
Abstract
The assessment of pain is of critical importance for mechanistic studies as well as for the validation of drug targets. This review will focus on knee joint pain associated with arthritis. Different animal models have been developed for the study of knee joint arthritis. Behavioral tests in animal models of knee joint arthritis typically measure knee joint pain rather indirectly. In recent years, however, progress has been made in the development of tests that actually evaluate the sensitivity of the knee joint in arthritis models. They include measurements of the knee extension angle struggle threshold, hind limb withdrawal reflex threshold of knee compression force, and vocalizations in response to stimulation of the knee. A discussion of pain assessment in humans with arthritis pain conditions concludes this review.
Similar content being viewed by others


Review
Arthritis represents one of the most prevalent chronic health problems and is a leading cause of disability. More than 40 million people in the United States have arthritis or chronic joint symptoms that are often accompanied by joint pain [1]. By the year 2020, this number is expected to reach 60 million. The most common form of arthritis is osteoarthritis affecting an estimated 21 million adults in the United States. Other common arthritic conditions include rheumatoid arthritis (about 2.1 million people in the United States) and gout [2]. The assessment of arthritic pain is of critical importance for the better understanding of underlying mechanisms and for the evaluation of therapeutic targets. Different animal models of arthritis are available for the assessment of joint pain and analgesic drug effects. This review will focus on arthritis models of knee joint pain and on behavioral tests used in these models. Information about the assessment of knee joint pain in humans with arthritis will also be provided.
Discussing the merits of electrophysiological studies of nociceptive processing in arthritis pain models is beyond the scope of this article. Arthritis pain-related electrophysiological changes have been measured in primary afferent nerve fibers [peripheral sensitization; 3] and in central nervous system neurons (central sensitization), including neurons in the spinal dorsal horn [4], spinal trigeminal nucleus [5], pain modulating brainstem centers [6], ventrobasal thalamus [7], somatosensory cortex [8] and amygdala [9]. While electrophysiological studies are important and necessary for the analysis of pathways, circuitry, neuronal plasticity, transmitter action and signal transduction mechanisms, behavioral tests are needed for the assessment of pain.
Arthritis pain models
Arthritis is the inflammation of a joint, which can include infiltration of inflammatory cells (monocytes), synovial hyperplasia, bone erosion and new bone formation, narrowing of the joint space, and ankylosis of the joint [10]. The most common form of arthritis is osteoarthritis. Osteoarthritis is a degenerative disease characterized by damage to the articular cartilage, changes in subchondral and marginal bone, synovitis and capsular thickening, typically affecting weight bearing joints (knee and hips) [11]. Pain in osteoarthritis is localized and use-related, occurring during movement or weight bearing [12–14]. Rheumatoid arthritis is an autoimmune disease of the synovium that leads to an inflammatory poly-arthritis. It is characterized by the symmetrical pattern of affected joints and by morning stiffness, joint swelling and tenderness. Pain in rheumatoid arthritis improves with movement [15, 16]. Gout represents one of the most painful forms of arthritis. A metabolic disorder with high blood levels of uric acid (hyperuricemia), gout is characterized by recurrent episodes of acute arthritis resulting from deposits of needle-like crystals of uric acid in the joints. The metatarsophalangeal joint (big toe) is typically affected, but other joints can be involved as well, including the knee [17, 18]. The following animal models have been developed to investigate the pathophysiology of different forms of knee joint arthritis. They are also used for the assessment of joint pain but not all of them have a proven track record of predictability for human disease.
Osteoarthritis
Animal models include spontaneous osteoarthritis in specific strains (mouse and guinea pig) and osteoarthritis induced chemically or mechanically (surgically) [12–14]. Chemical models involve intra-articular injections of compounds that cause joint pathology through inhibition of chondrocyte metabolism by papain or monosodium iodoacetate (MIA) and damage of ligaments and tendons with collagenase. Surgical models induce joint instability by (partial) meniscectomy combined with transection of collateral and/or cruciate ligaments [12–14]. The MIA model has emerged as a particularly useful osteoarthritis model for the study of pain and analgesic drug effects because it is reproducible and mimics pathological changes and pain of osteoarthritis in humans. Intraarticular injection of MIA produces progressive joint degeneration through inhibition of glycolysis and subsequent chondrocyte death that develops over several weeks. Similar to human osteoarthritis, joint pathology is characterized by chondrocyte necrosis resulting in decreased thickness of the articular cartilage and fibrillation of the cartilage surface, separation of the necrotic cartilage from the underlying bone and exposure of the subchondral bone; osteolysis and swelling; and reductions in bone mineral content and density [13, 14, 19].
Inflammatory mono-arthritis
Recurrent inflammatory phases are common in human osteoarthritis [1]. The acute inflammatory phase of osteoarthritis is also mimicked by the kaolin/carrageenan-induced knee joint arthritis model (K/C arthritis). Intraarticular kaolin and carrageenan injections into one knee produce an aseptic use-dependent monoarthritis with damage to the cartilage, inflammation of the synovia and synovial fluid exudate. The K/C arthritis develops rapidly within hours and persists for weeks. Pathological, behavioral and electrophysiological changes have been studied extensively in the K/C arthritis model in mouse, rat, cat and non-human primate [20–25]. A modification of the K/C arthritis model is the knee joint monoarthritis induced by intraarticular injection of carrageenan alone. The time course of the carrageenan-arthritis is shorter (hours to days) and the cartilage damage less pronounced than in the K/C model [26–29].
Other models of inflammatory mono-arthritis in the knee include the acute zymosan-induced arthritis and the chronic complete Freund's adjuvant (CFA) induced arthritis. Injection of zymosan into one knee produces an erosive synovitis in mouse and rat. The zymosan arthritis is characterized by an acute phase of increased vascular permeability, edema formation, neurophil infiltration and exudate within hours, whereas the chronic phase (days to several weeks) resembles chronic rheumatoid synovitis with mononuclear cell infiltration (macrophages and lymphocytes), fibroblast reaction and pannus formation [30–32]. The CFA mono-arthritis of the knee is induced by intraarticular injection of complete Freund's adjuvant, suspension of heat-killed Mycobacterium butyricum or Mycobacterium tuberculosum [33–36]. This chronic monoarthritis is characterized by joint inflammation, cartilage destruction and bone erosion, which persist for at least several weeks. The CFA mono-arthritis model represents a modification of the classical adjuvant-induced poly-arthritis. While the CFA model is well established in rats, it has been difficult to produce a reliable CFA arthritis in mice. Only recently a CFA-arthritis model was developed in mice in which repeated injections of a much higher concentration of CFA into one knee (once per week for 4 weeks) produced a monoarthritis of the knee with synovial hypertrophy, neutrophil infiltration, mild erosion of cartilage and bone, and small amounts of pannus [37]. The murine CFA-monoarthritis lasted for at least 5 weeks after the first intraarticular injection whereas a single injection produced a short-lasting inflammation that resolved within 7 days.
