
Abstract
Desmoplastic fibroma (DF) is a rare, benign but locally aggressive, intraosseous lesion with a high tendency of local recurrence. In this report the actual literature is reviewed regarding epidemiological data, pathology, clinical diagnostic criterias, therapy and prognosis. Moreover, a report of an interesting case is included localized in the mandibular corpus.
Similar content being viewed by others


Introduction
Desmoplastic fibroma (DF) is a benign but locally aggressive neoplasm of the bones [1, 2] and it is very rare in the mandible like some other intraoral tumours [3]. There is no metastasis but beside of their destructive growth they show a high frequent recurrence after local resection [4]. In 1838 the German physiologist and anatomist Johannes Müller [5] characterised the term „desmoid“ (Greek: „desmos“ = „band/ligament“). In 1958 Jaffe [6] firstly described a primarily osseous-arised aggressive fibromatosis of the femur, the tibia and also of the scapula. He declared these tumours as „desmoplastic fibromas“. In 1965 the first report about a desmoplastic fibroma of the jaw was presented by Griffith und Irby [7] and since that time a considerable number of similar cases have been published [2, 4, 8–40]. In jaw area non-odontogenetic fibromatosis was declared as desmoplastic fibroma what distinguished it from odontogenic fibroma [1, 36, 41, 42].
For reviewing the international literature a systematic search in the PupMed database of the National Library of Medicine was performed using the key words "desmoplastic fibroma", "mandible" and "jaw". This search revealed that only 76 cases (from 1968 to 2009) of desmoplastic fibroma in the jaw area have been published to date, which reconfirms the infrequency of these tumours and the low incidence.
Intraosseous desmoplastic fibromas (DF) are very rare myofibroblastic tumours (far less than 1% of all bone tumours) [43, 44] and they can occur in every bone of the body. In 22% of all cases the mandible is mostly affected [4, 43]. These benign but locally agressive lesions offer many similarities to soft-tissue DF [41]. The incidence of desmoplastic fibroma of the jaw is equal in male and female patients [45]. On average, patients are 15.1 years old at the time of the final diagnosis [46]. Pathognomonic symptoms do not exist and their occurence is mostly insidious. Some cases described pain and swellings [47–49]. Radiologic findings are unspecific and extend from mono- to polycystic appearance with a partially sharp or diffuse borderline [50]. Magnetic resonance imaging can clearly distinguish between intraosseous tumours and normal bone marrow and is particularly suitable for surgical planning [43]. As therapy, surgical resections, radiotherapy and if necessary, pharmacological treatments are recommended. In respect of the high recurrence rate, surgical resection is the most favourite option [44, 51, 52], but depending on tumour localisation (e.g. cerebric) or resulting mutilations it is not always feasible. In cases of non-in-sano resected fibromatosis the recurrence rate can be lowered significantly by adjuvant radiotherapy [53]. However, the prospected mutagenic effects makeradiotherapy not suitable as a solitary treatment [47]
In this report we present the clinical course and therapy of a patient with the first diagnosis of a desmoplastic fibroma in the left mandibular corpus, after resection of an extensive but low-grade myofibroblastic sarcoma in the right ramus 8 years before. Regarding the mental nerve we decided on a gentle resection and an observing follow-up strategy after the final diagnosis had been confirmed. Ten months after resection, clinical and radiographical controls of our patient showed no recurrence of the DF, but a periodic follow-up over at least 3 years is recommended [54]
Case Report
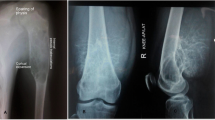
A 23-year-old Caucasian male patient consulted the Department for Cranio- and Maxillofacial Surgery for analysing an intraosseus, rounded tumour in the left mandibular corpus, which was initially diagnosed by an MRI scan 12 months ago in a different institute (Fig. 1). This MRI was part of a routinely follow-up, since 10 years before two intracranial, solid and non-proliferating soft-tissue-tumours were diagnosed in the right cerebellar hemisphere (close to the foramen magnum) and underneath the left temporal lobe. Additionally, two years later an extensive but low-grade myofibroblastic sarcoma in the right ramus of the mandible was resected. A current panoramic radiography (Fig. 2) showed a well circumscribed, rounded osteolysis with a diameter of 13 mm in immediate proximity to the left mental foramen. Besides, the known and in size constant translucency within the right ramus (after sarcoma-resection 8 years before) appeared inconspicuously. There were no other pathological findings.

MRI (T1-weighted) illustrating a 10 mm tumour within the left mandibular corpus (red arrow).

Panoramic radiography (patient, 23 years): 13 mm osteolysis in left mandible (red arrow). Noted translucency within the right ramus (blue arrow).
