
Abstract
Background
Interferon-gamma release assays (IGRAs) are increasingly used in the tuberculosis (TB) screening of health care workers (HCWs). However, comparatively high rates of conversions and reversion as well as growing evidence of substantial within-subject variability of interferon-gamma responses complicate their interpretation in the serial testing of HCWs.
Methods
We conducted a systematic review on the repeat use of the two commercial IGRAs, the QuantiFERON-TB Gold or In-Tube version (QFT) and the T-SPOT.TB (T-SPOT), in the serial testing and its with-subject variability among HCWs in order to provide guidance on how to interpret serial testing results in the context of the periodic screening of subjects with an increased occupational risk of latent TB infection (LTBI) in countries with low and intermediate TB incidence rates. The Medline, Embase, and Cochrane databases were searched without restrictions. Retrieved articles were complemented by additional hand searched records. Only studies that used commercial IGRAs among HCWs apart from contact and outbreak investigations and those fulfilling further predefined criteria were included.
Results
Overall, 20 studies, five using the T-SPOT and 19 using the QFT assay, were included. Fifteen studies met eligibility criteria for serial testing and five studies for within-subject variability. Irrespective of TB incidence rates in the study’s country of origin, reversion rates were consistently higher than conversion rates (range 22–71% vs. 1–14%). Subjects with baseline results around the diagnostic threshold were more likely to show inconsistent results on retesting. The within-subject variability of interferon-gamma responses was considerable across all studies systematically assessing it.
Conclusions
On the basis of reviewed studies we advocate using a borderline zone from 0.2–0.7 IU/ml for the interpretation of repeat QFT results in the routine screening of HCWs with an increased LTBI risk. Subjects with QFT results within this borderline zone, with suspected fresh infection, and those who are considered for preventive chemotherapy should be retested with the QFT within a period of about four weeks before preventive chemotherapy is recommended. However, the available data regarding the use of the T-SPOT in the serial testing of HCWs is remarkably limited and warrants further research.
Similar content being viewed by others

Background
Health care workers (HCWs) may have an increased risk of occupational tuberculosis (TB) infection due to possible nosocomial exposure [1–4]. Therefore, exposed HCWs are subject to periodic TB screening with a view to identifying infection at an early stage and preventing the development of active TB by means of preventive chemotherapy [5, 6]. In the absence of clinical evidence of active TB, latent TB infection (LTBI) is understood by current consensus to be proven by a Mycobacterium tuberculosis-specific T-cell-mediated adaptive immune response, either by a positive tuberculin skin test (TST) or a positive interferon-γ release assay (IGRA) [7]. However, that does not necessarily have to mean that live and augmentable mycobacteria exist. In Germany, section 4 of the regulation on occupational safety and health (OSH) prescribes regular compulsory screening of employees in infectious diseases, respiratory medicine, and in laboratories insofar as they come into regular contact with people suffering or suspected of suffering from TB, or possibly coming into contact with infectious or contaminated material [8]. Usually, these OSH screenings are performed at one-year to three-year intervals. In addition to identifying LTBI as an irregular physical condition by the terms of OSH legislation, these screenings are aimed at establishing the rate of new TB infections as a measure of the effectiveness of the preventive measures implemented and at reducing the risk of a HCW to develop active TB, e.g. by prescribing preventive chemotherapy.
Despite its known limitations, in particular its cross-reactivity after vaccination with the attenuated Mycobacterium bovis live strain of bacillus Calmette-Guérin (BCG) and infection with nontuberculous mycobacteria, the TST, which is more than 100 years old, has been the only way to diagnose LTBI for decades [9, 10]. Its use in serial testing is complicated by sensitization as a result of repeated use (the so-called “boosting” phenomenon) [11]. In this respect the two IGRAs, the QuantiFERON-TB Gold and In-Tube version (QFT) and T-SPOT.TB (T-SPOT), which have been commercially available for a number of years, offer distinct advantages. They have now established as alternatives to the TST [12]. IGRAs are ex-vivo blood tests that avoid the sensitization of the immune system to mycobacterial antigens in serial testing (“boosting”). Even among BCG-vaccinated HCWs, IGRAs have a high specificity and correlate well to the occupational risk of TB exposure [13–15]. They also possess certain logistical advantages over the TST in that a second appointment to read the result is no longer required.
