
Abstract
Background
Evaluation of self perceived and actual need for orthodontic treatment helps in planning orthodontic services and estimating the required resources and man power. In the present study, the perceptive need as evaluated by patients and the actual need to orthodontic treatment, as assessed by orthodontists, were evaluated at two types of dental practices in the city of Jeddah using the Index of Orthodontic Treatment Need (IOTN).
Methods
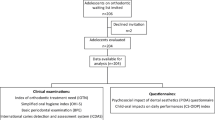
A consecutive sample of 743 adults seeking orthodontic treatment at two different types of dental practices in Jeddah; King Abdulaziz University, Faculty of Dentistry (KAAU) (Free treatment) and two private dental polyclinics (PDP) (Paid treatment), was examined for orthodontic treatment need using the dental health component (DHC) of the IOTN. The self-perceived need for orthodontic treatment was also determined using the aesthetic component (AC) of the IOTN. The IOTN score and the incidence of each variable were calculated statistically. AC and DHC categories were compared using the Chi-Square and a correlation between them was assessed using Spearman's correlation test. AC and DHC were also compared between the two types of dental practices using the Chi-Square.
Results
The results revealed that among the 743 patients studied, 60.6% expressed no or slight need for treatment, 23.3% expressed moderate to borderline need and only16.1% thought they needed orthodontic treatment. Comparing these estimates to professional judgments, only 15.2% conformed to little or no need for treatment, 13.2% were assessed as in borderline need and 71.6% were assessed as in need for treatment (p < 0.001). Spearman's correlation test proved no correlation (r = -.045) between the two components. Comparing the AC and the DHC between the KAAU group and PDP group showed significant differences between the two groups (p < 0.001).
Conclusion
Patient's perception to orthodontic treatment does not always correlate with professional assessment. The IOTN is a valid screening tool that should be used in orthodontic clinics for better services especially, in health centers that provide free treatment.
Similar content being viewed by others


Background
Orthodontic treatment is an elective treatment that depends on the perception of both the patient and the treating orthodontist. In Saudi Arabia, governmental sectors provide free orthodontic treatment for Saudi citizens. This has generated long waiting lists of patients that can extend for two to four years. Evaluation of self perceived and actual need for orthodontic treatment as well as other factors affecting these needs such as personal, socio-demographic, and psychosocial factors help in planning orthodontic services and estimating the required resources and manpower. Moreover, unnecessary referrals by general practitioners and lengthy waiting lists for orthodontic treatment can be eliminated by limiting free treatment to patients with malocclusions sever enough to warrant treatment [1, 2]. It may also predict patients' level of interest and motivation toward the orthodontic treatment, which could help in planning educational programs in schools and media to increase patient's awareness and to overcome obstacles and barriers in seeking treatment [3].
Perceptive or self assessed need to dental care is reported to be associated with certain signs and symptoms [4], socio-demographic factors and satisfaction with previous dental treatment [5, 6]. Previous studies have shown differences between patients' and professionals' perception on orthodontic treatment need [8–13]. It seems that normative or actual need as assessed by dental professionals may not be linked to patients' perceptions unless the condition has progressed sufficiently to be symptomatic [7]. Several indices were developed to evaluate malocclusion, such as the IOTN [11], PAR (Peer Assessment Rating Index) [14] and ICON (Index of Complexity, outcome and Need) [15]. The IOTN and the ICON can serve as neutral instruments to determine treatment needs and to allocate financial resources for orthodontic cases [16]. Although the IOTN and the ICON are similar and largely in agreement in measuring treatment needs of patients from different ethnic backgrounds [17], the IOTN has been used extensively in literature to evaluate actual and perceptive treatment needs in different ethnic backgrounds and it seems to be a more popular research tool in the Middle East than the ICON [18–32]. In addition, the IOTN is simpler than the ICON in assessing treatment needs since ICON was designed to measure complexity of treatment in addition to treatment needs [15].
The IOTN is a scoring system for malocclusion, developed by Brook & Shaw (1989) [11]. It consists of two independent components; the DHC, which is a five grade index that records the dental health need for orthodontic treatment, and the AC that records the aesthetic need for orthodontic treatment using a ten grade standardized ranking scale of colored photographs showing different levels of dental attractiveness. In Saudi Arabia, not a single study has been conducted regarding treatment needs among regular orthodontic patients.
