
Abstract
Background
The beneficial effects of omega-3 polyunsaturated fatty acids (n-3 PUFAs), especially in dyslipidemic subjects with a high risk of cardiovascular disease, are widely described in the literature. A lot of effects of n-3 PUFAs and their oxidized metabolites are triggered by regulating the expression of genes. Currently, it is uncertain if the administration of n-3 PUFAs results in different expression changes of genes related to antioxidative mechanisms in normo- and dyslipidemic subjects, which may partly explain their cardioprotective effects. The aim of this study was to investigate the effects of n-3 PUFA supplementation on expression changes of genes involved in oxidative processes.
Methods
Ten normo- and ten dyslipidemic men were supplemented for twelve weeks with fish oil capsules, providing 1.14 g docosahexaenoic acid and 1.56 g eicosapentaenoic acid. Gene expression levels were determined by whole genome microarray analysis and quantitative real-time polymerase chain reaction (qRT-PCR).
Results
Using microarrays, we discovered an increased expression of antioxidative enzymes and a decreased expression of pro-oxidative and tissue enzymes, such as cytochrome P450 enzymes and matrix metalloproteinases, in both normo- and dyslipidemic men. An up-regulation of catalase and heme oxigenase 2 in both normo- and dyslipidemic subjects and an up-regulation of cytochrome P450 enzyme 1A2 only in dyslipidemic subjects could be observed by qRT-PCR analysis.
Conclusions
Supplementation of normo- and dyslipidemic subjects with n-3 PUFAs changed the expression of genes related to oxidative processes, which may suggest antioxidative and potential cardioprotective effects of n-3 PUFAs. Further studies combining genetic and metabolic endpoints are needed to verify the regulative effects of n-3 PUFAs in antioxidative gene expression to better understand their beneficial effects in health and disease prevention.
Trial registration
ClinicalTrials.gov (ID: NCT01089231)
Similar content being viewed by others

Background
Cardiovascular disease (CVD) is the leading cause of morbidity and mortality in Europe, and frequently appears in subjects with disorders of lipid metabolism. Evidence of an association between dyslipidemia and increased oxidative stress [1, 2], as well as between increased oxidative stress and the pathogenesis of CVD, are given by many studies [3–7]. These associations indicate that dyslipidemia increases oxidative stress, and thus promotes the pathogenesis of CVD.
Enhanced oxidative stress results from either an overproduction of reactive oxygen species (ROS) or a decreased antioxidative defence system. The most important ROS producers are nicotinamide adenine dinucleotide phosphate oxidase [8], xanthine oxidase [9], uncoupled endothelial nitric oxide synthase [10], and enzymes of the arachidonic acid (AA, 20:4n-6) metabolism and the mitochondria [11]. The consequences of an increased ROS production in CVD are vascular cell dysfunction [12], increased growth of the myocard, apoptosis [13], and cardiac remodelling via activation of matrix metalloproteinases (MMP) [14].
The human body possess enzymatic and non-enzymatic strategies to compensate oxidative damage and protect itself against such cytotoxic effects. Important antioxidative enzymes include catalase (CAT), superoxide dismutase (SOD), heme oxygenase (HMOX), and glutathione peroxidase (GPX). Non-enzymatic antioxidants, such as glutathione, ascorbate and α-tocopherol, are also important regulators of the oxidative status. In the last few decades, numerous observational and intervention studies have shown the beneficial effects of fish oil (FO) and its principal omega-3 polyunsaturated fatty acids (n-3 PUFAs), eicosapentaenoic acid (EPA, 20:5n-3) and docosahexaenoic acid (DHA, 22:6n-3), in the prevention of atherosclerosis and CVD [15–17]. Beyond the beneficial effects of n-3 PUFAs on the lipid profile [18–20], especially in subjects with hypertriglyceridemia [21–23], n-3 PUFAs appear to increase antioxidative capacity and thus reduce oxidative stress [24, 25]. However, the effects of n-3 PUFAs on oxidative stress have not been studied in detail and some existing results are inconsistent. Investigations in patients with chronic renal failure showed reduced oxidative stress after n-3 PUFA supplementation [24]. Furthermore, in vitro studies with human aortic endothelial and HepG2 cells also determined reduced oxidative stress after n-3 PUFA treatment [25]. However, an indication of increased oxidative stress in healthy judo athletes after n-3 PUFA supplementation was observed [26]. The underlying molecular mechanisms by which EPA and DHA influence oxidative stress are not completely understood. Changes in expression levels of antioxidative genes in response to FO supplementation have not been investigated in dyslipidemic subjects so far. In regard to the fact that dyslipidemia increases oxidative stress and that dyslipidemic subjects possess a pro-oxidant status [27, 28], we hypothesised that n-3 PUFAs show their potential antioxidative effects especially in dyslipidemic subjects. Therefore, this intervention trial aimed to investigate the expression changes of oxidative stress-related genes in normo- and dyslipidemic subjects after FO supplementation to gain information about the potential antioxidative effects of n-3 PUFAs.
Methods
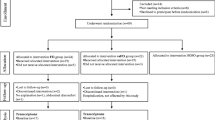
This study focused on changes in oxidative stress-related genes as part of a trial investigating the effects of FO supplementation on whole-genome gene expression profiles in normo- and dyslipidemic men. The randomized, controlled, parallel intervention study was conducted at the Institute of Food Science and Human Nutrition at the Leibniz University of Hannover in Germany, and was designed and performed according to the principles of the Good Clinical Practice Guidelines laid down in the Declaration of Helsinki. It was approved by the Freiburg International Ethical Commission and registered at ClinicalTrials.gov (ID: NCT01089231).
Subjects
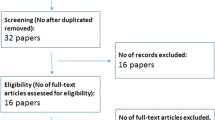
Normo- and dyslipidemic men were recruited by several advertisements and study placards in Hannover. The suitability of volunteers was checked in telephone interviews and by diet, lifestyle and disease questionnaires. Exclusion criteria comprised smoking; body mass index > 35; intake of any corticosteroids, lipid-lowering or anti-inflammatory drugs; diagnosed chronically cardiovascular or liver diseases; gastrointestinal disorders; blood coagulation disorders and intake of coagulation-inhibiting drugs; renal failure; periodic intake of laxatives; ingestion of supplements enriched with n-3 PUFAs, phytosterols, polyglucosamines, other lipid-binding ingredients or daily eating of fatty fish; allergy to fish or FO; and participation in another clinical study < 30 days before the start of the study or at the same time. Selected subjects were invited for a screening examination to collect fasting blood and determine serum lipid levels. Among these subjects, ten normolipidemic (total cholesterol (TC) < 200 mg/dl; low density lipoprotein cholesterol (LDL-C) < 130 mg/dl; triacyltriglyceride (TG) < 150 mg/dl) and ten dyslipidemic (TC > 200 mg/dl; LDL-C > 130 mg/dl; TG > 150 mg/ml) men, aged between 29 and 51 years, were enrolled in the study population. All participants included gave their written informed consent to take part in the study. The study protocol was approved by the Freiburger ethics committee.