However, IGRAs are also subject to a certain biological and technical variability. Thus, they must be considered as dynamic tests [14, 16, 17]. Different borderline zones (“gray zones”) have been proposed for defining “genuine” conversions and reversions in order to improve the interpretation of test results as part of IGRA serial testing [12, 17–21]. As there is no gold standard for diagnosing LTBI, the definition of an appropriate borderline zone is challenging and an issue of ongoing scientific debate. Data on the prediction of active TB after conversion, reversion, or persistently positive IGRA results may help to determine these borderline zones, but this data is not readily available [22].
We performed a systematic review on the repeat use of commercial IGRAs among HCWs, either in serial testing studies or in studies on the within-subject variability of interferon-(IFN)-γ responses (as determined by commercial IGRAs), in order to inform policies and practices related to the TB serial testing of HCWs in countries with low and intermediate TB incidence rates.
Methods
Search strategy, study selection, and eligibility
This systematic review was conducted according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement [23]. We searched the Medline, Embase, and Cochrane databases without restrictions regarding language or study design though 15 Mar 2012. The following search string was used: ("Tuberculosis" OR "TB infection") AND ("interferon-gamma" OR “gamma-interferon” OR "interferon" OR “interferon-gamma release assay” OR “IGRA” OR "Quantiferon" OR "T-SPOT") AND ("health care workers" OR "healthcare workers" OR "health-care workers" OR "health personnel"). In addition reference lists, citations of previous reviews, and abstracts from conference proceedings were hand searched. In case of doubt authors of original studies were contacted to obtain additional information. Only original studies (research articles or letters containing original data) among HCWs or those containing a significant proportion of HCWs (> 50% of the study population) that were conducted apart from (cross-sectional) LTBI prevalence, contact tracing, or outbreak investigations and repeatedly used one of the two or both commercially available IGRAs on the same group of subjects (at least twice with the same assay; longitudinal or serial testing design) were considered eligible. Case reports, case series, comments, editorials, reviews, cost effectiveness analyses, studies not following the manufacturers’ instructions (e.g. studies using prolonged incubation or freezing of cells), and studies involving less than 10 subjects or any kind of therapeutic intervention such as treatment for LTBI or active TB (i.e. studies using an IGRA for the monitoring of treatment response) were excluded.
For an optimal assessment of the behavior of IGRAs in serial testing, these studies had to be performed among HCWs with a low or intermediate occupational TB risk, i.e. not in a context of point source exposure and not within a TB contact or outbreak investigation, and with a follow-up for repeat IGRA testing of at least four weeks. In principle, the same preconditions applied to studies on the within-subject variability of IFN-γ responses as determined by commercial IGRAs. The risk of exposure to TB in the course of the study is particularly important for the results of any such study. Those studies performed in countries with an intermediate or high incidence of TB should therefore have been conducted over as short a period as possible (less than four weeks) in order to avoid conversions due to fresh TB infection. Furthermore, consistent, well defined, and controlled or controlled-modified test conditions should have been applied and additional quality assurance measures should have been implemented. Studies with subjects who have had a TST within the past three months were explicitly excluded due to evidence that a recent TST may influence IGRA results by the “boosting” of IFN-γ responses. Apparently, this applies if sensitization to mycobacterial antigens preexists [20, 24, 25].
Data extraction, data analysis, and quality assessment
Two reviewers (AS and FCR) independently assessed articles for eligibility. Disagreement was resolved by consensus. Data extraction was performed using a data extraction form by one reviewer (FCR) and confirmed by a second reviewer (AS). In serial testing studies the outcomes of interest were: recruitment period, country and epidemiological setting of the study according to the World Health Organization (WHO) [26], IGRA(s) used, interval(s) between repeat IGRA testing, number of included subjects, rate of positive results at baseline, rate of reversions, and rate of conversions. In studies on the IGRA within-subject variability the outcomes of interest were: country and epidemiological setting of the study according to the WHO, IGRA(s) used, number of included subjects and total number of tests conducted, time points at which IGRAs were performed, and results with respect to the observed IGRA within-subject variability.
Weighted mean incidence rates were calculated for reversions and conversions. The completeness of reported outcome parameters, the reporting of quantitative follow-up IGRA results stratified according to the quantitative baseline results, and a prospective study design were considered as quality indicators. Due to the apparent heterogeneity of study designs and study quality, time intervals between repeat IGRAs, included study populations, epidemiological settings, and the applied assays, performing pooled analysis (meta-analysis) was considered inappropriate.
Results
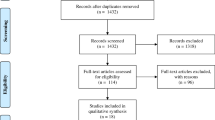
Figure 1 summarizes the process of study selection. Finally, after excluding two full-text articles that had been assessed for eligibility in detail [27, 28], 20 studies were included in the review. Of those, 15 studies met eligibility criteria for the serial testing analysis [17, 29–42], while 5 studies met eligibility criteria for the within-subject variability analysis [20, 21, 24, 43, 44].