The objectives of the present study were:
1- To assess the perceptive and actual treatment needs for orthodontic treatment among subjects seeking orthodontic treatment in the city of Jeddah using the IOTN
2- To compare those subjects attending a governmental dental clinic (KAAU), with those attending PDP utilizing the IOTN.
Methods
A consecutive sample of 743 subjects (aged 17–24 years) seeking orthodontic treatment was used in this study. The sample was collected from two different types of practices; KAAU (N = 489) and two PDPs in the city of Jeddah (N = 254) during the period of August-November 2004. All subjects were of Arabic descendants and with no history of orthodontic treatment. The treatment at KAAU is free of charge while the treatment at PDPs is quite expensive for the general Saudi population. All subjects who were enrolled in the study signed a consent form. Each subject was examined for orthodontic treatment need using the DHC of the IOTN. Additionally, the self-perceived need for orthodontic treatment was determined by asking each subject to evaluate his or her own attractiveness by comparing it to the standard photographs of the AC of the IOTN. Two examiners were involved in the study, one for the DHC and the other for the AC. The examiners were trained to use the IOTN following the instructions provided with the IOTN materials. The IOTN score and the incidence of each variable were calculated statistically. The sample used in the present study was distribution free and therefore non-parametric tests were used. The AC and DHC categories were compared between the two groups using the Chi-Square. The DHC and the AC were also compared using the Chi-Square and were correlated using Spearman's Correlation coefficient. The protocol of the present study was approved by the Ethical Committee of the Faculty of Dentistry at King Abdulaziz University.
Results
The highest incidence of orthodontic problems in the current study was for displacement (89.1%), followed by crossbite (44.5%), deep overbite (33.6%), increased overjet (33.6) and openbite (20%). Impaction incidence was relatively low (8.2%). The incidence of cleft lip and palate was 3.9% (Table 1)
Results of the AC revealed that among the 743 patients studied, 60.6% expressed no or slight need for treatment, while 23.3% expressed moderate to borderline need and 16.1% expressed great need for orthodontic treatment. Comparing these estimates to professional judgments using the Chi Square, the DHC was significantly (<0.001) different from the AC in the three groups; 15.2% had little to no treatment need (grades I & II), 13.2% had borderline treatment need (grade III) and 71.6% had a great need for orthodontic treatment (grade IV & V) (Table 2 & Figure 1). Spearman's correlation between the AC and DHC proved no correlation (r = -0.045) between the two components.

Graphical representation table 2.
Comparing the grades of DHC between the KAAU group and the PDP group (Table 3 & Figure 2) revealed that the proportion of the sample estimated to have little to no treatment need (Grade I & II) was significantly higher in the KAAU group (18.2%) than that of PDP Group (9.4%) (p < 0.001). The border line proportion (Grade III) was insignificantly different between the two groups. The proportion of the sample estimated to have a great treatment need was significantly higher in the PDP group than the KAAU group (p < 0.001).

Graphical representation of table 3.
Comparing the grades of the AC between the KAAU group and the PDP group (Table 4 & Figure 3) revealed significant differences between the two groups; no or slight treatment need was higher in the KAAU group (72.7%) than PDP group (37.4%) and border line and great treatment needs were higher in the PDP group (40.55% & 22.04% respectively) than in the KAAU group (14.3% & 12.9% respectively).

Graphical representation of table 4.
Discussion
The results of the DHC shed some light on the pattern of malocclusion that is seen in the city of Jeddah, Saudi Arabia, which is dominant mainly of displacement, crossbite, deep bite and increased overjet. However, larger scale studies are required to evaluate the actual pattern of malocclusion in the western region of Saudi Arabia via conducting survey studies on a random sample. The age group targeted in the present study was different than most of the previous studies [1, 8, 9, 13, 19], which were conducted on children and adolescents who are less reliable in their perception than adults, especially when using the IOTN which moderately reflects the subjective perception of dental aesthetics and demand for orthodontic treatment [30].
The significant differences between the AC and DHC and the negative weak correlation between the perceptive and actual need for orthodontic treatment indicates a general lack of awareness among the Saudis about the severity of their existing malocclusion. This can be attributed to their weak oral health knowledge as well as parents' neglect towards malocclusion. This is in agreement with several other studies [8–10]. Moreover, the perception of occlusal traits in the buccal segments is generally underestimated by people when compared to those present in the anterior segment [22, 23]. The results can also be attributed to the nature of the IOTN itself. The scores of the DHC may have been exaggerated by the rank of displacement, which would give a high score in otherwise normal occlusion. In addition, the standard photographs of the AC do not show common orthodontic problems such as open bite, which represents a relatively high incidence in the studied sample (20%). This may have misled those subjects with openbite in their perception of their malocclusion. Also, there is no evidence of how the severity of those traits is perceived by people. These shortcomings of the IOTN indicate the need to study the appropriateness of the IOTN or ICON as an index for the Saudi Arabians or even to develop a new index that suits such population.