Study design
The normo- and dyslipidemic subjects each ingested six FO capsules per day for a period of twelve weeks. The daily n-3 PUFA intake for each subject via FO capsules was 2.7 g (1.14 g DHA and 1.56 g EPA). The subjects were instructed to take the capsules together with food, three in the morning and three in the evening, and to maintain their usual exercise and dietary habits throughout the intervention time. As an exception, on the first intervention day, all six capsules were ingested at the same time in the morning after a standardised breakfast. Additionally, participants completed a questionnaire to obtain information about changes in medication, diet (e.g. changes in weekly fish intake, preferred fish dishes or species, respectively) and lifestyle habits (e.g. physical activity), as well as the tolerability of the capsules.
Determination of red blood cell membrane fatty acid composition
Fasting venous blood samples were collected into BD Vacutainer® Blood Collection Tubes (Becton Dickinson, Heidelberg, Germany). Red blood cell (RBC) membrane fatty acid (FA) composition, including the omega-3 index (EPA + DHA levels in RBC membranes), was analysed at baseline (t0) and after twelve weeks of supplementation with FO (t12), according to the omega-3 index methodology [29]. Accordingly, the RBCs were first transesterificated, resulting in a generation of FA methyl esters, followed by gas chromatography analysis using a GC2010 Gas Chromatograph (Shimadzu, Freising, Germany) equipped with a SP2560, 100 m column (Supelco, Bellefonte, PA) using hydrogen as the carrier gas. Identification of the FAs was enabled by comparison with a standard mixture of the FAs characteristic for RBCs. The results are presented as a percentage of the total FAs identified. The analytical coefficient of variation for EPA and DHA was 5%. Quality was assured according to DIN ISO 15189.
Gene expression analyses
Sample collection
Fasting venous blood samples were collected in PAXgene Blood RNA Tubes (PreAnalytiX, Hombrechtikon, Switzerland) at baseline (t0), after one week (t1) and after twelve weeks (t12) of supplementation to analyse medium- and long-term effects of the FO supplementation on gene expression regulation. For short-term effects, venous blood samples were collected four hours (t4h) after the first intake of the capsules. The whole blood samples were collected and incubated for 24 hours in the PAXgene Blood RNA Tubes at room temperature. Whole blood samples were used for the RNA isolation and examination of gene expression because cell fractioning steps, such as lymphocyte isolation, could alter the gene expression pattern [30].
Total RNA isolation from human whole blood, RNA purification and sample pooling
The total RNA was isolated with the PAXgene Blood RNA Kit (PreAnalytiX, Hombrechtikon, Switzerland), according to the manufacturer’s recommended procedures. The RNA yield was quantified by Nanodrop ND-1000 spectrophotometer (peQLab Biotechnologie GmbH, Erlangen, Germany) measurement. The total RNA was purified with the Globin Clear Kit (Ambion, Applied Biosystems, Darmstadt, Germany), according to the manufacturer’s instructions. The reduction of highly abundant globin mRNA transcripts in whole blood samples is necessary to enable the detection of low-abundance transcripts [31]. The purified RNA was quantified again, and the quality was measured with an Agilent 2100 Bioanalyzer using RNA 6000 Nano Chips and a RNA 6000 Nano Kit (Agilent Technologies, Böblingen, Germany).
Equal amounts of purified RNA samples from each member of the respective group were pooled together. This was done for all different time points (t0, t4h, t1, and t12). Therefore, four pool samples were generated by this process for each group. The approach of sample pooling was chosen to reduce biological inter-individual variability, which is frequent due to variations in the relative proportions of specific blood cell subsets, gender, age, and disease state [32].
Microarray analysis (cDNA synthesis, hybridisation and data analysis)
First-strand cDNA synthesis and tyramide signal amplification (TSA) was performed using the Micromax TSA Labelling and Detection Kit (Perkin Elmer Life Sciences, Rodgau, Germany) with several protocol modifications. A total amount of 6 μg from every RNA pool, as well as random hexamer primer (Fermentas, St. Leon-Rot, Germany) and oligo(dT) primer (Roth, Karlsruhe, Germany), were used for the cDNA synthesis, which was facilitated by using Superskript III reverse transcriptase (Invitrogen, Karlsruhe, Germany). The incubation time of two hours was split into two one-hour incubations and additional Superskript III was added after the first hour. Each RNA pool was synthesized into two differently labelled cDNAs, fluorescein-labelled and biotin-labelled cDNA.
After labelling, the cDNA samples were purified with the QIAquick PCR Purification Kit (Qiagen, Hilden, Germany), according to the manufacturer’s instructions. Furthermore, the cDNA samples were first vacuum-dried and then resolved in hybridization buffer (4 x SSPE; 2.5 x Denhardt’s reagent; 30% formamid). After a final degradation step (3 minutes, 95°C), one-tenth of top-block (Sigma-Aldrich, Steinheim, Germany) was added. Equal amounts of biotin-labelled and fluorescein-labelled cDNA were hybridized simultaneously in oneexperiment to human whole genome OneArray™ Microarrays (Phalanx Biotech Group; Belmont, CA, USA). Hybridizations were carried out overnight at 42°C in hybridization chambers (Eppendorf AG, Hamburg, Germany). After hybridization, unbound and non-specific fixed cDNA was removed by stringent washing from the array. Specifically bound fluorescein- and biotin-labelled cDNA were sequentially detected with a series of conjugate reporter molecules according to the TSA process, ultimately with tyramide-Cy3 and tyramideCy5. Microarray experiments were performed for each study group in a loop design to prevent dye-dependent variety effects [33].
The array data were submitted to Gene Expression Omnibus [34], which supports minimum information about a microarray experiment [35]. The accession number of the submitted dataset is GSE34898. Genes that were detected as differentially expressed between baseline and time point t4h, t1 or t12 were subjected to pathway analysis using the Kyoto Encyclopaedia of Genes and Genomes (KEGG) database and GenMAPP [36].
Quantitative real-time polymerase chain reaction (qRT-PCR) and data analysis
In order to quantify the expression levels of selected genes, equal amounts of cDNA were synthesized using 2 μg of purified RNA and M-MLV reverse transcriptase (Promega, Mannheim, Germany), as well as random hexamer (Fermentas, St. Leon-Rot, Germany) and oligo(dT) primers (Carl Roth; Karlsruhe, Germany). Synthesized cDNA was diluted 1:20 with nuclease-free water and used for the qRT-PCR together with iQ SYBR Green Supermix (Bio-Rad Laboratories, Hercules, Ca, USA) and 5 pmol of both forward and reverse primers. The sequences for target and reference genes were retrieved from GenBank and applied primers were manually designed with the Primer-BLAST tool of the National Centre for Biotechnology Information, which is based on the program Primer3 [37]. The primer sequences used are listed in Table 1. Glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and ribosomal protein S2 (RPS2) were identified as the most stable reference genes by the freely available algorithm geNorm version 3.5.