Flow diagram for study selection. Abbreviation: IGRA = interferon-γ release assay.
Studies on IGRA serial testing
Table 1 provides an overview of publications to date on the serial testing of HCWs using commercial IGRAs by the incidence of TB in the study’s country of origin and summarizes their most important characteristics and results. Overall, these studies included 6605 subjects. Reversion rates ranged from 22.1 to 71.4%, while conversion rates ranged from 0.7 to 14.4%. The weighted mean incidence rate of QFT reversions based on 3849 subjects from 9 studies from countries with low and intermediate TB incidence rates [30, 33–35, 37–40, 42] was 33.6% (95% confidence interval 29.6 – 37.7). The weighted mean incidence rate of QFT conversions based on 6072 subjects from 12 studies from countries with low and intermediate TB incidence rates [29, 30, 32–34, 36–42] was 5.1% (95% confidence interval 4.5 – 5.7). The number of subjects included in the two studies using the T-SPOT assay was comparatively low (overall 1463 subjects) [31, 34]. Only one study reported the reversion rate for the T-SPOT [34]. Based on their retrospective study design [35, 41] and the incompleteness of data reporting [29, 31–34, 36] eight studies were considered to be of minor quality, while seven studies were considered to be of superior quality [17, 30, 37–40, 42].
Even though the included serial testing studies differed substantially in their design and epidemiological setting, what they all had in common is that inconsistent IGRA serial testing results (conversions and reversions) occurred fairly frequently and that even in countries with an intermediate or high incidence of TB, reversions of positive IGRA results were observed more frequently than conversions of negative results ( 1). Moreover, in studies reporting (stratified) quantitative QFT results, the likelihood of conversions and reversions of QFT results increased in subjects with initial test results close to the diagnostic threshold, generally within a borderline zone between 0.2 to 0.7 IU/ml [37–42]. However, published serial testing studies reporting quantitative T-SPOT results for analysis were unavailable within the searched databases.
Studies on the within-subject variability of the IFN-γ response
So far, there were only few well-conceived studies that have investigated the (biological) within-subject variability or the influence of technical issues on the reproducibility of the Mycobacterium tuberculosis-specific IFN-γ response [20, 21, 24, 43, 44]. Table 2 summarizes the studies on the within-subject variability of IFN-γ responses that have been published to date and that met the eligibility criteria mentioned above. However, the number of subjects tested in the available studies was low (overall 219 subjects) and ranged from 14 to 117 subjects. These studies were carried out almost exclusively on HCWs. Remarkably, studies from countries with a low incidence of TB [24, 39, 44] as well as studies comparing the two commercially available IGRAs [20, 24, 44] have rarely been published. Differences in the statistical assessment of within-subject variability handicap comparability (Table 2), but what all the above-mentioned studies had in common was that the amount of observed within-subject variability was considerable and, again, that conversions or reversions of IGRA results were more likely to be found if the initial test result was close to the diagnostic cut-off [20, 21, 24, 43, 44].
Discussion
Despite the remarkable amount of publications on the two commercially available IGRAs, their implementation in recommendations and guidelines [5, 12, 45–49], and their widespread use in daily clinical practice, only a few studies have been published to date on their use in the serial testing of HCWs [17, 29–42] and on their within-subject variability [20, 21, 24, 43, 44]. Two other recently published systematic reviews identified a mere ten original studies on serial testing and four on within-subject variability that corresponded to previously defined selection criteria and quality indicators [15, 25]. The medical literature available suggests that conversions and reversions occurring in IGRA serial testing are due to the considerable biological (within-subject) and technical variability of the IFN-γ response. The test manufacturers’ dichotomous cut-off values seem to be only partly appropriate for the interpretation of repeat IGRA results. A current review by Zwerling and colleagues on the TB screening of HCWs using IGRAs found existing data to be insufficient to make a general recommendation regarding their use instead of the TST in serial testing [15]. However, in our own experience, in a country with a low incidence of TB and a high BCG vaccination coverage the use of an IGRA instead of the TST may safely reduce the prevalence of positive test results and thereby the number of HCWs who require a chest X-ray to rule out active TB [50].