The results have also shown less awareness and appreciation of the severity of malocclusion among patients seeking treatment in a governmental dental clinic such as KAAU, when compared to those paying for their treatment at private dental polyclinics. This could explain the lack of compliance seen among those patients. Little awareness for the actual need for treatment in the KAAU group could be attributed to the free treatment provided, which attracts anyone to seek treatment regardless of the severity of his or her malocclusion. Therefore, it is recommended to use the DHC of the IOTN as a screening tool to reevaluate the waiting lists of patients seeking orthodontic treatment at governmental clinics. This would identify those patients who could benefit the most from such free services and subsequently reduce the long waiting lists at such centers. In addition, the application of minimum charge for treatment at governmental dental clinics can serve the same purpose.
Conclusion
There is a definitive need for orthodontic treatment among Saudis living in the city of Jeddah, which is not matched with a similar level of perceptive need by the same population. The grades of AC and DHC were significantly different between those patients seeking free treatment at governmental dental centers and those who pay for their treatment at private dental practices.
References
Burden DJ, Pine CM: Self-perception of malocclusion among adolescents. Community Dent Health. 1995, 12: 89-92.
Chew MT, Aw AK: Appropriateness of orthodontic referrals: self-perceived and normative treatment needs of patients referred for orthodontic consultation. Community Dent Oral Epidemiol. 2002, 30: 449-454. 10.1034/j.1600-0528.2002.00017.x.
Grzywacz I: The value of the aesthetic component of the Index of Orthodontic Treatment Need in the assessment of subjective orthodontic treatment need. Eur J of Orthod. 2003, 25: 57-63. 10.1093/ejo/25.1.57.
Gilbert GH, Heft MW, Duncan RP, Ringelberg ML: Perceived need for dental care in dentate older adults. Int Dent J. 1994, 44: 145-152.
Atchison KA, Matthias RE, Dolan TA, Lubben JE, De Jong F, Schweitzer SO, Mayer-Oakes SA: Comparison of oral health ratings by dentists and dentate elders. J Public Health Dent. 1993, 53: 223-230.
Matthias RE, Atchison KA, Lubben JE, De Jong F, Schweitzer SO: Factors affecting self-ratings of oral health. J Public Health Dent. 1995, 55: 197-204.
Heft MW, Gilbert GH, Shelton BJ, Duncan RP: Relationship of dental status, sociodemographic status, and oral symptoms to perceived need for dental care. Community Dent Oral Epidemiol. 2003, 31: 351-360. 10.1034/j.1600-0528.2003.00014.x.
Lindsay SJ, Hodgkins JF: Children's perceptions of their own malocclusions. Br J Orthod. 1983, 10: 13-20.
Roberts EE, Beales JG, Dixon L, Willcocks AJ, Willmot DR: The orthodontic condition and treatment status of a sample of 14-year-old children in North Derbyshire. Community Dent Health. 1989, 6: 249-256.
Tulloch JF, Shaw WC, Underhill C, Smith A, Jones G, Jones M: A comparison of attitudes toward orthodontic treatment in British and American communities. Am J Orthod. 1984, 85: 253-259. 10.1016/0002-9416(84)90064-2.
Brook PH, Shaw WC: The development of an index of orthodontic treatment priority. Eur J Orthod. 1989, 11: 309-320.
Burden DJ, Pine CM, Burnside G: Modified IOTN: an orthodontic treatment need index for use in oral health surveys. Community Dent Oral Epidemiol. 2001, 29: 220-225. 10.1034/j.1600-0528.2001.290308.x.
Hamdan AM: The relationship between patient, parent and clinician perceived need and normative orthodontic treatment need. Eur J Orthod. 2004, 26: 265-271. 10.1093/ejo/26.3.265.
Richmond S, Shaw WC, O'Brien KD, Buchanan IB, Jones R, Stephens CD, Roberts CT, Andrews M: The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod. 1992, 14: 125-139.
