oliver T, members of the Breast Cancer Disease Site Group: The role of the taxanes in the management of metastatic breast cancer. Practice Guideline Report # 1-3 Version 2.2003., [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=34140]
Trudeau M, Eisen A, Messersmith H, Pritchard KI, and the Breast Cancer Disease Site Group: Adjuvant taxane therapy for women with early-stage, invasive breast cancer: A Clinical Practice Guideline. 2006, Evidence-based Series #1-7., [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=34128]
Trudeau M, Sinclair S, Clemons M, Shelley W, members of the Breast Cancer Disease Site Group: The role of taxanes in neoadjuvant chemotherapy for women with non-metastatic breast cancer. 2004, Practice Guideline Report #1-20,, [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13886]
Crump M, Trudeau M, Sinclair S, O'Malley F, members of the Breast Cancer Disease Site Group: The role of trastuzumab (Herceptin®) in the treatment of women with HER2/neu-overexpressing metastatic breast cancer. Practice Guideline Report #1-15 (Version 2.2004), [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13870]
Hanks G, Cherny N, Fallon M: Opioid analgesic therapy. Oxford Textbook of Palliative Medicine. Edited by: Doyle D, Hanks G, Cherny N and Calman K. 2005, New York: Oxford University Press, 318-3
Francke AL, Smit MC, de Veer AJE, Mistiaen P: Factors influencing the implementation of clinical guidelines for health care professionals: a systematic meta-review. BMC Med Inform Decis Mak. 2008, 8: 38-10.1186/1472-6947-8-38.
Cancer Quality Council of Ontario: Cancer Quality Index of Ontario 2009. 2010, [http://csqi.cancercare.on.ca/cms/One.aspx?portalId=40955&pageId=41027]
Graham ID, Logan J, Harrison MB, Straus SE, Tetroe J, Caswell W, Robinson N: Lost in knowledge translation: Time for a map?. J Contin Educ Health Prof. 2006, 26: 13-24. 10.1002/chp.47.
Dobrow MJ, Goel V, Lemieux-Charles L, Black NA: The impact of context on evidence utilization: a framework for expert groups developing health policy recommendations. Soc Sci Med. 2006, 63: 1811-1824. 10.1016/j.socscimed.2006.04.020.
Kitson A, Rycroft-Malone J, Harvey G, McCormack B, Seers K, Titchen A: Evaluating the successful implementation of evidence into practice using the PARIHS framework: theoretical and practical challenges. Implement Sci. 2008, 3: 1-10.1186/1748-5908-3-1.
Ward V, House A, Hamer S: Developing a framework for transferring knowledge into action: a thematic analysis of the literature. J Health Serv Res Policy. 2009, 14: 156-164. 10.1258/jhsrp.2009.008120.
Shojania KG, Sampson M, Ansari MB, Ji J, Doucette S, Moher D: How quickly do systematic reviews go out of date? A survival analysis. Ann Intern Med. 2007, 21: 224-233.
Brouwers M, De Vito C, Carol A, Carroll J, Cotterchio M, Dobbin M, Lent B, Levitt C, Lewis N, McGregor SE, Paszat L, Rand C, Wathen N: Interventions to increase the uptake of cancer screening: guideline recommendations. 2009, Special Report EBS 15-7., [http://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=43168]
Shea BJ, Grimshaw JM, Wells GA, Boers M, Andersson N, Hamel C, Porter AC, Tugwell P, Moher D, Bouter LM: Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Med Res Methodol. 2007, 7: 10-10.1186/1471-2288-7-10.
Grimshaw J, Eccles M, Thomas R, MacLennan G, Ramsay C, Fraser C, Vale L: Toward evidence-based quality improvement. Evidence (and its limitations) of the effectiveness of guideline dissemination and implementation strategies 1966-1998. J Gen Intern Med. 2006, 21: S14-20.
Michie S: Designing and implementing behavior change interventions to improve population health. J Health Serv Res Policy. 2008, 13: 64-69. 10.1258/jhsrp.2008.008014.
Abraham C, Michie S: A taxonomy of behavior change techniques used in interventions. Health Psychol. 2008, 27: 379-387.
Cochrane Effective Practice and Organisation of Care Group (EPOC) (2011): The data collection checklist. 2011, [http://www.epoc.cochrane.org/]
Ammenwerth E, Schnell-Inderst P, Machan C, Siebert U: The effect of electronic prescribing on medication errors and adverse drug events: A systematic review. J Am Med Inform Assoc. 2008, 15: 585-600. 10.1197/jamia.M2667.