As therapy a paramarginal approach showed the intact vestibular cortical surface with an inconspicuous mental foramen and a normal structured mental nerve. The osteotomy exposed a rounded cavity, in which a 1.3 × 0.9 × 0.6 cm sized, greying, tubercular, firm-elastic conjunctive-tissue-tumour was located. This tumour showed a very slight adherence to the surrounding bone and was resected easily. After that the bone cavity was carefully reamed under preservation of the mental nerve. Because of the small defect-size any bone-grafting material could be dispensed. The histopathological examination revealed a mesenchymal tumor, composed of spindle-shaped cells with myofibroblastic differentiation, abundant collagen formation and low proliferation activity (Fig. 3 and 4). In immunohistochemical stainings the tumour-cells showed a positive reaction for smooth muscle actin and a negative reaction for S100 (data not shown). With the proliferation marker Mib1 less than 5% of the tumour-cells proved to be positive. Based on these characteristics the diagnosis of a desmoplastic fibroma was made, and this diagnosis was confirmed by a reference institute. The post-operative recovery was normal based on clinical examination The radiographical (panoramic X-ray) follow-up showed an obvious ossification of the former resection cavity (Fig. 5) and the patient described no hypaesthesia of the mental nerve at any time.

Partially parallel or plexiform arranged spindelcells with slim and elongated nucleus without cytological sings of malignity (HE-staining; original magnification: 100×).

High-grade formation of collagen fibres (red) (EvG-staining; original magnification: 100×).

Panoramic radiography (10 month after resection): No recurrence and obvious ossification in the area of the former osteolysis (red arrow).
In conclusion the Desmoplastic fibroma (DF) is a rare, benign but locally aggressive, intraosseous lesion with a high tendency of local recurrence. With respect of the patient's post-operative well-being and if periodic follow-ups are guaranteed, the tumor should be carefully resected with only narrow safety margins.
Consent
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal
References
Langlais RP, Langland OE, Nortje CJ: Multilocular radiolucencies. 1995, Baltimore: Williams & Williams
Siemssen SJ, Anagnostaki T: Aggressive fibromatosis (extra-abdominal desmoids) of the head and neck. Br J Plast Surg. 1984, 37: 453-457. 10.1016/0007-1226(84)90129-2.
Handschel J, Herbst H, Brand B, Meyer U, Piffko J: Intraoral sebaceous carcinoma. Br J Oral Maxillofac Surg. 2003, 41: 84-87. 10.1016/S0266-4356(03)00036-6.
Said-Al-Naief N, Fernandes R, Louis P, Bell W, Siegal GP: Desmoplastic fibroma of the jaw: a case report and review of literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006, 101: 82-94. 10.1016/j.tripleo.2005.03.034.
Müller J: Über den feineren Bau und die Formen der krankhaften Geschwülste. Erste Lieferung. 1838, Berlin: G. Reimer
Jaffe HL: Tumors and thrombus conditions of the bones and joints. 1958, Philadelphia: Lea & Febiger
Griffith JG, Irby WB: Desmoplastic Fibroma. Report of a Rare Tumor of the Oral Structures. Oral Surg Oral Med Oral Pathol. 1965, 20: 269-275. 10.1016/0030-4220(65)90201-X.
Badger GA, Syed AA, Malby FC: Desmoplastic fibroma of the mandible. Can J Otolaryngol. 1974, 3: 605-610.
Bakaeen G, Rajab LD: Desmoplastic fibroma of the mandible: report of a case. Int J Paediatr Dent. 1999, 9: 117-121. 10.1046/j.1365-263x.1999.00115.x.
Buhl TJ, Pedersen U, Steiniche T, Fink-Jensen V: [Desmoplastic fibroma of the mandible]. Ugeskr Laeger. 2004, 166: 281-282.
Calatrava L, Donado M: Desmoplastic fibroma of the mandible: case report. J Maxillofac Surg. 1976, 4: 238-241. 10.1016/S0301-0503(76)80045-8.
Chemli H, Karray F, Dhouib M, Makni S, Abdelmoula M: [Mandibular desmoplastic fibroma: Diagnosis and therapeutics difficulties]. Rev Stomatol Chir Maxillofac. 2009, 110 (4): 239-41. 10.1016/j.stomax.2009.03.002.
Chen YG, Peng LL, Lu QN, Sun YH, Qiao JG, Zhao Y: [Skeletal desmoplastic fibroma in right mandible: a case report]. Hua Xi Kou Qiang Yi Xue Za Zhi. 2008, 26: 222-224.
Christiansen RL: Desmoplastic fibroma of the ramus and body of the mandible. Cranio. 1990, 8: 271-275.