Statistics
Statistical analysis of blood lipids and RBC membrane FAs were processed with SPSS software version 20 (SPSS Inc., Chicago, IL, USA). The results are based on per protocol population, defined as subjects completing all visits not infringing the study protocol, and are presented as mean ± SD. Differences between baseline blood lipid values of both groups were tested by t-test. Differences of FAs in RBC membranes between t0 and t12 were tested within groups by paired t-test. Statistical significance was generally accepted at p ≤ 0.05. The arrays were scanned with a 4000 B scanner (Axon Instruments, Union City, CA, USA) and images were quantified using GenePixPro 6.0 software for the statistical analysis of the microarray data. The average pixel intensity within each spot was determined and a local background was computed for each spot. The net signal was determined by subtracting local background from the average intensity. Signals not consistently detectable (background corrected signal lower than twice background standard deviation) were excluded from further analysis. Following the primary analysis, data from different scans had to be summarized. The scans firstly had to be normalized by the sum of all corresponding spot-intensities due to different laser power and photomultiplier tube settings. Afterwards, data from different scans for each individual spot could be averaged by the mean. The mean of the data for differently labelled targets for each gene on two microarrays was taken. In order to deduce if expression of a gene is significantly different in the two samples, the preprocessed data was analyzed by hypothesis testing. It was assumed that the distribution of the preprocessed data was normal, and hence, a standard two-state pooled-variance t-test (1% and 5% probability of error) was applied in order to detect differentially expressed genes. The genes can be categorized into three groups using the calculated p-value of those t-tests [1: slightly significant regulation (p = 0.05); 2: significant regulation (p < 0.05); 3: highly significant regulation (p < 0.01)].
Statistical analysis of the expression ratios of genes, which were quantified by qRT-PCR, were calculated with the Gene Expression Macro tool (Bio-Rad), which is based on the algorithm of geNorm [38]. Firstly, normalization factors were calculated from the geometric mean of the reference genes GAPDH and RPS2. Furthermore, the baseline values of the normolipidemic group were defined as control values so that relative expression values could be calculated. Therefore, the baseline samples of the normolipidemic group are given a value of 1. Due to the lack of Gene Expression Macro tool to calculate statistics, differences between baseline and endpoint (t12) Ct values were tested by paired t-test using the statistical package R version 2.15.0.
Results
Subject characteristics
All 20 subjects (ten normolipidemic and ten dyslipidemic men) completed the study. No significant differences of the mean age and mean weight were observed between both study groups at baseline. The dyslipidemic subjects presented a 4.47 kg/m² higher BMI, higher TC and TG level, as well as a higher LDL-C/HDL-C quotient, than the normolipidemic subjects (Table 2). Subjects of the dyslipidemic group can be characterised as pre-obese (BMI 25–30), which is, among others, an underlying cause for dyslipidemia. The BMI was not changed by dietary intervention in either study groups (data not shown).
Fatty acid composition of RBC membranes and omega-3 index
No significant differences of EPA or DHA levels in RBC membranes or in the omega-3 index were observed between the study groups at baseline (Table 3). However, dyslipidemic subjects presented lower AA levels in RBC membranes than normolipidemic subjects at baseline. The percentage of EPA and DHA, and the omega-3 index in RBC membranes significantly increased within both study groups after twelve weeks of supplementation. Additionally, the normolipidemic group showed a significant decrease of the percentage of AA in RBC membranes.
Regulation of gene expression by n-3 PUFA supplementation
It was necessary to exclude the RNA samples of one normo- and three dyslipidemic subjects from the microarray experiments and following data analysis due to several reasons: Low RNA yield (three subjects) and consumption of medication that led to exclusion (one subject). Therefore, RNA pools were generated and data was analysed from nine normolipidemic and seven dyslipidemic subjects for each investigation time point.
Microarray experiments showed that several genes related to different oxidative processes were regulated. These genes are listed with the respective regulation ratio for each time point in Table 4. Several enzymes of the glutathione metabolism are regulated after FO supplementation, particularly in dyslipidemic subjects. While genes related to the glutathione synthesis were similarly up- and down-regulated during the first two time points (t4h and t1), these genes were mainly up-regulated after twelve weeks of FO supplementation. Two different glutathione transferases (GST) and glutathione reductase (GR) were up-regulated, whereas glutathione peroxidases were down-regulated in both normo- and dyslipidemic subjects. MMPs were down-regulated in both normolipidemic (MMP25) and dyslipidemic subjects (MMP2, MMP3) after twelve weeks of supplementation. Furthermore, cytochrome P450 (CYP) enzymes were mainly down-regulated after twelve weeks of supplementation, especially in dyslipidemic subjects. Additionally, some antioxidative enzymes, such SOD3, CAT and HMOX2, were up-regulated after twelve weeks of supplementation in dyslipidemic subjects. Moreover, pathway analysis discovered several regulated genes within stress-activated signalling pathways, such as the mitogen-activated protein kinase (MAPK) signalling pathway, the nuclear factor kappa b (NFkB) pathway and the oxidative stress athway (Additional file 1).
Several genes were selected for analyses of gene expression ratios by qRT-PCR, including the two antioxidative enzymes, CAT and HMOX2, and CYP1A2 (Figure 1), a member of the CYP family known to be involved in epoxidation of EPA and DHA [39]. The expression of HMOX2 was significantly up-regulated after FO supplementation over a period of twelve weeks in both normo- and dyslipidemic subjects (p=0.02 and p=0.04). The expression of CAT was also up-regulated, but reached significance only in normolipidemic subjects (p=0.002). The expression of CYP1A2 was significantly up-regulated only in dyslipidemic subjects (p=0.04). The qRT-PCR results mainly confirm the microarray results observed, whereupon differences in the strength of expression occur.

Transcript levels of target genes in normo- and dyslipidemic men. Transcript levels of catalase (CAT), heme oxygenase 2 (HMOX2) and cytochrome P450 enzyme 1 A2 (CYP1A2) was determined by qRT-PCR in normo- and dyslipidemic men before (t0) and after twelve weeks (t12) of fish oil supplementation. Pooled group samples were used in triplicates. Triplicates were averaged and corrected by two reference genes, glyceraldehyde-3-phosphate dehydrogenase (GAPDH) and ribosomal proteine S2 (RPS2). Corrected expressions were compared with baseline gene expression of normolipidemic subjects and relative expression changes are displayed. Differences between baseline and endpoint (t12) Ct values were tested by a paired t-test and differences between groups at each time point were tested by unpaired t-test.
Discussion
To the best of our knowledge, this is the first intervention study disclosing gene expression changes in normo- and dyslipidemic subjects after FO supplementation. We identified several genes involved in oxidative processes, which were regulated by FO. The expression of antioxidative enzymes was up-regulated particularly in dyslipidemic subjects, while the expression of pro-oxidative or tissue damage-related enzymes was down-regulated. We suggest that n-3 PUFAs may have an antioxidative potential.
Antioxidative effects could be facilitated by either a reduced production of ROS or an increased production of antioxidative enzymes. Several human studies and in vitro experiments showed reduced superoxide or ROS production by monocytes and neutrophils after n-3 PUFA administration [40–42]. Additionally, negative correlations between ROS production and n-3 PUFA membrane content in healthy [40] and dyslipidemic subjects [41] were observed. On the other hand, positive correlations between the n-3 PUFA membrane content and the activity of antioxidative enzymes could be investigated in fibroblasts cell cultures [43] and in type 2 diabetes patients [44]. In the present study, the supplementation of normo- and dyslipidemic subjects with FO resulted in decreasing AA levels in RBC membranes in favour of EPA and DHA, whose levels increased considerably. Accordingly, the increase of EPA and DHA levels observed in RBC membranes together with an increased expression ratio of the antioxidative enzymes CAT and HMOX2 are in agreement with the findings of Benito [43] and Smaoui [44]. Moreover, the replacement of AA, which is an important ROS producer, in biological membranes may partly explain the antioxidative properties of n-3 PUFAs. On the other hand, the incorporation of EPA and DHA in RBC membranes in response to long-term n-3 PUFA administration results in increased induced lipid peroxidation [45]. In this context, an activation of antioxidative gene expression in response to n-3 PUFA supplementation might be a reaction of the defence system to lower lipid peroxidation. Complementary analysis of oxidative damage or oxidative stress markers combined with expression changes of anti- and pro-oxidant genes should be used to indentify global antioxidative effects.