Rheumatoid Arthritis
Animal models include poly-arthritis induced by immunogenic adjuvants (CFA and cartilage antigens) and non-immunogenic adjuvants (lacking bacterial cell wall or peptide-containing components) [15, 38]. The knee joint is not the primary target and area of interest in these models. Further, the systemic nature of this arthritis may affect the overall condition and well being of the animals and may confound pain assessment. The widely used CFA poly-arthritis represents a model of chronic immune-mediated joint inflammation that is induced by intradermal or subcutaneous injection of a suspension of heat killed Mycobacterium butyricum or Mycobacterium tuberculosum (CFA) at the base of the tail or in the foodpad. The ensuing poly-arthritis represents a systemic disease with inflammation of distal joints of the limbs (ankle, wrist, tarsal, carpal, interphalangeal joints) and spinal joints, lesions of the eyes, ears, nose, skin and genitourinary and gastrointestinal tracts, as well as anorexia and profound weight loss [3, 15]. The CFA arthritis follows a biphasic time course, consisting of an acute local inflammatory reaction within hours that subsides after 3–5 days and a chronic systemic reaction that shows a relapsing-remitting course after the initial two weeks and can persist for several months. The persistent disease ultimately results in chronic joint deformation and signs of joint destruction, including synovitis and synovial hyperplasia, angiogenesis, pannus formation, capsular fibrosis, cartilage destruction, bone erosion and new periosteal bone formation, bone matrix resorption, inflammation of the bone marrow, and ankylosis [39]. The CFA poly-arthritis model is well established and reproducible in rats but not in mice (however, see CFA mono-arthritis).
Another immunogenic adjuvant model of rheumatoid arthritis model is induced by cartilage-derived proteins such as collagen II, collagen XI and cartilage oligomeric matrix protein (COMP) in rat and mouse [38]. Emulsified with CFA the cartilage antigens are injected intradermally at the base of the tail. The best characterized cartilage-induced arthritis model is the collagen type II arthritis (CIA arthritis), which leads to a severe erosive poly-arthritis affecting the hind paws and knees [40, 41]. Periarticular erythema and edema and neutrophil infiltration appear in the hind paws after 2–3 weeks followed by a chronic relapsing phase (5 weeks) when the severity of arthritis progresses to include pannus formation, erosion of cartilage, bone resorption, osteophyte formation, restructuring and ankylosis of the joints [38, 40, 42]. The autologous collagen type XI-induced arthritis shows a more aggressive course and pathology, whereas the COMP-induced arthritis is rather acute and self-limited [38].
Adjuvant arthritis without an autoimmune component is induced by compounds which do not contain major histocompatibility complex binding peptides but involve T-cell activation. These "pure" adjuvants include mineral oil (incomplete Freund's adjuvant), avridine, squalene and pristane [38]. Intradermal or subcutaneous injections of pure adjuvants produce a chronic relapsing arthritis with characteristics of rheumatoid arthritis. The severe and long-lasting (months) arthritis appears after 1–2 weeks in peripheral joints, mainly in the hind limbs, with pannus formation, erosion of cartilage and bone, and joint deformation [38].
Gouty arthritis
Gout is a metabolic disease characterized by recurrent episodes of acute arthritis in the metatarsophalangeal joint but can also affect the knee joint [17, 18]. Gouty arthritis results from the deposits of needle-like crystals of uric acid in the joints, causing inflammation with severe pain in the affected joint. Injection of monosodium urate crystals dissolved in saline [43] or uric acid suspended in mineral oil [17] into the knee joint leads to an acute inflammation (synovitis) within 2–3 hours, which persists at maximum levels for hours and resolves after 3–7 days
Pain behavior of arthritic animals
The main challenge of assessing knee joint pain has been to develop tests that actually measure the sensitivity of the knee joint rather than that of the hind paw [33]. Behavioral tests that use indirect measures of knee joint pain in arthritis models include static and dynamic weight bearing [13, 26, 43–46]; foot posture [43, 47] and gait analysis [43, 48], including paw elevation time during walking [17, 27, 32, 49]; spontaneous mobility [50, 51]; and mechanical or heat sensitivity of the paw [14, 45–47, 52]. Though indirect measures, weight bearing and gait analysis have the advantage that they are also used in the clinical setting to assess pain in patients with arthritis (see "Pain assessment in patients with arthritis").
More recently, behavioral tests have been developed that directly assess the mechanical sensitivity of the knee by measuring the hind limb withdrawal reflex threshold of knee compression force [33, 37, 51, 53], struggle threshold angle of knee extension [33, 35], and vocalizations evoked by stimulation of the knee [33, 51, 54].
Weight bearing
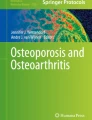
Measurements of weight bearing have been used in mono-arthritis models induced in the knee joint by carrageenan, urate, MIA or papain and by surgery (partial meniscectomy). Most commonly, the weight distribution on the two hind paws is measured as the force exerted by each limb on a transducer plate in the floor over a given time period [13, 26, 43–46]. Weight borne by each hind limb is expressed as percent of body weight [14, 44] or percent of weight borne by both hind limbs [13, 45]. The ratio [19, 43] or difference [46, 55] of weight distribution (force) between each hind limb are also calculated. A significant shift of weight from the arthritic site to the contralateral limb, i.e., a weight-bearing deficit, is taken as a pain measure and has been shown in knee joint arthritis models induced by intraarticular MIA [13, 14, 45, 46, 55], papain [13], urate [43] and carrageenan [44] and by partial meniscectomy [14, 56]. Figure 1 illustrates the weight bearing deficit in rats with MIA-induced knee joint arthritis. These static measurements of weight bearing by the hind limbs typically involve restraining the animals and do not assess the shift of weight distribution to the forelimbs as occurs with hind limb injury such as arthritis [48].

