
Abstract
Background
Low back pain affects approximately 80% of people at some stage in their lives. Exercise therapy is the most widely used nonsurgical intervention for low back pain in practice guidelines. Whole body vibration exercise is becoming increasingly popular for relieving musculoskeletal pain and improving health-related quality of life. However, the efficacy of whole body vibration exercise for low back pain is not without dispute. This study aims to estimate the effect of whole body vibration exercise for chronic low back pain.
Methods/Design
We will conduct a prospective, single-blind, randomized controlled trial of 120 patients with chronic low back pain. Patients will be randomly assigned into an intervention group and a control group. The intervention group will participate in whole body vibration exercise twice a week for 3 months. The control group will receive general exercise twice a week for 3 months. Primary outcome measures will be the visual analog scale for pain, the Oswestry Disability Index and adverse events. The secondary outcome measures will include muscle strength and endurance of spine, trunk proprioception, transversus abdominis activation capacity, and quality of life. We will conduct intention-to-treat analysis if any participants withdraw from the trial.
Discussion
Important features of this study include the randomization procedures, single-blind, large sample size, and a standardized protocol for whole body vibration in chronic low back pain. This study aims to determine whether whole body vibration exercise produces more beneficial effects than general exercise for chronic low back pain. Therefore, our results will be useful for patients with chronic low back pain as well as for medical staff and health-care decision makers.
Trial registration
Chinese Clinical Trial Registry: ChiCTR-TRC-13003708.
Similar content being viewed by others

Background
Low back pain (LBP) is a major public health challenge all over the world [1, 2]. The lifetime prevalence of LBP is shown to be 84%, and the prevalence of chronic LBP is about 23%, 11 to 12% of people are disabled by LBP [3]. Because of its high prevalence, LBP often leads to a large economic burden with regard to medical expenses and lost wages [4, 5]. In the United States, statistics show that total direct and indirect costs for the treatment of LBP are estimated to be more than $100 billion each year [6, 7].
Exercise therapy is recommended as an effective treatment for relieving pain and improving back function for patients with LBP by most clinical guidelines [3, 8–11]. During the past decade, whole body vibration (WBV) exercise has become increasingly popular for relieving musculoskeletal pain and improving health-related quality of life [12, 13]. In whole body vibration, the vibration signals are delivered through a vibratory platform or chair to expose a larger part of the body to the stimulation [14]. WBV exercise consists of standing statically or performing dynamic movements on an oscillating platform. Exercise training using vibratory platforms may be a complementary training to standard physical rehabilitation programs. WBV provides amplitude of displacement (ranging from 0.7 to 14 mm) and a mechanical oscillation of a specific frequency (ranging from 0.5 to 80 Hz) [15, 16]. Several studies have demonstrated that whole body vibration exercise can reduce pain for women with fibromyalgia syndrome [17], young patients with musculoskeletal pain [18], and elderly patients with knee osteoarthritis [19].
At present, WBV exercise is being marketed as an intervention for patients with LBP [20–25]. There are two reasons WBV exercise may be useful for alleviating pain in patients with LBP. First, LBP is known to be associated with reduced abdominal and back extensor stabilization muscle activity [26]. It has been proposed that WBV may assist in reducing LBP by activating stretch reflexes and subsequently activating and strengthening the abdominal and back extensor stabilization muscles [23]. Second, LBP is known to be associated with paravertebral muscle spasm, and it has been suggested that WBV at frequencies below 20 Hz may reduce LBP by inducing muscle relaxation [27].
Whole body vibration exercise has a theoretical basis in treatment of LBP, as is evidenced by its clinical use. However, the efficacy of WBV exercise for low back pain is not without dispute. The results of several studies suggest that whole body vibration exercise relieves chronic back pain through a genuine analgesic effect [21–23]. On the other hand, some studies show that WBV exercise was not effective for patients with LBP [28, 29], and WBV has even been considered harmful [30].
It is important to ensure that the determination of the effectiveness of WBV exercise for LBP is based on scientific evidence so as not to waste staff time and resources and to avoid unnecessary stress for patients with LBP and their families. Thus, we conduct a single-blind randomized controlled trial (RCT) to determine the effects of WBV for patients with LBP compared to general exercise.
Methods/Design
Aim of the study
We will perform an RCT involving whole body vibration exercise in patients with chronic low back pain in order to determine:
-
1)
whether WBV exercise is effective for the treatment of chronic LBP,
-
2)
whether WBV exercise produces more beneficial effects than general exercise for chronic LBP, and
-
3)
adverse effects associated with whole body vibration.