Nevertheless, an increased expression of HMOX2 and CAT in normo- and dyslipidemic subjects may indicate some antioxidative effects of n-3 PUFAs. To our knowledge, this is the first study at all showing a regulation of HMOX2 expression after n-3 PUFA supplementation in humans. HMOXs are antioxidative enzymes which catabolise heme to biliverdin and carbon monoxide. The two existing HMOXs 1 and 2 differ in their activity. HMOX2 is constitutively expressed, whereas HMOX1 is inducible, e.g. by cellular stress [46]. HMOX2 was identified as part of the large-conductance calcium and voltage-activated potassium (BK(Ca)) channel complex and could enhance its activity, while knockdown of HMOX2 expression reduced channel activity [47]. BK(Ca) channels could influence the cell membrane potential and, therefore, play an important role in many physiological functions, including oxygen-sensing, neuronal excitability, vascular tone regulation, and neurotransmitter release [48, 49]. However, a possible clinical relevance of an increased HMOX2 expression after FO supplementation has to be clarified in further studies.
CAT is an effective antioxidative enzyme [50] known to compensate H2O2[51, 52], e.g. in the centre of inflammation [53, 54]. In this study, expression ratios of the microarray experiments showed an increased expression of CAT in dyslipidemic subjects, whereas qRT-PCR showed an increased expression in both study groups, reaching statistical significance only in normolipidemic subjects. These differences are also known from several other gene expression studies and are mainly explained by the greater sensitivity of the qRT-PCR [55, 56]. The increased expression of CAT in normolipidemic subjects is in contrast to studies with healthy volunteers, which mostly showed no effects on CAT activity after FO supplementation [57, 58]. Results from animal studies, however, indicated an increased CAT activity after treatment with n-3 PUFA [59, 60]. Human studies analysing the effects of n-3 PUFAs on the activity or expression of CAT in dyslipidemic subjects are very limited. In accordance with our results, Bouzidi and coworkers [24] reported an increased CAT activity in patients with dyslipidemia and chronic renal failure after n-3 PUFA supplementation, assuming a greater protection against oxidative stress and prevention of vascular complications. Similarly, an animal study with hypercholesterolemic rats also observed increased CAT activity after DHA feeding. Taken together, these findings suggest that longterm supplementation with n-3 PUFAs results in an enhanced capacity to detoxify H2O2 and might induce adaptive changes in the antioxidative defence system [61].
Glutathione is an important antioxidant which could be readily oxidized non-enzymatically to glutathione disulfide [62]. Most studies analysing the effects of n-3 PUFA supplementation on the activity of glutathione metabolism related enzymes, such as GPX, gamma-glutamylcysteine synthetase (gamma-GCL), GST, and GR, in healthy and dyslipidemic subjects showed increased activities of these enzymes [63–65]. In our study, the expression of GST and GR was increased in dyslipidemic subjects, while the expression of GPX was decreased in both normo- and dyslipidemic subjects. The increased expression of GST and GR is an indication of an increased glutathione synthesis and, therefore, an increased antioxidative defence status. GPX is recognized as an antioxidative enzyme which oxidizes glutathione to reduce and detoxify H2O2. Consequently, this enzyme is required when H2O2 levels rise in phases of oxidative stress [66, 67]. Therefore, a decreased expression of GPX - observed in this study - could be an indicator of decreased oxidative stress. However, the results in the literature are inconsistent. Mabile and co-workers could not observe a change in the GPX activity in healthy and hypertriglyceridemic subjects [68], while other studies reported a stimulated GPX activity after n-3 PUFA supplementation in healthy [63] and hyperlipidemic subjects [64]. Furthermore, it was shown that DHA increased the activity of GST, gammaGCL and GR, as well as the mRNA expression of gamma-GCL and GR [65], in human fibroblasts, which is in agreement with our results.
CYP enzymes catalyze the oxidation of xenobiotic substances, such as pharmaceuticals, but also metabolize many endogenous substances, such as lipids and steroidal hormones. Besides cyclooxygenases and lipoxygenases, CYPs are also involved in the metabolism of PUFAs to form numerous different oxidized FA metabolites, also named oxylipines. The CYP isoforms of families 1 to 3 are mainly epoxygenases, and CYP isoforms from family 4 are mainly ω-hydroxylases [69]. In this study, several CYPs, mostly isoforms of family 2, were regulated after FO supplementation. The oxidation of EPA and DHA by epoxygenases could produce epoxy-derivates [70] and highly anti-inflammatory resolvins and protectins [71].
Generated EPA and DHA epoxides are effective dilators of coronary arterioles, facilitated by the activation of calcium-activated potassium channels [72, 73]. The qRT-PCR showed that CYP1A2, which is one of the most efficient CYPs for the epoxidation of EPA and DHA in human liver microsomes [39], was up-regulated in dyslipidemic subjects after FO supplementation, suggesting the formation of specific EPA and DHA epoxides. Expression ratios of the microarray experiments showed decreased expression of CYP1A2 in normolipidemic subjects, which was, however, not confirmed by qRT-PCR. According to qRT-PCR experiments, the expression of CYP1A2 in normolipidemic subjects was not affected by FO treatment. Both results are in contrast to microarray experiments, where CYP1A2 was unregulated in dyslipidemic subjects and down-regulated in normolipidemic subjects. In view of the higher accuracy of qRT-PCR, it is suggested that the microarray result for CYP1A2 was false positive for normolipidemic subjects, while the microarray technique was insensitive to analyse the up-regulation of CYP1A2 in dyslipidemic subjects, which was generally much weaker. Interestingly, human liver microsomes, which were incubated with EPA and DHA (200 μM) showed a decreased CYP1A2 activity [74]. Although the results are contradictory, it has been repeatedly shown that n-3 PUFAs could induce the expression or activity of CYP enzymes, resulting in the formation of EPA and DHA metabolites [39, 69, 70, 74, 75]. The complex formation of n-3 PUFA metabolites by CYPs has not been investigated systematically so far; however, it is likely that the formation of these metabolites may explain numerous of the anti-inflammatory and cardioprotective effects of n-3 PUFAs [76].