Torres Costa and colleagues, who in Portugal carried out repeat testing of the largest European cohort of HCWs to date, found a close relation between the IFN-γ response of initial and follow-up QFT results. QFT results in a borderline zone between 0.2 and 0.7 IU/ml had, when the test was repeated, undergone an especially frequent qualitative change (i.e. a change from a negative to a positive result and vice versa; 49.0% vs. 8.7% of subjects with a QFT result of < 0.2 or > 0.7 IU/ml) [40]. Furthermore, their study also revealed that using a borderline zone between 0.2 und 0.7 IU/ml could reduce the rate of QFT conversions and reversions significantly and safely. The conversion rate was reduced from 11.0% to 3.6% and the reversion rate from 22.1% to 5.2%. This observation is in accordance with the findings of two current studies of German HCWs by our own working group. Using this borderline zone, the conversion rates were reduced from 1.9% to 0.6% and from 6.1% to 2.6% and the reversion rates from 33.3% to 16.7% and from 32.6% to 15.4%, respectively [37, 38]. No cases of active TB occurred during the follow-up period of more than two years. In one of the two studies in which 182 HCWs underwent repeat QFT tests we were able to show that along with increasing age and the extent of the initial IFN-γ response, a positive TST both in the past and at the time of the current evaluation was a significant predictor of a persistently positive IFN-γ response in serial testing [37]. These findings have largely been confirmed by a recent study by Gandra and colleagues in another low TB incidence country (USA) [35].
In a further recent study of our own we showed that the within-subject variability of the IFN-γ response of both IGRAs in middle-aged HCWs (mean 42 ± 10.5 years old) with a low to intermediate risk of TB exposure over a period of four weeks was quite considerable [44]. Changes in mean IFN-γ response of about ± 70% (QFT) and ± 60% (T-SPOT) accounted for 95% of the within-subject variability. With dichotomous interpretation of test results, inconsistent results occurred with significantly greater frequency with the QFT (29%) than with the T-SPOT (9%; p < 0.001). The statistical phenomenon of regression towards the means led to a significant reduction in the mean IFN-γ response of both IGRAs by about −25% from week to week. Applying borderline zones between 0.2 to 0.7 IU/ml (QFT) and between 4 to 8 spot-forming cells (SFCs; T-SPOT) reduced primarily the rate of QFT reversions (from 50% to 17%). These results are comparable with those of a South African study in which changes of ± 80% (QFT) and ± 3 SFCs (T-SPOT) were responsible for 95% of the within-subject variability ( 2) [20]. Discordant results for the two IGRAs occurred in a total of 9% (8/88) of subjects and were thus similar in frequency to our own findings (13%, 20/158 subjects) [20, 44]. The three studies conducted in countries with a high TB incidence (India, South Africa) can only to a limited extent be compared with studies conducted in TB low incidence countries (Germany, USA), because they included only a small number of subjects with IGRA results close to the diagnostic threshold and had high overall rates of positive IGRA results of between 40% and 57% and large maximum individual variation ranges of the absolute IFN-γ response (8.41 to 11.11 IU/ml for the QFT) [20, 21, 43].
Another study by our own working group investigated the specificity and the negative predictive value of the QFT among trainee nurses and HCWs. The average age of study participants was 23 ± 5.8 years. In this cohort with a very low risk of previous TB exposure there was, with respect to the qualitative findings, only a low within-subject variability of IFN-γ responses over a one-year period. Out of a total of 154 subjects who underwent a repeat test, two were positive in the first test. One of the two remained positive in the second test, whereas the other showed a reversion. Of the 152 trainees who were negative in the first test, 151 had consistently negative QFT results (99%). The one subject with a conversion showed an increase in IFN-γ concentration from 0.01 to 0.67 IU/ml. Applying the borderline zone from 0.2 to 0.7 IU/ml, this increase would not be counted as a conversion. This individual had no TB infection risk. Overall, the quantitative results were mainly stable at < 0.1 IU/ml and emphasized the high specificity of the QFT in this young cohort with a low risk of TB exposure. None of the trainees developed TB during the two-year observational period, indicating a negative predictive value of 100% among this population.
In summary, IGRA reversions have been observed more frequently than conversions in serial testing studies. A possible explanation for this observation could be the frequently inevitable statistical phenomenon of regression towards the means, which occurs wherever repeat measurements are performed of the same individual with a random measurement error, i.e. with an unsystematic spread around a true mean [51]. Taking this phenomenon into account is especially important if subjects are categorized or stratified on the basis of certain initial measurements, e.g. if the effect of a therapy or the incidence of a disease is estimated on the basis of repeat measurements of surrogate parameters. As the effect of regression towards the means increases in proportion to the variability of the method employed it can be reduced by increasing the number of independent initial measurements, i.e. by an approximation to the “true” mean. However, this approach will rarely be applicable in practice. Hence, the definition of a borderline zone for the interpretation of serial measurements is an appropriate alternative.