Study design
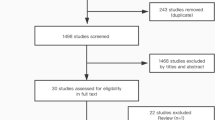
This is a single-blind randomized controlled trial comparing a WBV exercise with general exercise (Figure 1). A total of 120 patients with chronic LBP will be recruited and investigated from Shanghai Shangti Orthopedic Hospital and Shanghai University of Sport, Shanghai City, China.

Flow diagram showing whole body vibration exercise for patients with low back pain (LBP).
All participants, prior to initiation of the study, will accept a questionnaire asking for the following details: basic information (for example, age), past and present job status, medical history, pain (visual analog scale, VAS), back function (Oswestry Disability Index, ODI) and exercise habits (for example, frequency and time/session). Prior to inclusion, informed consent will be sought from all participants in the study.
The subjects will be allocated in a 1:1 ratio by computer-generated randomization if they meet the inclusion criteria. After randomization, patients with chronic LBP will be assigned to the control group (general exercise) or to the intervention group (WBV exercise). The total study period will be 6 months, which has a 3-month intervention and 3-month follow-up period with no intervention. The study will include assessments at the following time points: before intervention, at 3 months, and at 6 months.
Participants
Inclusion criteria are:
-
1.
age 18 to 60 years old,
-
2.
pain for more than 3 months,
-
3.
lack of abnormal sense and reflection of the lower extremity,
-
4.
medication not expected to change during the study period, and
-
5.
availability 3 times a week over a period of 3 months.
Exclusion criteria are:
Subjects who have any of the following conditions will be excluded:
-
1.
undergone previous surgery, dislocation, fracture, rheumatoid arthritis, and ankylosing spondylitis;
-
2.
severe cardiovascular, progressive neurological deficits, severe osteoporosis, or metabolic diseases;
-
3.
low back pain caused by visceral disease;
-
4.
VAS score (from 1 to 10) above 8;
-
5.
inability to communicate in Chinese;
-
6.
attended WBV exercise last 3 months;
-
7.
pregnant or lactating.
-
8.
uncontrolled hypertension; or
-
9.
other illness, judged by the patient or study physician to make participation in this study inadvisable.
Withdrawal criteria and management
Patients with chronic LBP will be allowed or be asked to withdraw from the study if:
-
1.
The patient makes such a request.
-
2.
The patient develops a serious disease, such as stroke or heart disease.
-
3.
The patient has an adverse effects related to the WBV exercise.
Ethical considerations
Before the intervention, each subject will be asked to sign a written informed consent. The study was approved by the ethics committee of the Shanghai University of Sport, China.
Interventions
Both groups will receive exercise intervention twice a week for 3 months, and each session will involve a warm-up for 5 minutes and cool down for 5 minutes. The participants will be asked to fill out forms to record the times and durations of exercise intervention.
Intervention group
All subjects will perform whole body vibration exercise by an available vibration device (AV001; BODYGREEN, Taiwan, China). To eliminate any effect of vibrations, we ask patients to remove their shoes. The WBV exercise protocol includes five exercise positions: double leg stance, deep squat, lower back extension, bridge pose, and push up. More information about the WBV protocol is shown in Table 1 and Figure 2. WBV exercise programs will be led by registered physical therapists.

Illustration of five movements. A. Double leg stance: place the feet parallel on both sides of machine with heals turned slightly outward. B. Deep squat. C. Lower back extension. D. Bridge pose. E. Push up.
Control group
The participants in the control group will perform the same exercise protocol as the WBV group, but without vibration. The participants in the both groups will be asked to maintain their previous lifestyle and not take part in any other regular rehabilitation programs.
Outcome measures
Primary outcome measures include the following:
-
1.
Pain intensity, which will be assessed using the VAS. It is usually a horizontal line, 100 mm in length, which is marked with ‘no pain’ (score 0) and ‘unbearable pain’ (score 10) from the left to the right. The patient marks on the line the point that they feel represents their perception of their current state. The amount of pain that a patient feels ranges across a continuum from none to an extreme amount of pain [31].
-
2.
Back function, which will be measured using the Oswestry Disability Index [32], an index that consists of ten sections related to activities of daily living commonly affected by low back pain. Each section is scored from 0 to 5 with higher values indicating more severe impact.
-
3.
Adverse events associated with whole body vibration exercise, which will be reported.
Secondary outcome measures include:
-
1.
Muscle strength and endurance of trunk, which will be tested using a Biodex 3 dynamometer (Biodex Medical Systems, New York, USA). Participants will perform ten maximum concentric contractions for trunk extensors and flexors at the angular velocities of 60°/s, 120°/s. The muscle endurance index is defined as the ratio of the work done during the last five contractions over the first five contractions. Main outcome parameters will be peak torque (Newton-meters), peak torque/ body weight, maximal power output (power) in Watts, work (work) in Joules [33].