Daniels CP, Richmond S: The development of the Index of Complexity Outcome and Need (ICON). J Orthod. 2000, 27: 149-162. 10.1093/ortho/27.2.149.
Kuijpers MA, Kiekens RM: Research methods in dentistry 10. Assessment of orthodontic treatment need. Ned Tijdschr Tandheelkd. 2005, 112: 206-210.
Fox NA, Daniels C, Gilgrass T: A comparison of the index of complexity outcome and need (ICON) with the peer assessment rating (PAR) and the index of orthodontic treatment need (IOTN). Br Dent J. 2002, 193: 225-30. 10.1038/sj.bdj.4801530.
Al Yami EA, Kuijpers-Jagtman AM, van't Hof MA: Orthodontic treatment need prior to treatment and 5 years postretention. Community Dent Oral Epidemiol. 1998, 26: 421-427.
Birkeland K, Boe OE, Wisth PJ: Orthodontic concern among 11-year-old children and their parents compared with orthodontic treatment need assessed by index of orthodontic treatment need. Am J Orthod Dentofacial Orthop. 1996, 110: 197-205. 10.1016/S0889-5406(96)70109-9.
Tickle M, Kay EJ, Bearn D: Socio-economic status and orthodontic treatment need. Community Dental Oral Epidemiol. 1999, 27: 413-418.
Wang G, Hagg U, Ling J: The orthodontic treatment need and demand of Hong Kong Chinese children. Chin J Dent Res. 1999, 2: 84-92.
Mandall NA, Wright J, Conboy FM, O'Brien KD: The relationship between normative orthodontic treatment need and measures of consumer perception. Community Dent Health. 2001, 18: 3-6.
Ahmed B, Gilthorpe MS, Bedi R: Agreement between normative and perceived orthodontic need amongst deprived multiethnic school children in London. Clin Orthod Res. 2001, 4: 65-71. 10.1034/j.1600-0544.2001.040202.x.
Abdullah MS, Rock WP: Perception of dental appearance using Index of Treatment Need (Aesthetic Component) assessments. Community Dent Health. 2002, 19: 161-165.
Chew MT, Aw AK: Appropriateness of orthodontic referrals: self-perceived and normative treatment needs of patients referred for orthodontic consultation. Community Dent Oral Epidemiol. 2002, 30: 449-454. 10.1034/j.1600-0528.2002.00017.x.
Al-Sarheed M, Bedi R, Hunt NP: Orthodontic treatment need and self-perception of 11–16-year-old Saudi Arabian children with a sensory impairment attending special schools. J Orthod. 2003, 30: 39-44. 10.1093/ortho/30.1.39.
Helm S, Petersen PE, Kreiborg S, Solow B: Effect of separate malocclusion traits on concern for dental appearance. Community Dent Oral Epidemiol. 1986, 14: 217-220.
Espeland LV, Stenvik A: Perception of personal dental appearance in young adults: relationship between occlusion, awareness, and satisfaction. Am J Orthod Dentofacial Orthop. 1991, 100: 234-241.
Abu Alhaija ES, Al-Nimri KS, Al-Khateeb SN: Self-perception of malocclusion among north Jordanian school children. Eur J Orthod. 2005, 27: 292-295. 10.1093/ejo/cjh094.
Grzywacz I: The value of the aesthetic component of the Index of Orthodontic Treatment Need in the assessment of subjective orthodontic treatment need. Eur J Orthod. 2003, 25: 57-63. 10.1093/ejo/25.1.57.
Kerosuo H, Al Enezi S, Kerosuo E, Abdulkarim E: Association between normative and self-perceived orthodontic treatment need among Arab high school students. Am J Orthod Dentofacial Orthop. 2004, 125: 373-8. 10.1016/j.ajodo.2003.04.009.
Mugonzibwa EA, Kuijpers-Jagtman AM, Van't Hof MA, Kikwilu EN: Perceptions of dental attractiveness and orthodontic treatment need among Tanzanian children. Am J Orthod Dentofacial Orthop. 2004, 125: 426-33. 10.1016/j.ajodo.2003.11.002.
Acknowledgements
The author would like to thank Prof. Hala Amer, Dr. Amna Siddiqi and Dr. Reema Al Ghaithy at the Faculty of Dentistry, King Abdulaziz University for their valuable contributions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Hassan, A.H. Orthodontic treatment needs in the western region of Saudi Arabia: a research report. Head Face Med 2, 2 (2006). https://doi.org/10.1186/1746-160X-2-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1746-160X-2-2