Our review is subject to limitations. The number of eligible and accessible studies as well as their quality and the number of included subjects were limited. Furthermore, we did not systematically assess risk factors for conversion, reversion, or persistent positivity of IGRA responses, which recently have been reported in detail somewhere else [15].
Finally, it should be emphasized that even a negative IGRA result can never rule out either active TB or LTBI with absolute certainty. Moreover, clinical information on the individual risk of exposure and the susceptibility to TB along with recent or previous TST or IGRA results should always be taken into account in the overall context. The safety of a borderline zone for the interpretation of IGRA serial results with regard to the progression toward active TB may not be inferred from studies on within-subject variability because these studies generally cover a limited follow-up period. Further studies on large cohorts of HCWs with sufficiently long follow-up periods of more than two years are required to define more precisely the prognosis of conversions, reversions, and persistently positive IGRA results.
Conclusion
So far, the published studies on IGRA serial testing and on the within-subject variability of the IFN-γ response among HCWs in countries with a low or intermediate incidence of TB demonstrate convincingly that subjects with a QFT result in a borderline zone between 0.2 to 0.7 IU/ml are significantly more likely to show an inconsistent result on retesting [37–40, 42, 44]. Furthermore, applying this borderline zone to the interpretation of QFT results in the serial testing of German HCWs appears to be safe because none of the 623 HCWs in our own studies developed active TB in the follow-up period of more than two years [37–39]. According to the current literature, the experience regarding the use of the T-SPOT in the serial testing and its within-subject variability among HCWs is remarkably limited. The borderline zone of 4 to 8 SFCs propagated for the T-SPOT and following the US regulatory authority FDA (5 to 7 SFCs) is based mainly on a single published study and must be considered to be not yet sufficiently substantiated by scientific evidence, especially as the study by van Zyl-Smit et al. covered a follow-up observation period of only six months [20].
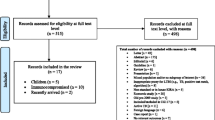
Hence, in view of the available data on the within-subject variability of the IFN-γ response and the use of IGRAs in the serial testing of HCWs in countries with low and intermediate incidences of TB, we recommend using a borderline zone from 0.2 to 0.7 IU/ml for the interpretation of repeat QFT results in routine screening of HCWs with an increased LTBI risk (Figure 2). Subjects with QFT results within this borderline zone, with suspected fresh infection due to their risk of TB exposure, and who are considered for preventive chemotherapy should be retested with the QFT within a period of about four weeks before preventive chemotherapy is recommended. If a HCW with a previously positive IGRA is to be retested in accordance with OSH regulations, repeating the IGRA appears appropriate. Only if repeat IGRA testing has demonstrated that the HCW remains persistently IGRA-positive with accordingly high IFN-γ responses should they be x-rayed immediately at their next TB screening in order to rule out active disease.

Proposed flow chart for the interpretation of repeat QFT results in the serial testing of health care workers in countries with low or intermediate TB incidence rates. Abbreviations: QFT = QuantiFERON-TB Gold In-Tube; TB = tuberculosis.
Abbreviations
- BCG :
-
Bacillus Calmette-Guérin
- HCW(s) :
-
Health care worker(s)
- IFN-γ :
-
Interferon-γ
- IGRA(s) :
-
Interferon-γ release assay(s)
- LTBI :
-
Latent tuberculosis infection
- OSH :
-
Occupational safety and health
- QFT :
-
QuantiFERON-TB Gold In-Tube
- SFCs :
-
Spot-forming cells
- TB :
-
Tuberculosis
- T-SPOT :
-
T-SPOT.TB
- TST :
-
Tuberculin skin test
- WHO :
-
World Health Organization.
References
Diel R, Seidler A, Nienhaus A, Rusch-Gerdes S, Niemann S: Occupational risk of tuberculosis transmission in a low incidence area. Respir Res 2005, 6: 35. 10.1186/1465-9921-6-35
Menzies D, Joshi R, Pai M: Risk of tuberculosis infection and disease associated with work in health care settings. Int J Tuberc Lung Dis 2007,11(6):593–605.
Schwartzman K, Menzies D: Tuberculosis: 11. Nosocomial disease. CMAJ 1999,161(10):1271–1277.