Cranin AN, Gallo L, Madan S: Desmoplastic fibroma. A rare oral tumor in children. N Y State Dent J. 1994, 60: 34-39.
Cunningham CD, Smith RO, Enriquez P, Singleton GT: Demoplastic fibroma of the mandible. A case report. Ann Otol Rhinol Laryngol. 1975, 84: 125-129.
Freedman PD, Cardo VA, Kerpel SM, Lumerman H: Desmoplastic fibroma (fibromatosis) of the jawbones. Report of a case and review of the literature. Oral Surg Oral Med Oral Pathol. 1978, 46: 386-395. 10.1016/0030-4220(78)90404-8.
Green TL, Gaffney E: Desmoplastic fibroma of the mandible. J Oral Med. 1981, 36: 47-49.
Herford AS, Reder P, Ducic Y: Multifocal desmoplastic fibromas of the mandible. J Oral Maxillofac Surg. 2001, 59: 1078-1081. 10.1053/joms.2001.25032.
Hietanen J, Lukinmaa PL, Calonius PE, Kassila O: Desmoplastic fibroma involving the mandible. Br J Oral Maxillofac Surg. 1986, 24: 442-447. 10.1016/0266-4356(86)90060-4.
Hinds EC, Kent JN, Fechner RE: Desmoplastic fibroma of the mandible: report of case. J Oral Surg. 1969, 27: 271-274.
Hopkins KM, Huttula CS, Kahn MA, Albright JE: Desmoplastic fibroma of the mandible: review and report of two cases. J Oral Maxillofac Surg. 1996, 54: 1249-1254. 10.1016/S0278-2391(96)90363-8.
Hovinga J, Ingenhoes R: A desmoplastic fibroma in the mandible. Int J Oral Surg. 1974, 3: 41-44. 10.1016/S0300-9785(74)80035-9.
Iatrou IA, Theologie-Lygidakis N, Leventis MD: Case report: desmoplastic fibroma of the mandible in a child presenting with TMJ dysfunction. Eur Arch Paediatr Dent. 2008, 9: 105-108.
Ikeshima A, Utsunomiya T: Case report of intra-osseous fibroma: a study on odontogenic and desmoplastic fibromas with a review of the literature. J Oral Sci. 2005, 47: 149-157. 10.2334/josnusd.47.149.
Iwai S, Matsumoto K, Sakuda M: Desmoplastic fibroma of the mandible mimicking osteogenic sarcoma: report of a case. J Oral Maxillofac Surg. 1996, 54: 1370-1373. 10.1016/S0278-2391(96)90500-5.
Kwon PH, Horswell BB, Gatto DJ: Desmoplastic fibroma of the jaws: surgical management and review of the literature. Head Neck. 1989, 11: 67-75. 10.1002/hed.2880110112.
Makek M, Lello GE: Desmoplastic fibroma of the mandible: literature review and report of three cases. J Oral Maxillofac Surg. 1986, 44: 385-391. 10.1016/0278-2391(86)90077-7.
Marlette RH, Gerhard RC: Intraosseous "fibroma" and "fibromyxoma" of the mandible. Report of three cases. Oral Surg Oral Med Oral Pathol. 1968, 25: 792-799. 10.1016/0030-4220(68)90049-2.
Nussbaum GB, Terz JJ, Joy ED: Desmoplastic fibroma of the mandible in a 3-year-old child. J Oral Surg. 1976, 34: 1117-1121.
Rabhan WN, Rosai J: Desmoplastic fibroma. Report of ten cases and review of the literature. J Bone Joint Surg Am. 1968, 50: 487-502.
Reid EN, Lawoyin DO, Suresh L, Longwe E: Desmoplastic fibroma of the anterior mandible. Case report and review of literature. N Y State Dent J. 2009, 75: 32-33.
Rubin MM, Cozzi GM, Shih HJ: Recurrent desmoplastic fibroma of the mandible: report of case. J Am Dent Assoc. 1987, 115: 705-707.
Schmaman A, Smith I, Ackerman LV: Benign fibro-osseous lesions of the mandible and maxilla. A review of 35 cases. Cancer. 1970, 26: 303-312. 10.1002/1097-0142(197008)26:2<303::AID-CNCR2820260210>3.0.CO;2-V.
Shi H, Wang P, Wang S, Yu Q: Desmoplastic fibroma of the mandible. Dentomaxillofac Radiol. 2008, 37: 408-411. 10.1259/dmfr/86899184.
Slootweg PJ, Muller H: Central fibroma of the jaw, odontogenic or desmoplastic. Oral Surg Oral Med Oral Pathol. 1983, 56: 61-70. 10.1016/0030-4220(83)90057-9.
Taguchi N, Kaneda T: Desmoplastic fibroma of the mandible: report of case. J Oral Surg. 1980, 38: 441-444.