-
2.
Trunk proprioception, which will be assessed with a joint position matching test [24]. The subject’s trunk will be moved to reference position (flexion or extension), and maintained at the position for 3 s. Then the subjects will be asked to reproduce the reference position from the neutral position. The subject is instructed to stop a position when he or she thinks that the test position has been reached. The assessor records the position and angle. This sequence of events will be repeated three times, and these three measures were averaged for a score of repositioning error for the first pre-test. The large absolute error is considered as poor proprioceptive acuity.
-
3.
Transversus abdominis activation capacity, which we will assess using the Stabilizer Pressure Biofeedback Unit (PBU, Chattanooga Group, Australia) [34]. The subject will be asked to lie in prone position over a rigid surface, then a PBU device will be placed under the transversus abdominis. The subjects are asked to contract the lower stomach for 10 seconds without moving the back or the hips. Then the assessor will record the pressure reduction from the PBU.
-
4.
Quality of life, which will be assessed with the short form 36 (SF-36) health survey [35]. The SF-36 includes eight scaled scores: vitality, physical functioning, bodily pain, general health perceptions, physical role functioning, emotional role functioning, social role functioning, and mental health. A score of SF-36 is from 0 (worst) to 100 (best).
Statistical analysis
The SPSS 17.0 and Microsoft Excel 2007 software will be used to perform statistical analyses. Data will be expressed as mean?±?standard deviation (SD). We will use two-way repeated measures analysis of variance (group?×?time) to compare the effect of WBV exercise group with the control group, including the primary and secondary outcomes. If subjects are lost to follow-up, an intention-to-treat analysis will be conducted. A T-test will be used to compare the changes in measures within groups when the analysis of variance reveals a significant difference. Statistical significance is a P less than 0.05.
Discussion
Based on the theory of WBV, it should be an effective treatment for chronic LBP. However, the evidence of WBV is inadequate, and the effect of WBV exercise is disputed for LBP. We will perform a prospective, single-blind, randomized controlled trial of WBV exercise for patients with chronic LBP. We think the study could bring about the proof that WBV may offer an alternative treatment for chronic LBP. WBV exercise could produce more beneficial effects than general exercise for chronic LBP, by reducing pain and improving function and quality of life.
Strengths and limitations
First, most previous WBV exercise studies have typically ranged in duration from a few weeks to 3 months [20, 21, 23, 24]. The study duration is an intervention period of 3 months and a follow-up period (with no active intervention) of 3 months, giving a total study period of 6 months. Second, in our study, intervention group performs five movements with vibration, but the control group receives the five same movements without vibration for an equal amount of time. Based on this point, the study could reduce other bias compared to previous studies [20–25]. Third, previous studies have mainly focused on pain, back disability, and quality of life. But trunk proprioception and transversus abdominis activation capacity are rarely analysed for WBV exercise on chronic LBP. There are also some limitations in our trial. The total number of subjects involved in the study is not large (120 patients). Moreover, only one vibration frequency (18 Hz) is used to estimate the effect of WBV for chronic LBP; different vibration frequency groups should be added to subsequent studies.
In conclusion, this study aims to determine the effect of WBV exercise for chronic LBP, and to estimate whether WBV exercise produces more beneficial effects than general exercise for chronic LBP. The results of the study will be of benefit to patients, researchers and policy makers with an interest in treatment of LBP.
Trial status
Patient recruitment is underway.
Abbreviations
- LBP:
-
low back pain
- ODI:
-
Oswestry disability index
- PBU:
-
pressure biofeedback unit
- RCT:
-
randomized controlled trial
- SD:
-
standard deviation
- SF-36:
-
short form 36
- VAS:
-
visual analog scales
- WBV:
-
whole body vibration.
References
Balagué F, Mannion AF, Pellisé F, Cedraschi C: Non-specific low back pain. Lancet. 2012, 379: 482-491. 10.1016/S0140-6736(11)60610-7.
Berman BM, Langevin HM, Witt CM, Dubner R: Acupuncture for chronic low back pain. N Engl J Med. 2010, 363: 454-461. 10.1056/NEJMct0806114.
Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G, COST B13 Working Group on Guidelines for Chronic Low Back Pain: Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006, 15: S192-S300. 10.1007/s00586-006-1072-1.
Ivanova JI, Birnbaum HG, Schiller M, Kantor E, Johnstone BM, Swindle RW: Real-world practice patterns, health-care utilization, and costs in patients with low back pain: the long road to guideline-concordant care. Spine J. 2011, 11: 622-632. 10.1016/j.spinee.2011.03.017.