Seidler A, Nienhaus A, Diel R: Review of epidemiological studies on the occupational risk of tuberculosis in low-incidence areas. Respiration 2005,72(4):431–446. 10.1159/000086261
Centers for Disease Control and Prevention: Guidelines for preventing the transmission of Mycobacterium tuberculosis in health-care settings, 2005. MMWR Recomm Rep 2005,54(RR-17):1–141.
World Health Organization: WHO policy on TB infection control in health-care facilities, congregate settings and households. WHO, Geneva; 2009.
Mack U, Migliori GB, Sester M, Rieder HL, Ehlers S, Goletti D, Bossink A, Magdorf K, Holscher C, Kampmann B, et al.: LTBI: latent tuberculosis infection or lasting immune responses to M. tuberculosis? A TBNET consensus statement. Eur Respir J 2009,33(5):956–973. 10.1183/09031936.00120908
German Federal Ministry of Justice: Regulation on Occupational Safety and Health (issued 18 Dec 2008; last modified 26 Nov 2010) . German. Last accessed 15 Mar, 2012 http://www.gesetze-im-internet.de/arbmedvv/BJNR276810008.html
von Pirquet C: Frequency of tuberculosis in childhood. JAMA 1909, 52: 675–678.
Ringshausen FC: Tuberculosis contact investigation in health care. Südwestdeutscher Verlag für Hochschulschriften Aktiengesellschaft & Co. KG, Saarbrücken; 2010.
Menzies D: Interpretation of repeated tuberculin tests. Boosting, conversion, and reversion. Am J Respir Crit Care Med 1999,159(1):15–21.
Mazurek GH, Jereb J, Lobue P, Iademarco MF, Metchock B, Vernon A: Guidelines for using the QuantiFERON-TB Gold test for detecting Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep 2005,54(RR-15):49–55.
Diel R, Goletti D, Ferrara G, Bothamley G, Cirillo D, Kampmann B, Lange C, Losi M, Markova R, Migliori GB, et al.: Interferon-gamma release assays for the diagnosis of latent Mycobacterium tuberculosis infection: a systematic review and meta-analysis. Eur Respir J 2011,37(1):88–99. 10.1183/09031936.00115110
Pai M, Zwerling A, Menzies D: Systematic review: T-cell-based assays for the diagnosis of latent tuberculosis infection: an update. Ann Intern Med 2008,149(3):177–184.
Zwerling A, van den Hof S, Scholten J, Cobelens F, Menzies D, Pai M: Interferon-gamma release assays for tuberculosis screening of healthcare workers: a systematic review. Thorax 2012,67(1):62–70. 10.1136/thx.2010.143180
Andersen P, Doherty TM, Pai M, Weldingh K: The prognosis of latent tuberculosis: can disease be predicted? Trends Mol Med 2007,13(5):175–182. 10.1016/j.molmed.2007.03.004
Pai M, Joshi R, Dogra S, Mendiratta DK, Narang P, Kalantri S, Reingold AL, Colford JM, Riley LW, Menzies D: Serial testing of health care workers for tuberculosis using interferon-gamma assay. Am J Respir Crit Care Med 2006,174(3):349–355. 10.1164/rccm.200604-472OC
Pai M, Joshi R, Dogra S, Zwerling AA, Gajalakshmi D, Goswami K, Reddy MV, Kalantri A, Hill PC, Menzies D, et al.: T-cell assay conversions and reversions among household contacts of tuberculosis patients in rural India. Int J Tuberc Lung Dis 2009,13(1):84–92.
Perry S, Sanchez L, Yang S, Agarwal Z, Hurst P, Parsonnet J: Reproducibility of QuantiFERON-TB gold in-tube assay. Clin Vaccine Immunol 2008,15(3):425–432. 10.1128/CVI.00398-07
van Zyl-Smit RN, Pai M, Peprah K, Meldau R, Kieck J, Juritz J, Badri M, Zumla A, Sechi LA, Bateman ED, et al.: Within-subject variability and boosting of T-cell interferon-gamma responses after tuberculin skin testing. Am J Respir Crit Care Med 2009,180(1):49–58. 10.1164/rccm.200811-1704OC
Veerapathran A, Joshi R, Goswami K, Dogra S, Moodie EE, Reddy MV, Kalantri S, Schwartzman K, Behr MA, Menzies D, et al.: T-cell assays for tuberculosis infection: deriving cut-offs for conversions using reproducibility data. PLoS One 2008,3(3):e1850. 10.1371/journal.pone.0001850
Pai M: Spectrum of latent tuberculosis - existing tests cannot resolve the underlying phenotypes. Nat Rev Microbiol 2010,8(3):242.