Development of punctate (A) and dynamic (B) allodynia and weight bearing deficit (C) following intraarticular injection of monosodium iodoacetate (MIA, 2 mg; ■) MIA or saline (○) in the right knee. (A) Baseline (BL) paw withdrawal thresholds (PWT) were determined in both hind paws prior to injection. PWT to von Frey hair stimulation of the plantar paw surface were assessed on various days post-injection. Results are expressed as median force (g) required for a paw withdrawal in 10 animals per group (vertical bars represent first and third quartiles). * P < 0.05, ** P < 0.01, *** P < 0.001 significantly different (Mann-Whitney U test) from saline-treated group at each time point. (B) Baseline (BL) paw withdrawal latencies (PWL) to stroking the plantar paw surface with a cotton bud were determined for both hind paws prior to injection. Results are expressed as mean PWL (s) in 10 animals per group (vertical bars represent ± SEM). * P < 0.05, ** P < 0.01, *** P < 0.001 significantly different (one-way ANOVA followed by Dunnett's posthoc test) from saline-treated group. (C) Baseline (BL) hind paw weight distribution was determined prior to injection. Changes in hind paw weight distribution were assessed on various days post-injection. Results are expressed as mean change in weight distribution (contralateral-ipsilateral) (g) in 10 animals per group (vertical bars represent ± SEM). * P < 0.05, ** P < 0.01, *** P < 0.001 significantly different (one-way ANOVA followed by Dunnett's posthoc test) from saline-treated group. Reprinted from [46], Copyright 2004, with permission from Elsevier.
Weight bearing across all four limbs has been measured in rats with a carrageenan-induced knee joint arthritis [26, 29]. Weight load on each limb is detected while the animal is walking across four pairs of force sensor plates in the floor of an enclosed walkway. Time-weight curves for left and right fore limbs and hind limbs of rats with arthritis show a reduction of weight load on the affected limb for up to one week. Similarly, weight distribution across the four limbs has been measured in the MIA arthritis model using load cell platforms in two sections of the glass floor in the central portion of a chamber [48]. The digitized load cell output and simultaneously videotaped images are used to calculate the peak vertical load bearing by each limb. Load bearing by the affected limb is reduced for several weeks. Weight distribution across the four limbs has also been determined with a gait analysis system ("CatWalk") that measures the intensity of the illumination caused by paw contact with a glass floor [57]. The intensity correlates with pressure (weight support) and mechanical withdrawal thresholds and is significantly reduced in the affected limb of neuropathic rats. The CatWalk analysis system may also be useful for the assessment of weight-bearing in arthritis. A potential problem with dynamic weight bearing measurements is that animals are required to move, which can be influenced by a number of factors such as motivation (see mobility).
Posture and gait analysis
Related to the assessment of weight bearing, abnormal posture of the hind paw and gait have been quantified in knee joint arthritis models using subjective rating scales. Static (standing) and dynamic (walking) behaviors have been analyzed separately to calculate a "pain score" in rats with urate-induced knee joint arthritis [43]. Categories of the rating scale include complete touch of foot pad, partial touch or one foot stand (standing position) and slight limping, severe limping or one foot gait (walking state). A combination of posture and gait analysis has been used to rate pain-related spontaneous behavior in the carrageenan-induced knee joint arthritis [47]. Behavioral signs include curling toes, eversion of the foot, partial weight bearing, non-weight bearing and guarding, and avoiding contact with the limb.
Gait disturbance has also been detected using the knee joint incapacitation test in rats with knee joint arthritis induced by intraarticular injections of carrageenan [27], zymosan [32, 49] or uric acid [17]. Increased paw elevation times are measured in arthritic rats walking on a rotating mesh-covered steel drum. Metal gaiters ("electrodes") wrapped around the hind paws are connected via a simple circuit to a computer to record the time of contact between each hind paw and the cylinder, which is when the circuit is closed. Paw elevation time or the ratio of time of contact of the affected foot and the control foot serve as indicators of pain-related functional impairment. The advantage of this gait analysis test is that the quantitation (paw elevation time) is independent of the observer. Interestingly, temporal aspects of gait were not impaired in rats with a MIA knee joint arthritis when velocity of locomotion, stride, stance and swing times, and stride length were measured from the pattern of paw contact with the illuminated glass floor of a behavioral chamber [48].
Spontaneous mobility
Locomotor activity has been measured in arthritic rats using biotelemetry or activity boxes. The biotelemetry system comprises a transmitter implanted in the peritoneal cavity of the rodent, and a receiver beneath the cage. The receiver detects the radio waves and activity of the rodents as counts which are registered in the computer system [50]. Loss of spontaneous mobility has been detected in rats with knee joint arthritis induced by MIA, papain, collagenase or surgical ligament transection. All models show a transitory "primary" loss of mobility for about two days after arthritis induction, presumably related to pain; but only the MIA arthritis results in a prolonged secondary loss of mobility for more than four weeks due to pain and loss of function [50]. Spontaneous exploratory activity has been measured using activity boxes that are divided in zones by photobeams consisting of pairs of infra red Light Emitting Diodes (LEDs) and phototransistors. Frequency and pattern of photobeam interruption by the animal's movements are recorded on a computer. Rats with K/C arthritis show decreased entries (number of movements from one zone to another) and increased resting time (total time during which no movements occurred) [51].
Mechanical or heat sensitivity of the paw
Von Frey filaments and a modified Randall-Selitto analgesiometer have been used to assess the mechanical sensitivity of the hindpaw in animals with knee joint arthritis. Typically, paw withdrawal thresholds (PWT) are measured in response to increasing pressure stimuli applied to the plantar surface by von Frey filaments or to the dorsal surface by a wedge-shaped probe of a Randall-Selitto analgesiometer. Rats with knee joint arthritis induced by MIA [14, 45, 46] have decreased PWT (mechanical allodynia; see Figure 1) for several weeks on the affected limb measured with either technique, but show little dynamic allodynia assessed by stroking the plantar surface of the paw. Surgically induced knee joint arthritis appears to be more sensitive to von Frey hair testing than to Randall-Selitto analgesiometry [14, 56]. Bilateral decreases of mechanical PWT measured with von Frey filaments occur in the K/C knee joint arthritis model [52].
Thermal sensitivity of the paw has been measured in arthritic rats using the hot-plate test and the paw withdrawal latency (PWL) to noxious heat. A unilateral decrease of PWL is observed in rats with a K/C knee joint arthritis [20, 24, 47]. Heat hyperalgesia was observed for less than 48 hours by one group [24, 47] but lasted for at least two weeks in another study [20], which would be consistent with the prolonged time course of the K/C arthritis as mentioned earlier [see 33]. Mice with a K/C knee joint arthritis also show decreased PWL but unchanged hot-plate latency, which is the time until the animal shakes or licks its hind limb [25]. No thermal hyperalgesia has been found in the surgically induced knee joint osteoarthritis model [56].
These tests assess secondary hyperalgesia or allodynia, which has been reported in patients with osteoarthritis but is not very common [13]. The following direct measures of knee joint pain have been developed recently.