MMPs are zinc-based proteases and could cleave macromolecules of the extra cellular matrix (ECM), e.g. collagens, as well as non-ECM molecules, such as growth factors, cytokines and their receptors [77]. ROS could induce the activity of MMPs [78], which could result in tissue remodelling processes [79] and promote the pathogenesis of several CVDs [80, 81]. In this study, MMP2 and MMP3 in dyslipidemic subjects and MMP25 in normolipidemic subjects were down-regulated after FO supplementation. In accordance with our results, several other authors have shown decreased MMP2 and/or MMP9 expression or activity by n-3 PUFA in dyslipidemic subjects [82] and human cell cultures [83, 84]. However, no changes in MMP9 activity were detected after FO supplementation in patients with coronary heart disease [85]. Similarly, another study observed a slight increase of the MMP2 activity in hypertriglyceridemic men after FO supplementation [86]. Further studies are needed to clarify these discrepancies and the function of n-3 PUFAs in the regulation of MMPs with regard to potential cardioprotective effects.
Strengths and limitations
The methodological approach of this study was carefully elaborated. The use of whole blood for RNA isolation is advantageous in view of the easy sample collection and the prevention of altered gene expression patterns, which is a potential risk of cell fractionation steps [30]. In addition, the pooling of RNA samples reduces inter-individual variation, enabling one to focus on the effects of FO supplementation on the population level in contrast to an individual level [87]. However, the approach of sample pooling provides several limitations, primarily the reduction of statistical power. Finally, oxidative damage and oxidative stress markers were not analysed in this study, which complicates the evaluation of the antioxidative effects.
Conclusions
In conclusion, this study showed indications of the antioxidative potential of n-3 PUFAs, especially in dyslipidemic subjects. FO supplementation resulted in an increased expression of glutathione synthesis-related genes, an up-regulation of antioxidative enzymes, such as CAT and HMOX2, and a reduced expression of MMPs and several CYPs. Interestingly, CYP1A2 was up-regulated in dyslipidemic subjects, suggesting an increased formation of n-3 epoxides. Taken together, these results indicate that n-3 PUFAs may have numerous different possibilities to reduce oxidative stress. It appears that n-3 PUFAs not only up-regulates antioxidative enzymes, but rather induces a specific interplay of differential regulations to generate an optimal balance of the oxidative status. Although the molecular mechanisms by which n-3 PUFAs mediate potential antioxidative effects cannot be clarified here, we hypothesise an involvement of PPARs. In vitro studies with human hepatocytes and pancreatic ß-cells have demonstrated an activation of PPAR-α or -γ by n-3 PUFAs, which resulted in an increased expression of CAT, as well as antioxidative effects [88, 89]. Beside CAT, HMOX-1 has also been demonstrated as a target gene of PPAR [90]. Moreover, an increased expression of antioxidative genes could result in reduced oxidative stress, which further influences stress-activated pathways (MAPK and NFkB pathways), as well as other stress-related genes such as MMPs. However, studies analysing the expression of antioxidative enzymes, oxidative signalling processes and metabolic outcomes are needed to clarify the exact role of n-3 PUFAs within the antioxidative defence system.
Availability of supporting data
The data sets supporting the results of this article are included within the article.
Abbreviations
- AA:
-
Arachidonic acid
- BK(Ca):
-
Channel large-conductance calcium and voltage-activated potassium channel
- CAT:
-
Catalase
- CVD:
-
Cardiovascular disease
- CYP:
-
Cytochrome P 450
- DHA:
-
Docosahexaenoic acid
- ECM:
-
Extra cellular matrix
- EPA:
-
Eicosapentaenoic acid
- FA:
-
Fatty acid
- FO:
-
Fish oil
- gamma-GCL:
-
gamma-glutamylcysteine synthetase
- GAPDH:
-
Glyceraldehyde-3-phosphate dehydrogenase
- GPX:
-
Glutathione peroxidase
- GR:
-
Glutathione reductase
- GST:
-
Glutathione-S-transferase
- H2O2:
-
Hydrogenperoxide
- HMOX:
-
Heme oxygenase
- LDL-C:
-
Low density lipoprotein
- MAPK:
-
Mitogen-activated protein kinase
- MMP:
-
Matrix metalloproteinase
- n-3 PUFA:
-
Omega-3 polyunsaturated fatty acid
- NFkB:
-
Nuclear factor kappa b
- qRT-PCR:
-
Quantitative real-time polymerase chain reaction
- RBC:
-
Red blood cell
- ROS:
-
Reactive oxygen species
- RPS2:
-
Ribosomal protein S2
- SOD:
-
Superoxide dismutase
- t:
-
time point
- TC:
-
Total cholesterol
- TG:
-
Triacylglyceride
- TSA:
-
Tyramide signal amplification.
References
Ohara Y, Peterson TE, Harrison DG: Hypercholesterolemia increases endothelial superoxide anion production. J Clin Invest. 1993, 6: 2546-2551.
Rocha-Pereira P, Santos-Silva A, Rebelo I, Figueiredo A, Quintanilha A, Teixeira F: Dislipidemia and oxidative stress in mild and in severe psoriasis as a risk for cardiovascular disease. Clin Chim Acta. 2001, 1–2: 33-39.
Knight JA: Diseases related to oxygen-derived free radicals. Ann Clin Lab Sci. 1995, 2: 111-121.
Madamanchi NR, Vendrov A, Runge MS: Oxidative stress and vascular disease. Arterioscler Thromb Vasc Biol. 2005, 1: 29-38.
Jung HH, Choi DH, Lee SH: Serum malondialdehyde and coronary artery disease in hemodialysis patients. Am J Nephrol. 2004, 5: 537-542.
Wang XL, Adachi T, Sim AS, Wilcken DE: Plasma extracellular superoxide dismutase levels in an Australian population with coronary artery disease. Arterioscler Thromb Vasc Biol. 1998, 12: 1915-1921.
Landmesser U, Merten R, Spiekermann S, Büttner K, Drexler H, Hornig B: Vascular extracellular superoxide dismutase activity in patients with coronary artery disease: relation to endothelium-dependent vasodilation. Circulation. 2000, 19: 2264-2270.
Griendling KK, Sorescu D, Ushio-Fukai M: NAD(P)H oxidase: role in cardiovascular biology and disease. Circ Res. 2000, 5: 494-501.
Spiekermann S, Landmesser U, Dikalov S, Bredt M, Gamez G, Tatge H, Reepschläger N, Hornig B, Drexler H, Harrison DG: Electron spin resonance characterization of vascular xanthine and NAD(P)H oxidase activity in patients with coronary artery disease: relation to endothelium-dependent vasodilation. Circulation. 2003, 10: 1383-1389.
Alp NJ, Channon KM: Regulation of endothelial nitric oxide synthase by tetrahydrobiopterin in vascular disease. Arterioscler Thromb Vasc Biol. 2004, 3: 413-420.
Mueller CFH, Laude K, McNally JS, Harrison DG: ATVB in focus: redox mechanisms in blood vessels. Arterioscler Thromb Vasc Biol. 2005, 2: 274-278.
Kondo T, Hirose M, Kageyama K: Roles of oxidative stress and redox regulation in atherosclerosis. J Atheroscler Thromb. 2009, 5: 532-538.
Tsutsui H, Kinugawa S, Matsushima S: Oxidative stress and heart failure. Am J Physiol Heart Circ Physiol. 2011, 6: H2181-H2190.
Kameda K, Matsunaga T, Abe N, Hanada H, Ishizaka H, Ono H, Saitoh M, Fukui K, Fukuda I, Osanai T, Okumura K: Correlation of oxidative stress with activity of matrix metalloproteinase in patients with coronary artery disease. Possible role for left ventricular remodellin. Eur Heart J. 2003, 24: 2180-2185. 10.1016/j.ehj.2003.09.022.