Moher D, Liberati A, Tetzlaff J, Altman DG: Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009,6(7):e1000097. 10.1371/journal.pmed.1000097
Belknap R, Kelaher J, Wall K, Daley C, Schluger N, Reves R: Diagnosis of Latent Tuberculosis Infection in U.S. Health Care Workers: reproducibility, repeatability and 6 month follow-up with Interferon-gamma Release Assays (IGRAs). Am J Respir Crit Care Med 2009, 179: A4101.
van Zyl-Smit RN, Zwerling A, Dheda K, Pai M: Within-subject variability of interferon-g assay results for tuberculosis and boosting effect of tuberculin skin testing: a systematic review. PLoS One 2009,4(12):e8517. 10.1371/journal.pone.0008517
World Health Organization: WHO Global TB database. http://www.who.int/tb/country/global_tb_database/en/index2.html
Cummings KJ, Smith TS, Shogren ES, Khakoo R, Nanda S, Bunner L, Smithmyer A, Soccorsi D, Kashon ML, Mazurek GH, et al.: Prospective comparison of tuberculin skin test and QuantiFERON-TB Gold In-Tube assay for the detection of latent tuberculosis infection among healthcare workers in a low-incidence setting. Infect Control Hosp Epidemiol 2009,30(11):1123–1126. 10.1086/644754
Escombe AR, Huaroto L, Ticona E, Burgos M, Sanchez I, Carrasco L, Farfan E, Flores F, Moore DA: Tuberculosis transmission risk and infection control in a hospital emergency department in Lima, Peru. Int J Tuberc Lung Dis 2010,14(9):1120–1126.
Pollock NR, Campos-Neto A, Kashino S, Napolitano D, Behar SM, Shin D, Sloutsky A, Joshi S, Guillet J, Wong M, et al.: Discordant QuantiFERON-TB Gold test results among US healthcare workers with increased risk of latent tuberculosis infection: a problem or solution? Infect Control Hosp Epidemiol 2008,29(9):878–886. 10.1086/590262
Yoshiyama T, Harada N, Higuchi K, Nakajima Y, Ogata H: Estimation of incidence of tuberculosis infection in health-care workers using repeated interferon-gamma assays. Epidemiol Infect 2009,137(12):1691–1698. 10.1017/S0950268809002751
Chee CB, Lim LK, Barkham TM, Koh DR, Lam SO, Shen L, Wang YT: Use of a T cell interferon-gamma release assay to evaluate tuberculosis risk in newly qualified physicians in Singapore healthcare institutions. Infect Control Hosp Epidemiol 2009,30(9):870–875. 10.1086/599284
Lee K, Han MK, Choi HR, Choi CM, Oh YM, Lee SD, Kim WS, Kim DS, Woo JH, Shim TS: Annual incidence of latent tuberculosis infection among newly employed nurses at a tertiary care university hospital. Infect Control Hosp Epidemiol 2009,30(12):1218–1222. 10.1086/648082
Zwerling A, Cloutier Ladurantaye J, Pietrangelo F, Behr M, Schwartzman K, Dendukuri N, Menzies D, Pai M: Conversions and reversions in health care workers in montreal, Canada using QuantiFERON-TB-gold in-tube. Am J Respir Crit Care Med 2009, 179: A1012.
Belknap R, Wall K, Teeter L, Dorman S, Weinfurter P, Reves R, Daley CL: Interferon-gamma release assays (IGRAs) in serial testing for latent tuberculosis infection in U.S. health care workers. Am J Respir Crit Care Med 2010, 181: A2263.
Gandra S, Scott WS, Somaraju V, Wang H, Wilton S, Feigenbaum M: Questionable effectiveness of the QuantiFERON-TB Gold Test (Cellestis) as a screening tool in healthcare workers. Infect Control Hosp Epidemiol 2010,31(12):1279–1285. 10.1086/657336
Park HY, Jeon K, Suh GY, Kwon OJ, Chung DR, Yoonchang SW, Kang ES, Koh WJ: Interferon-gamma release assay for tuberculosis screening of healthcare workers at a Korean tertiary hospital. Scand J Infect Dis 2010,42(11–12):943–945.
Ringshausen FC, Nienhaus A, Schablon A, Schlosser S, Schultze-Werninghaus G, Rohde G: Predictors of persistently positive Mycobacterium-tuberculosis-specific interferon-gamma responses in the serial testing of health care workers. BMC Infect Dis 2010, 10: 220. 10.1186/1471-2334-10-220
Schablon A, Harling M, Diel R, Ringshausen FC, Torres Costa J, Nienhaus A: Serial testing with an interferon-gamma release assay in German healthcare workers. GMS Krankenhhyg Interdiszip 2010,5(2):pii: Doc05.