Baker R, Camosso-Stefinovic J, Gillies C, Shaw EJ, Cheater F, Flottorp S, Robertson N: Tailored interventions to overcome identified barriers to change: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2010, 3: CD005470-
Beach MC, Gary TL, Price EG, Robinson K, Gozu A, Palacio A, Smarth C, Jenckes M, Feuerstein C, Bass EB, Powe NR, Cooper LA: Improving health care quality for racial/ethnic minorities: A systematic review of the best evidence regarding provider and organization interventions. BMC Public Health. 2006, 6: 104-10.1186/1471-2458-6-104.
Bennett MI, Bagnall AM, José Closs S: How effective are patient-based educational interventions in the management of cancer pain? Systematic review and meta-analysis. Pain. 2009, 143: 192-199. 10.1016/j.pain.2009.01.016.
Bosch-Capblanch X, Abba K, Prictor M, Garner P: Contracts between patients and healthcare practitioners for improving patients' adherence to treatment, prevention and health promotion activities. Cochrane Database Syst Rev. 2007, 18: CD004808-
Chaudhry B, Wang J, Wu S, Maglione M, Mojica W, Roth E, Morton SC, Shekelle PG: Systematic review: impact of health information technology on quality, efficiency, and costs of medical care. Ann Intern Med. 2006, 144: 742-752.
Coleman K, Austin BT, Brach C, Wagner EH: Evidence on the chronic care model in the new millennium. Health Aff (Millwood). 2009, 28: 75-85. 10.1377/hlthaff.28.1.75.
Conn VS, Hafdahl AR, Brown SA, Brown LM: Meta-analysis of patient education interventions to increase physical activity among chronically ill adults. Patient Educ Couns. 2008, 70: 157-172. 10.1016/j.pec.2007.10.004.
Doumit G, Gattellari M, Grimshaw J, O'Brien MA: Local opinion leaders: Effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007, 1: CD000125-
Edwards A, Gray J, Clarke A, Dundon J, Elwyn G, Gaff C, Hood K, Iredale R, Sivell S, Shaw C, Thornton H: Interventions to improve risk communication in clinical genetics: systematic review. Patient Educ Couns. 2008, 71: 4-25. 10.1016/j.pec.2007.11.026.
Evans R, Edwards A, Brett J, Bradburn M, Watson E, Austoker J, Elwyn G: Reduction in uptake of PSA tests following decision aids: systematic review of current aids and their evaluations. Patient Educ Couns. 2005, 58: 13-26. 10.1016/j.pec.2004.06.009.
Garg AX, Adhikari NK, McDonald H, Rosas-Arellano MP, Devereaux PJ, Beyene J, Sam J, Haynes RB: Effects of computerized clinical decision support systems on practitioner performance and patient outcomes: a systematic review. JAMA. 2005, 293: 1223-1238. 10.1001/jama.293.10.1223.
Gaston CM, Mitchell G: Information giving and decision-making in patients with advanced cancer: a systematic review. Soc Sci Med. 2005, 61: 2252-2264. 10.1016/j.socscimed.2005.04.015.
Goldberg GR, Morrison RS: Pain management in hospitalized cancer patients: a systematic review. J Clin Oncol. 2007, 25: 1792-1801. 10.1200/JCO.2006.07.9038.
Gysels M, Richardson A, Higginson IJ: Does the patient-held record improve continuity and related outcomes in cancer care: a systematic review. Health Expect. 2007, 10: 75-91. 10.1111/j.1369-7625.2006.00415.x.
Haynes RB, Ackloo E, Sahota N, McDonald HP, Yao X: Interventions for enhancing medication adherence. Cochrane Database Syst Rev. 2008, 2: CD000011-
Heneghan CJ, Glasziou P, Perera R: Reminder packaging for improving adherence to self-administered long-term medications. Cochrane Database Syst Rev. 2006, 1: CD005025-
Jamtvedt G, Young JM, Kristoffersen DT, O'Brien MA, Oxman AD: Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2006, 2: CD000259-
Joosten EA, DeFuentes-Merillas L, de Weert GH, Sensky T, van der Staak CP, de Jong CA: Systematic review of the effects of shared decision-making on patient satisfaction, treatment adherence and health status. Psychother Psychosom. 2008, 77: 219-226. 10.1159/000126073.
Lewis RA, Neal RD, Williams NH, France B, Hendry M, Russell D, Hughes DA, Russell I, Stuart NS, Weller D, Wilkinson C: Follow-up of cancer in primary care versus secondary care: systematic review. Br J Gen Pract. 2009, 59: e234-47.