Mechanical sensitivity of the knee
The threshold for hind limb withdrawal reflexes evoked by compression of the knee has been measured in arthritic rats and mice [37, 51, 53]. The knee joint of rats is compressed with a calibrated forceps equipped with force transducers (strain gauges) whose output is amplified, digitized and recorded on a computer and/or displayed in grams on a liquid crystal display screen [33, 51, 53]. Hind limb withdrawal reflexes in mice have been assessed by scoring the intensity of the manual compression of the knee required to evoke the reflex [37]. Withdrawal thresholds for stimulation of the arthritic, but not the contralateral, knee decrease in rats with K/C arthritis [51, 53] and in mice with CFA-induced knee joint arthritis [37]. This may be an important difference to the measurement of secondary mechanical allodynia in the PWT test that has shown bilateral changes in the K/C knee joint arthritis model [52].
Struggle threshold angle of knee extension
Reduced range of motion and mechanical sensitivity of the arthritic knee have been assessed by measuring the struggle threshold of the knee extension angle [33, 35]. In this quantitative test the tibia is extended until the rat shows struggling behavior, while the femur is held in position. The extension distance that the heel travels during movement is measured to calculate the extension angle by a trigonometric function that uses the length of the tibia and extension distance. In rats with knee joint arthritis induced by K/C [33] or CFA [33, 35] the struggle threshold angle of the extension of the arthritic knee is decreased compared to the contralateral knee for nearly two weeks in the K/C model and for 2–3 weeks in the CFA model. Figure 2 shows the time course of decreased struggle threshold in the K/C arthritis model.

Time course of the changes of three outcome measures in rats with a kaolin/carrageenan (K/C)-induced arthritis. (A) Circumference of the knee before and after K/C injection. (B) Angle at which the knee could be extended before eliciting struggling behavior in the rat. (C) Vocalization threshold of the compression force, which was applied to the knee. Post-injection time is expressed as hours (h) or days (d) after K/C injection. Pre-injection control was taken one day before the injection (-1 d). Asterisks indicate values significantly different from the pre-injection control value by one-way ANOVA followed by the Dunnett's posthoc test (n = 10). Symbols and error bars represent mean ± SE. Reprinted from [33], Copyright 2002, with permission from Elsevier.
Vocalizations evoked by compression of the knee
Rodents vocalize in the audible and ultrasonic ranges. When evoked by noxious stimuli, audible vocalizations represent a nocifensive reaction whereas ultrasonic vocalizations in the 22 kHz range reflect an emotional-affective response [51, 54]. The threshold of audible vocalizations has been measured by compressing the knee of manually restrained rats with a calibrated forceps as described above [33]. Vocalization thresholds are significantly decreased for one week in rats with a K/C arthritis (see Figure 2) and for two weeks in the CFA knee joint arthritis model [33]. A recording chamber and computerized analysis system has been developed to measure simultaneously audible and ultrasonic vocalizations evoked by stimulation of the knee [51, 54]. Rate and duration of audible and ultrasonic vocalizations are increased in rats with a K/C knee joint arthritis [51]. It should be noted that the functional relationship between audible and ultrasonic vocalizations, which are generated by different neural mechanisms, has not been addressed in these studies. Vocalizations that occur during stimulation (VDS) and vocalizations that outlast the stimulus (vocalization afterdischarges, VAD) have also been analyzed separately. VDS are organized in the brainstem at the medullary level whereas VAD are organized in the limbic forebrain, including the amygdala. Figure 3 shows that both VDS and VAD increase in rats with a K/C arthritis [54].

Increased audible and ultrasonic vocalizations in the K/C model of arthritic pain. (A, B) Original recordings of ultrasonic vocalizations evoked by innocuous (upper trace) and noxious (lower trace) stimulation of the knee joint in a rat before (A) and after (B) induction of arthritis with intraarticular kaolin and carrageenan injections. Mechanical stimuli were applied for 15 s; duration of the recording period was 1 min. Vocalizations during and after stimulation (VDS and VAD, respectively) were analyzed separately. (C) Duration of audible and ultrasonic VDS increased significantly 6 h after induction of arthritis compared to the values measured in the same animals before arthritis (n = 16). Stimuli of innocuous (left side) and noxious (right side) intensities evoked VDS of longer duration in arthritic animals compared to controls. (D) Duration of ultrasonic, but not audible, VAD following innocuous (left) and noxious (right) stimuli increased significantly in the arthritis pain model (6 h postinduction; n = 16). Symbols and error bars represent mean ± SE. ** P < 0.01, *** P < 0.001. Reprinted from Han JS & Neugebauer V [54]. PAIN 2005;113-211-222. Used with permission from the International Association for the Study of Pain®.
Pain assessment in patients with arthritis
Mechanical pain thresholds, range of motion, weight bearing and gait analysis have been measured in patients with knee joint arthritis. In addition, a variety of patient self-report questionnaires are frequently used to assess pain and function in patients with arthritis, including the Visual Analog Scale (VAS) and other rating scales, McGill Pain Questionnaire (MPQ) and its short form (SF-MPQ), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Health Assessment Questionnaire (HAQ), Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), and Disease Activity Score (DAS 28) [58].
Pain thresholds
Mechanical thresholds for pain are decreased in patients with osteoarthritis or rheumatoid arthritis [59]. Figure 4 shows the results obtained with von Frey filaments applied to the arthritic knee similar to studies in animals (see above). Whereas patients with osteoarthritis or rheumatoid arthritis have increased thresholds for mechanosensation, their cutaneous pain thresholds are lower than those of normal subjects [59].

Altered thresholds for mechanosensation (A) and pain (B) in patients with rheumatoid arthritis and osteoarthritis. (A) Mechanical sensation thresholds (g) for normal (Norm), rheumatoid arthritis (RA) and osteoarthritis (OA) patients, determined by von Frey monofilament testing. The RA and OA groups had significantly higher average mechanical sensation thresholds in both knees. Monofilament diameter scores for each knee were converted to grams per protocol convention for threshold determination. Average and standard error mechanical sensation scores for both knees and for the most symptomatic (worst) knee are demonstrated. * P < 0.05 when compared to normal controls, analyzed by paired and unpaired Student t-tests. (B) Mechanical pain threshold scores (g) for Norm, RA and OA patients, determined by von Frey monofilament testing (see A). The average pain threshold for both knees and for the most painful (worst) knee was significantly lower in RA patients than in the Norm group. The average pain threshold for both knees and for the most painful knee in OA patients was significantly lower than in the Norm group. * P < 0.05 when compared to normal controls, analyzed by paired and unpaired Student t-tests. Reprinted from [59], Copyright 2003, with permission from Elsevier.
