
Abstract
Background
Cough reflex can be induced by the pepper extract capsaicin and by low pH in guinea-pig airways. Transient receptor potential vanniloid-1 (TPRV-1) is expressed in the sensory and afferent nerve fibres in airways.
Objective
We hypothesized that a novel pyridazinylpiperazine analog TPRV-1 inhibitor can effectively reduce cough reflex stimulated by citric acid and capsaicin.
Methods
Guinea pigs were injected with specific TPRV-1 inhibitor, V112220, a pyridazinylpiperazine analog of N-(4-tertiarybutylphenyl)-4-(3-chloropyridin-2-yl) tetrahydropyrazine-1(2H)-carbox-amide (BCTC) (3 mg/kg) intra-peritoneally. One hour before cough response assessment. Coughs were recorded using a recorder system that identified cough sound and accompanying expiratory flows, distinct from sneezes. Guinea-pigs exposed to citric acid (0.4 M) and to capsaicin (10-4M) aerosols, in succession separately by 2 hours.
Results
V112220 significantly inhibited the number of coughs induced by citric acid (73 ± 11%, p < 0.01) and capsaicin (70 ± 9.4%, p < 0.05) compared to vehicle control.
Conclusion
A novel pyridazinylpiperazine analog TPRV-1 inhibitor can inhibit the cough reflex, induced by both low pH and capsaicin, suggesting that it could be clinically beneficial in treatment of cough.
Similar content being viewed by others

Introduction
Capsaicin is a potent tussive agent in most species including humans. It activates a capsaicin receptor, transient receptor potential vanilloid-1 (TRPV-1), which is a polymodal ion channel [1] that is activated by stimuli other than capsaicin such as, heat, acid [2] and endogenous compounds such as anandamide, bradykinin and endocannabinoids [1, 3, 4]. Acidification of the airway in guinea-pig also activates A-δ fibres and vagal C-fibre nerves, partly through activation of TRPV-1 [5, 6]. TRPV-1 expression has been found in epithelial nerves in guinea-pig and in humans [7–9]; in chronic cough patients, the expression of TRPV-1 in epithelial nerves is enhanced [7].
Several antagonists of TRPV-1 have now been described [10]. Capsazepine is one of the first antagonists described, and blocks cough induced by capsaicin and citric acid [11–13]. In addition, other antagonists such as iodo-resiniferatoxin and BCTC have also been shown to reduce capsaicin and citric acid cough in guinea-pigs [14, 15]. We investigated the effect of a novel and more selective TRPV-1 antagonist [16–18], V112220, on cough induced by capsaicin and citric acid in the conscious guinea-pig.
Materials and methods
The protocols were approved by the Imperial College BioSciences Group and performed under a Project License from the British Home Office, UK, under the Animals (Scientific Procedures) Act 1986.
Animals
Pathogen free Male Hartley guinea pigs (600 – 700 g) were used for the study. Animals were screened one week before the in vivo cough examination.
Reagents
Materials used in the study including: V112220, a selective TRPV1 antagonist (Purdue Pharma, Ardsley, New York); vehicle, 20% hydroxypropyl-β cyclodextrin (Sigma, Dorset, UK); Procaterol hydrochloride (Sigma, Dorset, UK); Citric Acid (Sigma, Dorset, UK) and Capsaicin (Sigma, Dorset, UK).
Pre-screening of animals
Conscious guinea pigs were pre-screened to assess their cough response to 0.4 M citric acid one week before the cough study with V112220 or diluent. Low responders (number of coughs < 3) and high responders (number of coughs > 20) were excluded from the study. After pre-screening, animals were allocated into 3 different groups, the control group (n = 4) and two treatment groups (either with V112220 or vehicle, n = 5).
In vivo cough measurements
Conscious animals were placed in a 4 L plethysmograph which was equipped with an internal microphone and a pressure transducer, and were connected to a Amplifier Interface Unit series pre-amplifier (EMMS, Hants, UK). Aerosols were generated with an ultrasonic nebuliser (DeVilbiss, London, UK) which was connected to a Basic Flow Supplier AIR 200 (EMMS, Hants, UK). Airflow was set at 8 L/min. Coughs were detected in three ways: via the microphone, via the pressure transducer and by observing the guinea-pig behaviour which was also captured with an external camera. Data acquisition was performed with the eDacq (EMMS, Hants, UK) acquisition software.