Sekikawa A, Curb JD, Ueshima H, El-Saed A, Kadowaki T, Abbott RD, Evans RW, Rodriguez BL, Okamura T, Sutton-Tyrrell K, Nakamura Y, Masaki K, Edmundowicz D, Kashiwagi A, Willcox BJ, Takamiya T, Mitsunami K, Seto TB, Murata K, White RL, Kuller LH: Marine-derived n-3 fatty acids and atherosclerosis in Japanese, Japanese-American, and white men: a cross-sectional study. J Am Coll Cardiol. 2008, 6: 417-424.
Amano T, Matsubara T, Uetani T, Kato M, Kato B, Yoshida T, Harada K, Kumagai S, Kunimura A, Shinbo Y, Kitagawa K, Ishii H, Murohara T: Impact of omega-3 polyunsaturated fatty acids on coronary plaque instability: an integrated backscatter intravascular ultrasound study. Atherosclerosis. 2011, 1: 110-116.
Sudheendran S, Chang CC, Deckelbaum RJ: N-3 vs. saturated fatty acids: effects on the arterial wall. Prostaglandins Leukot Essent Fatty Acids. 4–6: 205-209.
Harris WS: n-3 fatty acids and lipoproteins: comparison of results from human and animal studies. Lipids. 1996, 3: 243-252.
Harris WS: n-3 fatty acids and serum lipoproteins: human studies. Am J Clin Nutr. 1997, 5 (Suppl): 1645S-1654S.
Musa-Veloso K, Binns MA, Kocenas AC, Poon T, Elliot JA, Rice H, Oppedal-Olsen H, Lloyd H, Lemke S: Long-chain omega-3 fatty acids eicosapentaenoic acid and docosahexaenoic acid dose-dependently reduce fasting serum triglycerides. Nutr Rev. 2010, 3: 155-167.
Tremoli E, Eligini S, Colli S, Maderna P, Risè P, Pazzucconi F, Marangoni F, Sirtori CR, Galli C: n-3 fatty acid ethyl ester administration to healthy subjects and to hypertriglyceridemic patients reduces tissue factor activity in adherent monocytes. Arterioscler Thromb. 1994, 10: 1600-1608.
Balk EM, Lichtenstein AH, Chung M, Kupelnick B, Chew P, Lau J: Effects of omega-3 fatty acids on serum markers of cardiovascular disease risk: a systematic review. Atherosclerosis. 2006, 1: 19-30.
Skulas-Ray AC, West SG, Davidson MH, Kris-Etherton PM: Omega-3 fatty acid concentrates in the treatment of moderate hypertriglyceridemia. Expert Opin Pharmacother. 2008, 7: 1237-1248.
Bouzidi N, Mekki K, Boukaddoum A, Dida N, Kaddous A, Bouchenak M: Effects of omega-3 polyunsaturated fatty-acid supplementation on redox status in chronic renal failure patients with dyslipidemia. J Ren Nutr. 2010, 5: 321-328.
Richard D, Kefi K, Barbe U, Bausero P, Visioli F: Polyunsaturated fatty acids as antioxidants. Pharmacol Res. 2008, 6: 451-455.
Filaire E, Massart A, Portier H, Rouveix M, Rosado F, Bage AS, Gobert M, Durand D: Effect of 6 Weeks of n-3 fatty-acid supplementation on oxidative stress in Judo athletes. Int J Sport Nutr Exerc Metab. 2010, 6: 496-506.
Araujo FB, Barbosa DS, Hsin CY, Maranhão RC, Abdalla DS: Evaluation of oxidative stress in patients with hyperlipidemia. Atherosclerosis. 1995, 1: 61-71.
Hiramatsu K, Arimori S: Increased superoxide production by mononuclear cells of patients with hypertriglyceridemia and diabetes. Diabetes. 1988, 6: 832-837.
Harris WS, von Schacky C: The Omega-3 Index: a new risk factor for death from coronary heart disease?. Prev Med. 2004, 1: 212-220.
Vartanian K, Slottke R, Johnstone T, Casale A, Planck SR, Choi D, Smith JR, Rosenbaum JT, Harrington CA: Gene expression profiling of whole blood: comparison of target preparation methods for accurate and reproducible microarray analysis BMC Genomics. 2009, 10: 2-
Debey S, Zander T, Brors B, Popov A, Eils R, Schultze JL: A highly standardized, robust, and cost-effective method for genome-wide transcriptome analysis ofperipheral blood applicable to large-scale clinical trials. Genomics. 2006, 5: 653-664.
Whitney AR, Diehn M, Popper SJ, Alizadeh AA, Boldrick JC, Relman DA, Brown PO: Individuality and variation in gene expression patterns in human blood. Proc Natl Acad Sci U S A. 2003, 4: 1896-1901.
Kerr MK, Churchill GA: Experimental design for gene expression microarrays. Biostatistics. 2001, 2: 183-201. 10.1093/biostatistics/2.2.183.
Barrett T, Troup DB, Wilhite SE, Ledoux P, Evangelista C, Kim IF, Tomashevsky M, Marshall KA, Phillippy KH, Sherman PM, Muertter RN, Holko M, Ayanbule O, Yefanov A, Soboleva A: NCBI GEO: archive for functional genomics data sets-10 years on. Nucleic Acids Res. 2011, (Database issue): D1005-10-
Brazma A, Hingamp P, Quackenbush J, Sherlock G, Spellman P, Stoeckert C, Aach J, Ansorge W, Ball CA, Causton HC, Gaasterland T, Glenisson P, Holstege FC, Kim IF, Markowitz V, Matese JC, Parkinson H, Robinson A, Sarkans U, Schulze-Kremer S, Stewart J, Taylor R, Vilo J, Vingron M: Minimum information about a microarray experiment (MIAME)-toward standards for microarray data. Nat Genet. 2001, 4: 365-371.
Dahlquist KD, Salomonis N, Vranizan K, Lawlor SC, Conklin BR: GenMAPP, a new tool for viewing and analyzing microarray data on biological pathways. Nat Genet. 2002, 1: 19-20.
Rozen S, Skaletsky H: Primer3 on the WWW for general users and for biologist programmers. Methods Mol Biol. 2000, : 365-386.
Vandesompele J, Preter K, Pattyn F, Poppe B, van Roy N, Paepe A, Speleman F: Accurate normalization of real-time quantitative RT-PCR data by geometric averaging of multiple internal control genes. Genome Biol. 2002, 7: -RESEARCH0034
Fer M, Dréano Y, Lucas D, Corcos L, Salaün J, Berthou F, Amet Y: Metabolism of eicosapentaenoic and docosahexaenoic acids by recombinant human cytochromes P450. Arch Biochem Biophys. 2008, 2: 116-125.
Hill AM, Worthley C, Murphy KJ, Buckley JD, Ferrante A, Howe PRC: n-3 Fatty acid supplementation and regular moderate exercise: differential effects of a combined intervention on neutrophil function. Br J Nutr. 2007, 2: 300-309.
Luostarinen R, Saldeen T: Dietary fish oil decreases superoxide generation by human neutrophils: relation to cyclooxygenase pathway and lysosomal enzyme release. Prostaglandins Leukot Essent Fatty Acids. 1996, 3: 167-172.