Range of motion and stiffness
An ultrasonic device has been used to measure the position of external markers attached to anatomical reference points of the legs in the pendulum test of Wartenberg [60]. Patients with rheumatoid arthritis show increased knee stiffness (damping ratio) and reduced maximal amplitude of flexion and extension. Reduced range of motion has also been measured in patients with knee osteoarthritis [61].
Weight bearing and gait analysis
In patients with knee osteoarthritis, the percentage of pressure on forefoot and hindfoot (static pedobarography) and the peak pressures on forefoot, midfoot, and hindfoot (dynamic pedobarography) have been measured using a force platform with independent pressure-measuring cells [62]. Analysis of the pressure map showed that the percentage of hindfoot pressure during standing and peak pressure of the forefoot during walking are lower in patients with osteoarthritis, reflecting weight bearing changes. Spatiotemporal and kinematic data of patients with knee osteoarthritis have been obtained using a computerized gait analysis system with video cameras [63]. External reflective markers are placed on anatomical reference points of the legs to determine the limb position, and two force plates measure ground reaction forces. In the osteoarthritis group, walking velocity, cadence (steps/min) and stride length are reduced, stride time and double support time are increased, and the overall stance phase is prolonged. Knee flexion during stance and swing phases is reduced. Extensor and flexor moments (Nm/kg) are also altered and the peak values of ground reaction forces are lower, suggesting gait changes in osteoarthritis patients.
Pain assessment in self-report questionnaires
The Visual Analog Scale (VAS) has been used in patients with osteoarthritis and rheumatoid arthritis affecting the knee [59]. Other pain scales include numeric rating scales and the Neuropathic Pain Scale (NPS) for osteoarthritis [64]. The McGill Pain Questionaire (MPQ) uses word descriptors (sensory, affective and evaluative) and an intensity scale to generate three pain scores, the pain rating index, number of words chosen and Present Pain Intensity (PPI) index [65]. The Short-Form McGill Pain Questionnaire (SF-MPQ) includes sensory and affective descriptors, which are rated on an intensity scale to generate three pain scores (sensory, affective and total). The SF-MPQ also includes the PPI index of the standard MPQ and a VAS [66]. MPQ and SF-MPQ have been used for pain assessment in patients with arthritis.
The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) is one of the most commonly used measures of pain and physical disability in patients with osteoarthritis of the hip and/or knee [67, 68]. Its reliability and validity have been demonstrated in a range of patient groups and interventions. The WOMAC evaluates three dimensions (pain, stiffness and physical function) using a numeric rating scale (Likert version) or VAS. In addition to the score of each subscale, an index score or global score is calculated.
The Brief Pain Inventory (BPI) is an established tool for the assessment of cancer pain and has recently also been used in patients with osteoarthritis [69]. The BPI includes two numerical rating scales that assess the severity of pain and the impact of pain on daily functions (interference). The four-item severity subscale asks patients to rate their worst pain, least pain, average pain over the previous 24 hours, and pain right now. The seven-item interference subscale of the BPI assesses general activity, walking ability, normal work, mood, sleep, relations with people, and enjoyment of life. A modified BPI short form assesses three pain severity items (worst pain, pain on the average, and pain right now) and five interference items (walking ability, mood, sleep, relations with others, and ability to concentrate) [70].
The Health Assessment Questionnaire (HAQ) and its derivatives have been used in patients of osteoarthritis and rheumatoid arthritis as a predictor of functional and work disability, costs, joint replacement surgery, and mortality [71, 72]. The full HAQ assesses five dimensions (disability, pain, medication effects, costs of care, and mortality) with a scale of 20 activities of daily living (ADL) in eight categories and a VAS for pain. The short HAQ contains only the HAQ Disability Index (HAQ-DI) and the patient global and pain visual analog scales (VAS). Several modifications of the HAQ have been developed [58]. The multidimensional HAQ (MDHAQ) includes additional ADL and three psychological items concerning sleep, anxiety and depression. The clinical HAQ (CLINHAQ) includes anxiety and depression scales, a pain diagram, fatigue scale and other scales.
The Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36) is a generic, non-disease-specific questionnaire, which includes eight scales that assess limitations in physical activities, limitations in social activities, limitations in usual role activities because of physical problems, pain, general mental health (psychological distress and well-being), limitations in usual role activities because of emotional problems, vitality (energy and fatigue), and general health perceptions [73]. The Arthritis-Specific Health Index (ASHI) for the SF-36 includes the eight-scale SF-36 and five arthritis-specific measures of knee pain on weight bearing, time to walk 50 feet, physician global evaluation of symptom severity and impact, patient global evaluation of symptom severity and impact, and pain intensity VAS [74]. The ASHI has been used in patients with osteoarthritis and rheumatoid arthritis.
The Disease Activity Score (DAS) and its modified version including 28 joint count (DAS28) have been developed to measure disease activity in patients with rheumatoid arthritis [75]. The DAS provides an absolute number that can be compared to other patients and to past and future scores in the same patient. Measures include a swollen joint count, tender joint count, acute-phase reactant (erythrocyte sedimentation rate or C-reactive protein), and patient assessment of global status. Pain assessment in the DAS is only indirect via the global status assessment.
Conclusion
Animal models of different forms of arthritis have been developed for the assessment of knee joint pain. Limitations of their ability to mimic fully a condition as complex as arthritis in humans need to be considered carefully. Measurements of knee joint pain associated with arthritis in animal models include indirect (weight bearing, gait analysis, spontaneous mobility, and sensitivity of the paw to von Frey filaments or heat) and more direct measurements (probing the sensitivity of the knee, knee extension angle, and vocalizations evoked by stimulation of the knee). In patients with knee joint osteoarthritis or rheumatoid arthritis, physical measures include testing the mechanosensitivity of the knee, range of motion, weight bearing and gait analysis, whereas frequently used patient self-report questionnaires for pain assessment include the VAS and other rating scales, MPQ, WOMAC, BPI, HAQ, SF-36, and DAS.