Protocol
One week following screening, guinea pigs in the treatment groups were injected with either 1 ml of vehicle or 3 mg/kg V112220 intra-peritoneally (i.p.) 1 hour before cough response assessment. Each guinea pig received 0.1 mg/kg procaterol hydrochloride i.p. injection 10 minutes prior to each cough assessment in order to minimise bronchoconstriction. For cough assessment, animals were exposed to 0.4 M citric acid for 10 min and a 10 min cough response was recorded. Two hours following citric acid inhalation, the same animal was exposed to 10-4 M Capsaicin for 10 min and the cough response was assessed.
Data analysis
Data were recorded as number of coughs per 10 min assessment. Cough numbers of individual animal were compared among pre-screening, following citric acid inhalation and following capsaicin inhalation. Data from the treatment groups were compared with the control group. Mean values were statistically analyzed by one-way analysis of variance (ANOVA) to evaluate significant differences between groups. Values are expressed as means and 95%CI, with p < 0.05 being considered significant.
Results
Pre-screening of animals
Guinea-pigs (n = 24) were pre-screened regarding their cough response with citric acid. Ten guinea-pigs (8 low and 2 high cough responders) were excluded and subsequently, fourteen guinea-pigs were divided into 3 groups. No significant difference in baseline cough response was noted among the 3 groups of guinea pigs. Figure 1 shows the number of coughs in the 3 different groups for each guinea-pig and the number of coughs following exposure to citric acid and capsaicin at a later date either after no treatment (control) or after vehicle or after V112220 treatment.

Number of coughs per 10 min in conscious guinea-pigs on pre-screen, following exposure to citric acid and to capsaicin. Left panel shows the response in the control group, the central panel the response from vehicle-treated group, and the right panel the effect of treatment with V112220.
Effect of V112220
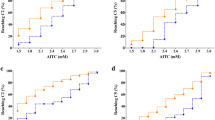
Figure 2 shows the mean cough number with 95% CI for the 3 groups of guinea-pigs for control, vehicle- and V112220-treated group. Vehicle treatment did not significantly change the number of coughs induced by either citric acid or capsaicin exposure. V112220 treatment (mean ± SEM: 2.6 ± 1.1; -0.4 to 5.6 coughs/10 min, p < 0.01) significantly reduced the number of coughs induced by citric acid compared to vehicle treatment (9.6 ± 1.6; 5.2 to 14.0 cough/10 min). V112220 treatment (2.6 ± 0.8; 0.3 to 4.9 coughs/10 min, p < 0.05) also significantly decreased the number of coughs compared to vehicle treatment (8.6 ± 0.7; 6.7 to 10.5 cough/10 min) for capsaicin. V112220 reduced citric acid-induced cough response by 73 ± 11% compared to vehicle treatment whereas capsaicin-induced cough response was reduced by 70 ± 9.4%.

Number of coughs following citric acid or capsaicin exposure. Left panel show results from citric acid exposure while the right panel the results from capsaicin exposure. Data shown as mean ± 95% CI (*, ** p < 0.05 and 0.01 compared to vehicle treatment).
Discussion
Our study demonstrated that blockade of the TRPV-1 receptors with a selective inhibitor, V112220, which is a pyridazinylpiperazine derivative, effectively decreased by 70% coughs evoked by citric acid or capsaicin aerosol exposure in the guinea pig. This is in agreement with a previous study using the earlier TRPV-1 antagonist, capsazepine, which inhibited coughs induced by citric acid or capsaicin but not coughs induced by 7% hypertonic saline solution[12]. In addition, there have been other studies with other TRPV-1 antagonists such as iodo-resiniferatoxin and BCTC that have shown inhibition of cough induced by citric acid and capsaicin in the guinea-pig [14, 15].