Zhang YW, Yao XS, Murota S, Morita I: Inhibitory effects of eicosapentaenoic acid (EPA) on the hypoxia/reoxygenation-induced tyrosine kinase activation in cultured human umbilical vein endothelial cells. Prostaglandins Leukot Essent Fatty Acids. 2002, 4: 253-261.
Benito S, Fernandez Y, Mitjavila S, Moussa M, Anglade F, Periquet A: Phospholipid fatty acid composition affects enzymatic antioxidant defenses in cultured Swiss 3T3 fibroblasts. Redox Rep. , 5–6: 281-286.
Smaoui M, Koubaa N, Hammami S, Abid N, Feki M, Chaaba R, Attia N, Abid M, Hammami M: Association between dietary fat and antioxidant status of Tunisian type 2 diabetic patients. Prostaglandins Leukot Essent Fatty Acids. 2006, 5: 323-329.
Palozza P, Sgarlata E, Luberto C, Piccioni E, Anti M, Marra G, Armelao F, Franceschelli P, Bartoli GM: n-3 fatty acids induce oxidative modifications in human erythrocytes depending on dose and duration of dietary supplementation. Am J Clin Nutr. 1996, 3: 297-304.
Abraham NG, Kappas A: Pharmacological and clinical aspects of heme oxygenase. Pharmacol Rev. 2008, 1: 79-127.
Williams SEJ, Wootton P, Mason HS, Bould J, Iles DE, Riccardi D, Peers C, Kemp PJ: Hemoxygenase-2 is an oxygen sensor for a calcium-sensitive potassiumchannel. Science. 2004, 5704: 2093-2097.
Salkoff L, Butler A, Ferreira G, Santi C, Wei A: High-conductance potassium channels of the SLO family. Nat Rev Neurosci. 2006, 12: 921-931.
Hou S, Heinemann SH, Hoshi T: Modulation of BKCa channel gating byendogenous signaling molecules. Physiology (Bethesda). 2009, 26-35.
Goyal MM, Basak A: Human catalase: looking for complete identity. Protein Cell. 2010, 10: 888-897.
Gaetani GF, Ferraris AM, Rolfo M, Mangerini R, Arena S, Kirkman HN: Predominant role of catalase in the disposal of hydrogen peroxide within human erythrocytes. Blood. 1996, 4: 1595-1599.
Mueller S, Riedel HD, Stremmel W: Direct evidence for catalase as the predominant H2O2 -removing enzyme in human erythrocytes. Blood. 1997, 12: 4973-4978.
Halliwell B, Gutteridge JM: Oxygen toxicity, oxygen radicals, transition metals and disease. Biochem J. 1984, 1: 1-14.
Agar NS, Sadrzadeh SM, Hallaway PE, Eaton JW: Erythrocyte catalase. A somatic oxidant defense?. J Clin Invest. 1986, 1: 319-321.
Rajeevan MS, Vernon SD, Taysavang N, Unger ER: Validation of array-based gene expression profiles by real-time (kinetic) RT-PCR. J Mol Diagn. 2001, 1: 26-31.
Toft JH, Lian IA, Tarca AL, Erez O, Espinoza J, Eide IP, Bjørge L, Draghici S, Romero R, Austgulen R: Whole-genome microarray and targeted analysis of angiogenesisregulating gene expression (ENG, FLT1, VEGF, PlGF) in placentas from pre-eclamptic and small-for-gestational-age pregnancies. J Matern Fetal Neonatal Med. 2008, 4: 267-273.
Poprzecki S, Zajac A, Chalimoniuk M, Waskiewicz Z, Langfort J: Modification of blood antioxidant status and lipid profile in response to high-intensity endurance exercise after low doses of omega-3 polyunsaturated fatty acids supplementation in healthy volunteers. Int J Food Sci Nutr. 2009, : 67-79.
Jenkinson A, Franklin MF, Wahle K, Duthie GG: Dietary intakes of polyunsaturated fatty acids and indices of oxidative stress in human volunteers. Eur J Clin Nutr. 1999, 7: 523-528.
Iraz M, Erdogan H, Ozyurt B, Ozugurlu F, Ozgocmen S, Fadillioglu E: Brief communication: omega-3 essential fatty acid supplementation and erythrocyte oxidant/antioxidant status in rats. Ann Clin Lab Sci. 2005, 2: 169-173.
Venkatraman JT, Angkeow P, Satsangi N, Fernandes G: Effects of dietary n-6 and n-3 lipids on antioxidant defense system in livers of exercised rats. J Am Coll Nutr. 1998, 6: 586-594.
Hossain MS, Hashimoto M, Gamoh S, Masumura S: Antioxidative effects of docosahexaenoic acid in the cerebrum versus cerebellum and brainstem of aged hypercholesterolemic rats. J Neurochem. 1999, 3: 1133-1138.
Wu G, Fang Y, Yang S, Lupton JR, Turner ND: Glutathione metabolism and its implications for health. J Nutr. 2004, 3: 489-492.
Bellisola G, Galassini S, Moschini G, Poli G, Perona G, Guidi G: Selenium and glutathione peroxidase variations induced by polyunsaturated fatty acids oral supplementation in humans. Clin Chim Acta. 1992, 1–2: 75-85.
Olivieri O, Negri M, de Gironcoli M, Bassi A, Guarini P, Stanzial AM, Grigolini L, Ferrari S, Corrocher R: Effects of dietary fish oil on malondialdehyde production and glutathione peroxidase activity in hyperlipidaemic patients. Scand J Clin Lab Invest. 1988, 7: 659-665.
Arab K, Rossary A, Flourié F, Tourneur Y, Steghens J: Docosahexaenoic acid enhances the antioxidant response of human fibroblasts by upregulating gamma-glutamyl-cysteinyl ligase and glutathione reductase. Br J Nutr. 2006, 1: 18-26.
Felice F, Lucchesi D, Di Stefano R, Barsotti MC, Storti E, Penno G, Balbarini A, Del Prato S, Pucci L: Oxidative stress in response to high glucose levels in endothelial cells and in endothelial progenitor cells: evidence for differential glutathione peroxidase-1 expression. Microvasc Res. 2010, 3: 332-338.
Matsunami T, Sato Y, Sato T, Ariga S, Shimomura T, Yukawa M: Oxidative stress and gene expression of antioxidant enzymes in the streptozotocin-induced diabetic rats under hyperbaric oxygen exposure. Int J Clin Exp Pathol. 2009, 2: 177-188.
Mabile L, Piolot A, Boulet L, Fortin LJ, Doyle N, Rodriguez C, Davignon J, Blache D, Lussier-Cacan S: Moderate intake of n-3 fatty acids is associated with stable erythrocyte resistance to oxidative stress in hypertriglyceridemic subjects. Am J Clin Nutr. 2001, 4: 449-456.
Lucas D, Goulitquer S, Marienhagen J, Fer M, Dreano Y, Schwaneberg U, Amet Y, Corcos L: Stereoselective epoxidation of the last double bond of polyunsaturated fatty acids by human cytochromes P450. J Lipid Res. 2010, 5: 1125-1133.