Abbreviations
- ADL:
-
activities of daily living
- ASHI:
-
Arthritis-Specific Health Index for the SF-36
- CIA:
-
collagen-induced arthritis
- CFA:
-
complete Freund's adjuvant
- CLINHAQ:
-
clinical HAQ
- DAS:
-
Disease Activity Score
- HAQ:
-
Health Assessment Questionnaire
- HAQ-DI:
-
Health Assessment Questionnaire Disability Index
- K/C:
-
kaolin-carrageenan
- MDHAQ:
-
multidimensional HAQ
- MIA:
-
monosodium iodoacetate
- MPQ:
-
McGill Pain Questionaire
- NPS:
-
Neuropathic Pain Scale
- PPI:
-
Present Pain Intensity
- PWL:
-
paw withdrawal latency
- PWT:
-
paw withdrawal threshold
- SF-36:
-
Medical Outcomes Study 36-Item Short-Form Health Survey
- SF-MPQ:
-
Short-Form McGill Pain Questionnaire
- VAD:
-
vocalization afterdischarge
- VAS:
-
Visual Analog Scale
- VDS:
-
vocalization during stimulation
- WOMAC:
-
Western Ontario and McMaster Universities Osteoarthritis Index
References
Ashburn MA: Guideline for the management of pain in osteoarthritis, rheumatoid arthritis, and juvenile chronic arthritis. Edited by: Ashburn MA. Glenview, IL, American Pain Society; 2002:1–178.
National Institute of Arthritis and Musculoskeletal and Skin Diseases (NIAMS): Arthritis and Rheumatic Diseases. NIH Publication No. 02–4999; 2002.
Schaible HG, Grubb BD: Afferent and spinal mechanisms of joint pain. Pain 1993, 55: 5–54. 10.1016/0304-3959(93)90183-P
Schaible HG, Ebersberger A, von Banchet GS: Mechanisms of pain in arthritis. Ann N Y Acad Sci 2002, 966: 343–354.
Iwata K, Tashiro A, Tsuboi Y, Imai T, Sumino R, Morimoto T, Dubner R, Ren K: Medullary dorsal horn neuronal activity in rats with persistent temporomandibular joint and perioral inflammation. J Neurophysiol 1999, 82: 1244–1253.
Ren K, Dubner R: Descending modulation in persistent pain: an update. Pain 2002, 100: 1–6. 10.1016/S0304-3959(02)00368-8
Guilbaud G, Benoist JM, Eschalier A, Kayser V, Gautron M, Attal N: Evidence for central phenomena participating in the changes of responses of ventrobasal thalamic neurons in arthritic rats. Brain Res 1989, 484: 383–388. 10.1016/0006-8993(89)90386-7
Lamour Y, Guilbaud G, Willer JC: Altered properties and laminar distribution of neuronal responses to peripheral stimulation in the SmI cortex of the arthritic rat. Brain Res 1983, 273: 183–187. 10.1016/0006-8993(83)91111-3
Neugebauer V, Li W, Bird GC, Han JS: The amygdala and persistent pain. The Neuroscientist 2004, 10: 221–234. 10.1177/1073858403261077
Bendele A, McComb J, Gould T, McAbee T, Sennello G, Chlipala E, Guy M: Animal models of arthritis: relevance to human disease. Toxicol Pathol 1999, 27: 134–142.
Kidd BL: Osteoarthritis and joint pain. Pain 2006, 123: 6–9. 10.1016/j.pain.2006.04.009
Bendele AM: Animal models of osteoarthritis. J Musculoskelet Neuronal Interact 2001, 1: 363–376.
Pomonis JD, Boulet JM, Gottshall SL, Phillips S, Sellers R, Bunton T, Walker K: Development and pharmacological characterization of a rat model of osteoarthritis pain. Pain 2005, 114: 339–346. 10.1016/j.pain.2004.11.008
Fernihough J, Gentry C, Malcangio M, Fox A, Rediske J, Pellas T, Kidd B, Bevan S, Winter J: Pain related behaviour in two models of osteoarthritis in the rat knee. Pain 2004, 112: 83–93. 10.1016/j.pain.2004.08.004
Bendele A: Animal models of rheumatoid arthritis. J Musculoskelet Neuronal Interact 2001, 1: 377–385.
Levine JD, Goetzl EJ, Basbaum AI: Contribution of the nervous system to the pathophysiology of rheumatoid arthritis and other polyarthritides. Rheum Dis Clin North Am 1987, 13: 369–383.
Ventura-Martinez R, ciga-Campos M, az-Reval MI, Gonzalez-Trujano ME, Lopez-Munoz FJ: Peripheral involvement of the nitric oxide-cGMP pathway in the indomethacin-induced antinociception in rat. Eur J Pharmacol 2004, 503: 43–48. 10.1016/j.ejphar.2004.09.018
Meiner SE: Gouty arthritis: not just a big toe problem. Geriatr Nurs 2001, 22: 132–134. 10.1067/mgn.2001.116378
Kobayashi K, Imaizumi R, Sumichika H, Tanaka H, Goda M, Fukunari A, Komatsu H: Sodium iodoacetate-induced experimental osteoarthritis and associated pain model in rats. J Vet Med Sci 2003, 65: 1195–1199. 10.1292/jvms.65.1195
Hong Y, Ji H, Wei H: Topical ketanserin attenuates hyperalgesia and inflammation in arthritis in rats. Pain 2006, 124: 27–33. 10.1016/j.pain.2006.03.010
Neugebauer V, Schaible HG: Evidence for a central component in the sensitization of spinal neurons with joint input during development of acute arthritis in cat's knee. J Neurophysiol 1990, 64: 299–311.
Neugebauer V, Lucke T, Schaible HG: N-methyl-D-aspartate (NMDA) and non-NMDA receptor antagonists block the hyperexcitability of dorsal horn neurons during development of acute arthritis in rat's knee joint. J Neurophysiol 1993, 70: 1365–1377.
Dougherty PM, Sluka KA, Sorkin LS, Westlund KN, Willis WD: Neural changes in acute arthritis in monkeys. I. Parallel enhancement of responses of spinothalamic tract neurons to mechanical stimulation and excitatory amino acids. Brain Res Brain Res Rev 1992, 17: 1–13. 10.1016/0165-0173(92)90002-4
Sluka KA, Westlund KN: Behavioral and immunohistochemical changes in an experimental arthritis model in rats. Pain 1993, 55: 367–377. 10.1016/0304-3959(93)90013-F
Zhang L, Hoff AO, Wimalawansa SJ, Cote GJ, Gagel RF, Westlund KN: Arthritic calcitonin/[alpha] calcitonin gene-related peptide knockout mice have reduced nociceptive hypersensitivity. Pain 2001, 89: 265–273. 10.1016/S0304-3959(00)00378-X
Min SS, Han JS, Kim YI, Na HS, Yoon YW, Hong SK, Han HC: A novel method for convenient assessment of arthritic pain in voluntarily walking rats. Neurosci Lett 2001, 308: 95–98. 10.1016/S0304-3940(01)01983-8
Tonussi CR, Ferreira SH: Rat knee-joint carrageenin incapacitation test: an objective screen for central and peripheral analgesics. Pain 1992, 48: 421–427. 10.1016/0304-3959(92)90095-S
Gaitan G, Herrero JF: Subanalgesic doses of dexketoprofen and HCT-2037 (nitrodexketoprofen) enhance fentanyl antinociception in monoarthritic rats. Pharmacol Biochem Behav 2005, 80: 327–332. 10.1016/j.pbb.2004.12.004
Oh JH, Bai SJ, Cho ZH, Han HC, Min SS, Shim I, Lee HJ, Lee H, Lee BH: Pain-relieving effects of acupuncture and electroacupuncture in an animal model of arthritic pain. Int J Neurosci 2006, 116: 1139–1156.