Miller P, Kendrick D, Bentley E, Fielding K: Cost-effectiveness of lumbar spine radiography in primary care patients with low back pain. Spine. 2002, 27: 2291-2297. 10.1097/00007632-200210150-00021.
Frymoyer JW, Cats-Baril WL: An overview of the incidences and costs of low back pain. Orthop Clin North Am. 1991, 22: 263-271.
Crow WT, Willis DR: Estimating cost of care for patients with acute low back pain: a retrospective review of patient records. J Am Osteopath Assoc. 2009, 109: 229-233.
Chou R, Qaseem A, Snow V, Casey D, Cross JT, Shekelle P, Owens DK, Clinical Efficacy Assessment Subcommittee of the American College of Physicians, American College of Physicians, American Pain Society Low Back Pain Guidelines Panel: Diagnosis and treatment of low back pain: a joint clinical practice guideline from the American College of Physicians and the American Pain Society. Ann Intern Med. 2007, 147: 478-491. 10.7326/0003-4819-147-7-200710020-00006.
Wang XQ, Zheng JJ, Chen PJ: Clinical pilates versus general exercise for chronic low back pain. Med Sci Sports Exerc. 2013, 45: 603-
Wang XQ, Zheng JJ, Bi X, Liu J: Effect of core stability training on patients with chronic low back pain. Health Med. 2012, 6: 754-759.
Wang XQ, Zheng JJ, Yu ZW, Bi X, Lou SJ, Liu J, Cai B, Hua YH, Wu M, Wei ML, Shen HM, Chen Y, Pan YJ, Xu GH, Chen PJ: A meta-analysis of core stability exercise versus general exercise for chronic low back pain. PLoS One. 2012, 7: e52082-10.1371/journal.pone.0052082.
Simão AP, Avelar NC, Tossige-Gomes R, Neves CD, Mendonça VA, Miranda AS, Teixeira MM, Teixeira AL, Andrade AP, Coimbra CC, Lacerda AC: Functional performance and inflammatory cytokines after squat exercises and whole-body vibration in elderly individuals with knee osteoarthritis. Arch Phys Med Rehabil. 2012, 93: 1692-1700. 10.1016/j.apmr.2012.04.017.
Adsuar JC, Del Pozo-Cruz B, Parraca JA, Olivares PR, Gusi N: Whole body vibration improves the single-leg stance static balance in women with fibromyalgia: a randomized controlled trial. J Sports Med Phys Fitness. 2012, 52: 85-91.
Lau RW, Teo T, Yu F, Chung RC, Pang MY: Effects of whole-body vibration on sensorimotor performance in people with Parkinson disease: a systematic review. Phys Ther. 2011, 91: 198-209. 10.2522/ptj.20100071.
Rehn B, Lidström J, Skoglund J, Lindström B: Effects on leg muscular performance from whole-body vibration exercise: a systematic review. Scand J Med Sci Sports. 2007, 17: 2-11.
Cardinale M, Rittweger J: Vibration exercise makes your muscles and bones stronger: fact or fiction?. J Br Menopause Soc. 2006, 12: 12-18. 10.1258/136218006775997261.
Alentorn-Geli E, Padilla J, Moras G, Lázaro Haro C, Fernández-Solà J: Six weeks of whole-body vibration exercise improves pain and fatigue in women with fibromyalgia. J Altern Complement Med. 2008, 14: 975-981. 10.1089/acm.2008.0050.
Elfering A, Thomann J, Schade V, Radlinger L: Stochastic resonance whole body vibration reduces musculoskeletal pain: A randomized controlled trial. World J Orthop. 2011, 2: 116-120. 10.5312/wjo.v2.i12.116.
Avelar NC, Simão AP, Tossige-Gomes R, Neves CD, Rocha-Vieira E, Coimbra CC, Lacerda AC: The effect of adding whole-body vibration to squat training on the functional performance and self-report of disease status in elderly patients with knee osteoarthritis: a randomized, controlled clinical study. J Altern Complement Med. 2011, 17: 1149-1155. 10.1089/acm.2010.0782.
Belavý DL, Armbrecht G, Gast U, Richardson CA, Hides JA, Felsenberg D: Countermeasures against lumbar spine deconditioning in prolonged bed rest: resistive exercise with and without whole body vibration. J Appl Physiol. 1801–1811, 2010: 109-
del Pozo-Cruz B, Hernández Mocholí MA, Adsuar JC, Parraca JA, Muro I, Gusi N: Effects of whole body vibration therapy on main outcome measures for chronic non-specific low back pain: a single-blind randomized controlled trial. J Rehabil Med. 2011, 43: 689-694. 10.2340/16501977-0830.