Templeton K, Glass N, Young SK: Desmoplastic fibroma of the mandible in a child: report of a case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997, 84: 620-623. 10.1016/S1079-2104(97)90362-0.
Valente G, Migliario M, Bianchi SD, Vercellino V: Desmoplastic fibroma of the mandible: a case with an unusual clinical presentation. J Oral Maxillofac Surg. 1989, 47: 1087-1089. 10.1016/0278-2391(89)90188-2.
Wagner JE, Lorandi CS, Ebling H: Desmoplastic fibroma of bone. A case in the mandible. Oral Surg Oral Med Oral Pathol. 1977, 43: 108-111. 10.1016/0030-4220(77)90358-9.
Regezi JA, Sciubba JJ: Odontogenic tumors, benign nonodontogenic tumors. Oral pathology: clinical pathologic correlations. 1999, Philadelphia: W.B. Saunders, 3
Depprich R, Handschel J, Sebald W, Kubler NR, Wurzler KK: [Comparison of the osteogenic activity of bone morphogenetic protein (BMP) mutants]. Mund Kiefer Gesichtschir. 2005, 9: 363-368. 10.1007/s10006-005-0644-2.
Bohm P, Krober S, Greschniok A, Laniado M, Kaiserling E: Desmoplastic fibroma of the bone. A report of two patients, review of the literature, and therapeutic implications. Cancer. 1996, 78: 1011-1023. 10.1002/(SICI)1097-0142(19960901)78:5<1011::AID-CNCR11>3.0.CO;2-5.
Weiss S, Goldblum J: Enzinger and Weiss's soft tissue tumors. St Louis. 2001, 4
Sinno H, Zadeh T: Desmoid tumors of the pediatric mandible: case report and review. Ann Plast Surg. 2009, 62: 213-219. 10.1097/SAP.0b013e31817f020d.
Ikeshima A, Utsunomiya T: Case report of intra-osseous fibroma: a study on odontogenic and desmoplastic fibromas with a review of the literature. J Oral Sci. 2005, 47: 149-157. 10.2334/josnusd.47.149.
Crim JR, Gold RH, Mirra JM, Eckardt JJ, Bassett LW: Desmoplastic fibroma of bone: radiographic analysis. Radiology. 1989, 172: 827-832.
Inwards CY, Unni KK, Beabout JW, Sim FH: Desmoplastic fibroma of bone. Cancer. 1991, 68: 1978-1983. 10.1002/1097-0142(19911101)68:9<1978::AID-CNCR2820680922>3.0.CO;2-H.
Meyer U, Kleinheinz J, Handschel J, Kruse-Losler B, Weingart D, Joos U: Oral findings in three different groups of immunocompromised patients. J Oral Pathol Med. 2000, 29: 153-158. 10.1034/j.1600-0714.2000.290402.x.
Fisker AV, Philipsen HP: Desmoplastic fibroma of the jaw bones. Int J Oral Surg. 1976, 5: 285-291. 10.1016/S0300-9785(76)80029-4.
Ayala AG, Ro JY, Goepfert H, Cangir A, Khorsand J, Flake G: Desmoid fibromatosis: a clinicopathologic study of 25 children. Semin Diagn Pathol. 1986, 3: 138-150.
Faulkner LB, Hajdu SI, Kher U, La Quaglia M, Exelby PR, Heller G, Wollner N: Pediatric desmoid tumor: retrospective analysis of 63 cases. J Clin Oncol. 1995, 13: 2813-2818.
Altmann S, Lenz-Scharf O, Schneider W: Therapeutic options for aggressive fibromatosis. Handchir Mikrochir Plast Chir. 2008, 40: 88-93. 10.1055/s-2007-965738.
Bridge JA, Swarts SJ, Buresh C, Nelson M, Degenhardt JM, Spanier S, Maale G, Meloni A, Lynch JC, Neff JR: Trisomies 8 and 20 characterize a subgroup of benign fibrous lesions arising in both soft tissue and bone. Am J Pathol. 1999, 154: 729-733.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
All authors disclaim any financial or non-financial interests or commercial associations that might pose or create a conflict of interest with information presented in this manuscript.
Authors' contributions
MS, AZ, RD, CN and JH made substantial contribution to the conception and design of the manuscript. RE carried out the pathological investigations and participated in creating this part of the manuscript.
All authors were involved in revising the manuscript critically and have given final approval of the version to be published.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Schneider, M., Zimmermann, A.C., Depprich, R.A. et al. Desmoplastic fibroma of the mandible - review of the literature and presentation of a rare case. Head Face Med 5, 25 (2009). https://doi.org/10.1186/1746-160X-5-25
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1746-160X-5-25