Penido C, Conte FP, Chagas MS, Rodrigues CA, Pereira JF, Henriques MG: Antiinflammatory effects of natural tetranortriterpenoids isolated from Carapa guianensis Aublet on zymosan-induced arthritis in mice. Inflamm Res 2006, 55: 457–464. 10.1007/s00011-006-5161-8
van de Loo FA, Bennink MB, Arntz OJ, Smeets RL, Lubberts E, Joosten LA, van Lent PL, Coenen-de Roo CJ, Cuzzocrea S, Segal BH, Holland SM, van den Berg WB: Deficiency of NADPH oxidase components p47phox and gp91phox caused granulomatous synovitis and increased connective tissue destruction in experimental arthritis models. Am J Pathol 2003, 163: 1525–1537.
JC SR, Peixoto ME, Jancar S, de QC, de AR, da Rocha FA: Dual effect of nitric oxide in articular inflammatory pain in zymosan-induced arthritis in rats. Br J Pharmacol 2002, 136: 588–596. 10.1038/sj.bjp.0704755
Yu YC, Koo ST, Kim CH, Lyu Y, Grady JJ, Chung JM: Two variables that can be used as pain indices in experimental animal models of arthritis. Journal of Neuroscience Methods 2002, 115: 107–113. 10.1016/S0165-0270(02)00011-0
McDougall JJ, Barin AK, McDougall CM: Loss of vasomotor responsiveness to the mu-opioid receptor ligand endomorphin-1 in adjuvant monoarthritic rat knee joints. Am J Physiol Regul Integr Comp Physiol 2004, 286: R634-R641.
Seino D, Tokunaga A, Tachibana T, Yoshiya S, Dai Y, Obata K, Yamanaka H, Kobayashi K, Noguchi K: The role of ERK signaling and the P2X receptor on mechanical pain evoked by movement of inflamed knee joint. Pain 2006, 123: 193–203. 10.1016/j.pain.2006.02.032
Staton PC, Wilson AW, Bountra C, Chessell IP, Day NC: Changes in dorsal root ganglion CGRP expression in a chronic inflammatory model of the rat knee joint: Differential modulation by rofecoxib and paracetamol. Eur J Pain 2006.
Gauldie SD, McQueen DS, Clarke CJ, Chessell IP: A robust model of adjuvant-induced chronic unilateral arthritis in two mouse strains. J Neurosci Methods 2004, 139: 281–291. 10.1016/j.jneumeth.2004.05.003
Holmdahl R, Lorentzen JC, Lu S, Olofsson P, Wester L, Holmberg J, Pettersson U: Arthritis induced in rats with nonimmunogenic adjuvants as models for rheumatoid arthritis. Immunol Rev 2001, 184: 184–202. 10.1034/j.1600-065x.2001.1840117.x
Cai X, Wong YF, Zhou H, Xie Y, Liu ZQ, Jiang ZH, Bian ZX, Xu HX, Liu L: The comparative study of Sprague-Dawley and Lewis rats in adjuvant-induced arthritis. Naunyn Schmiedebergs Arch Pharmacol 2006.
Cuzzocrea S, Mazzon E, Bevilaqua C, Costantino G, Britti D, Mazzullo G, De SA, Caputi AP: Cloricromene, a coumarine derivative, protects against collagen-induced arthritis in Lewis rats. Br J Pharmacol 2000, 131: 1399–1407. 10.1038/sj.bjp.0703695
Stuart JM, Townes AS, Kang AH: Type II collagen-induced arthritis. Ann N Y Acad Sci 1985, 460: 355–362. 10.1111/j.1749-6632.1985.tb51182.x
Saadat F, Cuzzocrea S, Di PR, Pezeshki M, Khorramizadeh MR, Sedaghat M, Razavi A, Mirshafiey A: Effect of pyrimethamine in experimental rheumatoid arthritis. Med Sci Monit 2005, 11: BR293-BR299.
Otsuki T, Nakahama H, Niizuma H, Suzuki J: Evaluation of the analgesic effects of capsaicin using a new rat model for tonic pain. Brain Res 1986, 365: 235–240. 10.1016/0006-8993(86)91634-3
Schott E, Berge OG, ngeby-Moller K, Hammarstrom G, Dalsgaard CJ, Brodin E: Weight bearing as an objective measure of arthritic pain in the rat. J Pharmacol Toxicol Methods 1994, 31: 79–83. 10.1016/1056-8719(94)90046-9
McDougall JJ, Watkins L, Li Z: Vasoactive intestinal peptide (VIP) is a modulator of joint pain in a rat model of osteoarthritis. Pain 2006, 123: 98–105. 10.1016/j.pain.2006.02.015
Combe R, Bramwell S, Field MJ: The monosodium iodoacetate model of osteoarthritis: a model of chronic nociceptive pain in rats? Neurosci Lett 2004, 370: 236–240. 10.1016/j.neulet.2004.08.023
Sluka KA, Milton MA, Willis WD, Westlund KN: Differential roles of neurokinin 1 and neurokinin 2 receptors in the development and maintenance of heat hyperalgesia induced by acute inflammation. Br J Pharmacol 1997, 120: 1263–1273. 10.1038/sj.bjp.0701044
Clarke KA, Heitmeyer SA, Smith AG, Taiwo YO: Gait analysis in a rat model of osteoarthrosis. Physiol Behav 1997, 62: 951–954. 10.1016/S0031-9384(97)00022-X
Rocha FA, Aragao AG Jr., Oliveira RC, Pompeu MM, Vale MR, Ribeiro RA: Periarthritis promotes gait disturbance in zymosan-induced arthritis in rats. Inflamm Res 1999, 48: 485–490. 10.1007/s000110050491
Gegout-Pottie P, Philippe L, Simonin MA, Guingamp C, Gillet P, Netter P, Terlain B: Biotelemetry: an original approach to experimental models of inflammation. Inflamm Res 1999, 48: 417–424. 10.1007/s000110050481
Han JS, Bird GC, Li W, Neugebauer V: Computerized analysis of audible and ultrasonic vocalizations of rats as a standardized measure of pain-related behavior. Neurosci Meth 2005, 141: 261–269. 10.1016/j.jneumeth.2004.07.005
Sluka KA, Skyba DA, Radhakrishnan R, Leeper BJ, Wright A: Joint mobilization reduces hyperalgesia associated with chronic muscle and joint inflammation in rats. J Pain 2006, 7: 602–607. 10.1016/j.jpain.2006.02.009
Skyba DA, Radhakrishnan R, Sluka KA: Characterization of a method for measuring primary hyperalgesia of deep somatic tissue. J Pain 2005, 6: 41–47. 10.1016/j.jpain.2004.10.002