Recently, 4-(2-pyridyl)piperazine-1-carboxamide analogues as potent TRPV-1 antagonists have been developed [19]. N-(4-tertiarybutylphenyl)-4-(3-chloropyridin-2-yl)tetrahydropyrazine-1(2H)-carboxamide (BCTC), a member of that new chemical series, was a highly potent TRPV-1 antagonist that effectively reverses the behavioral effects of inflammatory and neuropathic pain in rats [16, 17, 19] but is poor in metabolic stability, short half-life, aqueous solubility, and in oral bioavailability [18]. Nevertheless, BCTC when administered intraperitoneally (30 mg/kg) one hour before capsaicin cough challenge caused an inhibition of capsaicin cough by 65% maximally [15]. A newer series of pyridazinylpiperazine compounds with improved pharmaceutical and pharmacological properties of BCTC was developed leading to V112220 which we used in this study. V112220 is similar to V113886, another pyridazinylpiperazine derivative of BCTC [18]. The plasma half-life of this compound after administration intravenously or by gavage is reported to be around 6 hours in the rat [18]. For this reason, we performed capsaicin challenge after citric acid challenge on the basis that the compound would still maintain significant plasma levels for many hours after dosing. The degree of inhibition of capsaicin- and citric acid-cough by V112220 we observed was similar with 70% reduction of the induced cough. However, capsaicin- and citric acid-cough were not completely inhibited by V112220. The incomplete inhibition, particularly of capsaicin-induced cough may indicate that higher dose of V112220 may be needed for complete inhibition, since cough response induced by capsaicin is presumed to be entirely mediated by TRPV-1. However, further studies with higher doses will be needed to answer this issue.
TRPV1 is sensitive to vanilloid molecules, including capsaicin. It can be activated by low extracellular pH [2, 6, 20, 21], and by the endocannabionid, anandamide [22], lipoxygenase metabolites [23] and N-arachidonoyl-dopamine [24], and also by a change in temperature [25]. TRPV1 is highly expressed in a subset of primary sensory neurons of the trigeminal, vagal and dorsal root ganglia with C- and A-δ fibres [9]. These receptors are polymodal nociceptors. TRPV1 excites terminals of primary sensory neurons and causes the initiation of action potentials of reflex responses, such as cough in airways [26]. It may also cause a series of neurogenic inflammation via antidromic conduction of action potential to collateral nerve fibres [26]. Capsaicin is one of the most tussigenic stimuli available in conscious animals and humans, and TRPV1 has been identified as a possible component of the cough receptor in guinea pigs and humans [27]. Inflammatory stimuli such as prostaglandins, bradykinin, and nerve growth factor may upregulate the expression and function of TRPV-1 [28–30]. Chronic airway inflammation such as in asthma or COPD may increase the sensitivity of TRPV-1 to its agonists and trigger the cough reflex [27]. The expression of TRPV-1 in the epithelial airway nerves of patients with chronic persistent cough of diverse causes and with an enhanced capsaicin cough response has a 3-fold increase of TRPV-1 expression [7]. TRPV-1 receptors may therefore contribute to the enhanced cough reflex and the cough response in chronic persistent cough
Chronic persistent cough is a clinical problem, since antitussives available to control cough are often not effective [31]. More potent antitussives are needed. TRPV-1 antagonists may represent a potential class of antitussives that could be useful in the control of chronic persistent cough.
References
Caterina MJ, Julius D: The vanilloid receptor: a molecular gateway to the pain pathway. Annu Rev Neurosci. 2001, 24: 487-517. 10.1146/annurev.neuro.24.1.487.
Tominaga M, Caterina MJ, Malmberg AB, Rosen TA, Gilbert H, Skinner K, Raumann BE, Basbaum AI, Julius D: The cloned capsaicin receptor integrates multiple pain-producing stimuli. Neuron. 1998, 21: 531-543. 10.1016/S0896-6273(00)80564-4.
Zygmunt PM, Chuang H, Movahed P, Julius D, Hogestatt ED: The anandamide transport inhibitor AM404 activates vanilloid receptors. Eur J Pharmacol. 2000, 396: 39-42. 10.1016/S0014-2999(00)00207-7.
Premkumar LS, Ahern GP: Induction of vanilloid receptor channel activity by protein kinase C. Nature. 2000, 408: 985-990. 10.1038/35050121.
Kollarik M, Undem BJ: Activation of bronchopulmonary vagal afferent nerves with bradykinin, acid and vanilloid receptor agonists in wild-type and TRPV1-/- mice. J Physiol. 2004, 555: 115-123. 10.1113/jphysiol.2003.054890.
Kollarik M, Ru F, Undem BJ: Acid-sensitive vagal sensory pathways and cough. Pulm Pharmacol Ther. 2007, 20: 402-411. 10.1016/j.pupt.2006.11.010.