Iwamoto J, Takeda T, Sato Y, Uzawa M: Effect of whole-body vibration exercise on lumbar bone mineral density, bone turnover, and chronic back pain in post-menopausal osteoporotic women treated with alendronate. Aging Clin Exp Res. 2005, 17: 157-163. 10.1007/BF03324589.
Rittweger J, Just K, Kautzsch K, Reeg P, Felsenberg D: Treatment of chronic lower back pain with lumbar extension and whole-body vibration exercise: a randomized controlled trial. Spine. 1829–1834, 2002: 27-
Fontana TL, Richardson CA, Stanton WR: The effect of weight-bearing exercise with low frequency, whole body vibration on lumbosacral proprioception: a pilot study on normal subjects. Aust J Physiother. 2005, 51: 259-263. 10.1016/S0004-9514(05)70007-6.
Tiemessen IJ, Hulshof CT, Frings-Dresen MH: Low back pain in drivers exposed to whole body vibration: analysis of a dose–response pattern. Occup Environ Med. 2008, 65: 667-675. 10.1136/oem.2007.035147.
Hodges PW, Richardson CA: Inefficient muscular stabilization of the lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine. 1996, 21: 2640-2650. 10.1097/00007632-199611150-00014.
Rittweger J, Mutschelknauss M, Felsenberg D: Acute changes in neuromuscular excitability after exhaustive whole body vibration exercise as compared to exhaustion by squatting exercise. Clin Physiol Funct Imaging. 2003, 23: 81-86. 10.1046/j.1475-097X.2003.00473.x.
Tiemessen IJ, Hulshof CT, Frings-Dresen MH: Effectiveness of an occupational health intervention program to reduce whole body vibration exposure: an evaluation study with a controlled pretest-post-test design. Am J Ind Med. 2009, 52: 943-952. 10.1002/ajim.20769.
Hulshof CT, Verbeek JH, Braam IT, Bovenzi M, van Dijk FJ: Evaluation of an occupational health intervention programme on whole-body vibration in forklift truck drivers: a controlled trial. Occup Environ Med. 2006, 63: 461-468. 10.1136/oem.2005.020032.
Kåsin JI, Mansfield N, Wagstaff A: Whole body vibration in helicopters: risk assessment in relation to low back pain. Aviat Space Environ Med. 2011, 82: 790-796. 10.3357/ASEM.2982.2011.
Wewers ME, Lowe NK: A critical review of visual analogue scales in the measurement of clinical phenomena. Res Nurs Health. 1990, 13: 227-236. 10.1002/nur.4770130405.
Fairbank JC, Couper J, Davies JB, O’Brien JP: The Oswestry low back pain disability questionnaire. Physiotherapy. 1980, 66: 271-273.
Gruther W, Wick F, Paul B, Leitner C, Posch M, Matzner M, Crevenna R, Ebenbichler G: Diagnostic accuracy and reliability of muscle strength and endurance measurements in patients with chronic low back pain. J Rehabil Med. 2009, 41: 613-619. 10.2340/16501977-0391.
Grooms DR, Grindstaff TL, Croy T, Hart JM, Saliba SA: Clinimetric analysis of pressure biofeedback and transversus abdominis function in individuals with stabilization classification low back pain. J Orthop Sports Phys Ther. 2013, 43: 184-193. 10.2519/jospt.2013.4397.
Ferrari R: Responsiveness of the short-form 36 and oswestry disability questionnaire in chronic nonspecific low back and lower limb pain treated with customized foot orthotics. J Manipulative Physiol Ther. 2007, 30: 456-458. 10.1016/j.jmpt.2007.03.016.
Acknowledgements
This work was supported by Key Laboratory of Exercise and Health Sciences (Shanghai University of Sport), Ministry of Education; the Shanghai Key Lab of Human Performance (SUS) (11DZ2261100).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
XQW, YLP and PJC conception and design of the trial. XQW, YLP, PJC, LCL and JZ participated in the trial register, communication and monitoring. BLC, XL and XW participated in the design of statistical analysis. All authors contributed to drafting the manuscript, read and approved the final version.
Xue-Qiang Wang, Yan-Lin Pi contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Wang, XQ., Pi, YL., Chen, PJ. et al. Whole body vibration exercise for chronic low back pain: study protocol for a single-blind randomized controlled trial. Trials 15, 104 (2014). https://doi.org/10.1186/1745-6215-15-104
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1745-6215-15-104