Han JS, Neugebauer V: mGluR1 and mGluR5 antagonists in the amygdala inhibit different components of audible and ultrasonic vocalizations in a model of arthritic pain. Pain 2005, 113: 211–222. 10.1016/j.pain.2004.10.022
Bove SE, Calcaterra SL, Brooker RM, Huber CM, Guzman RE, Juneau PL, Schrier DJ, Kilgore KS: Weight bearing as a measure of disease progression and efficacy of anti-inflammatory compounds in a model of monosodium iodoacetate-induced osteoarthritis. Osteoarthritis Cartilage 2003, 11: 821–830. 10.1016/S1063-4584(03)00163-8
Bove SE, Laemont KD, Brooker RM, Osborn MN, Sanchez BM, Guzman RE, Hook KE, Juneau PL, Connor JR, Kilgore KS: Surgically induced osteoarthritis in the rat results in the development of both osteoarthritis-like joint pain and secondary hyperalgesia. Osteoarthritis Cartilage 2006, 14: 1041–1048. 10.1016/j.joca.2006.05.001
Vrinten DH, Hamers FF: 'CatWalk' automated quantitative gait analysis as a novel method to assess mechanical allodynia in the rat; a comparison with von Frey testing. Pain 2003, 102: 203–209. 10.1016/s0304-3959(02)00382-2
Pincus T, Sokka T: Quantitative measures and indices to assess rheumatoid arthritis in clinical trials and clinical care. Rheum Dis Clin North Am 2004, 30: 725–51, vi. 10.1016/j.rdc.2004.08.001
Hendiani JA, Westlund KN, Lawand N, Goel N, Lisse J, McNearney T: Mechanical sensation and pain thresholds in patients with chronic arthropathies. J Pain 2003, 4: 203–211. 10.1016/S1526-5900(03)00557-1
Valle MS, Casabona A, Sgarlata R, Garozzo R, Vinci M, Cioni M: The pendulum test as a tool to evaluate passive knee stiffness and viscosity of patients with rheumatoid arthritis. BMC Musculoskelet Disord 2006, 7: 89. 10.1186/1471-2474-7-89
Johnson SR, Archibald A, Davis AM, Badley E, Wright JG, Hawker GA: Is Self-Reported Improvement in Osteoarthritis Pain and Disability Reflected in Objective Measures? J Rheumatol 2006.
Kul-Panza E, Berker N: Pedobarographic findings in patients with knee osteoarthritis. Am J Phys Med Rehabil 2006, 85: 228–233. 10.1097/01.phm.0000200377.52610.cd
Gok H, Ergin S, Yavuzer G: Kinetic and kinematic characteristics of gait in patients with medial knee arthrosis. Acta Orthop Scand 2002, 73: 647–652. 10.1080/000164702321039606
Jensen MP, Dworkin RH, Gammaitoni AR, Olaleye DO, Oleka N, Galer BS: Assessment of pain quality in chronic neuropathic and nociceptive pain clinical trials with the Neuropathic Pain Scale. J Pain 2005, 6: 98–106. 10.1016/j.jpain.2004.11.002
Melzack R: The McGill Pain Questionnaire: major properties and scoring methods. Pain 1975, 1: 277–299. 10.1016/0304-3959(75)90044-5
Melzack R: The short-form McGill Pain Questionnaire. Pain 1987, 30: 191–197. 10.1016/0304-3959(87)91074-8
McConnell S, Kolopack P, Davis AM: The Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC): a review of its utility and measurement properties. Arthritis Rheum 2001, 45: 453–461. Publisher Full Text 10.1002/1529-0131(200110)45:5%3C453::AID-ART365%3E3.0.CO;2-W
Bellamy N: WOMAC: a 20-year experiential review of a patient-centered self-reported health status questionnaire. J Rheumatol 2002, 29: 2473–2476.
Williams VS, Smith MY, Fehnel SE: The validity and utility of the BPI interference measures for evaluating the impact of osteoarthritic pain. J Pain Symptom Manage 2006, 31: 48–57. 10.1016/j.jpainsymman.2005.06.008
Mendoza T, Mayne T, Rublee D, Cleeland C: Reliability and validity of a modified Brief Pain Inventory short form in patients with osteoarthritis. Eur J Pain 2006, 10: 353–361. 10.1016/j.ejpain.2005.06.002
Bruce B, Fries JF: The Health Assessment Questionnaire (HAQ). Clin Exp Rheumatol 2005, 23: S14-S18.
Yazici Y: Monitoring outcomes of arthritis and longitudinal data collection using patient questionnaires in routine care. Bull Hosp Jt Dis 2006, 64: 40–44.
Ware JE Jr., Sherbourne CD: The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care 1992, 30: 473–483. 10.1097/00005650-199206000-00002
Ware JE Jr., Keller SD, Hatoum HT, Kong SX: The SF-36 Arthritis-Specific Health Index (ASHI): I. Development and cross-validation of scoring algorithms. Med Care 1999, 37: MS40-MS50. 10.1097/00005650-199905001-00004
Pincus T: The DAS is the most specific measure, but a patient questionnaire is the most informative measure to assess rheumatoid arthritis. J Rheumatol 2006, 33: 834–837.
Acknowledgements
The authors' work is supported by NIH grants NS38261 and NS11255. We would like to thank Drs. Richard E. Coggeshall and William D. Willis for their critical reading of and valuable comments on this manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
VN and JSH hold a patent relating to the vocalization measurements in animals (U.S. Patent Application 98006/28). However, no royalties are being received and no financial gains are expected.
Authors' contributions
VN reviewed the literature, gathered background information, and wrote the article. JSH, HA, GJ and YF assisted with literature review and conducted the behavioral experiments in Dr. Neugebauer's laboratory as described in this article.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Neugebauer, V., Han, J.S., Adwanikar, H. et al. Techniques for assessing knee joint pain in arthritis. Mol Pain 3, 8 (2007). https://doi.org/10.1186/1744-8069-3-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1744-8069-3-8