Groneberg DA, Niimi A, Dinh QT, Cosio B, Hew M, Fischer A, Chung KF: Increased expression of transient receptor potential vanilloid-1 in airway nerves of chronic cough. Am J Respir Crit Care Med. 2004, 170: 1276-1280. 10.1164/rccm.200402-174OC.
Watanabe N, Horie S, Michael GJ, Spina D, Page CP, Priestley JV: Immunohistochemical localization of vanilloid receptor subtype 1 (TRPV1) in the guinea pig respiratory system. Pulm Pharmacol Ther. 2005, 18: 187-197. 10.1016/j.pupt.2004.12.002.
Kollarik M, Undem BJ: Sensory transduction in cough-associated nerves. Respir Physiol Neurobiol. 2006, 152: 243-254.
Chung KF: Drugs to suppress cough. Expert Opin Investig Drugs. 2005, 14: 19-27. 10.1517/13543784.14.1.19.
Bevan S, Hothi S, Hughes G, James IF, Rang HP, Shah K, Walpole CS, Yeats JC: Capsazepine: a competitive antagonist of the sensory neurone excitant capsaicin. Br J Pharmacol. 1992, 107: 544-552.
Lalloo UG, Fox AJ, Belvisi MG, Chung KF, Barnes PJ: Capsazepine inhibits cough induced by capsaicin and citric acid but not by hypertonic saline in guinea pigs. J Appl Physiol. 1995, 79: 1082-1087.
Mazzone SB, Mori N, Canning BJ: Synergistic interactions between airway afferent nerve subtypes regulating the cough reflex in guinea-pigs. J Physiol (Lond). 2005, 569: 559-573. 10.1113/jphysiol.2005.093153.
Trevisani M, Milan A, Gatti R, Zanasi A, Harrison S, Fontana G, Morice AH, Geppetti P: Antitussive activity of iodo-resiniferatoxin in guinea pigs. Thorax. 2004, 59: 769-772. 10.1136/thx.2003.012930.
McLeod RL, Fernandez X, Correll CC, Phelps TP, Jia Y, Wang X, Hey JA: TRPV1 antagonists attenuate antigen-provoked cough in ovalbumin sensitized guinea pigs. Cough. 2006, 2: 10-10.1186/1745-9974-2-10.
Valenzano KJ, Grant ER, Wu G, Hachicha M, Schmid L, Tafesse L, Sun Q, Rotshteyn Y, Francis J, Limberis J, Malik S, Whittemore ER, Hodges D: N-(4-tertiarybutylphenyl)-4-(3-chloropyridin-2-yl)tetrahydropyrazine -1(2H)-carbox-amide (BCTC), a novel, orally effective vanilloid receptor 1 antagonist with analgesic properties: I. in vitro characterization and pharmacokinetic properties. J Pharmacol Exp Ther. 2003, 306: 377-386. 10.1124/jpet.102.045674.
Pomonis JD, Harrison JE, Mark L, Bristol DR, Valenzano KJ, Walker K: N-(4-Tertiarybutylphenyl)-4-(3-cholorphyridin-2-yl)tetrahydropyrazine -1(2H)-carbox-amide (BCTC), a novel, orally effective vanilloid receptor 1 antagonist with analgesic properties: II. in vivo characterization in rat models of inflammatory and neuropathic pain. J Pharmacol Exp Ther. 2003, 306: 387-393. 10.1124/jpet.102.046268.
Tafesse L, Sun Q, Schmid L, Valenzano KJ, Rotshteyn Y, Su X, Kyle DJ: Synthesis and evaluation of pyridazinylpiperazines as vanilloid receptor 1 antagonists. Bioorg Med Chem Lett. 2004, 14: 5513-5519. 10.1016/j.bmcl.2004.09.010.
Sun Q, Tafesse L, Islam K, Zhou X, Victory SF, Zhang C, Hachicha M, Schmid LA, Patel A, Rotshteyn Y, Valenzano KJ, Kyle DJ: 4-(2-pyridyl)piperazine-1-carboxamides: potent vanilloid receptor 1 antagonists. Bioorg Med Chem Lett. 2003, 13: 3611-3616. 10.1016/S0960-894X(03)00759-5.
Bevan S, Geppetti P: Protons: small stimulants of capsaicin-sensitive sensory nerves. Trends Neurosci. 1994, 17: 509-512. 10.1016/0166-2236(94)90149-X.