Fer M, Goulitquer S, Dréano Y, Berthou F, Corcos L, Amet Y: Determination of polyunsaturated fatty acid monoepoxides by high performance liquidchromatography-mass spectrometry. J Chromatogr A. 2006, 1–2: 1-7.
Stables MJ, Gilroy DW: Old and new generation lipid mediators in acute inflammation and resolution. Prog Lipid Res. 2011, 1: 35-51.
Lauterbach B, Barbosa-Sicard E, Wang M, Honeck H, Kärgel E, Theuer J, Schwartzman ML, Haller H, Luft FC, Gollasch M, Schunck W: Cytochrome P450-dependent eicosapentaenoic acid metabolites are novel BK channel activators. Hypertension. 2002, 2 (Pt 2): 609-613.
Ye D, Zhang D, Oltman C, Dellsperger K, Lee H, VanRollins M: Cytochrome p-450 epoxygenase metabolites of docosahexaenoate potently dilate coronary arterioles by activating large-conductance calcium-activated potassium channels. J Pharmacol Exp Ther. 2002, 2: 768-776.
Yao H, Chang Y, Lan S, Chen C, Hsu JTA, Yeh T: The inhibitory effect of polyunsaturated fatty acids on human CYP enzymes. Life Sci. 2006, 26: 2432-2440.
Arnold C, Konkel A, Fischer R, Schunck W: Cytochrome P450-dependent metabolism of omega-6 and omega-3 long-chain polyunsaturated fatty acids. Pharmacol Rep. , 3: 536-547.
Calder PC: Polyunsaturated fatty acids and inflammatory processes: New twists in an old tale. Biochimie. 2009, 6: 791-795.
Shiomi T, Lemaître V, D'Armiento J, Okada Y: Matrix metalloproteinases, a disintegrin and metalloproteinases, and a disintegrin and metalloproteinases with thrombospondin motifs in non-neoplastic diseases. Pathol Int. 2010, 7: 477-496.
Lim CS, Shalhoub J, Gohel MS, Shepherd AC, Davies AH: Matrix metalloproteinasesin vascular disease–a potential therapeutic target?. Curr Vasc Pharmacol. 2010, 1: 75-85.
Clee SM: A role for MMP-3 genetic variation in atherosclerosis susceptibility?. Atherosclerosis. 2010, 1: 30-31.
Spinale FG, Coker ML, Heung LJ, Bond BR, Gunasinghe HR, Etoh T, Goldberg AT, Zellner JL, Crumbley AJ: A matrix metalloproteinase induction/activation system exists in the human left ventricular myocardium and is upregulated in heart failure. Circulation. 2000, 16: 1944-1949.
Tyagi SC, Campbell SE, Reddy HK, Tjahja E, Voelker DJ: Matrix metalloproteinase activity expression in infarcted, noninfarcted and dilated cardiomyopathic human hearts. Mol Cell Biochem. 1996, 1: 13-21.
Derosa G, Maffioli P, D'Angelo A, Salvadeo SAT, Ferrari I, Fogari E, Gravina A, Mereu R, Randazzo S, Cicero AFG: Effects of long chain omega-3 fatty acids on metalloproteinases and their inhibitors in combined dyslipidemia patients. Expert Opin Pharmacother. 2009, 8: 1239-1247.
Delbosc S, Glorian M, Le Port A, Béréziat G, Andréani M, Limon I: The benefit of docosahexanoic acid on the migration of vascular smooth muscle cells is partially dependent on Notch regulation of MMP-2/-9. Am J Pathol. 2008, 5: 1430-1440.
Kim HH, Lee Y, Eun HC, Chung JH: Eicosapentaenoic acid inhibits TNF-alpha-induced matrix metalloproteinase-9 expression in human keratinocytes, HaCaT cells. Biochem Biophys Res Commun. 2008, 2: 343-349.
Furenes EB, Seljeflot I, Solheim S, Hjerkinn EM, Arnesen H: Long-term influence of diet and/or omega-3 fatty acids on matrix metalloproteinase-9 and pregnancy-associated plasma protein-A in men at high risk of coronary heart disease. Scand J Clin Lab Invest. 2008, 3: 177-184.
Kelley DS, Siegel D, Fedor DM, Adkins Y, Mackey BE: DHA supplementation decreases serum C-reactive protein and other markers of inflammation in hypertriglyceridemic men. J Nutr. 2009, 3: 495-501.
Kendziorski C, Irizarry RA, Chen K, Haag JD, Gould MN: On the utility of pooling biological samples in microarray experiments. Proc Natl Acad Sci USA. 2005, 12: 4252-4257.
Li J, Wang Q, Luan H, Kang Z, Wang C: Effects of L-carnitine against oxidative stress in human hepatocytes: involvement of peroxisome proliferator-activated receptor alpha. J Biomed Sci. 2012, 1: 32-
Chung SS, Kim M, Lee JS, Ahn BY, Jung HS, Lee HM, Park KS: Mechanism for antioxidative effects of thiazolidinediones in pancreatic β-cells. Am J Physiol Endocrinol Metab. 2011, 5: E912-E921.
Krönke G, Kadl A, Ikonomu E, Blüml S, Fürnkranz A, Sarembock IJ, Bochkov VN, Exner M, Binder BR, Leitinger N: Expression of heme oxygenase-1 in human vascular cells is regulated by peroxisome proliferator-activated receptors. Arterioscler Thromb Vasc Biol. 2007, 6: 1276-1282.
Acknowledgements
The supply of the study supplements from Dr. Loges + Co. GmbH, Winsen, Germany, is gratefully acknowledged. Similarly, we thank Philip Saunders who proofread the manuscript. Most of all, we would like to thank the participants who contributed their time to this project.
This study was supported by the Federal Ministry of Education and Research, Germany.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors’ contributions
SS was involved in the study, experimental design, data analysis, interpretation, and manuscript writing. The study was mainly performed by SS. FS was involved in the experimental design and informed advice. KOM was involved in the experimental design, data analysis and manuscript editing. JPS was involved in study design, data interpretation and manuscript writing. The group leader of the Institute of Technical Chemistry, TS, was involved in the study design and manuscript editing. The group leader of the Institute of Food Science and Human Nutrition, AH, was involved in the study design and manuscript editing. Both JPS and AH were coordinators of the study. All authors have read and approved the final manuscript.
Andreas Hahn and Jan Philipp Schuchardt contributed equally to this work.
Electronic supplementary material
12986_2012_433_MOESM1_ESM.pdf
Additional file 1: Regulated genes within stress-activated pathways. Genes, which were regulated after four hours (t4h), one week (t1) and twelve weeks (t12) of fish oil supplementation in normolipidemic and dyslipidemic men were submitted to pathway analyses according to the KEGG database as well as performed with GenMAPP. Expression ratios of regulated genes within mitogen-activated protein kinase (MAPK) signalling pathway, nuclear factor kappa b (NFkB) pathway and oxidative stress pathway were displayed. (PDF 42 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Schmidt, S., Stahl, F., Mutz, KO. et al. Transcriptome-based identification of antioxidative gene expression after fish oil supplementation in normo- and dyslipidemic men. Nutr Metab (Lond) 9, 45 (2012). https://doi.org/10.1186/1743-7075-9-45
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1743-7075-9-45