Murray E, Burns J, See TS, Lai R, Nazareth I: Interactive health communication applications for people with chronic disease. Cochrane Database Syst Rev. 2005, 4: CD004274-
O'Brien MA, Rogers S, Jamtvedt G, Oxman AD, Odgaard-Jensen J, Kristoffersen DT, Forsetlund L, Bainbridge D, Freemantle N, Davis DA, Haynes RB, Harvey EL: Educational outreach visits: effects on professional practice and health care outcomes. Cochrane Database Syst Rev. 2007, 4: CD000409-
Raynor DK, Blenkinsopp A, Knapp P, Grime J, Nicolson DJ, Pollock K, Dorer G, Gilbody S, Dickinson D, Maule AJ, Spoor P: A systematic review of quantitative and qualitative research on the role and effectiveness of written information available to patients about individual medicines. Health Technol Assess. 2007, 11: iii,-1-160.
Rotter T, Kinsman L, James E, Machotta A, Willis J, Snow P, Kugler J: Clinical pathways: Effects on professional practice, patient outcomes, length of stay and hospital costs. Cochrane Database Syst Rev. 2010, 3: CD006632-
Santo A, Laizner AM, Shohet L: Exploring the value of audiotapes for health literacy: a systematic review. Patient Educ Couns. 2005, 58: 235-243. 10.1016/j.pec.2004.07.001.
Scheuner MT, Sieverding P, Shekelle PG: Delivery of genomic medicine for common chronic adult diseases: a systematic review. JAMA. 2008, 299: 1320-1334. 10.1001/jama.299.11.1320.
Shepperd S, McClaran J, Phillips CO, Lannin NA, Clemson LM, McCluskey A, Cameron ID, Barras SL: Discharge planning from hospital to home. Cochrane Database Syst Rev. 2010, 1: CD000313-
Shojania KG, Jennings A, Mayhew A, Ramsay CR, Eccles MP, Grimshaw J: The effects of on-screen, point of care computer reminders on processes and outcomes of care. Cochrane Database Syst Rev. 2009, 3: CD001096-
Smith SM, Allwright S, O'Dowd T: Effectiveness of shared care across the interface between primary and specialty care in chronic disease management. Cochrane Database Syst Rev. 2007, 3: CD004910-
Smith SM, Allwright S, O'Dowd T: Does sharing care across the primary-specialty interface improve outcomes in chronic disease? a systematic review. Am J Manag Care. 2008, 14: 213-224.
Thomas L, Cullum N, McColl E, Rousseau N, Soutter J, Steen N: Guidelines in professions allied to medicine. Cochrane Database Syst Rev. 2000, 2: CD000349-
Waljee JF, Rogers MA, Alderman AK: Decision aids and breast cancer: Do they influence choice for surgery and knowledge of treatment options?. J Clin Oncol. 2007, 25: 1067-73. 10.1200/JCO.2006.08.5472.
Wilson AD, Childs S: Effects of interventions aimed at changing the length of primary care physicians' consultation. Cochrane Database Syst Rev. 2006, 1: CD003540-
Wofford JL, Smith ED, Miller DP: The multimedia computer for office-based patient education: a systematic review. Patient Educ Couns. 2005, 2: 148-57.
Acknowledgements
The authors of this manuscript wish to acknowledge the research team of the project, the KT for Cancer Control Evidence Expert Panel Members, for their guidance and invaluable contributions. The Evidence Expert Panel Members include Dr. George Browman, Dr. Denise Bryant-Lukosius, Dr. Maureen Dobbins, Dr. Anna Gagliardi, Dr. Ian Graham, Dr. Jeremy Grimshaw, Dr. Mark Levine, Dr. Holger Shünemann, Dr. Hsien Seow, Dr. Marko Simunovic, Dr. Sharon Straus, and Dr. Jonathan Sussman.
The authors also wish to acknowledge Lisa Durocher for her assistance with data collection and auditing.
This review of reviews project was part of the overall "Knowledge Translation for Cancer Control in Canada" research study, conducted with the support of the Ontario Institute for Cancer Research (OICR) through funding provided by the Government of Ontario. The Canadian Partnership Against Cancer (CPAC) also supported the project through funding provided by the Government of Canada.
Author information
Authors and Affiliations
Consortia
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MCB conceived of the study and participated in its design and execution. JM participated in the study's design and coordination. MCB, JM, and KG were directly involved in the preparation of this manuscript. KG and LD were responsible for data collection and data synthesis. All authors read and approved the final manuscript.
Electronic supplementary material
13012_2011_447_MOESM4_ESM.DOC
Additional file 4: Interventions aimed at professionals. Table of data on each intervention aimed at professionals (DOC 94 KB)
13012_2011_447_MOESM5_ESM.DOC
Additional file 5: Interventions aimed at organizations. Table of data on each intervention aimed at organizations (DOC 62 KB)
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Brouwers, M.C., Garcia, K., Makarski, J. et al. The landscape of knowledge translation interventions in cancer control: What do we know and where to next? A review of systematic reviews. Implementation Sci 6, 130 (2011). https://doi.org/10.1186/1748-5908-6-130
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1748-5908-6-130