Geppetti P, Del Bianco E, Patacchini R, Santicioli P, Maggi CA, Tramontana M: Low pH-induced release of calcitonin gene-related peptide from capsaicin-sensitive sensory nerves: mechanism of action and biological response. Neuroscience. 1991, 41: 295-301. 10.1016/0306-4522(91)90218-D.
Zygmunt PM, Petersson J, Andersson DA, Chuang H, Sorgard M, Di M, Julius D, Hogestatt ED: Vanilloid receptors on sensory nerves mediate the vasodilator action of anandamide. Nature. 1999, 400: 452-457. 10.1038/22761.
Hwang SW, Cho H, Kwak J, Lee SY, Kang CJ, Jung J, Cho S, Min KH, Suh YG, Kim D, Oh U: Direct activation of capsaicin receptors by products of lipoxygenases: endogenous capsaicin-like substances. Proc Natl Acad Sci U S A. 2000, 97: 6155-6160. 10.1073/pnas.97.11.6155.
Huang SM, Bisogno T, Trevisani M, Al Hayani A, De Petrocellis L, Fezza F, Tognetto M, Petros TJ, Krey JF, Chu CJ, Miller JD, Davies SN, Geppetti P, Walker JM, Di M: An endogenous capsaicin-like substance with high potency at recombinant and native vanilloid VR1 receptors. Proc Natl Acad Sci U S A. 2002, 99: 8400-8405. 10.1073/pnas.122196999.
Caterina MJ, Schumacher MA, Tominaga M, Rosen TA, Levine JD, Julius D: The capsaicin receptor: a heat-activated ion channel in the pain pathway. Nature. 1997, 389: 816-824. 10.1038/39807.
Geppetti P, Materazzi S, Nicoletti P: The transient receptor potential vanilloid 1: role in airway inflammation and disease. Eur J Pharmacol. 2006, 533: 207-214. 10.1016/j.ejphar.2005.12.063.
Morice AH, Geppetti P: Cough {middle dot} 5: The type 1 vanilloid receptor: a sensory receptor for cough. Thorax. 2004, 59: 257-258. 10.1136/thx.2003.013482.
Chuang HH, Prescott ED, Kong H, Shields S, Jordt SE, Basbaum AI, Chao MV, Julius D: Bradykinin and nerve growth factor release the capsaicin receptor from PtdIns(4,5)P2-mediated inhibition. Nature. 2001, 411: 957-962. 10.1038/35082088.
De Petrocellis L, Harrison S, Bisogno T, Tognetto M, Brandi I, Smith GD, Creminon C, Davis JB, Geppetti P, Di M: The vanilloid receptor (VR1)-mediated effects of anandamide are potently enhanced by the cAMP-dependent protein kinase. J Neurochem. 2001, 77: 1660-1663. 10.1046/j.1471-4159.2001.00406.x.
Ji RR, Samad TA, Jin SX, Schmoll R, Woolf CJ: p38 MAPK activation by NGF in primary sensory neurons after inflammation increases TRPV1 levels and maintains heat hyperalgesia. Neuron. 2002, 36: 57-68. 10.1016/S0896-6273(02)00908-X.
Chung KF: Assessment and measurement of cough: the value of new tools. Pulm Pharmacol Ther. 2002, 15: 267-272. 10.1006/pupt.2002.0360.
Acknowledgements
We are grateful to Purdue Pharma (Ardsley, New York) for supplying the selective TRPV1 antagonist, V112220. We thank EMMS (Hants, UK) for technical assistance on cough measurement. FXB was the recipient of a travel grant from the French Société de Pneumologie de Langue Française and from the Chancellerie des Universités de Paris (legs Poix).
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors' contributions
SYL carried out the drugs administration and cough measurements, and performed the statistical analysis. AN helped in the design of the study. ASW & PN participated in animal maintenance. F-XB & QTD assisted in cough measurement, and drugs preparation. KFC conceived of the study, and participated in its coordination. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Leung, S.Y., Niimi, A., Williams, A.S. et al. Inhibition of citric acid- and capsaicin-induced cough by novel TRPV-1 antagonist, V112220, in guinea-pig. Cough 3, 10 (2007). https://doi.org/10.1186/1745-9974-3-10
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1745-9974-3-10