Schablon A, Diel R, Diner G, Anske U, Pankow W, Ringshausen FC, Nienhaus A: Specificity of a whole blood IGRA in German nursing students. BMC Infect Dis 2011, 11: 245. 10.1186/1471-2334-11-245
Torres Costa J, Silva R, Sa R, Cardoso MJ, Nienhaus A: Serial testing with the interferon-gamma release assay in Portuguese healthcare workers. Int Arch Occup Environ Health 2011,84(4):461–469. 10.1007/s00420-010-0571-x
Fong KS, Tomford JW, Teixeira L, Fraser TG, Vanduin D, Yen-Lieberman B, Gordon SM, Miranda C: Challenges of Interferon-gamma release assay conversions in serial testing of health care workers in a tuberculosis control program. Chest 2012. in press
Rafiza S, Rampal KG: Serial testing of Malaysian health care workers with QuantiFERON(R)-TB Gold In-Tube. Int J Tuberc Lung Dis 2012,16(2):163–168. 10.5588/ijtld.11.0364
Detjen AK, Loebenberg L, Grewal HM, Stanley K, Gutschmidt A, Kruger C, Du Plessis N, Kidd M, Beyers N, Walzl G, et al.: Short-term reproducibility of a commercial interferon gamma release assay. Clin Vaccine Immunol 2009,16(8):1170–1175. 10.1128/CVI.00168-09
Ringshausen FC, Nienhaus A, Torres Costa J, Knoop H, Schlosser S, Schultze-Werninghaus G, Rohde G: Within-subject variability of mycobacterium tuberculosis-specific gamma interferon responses in german health care workers. Clin Vaccine Immunol 2011,18(7):1176–1182. 10.1128/CVI.05058-11
Canadian Tuberculosis Committee (CTC): Updated recommendations on interferon gamma release assays for latent tuberculosis infection. An Advisory Committee Statement (ACS). Can Commun Dis Rep 2008,34(ACS-6):1–13.
Centers for Disease Control and Prevention: Guidelines for the investigation of contacts of persons with infectious tuberculosis; recommendations from the National Tuberculosis Controllers Association and CDC, and Guidelines for using the QuantiFERON®-TB Gold test for detecting Mycobacterium tuberculosis infection, United States. MMWR Recomm Rep 2005,54(RR-15):1–55.
Diel R, Forssbohm M, Loytved G, Haas W, Hauer B, Maffei D, Magdorf K, Nienhaus A, Rieder HL, Schaberg T, et al.: Recommendations for background studies in tuberculosis. Pneumologie 2007,61(7):440–455. 10.1055/s-2007-959219
European Centre for Disease Prevention and Control: Use of interferon-gamma release assays in support of TB diagnosis. ECDC, Stockholm; 2011.
Mazurek M, Jereb J, Vernon A, LoBue P, Goldberg S, Castro K: Updated guidelines for using interferon gamma release assays to detect mycobacterium tuberculosis infection - United States, 2010. MMWR Recomm Rep 2010,59(RR-5):1–25.
Ringshausen FC, Schlosser S, Nienhaus A, Schablon A, Schultze-Werninghaus G, Rohde G: In-hospital contact investigation among health care workers after exposure to smear-negative tuberculosis. J Occup Med Toxicol 2009, 4: 11. 10.1186/1745-6673-4-11
Barnett AG, van der Pols JC, Dobson AJ: Regression to the mean: what it is and how to deal with it. Int J Epidemiol 2005,34(1):215–220.
Acknowledgements
We would like to thank all HCWs for study participation, all occupational health physicians for recruitment and data collection, and our coauthors for their input in the above-mentioned original studies of our own.
Funding
This work was supported in part by a research grant from the Institution for Statutory Accident Insurance and Prevention in Health and Welfare Services, Hamburg, Germany.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
FCR, AS, and AN have made substantial contributions to the conception and design of the review, the acquisition and analysis of the review data, and have been involved in drafting and revising the manuscript. All authors have read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Ringshausen, F.C., Schablon, A. & Nienhaus, A. Interferon-gamma release assays for the tuberculosis serial testing of health care workers: a systematic review. J Occup Med Toxicol 7, 6 (2012). https://doi.org/10.1186/1745-6673-7-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1745-6673-7-6