
Abstract
Background
Porcine reproductive and respiratory syndrome virus (PRRSV) and Streptococcus suis are common pathogens in pigs. In samples collected during the porcine high fever syndrome (PHFS) outbreak in many parts of China, PRRSV and S. suis serotype 7 (SS7) have always been isolated together. To determine whether PRRSV-SS7 coinfection was the cause of the PHFS outbreak, we evaluated the pathogenicity of PRRSV and/or SS7 in a pig model of single and mixed infection.
Results
Respiratory disease, diarrhea, and anorexia were observed in all infected pigs. Signs of central nervous system (CNS) disease were observed in the highly pathogenic PRRSV (HP-PRRSV)-infected pigs (4/12) and the coinfected pigs (8/10); however, the symptoms of the coinfected pigs were clearly more severe than those of the HP-PRRSV-infected pigs. The mortality rate was significantly higher in the coinfected pigs (8/10) than in the HP-PRRSV- (2/12) and SS7-infected pigs (0/10). The deceased pigs of the coinfected group had symptoms typical of PHFS, such as high fever, anorexia, and red coloration of the ears and the body. The isolation rates of HP-PRRSV and SS7 were higher and the lesion severity was greater in the coinfected pigs than in monoinfected pigs.
Conclusion
HP-PRRSV infection increased susceptibility to SS7 infection, and coinfection of HP-PRRSV with SS7 significantly increased the pathogenicity of SS7 to pigs.
Similar content being viewed by others


Background
Porcine reproductive and respiratory syndrome (PRRS) is a threat to the swine industry, and has spread globally to almost every country involved in pig farming, with a few exceptions like Sweden, Switzerland, New Zealand, and Australia [1–4]. PRRS mainly affects pigs and sows; it mainly causes premature delivery, miscarriage, stillbirth, and mummies in sows, and severe pneumonia, edema, and conjunctivitis in pigs. Previous studies have shown that coinfection of PRRSV and bacteria, such as Streptococcus suis, aggravates PRRS [5]. It has been confirmed that PRRSV-infected pigs are more susceptible to S. suis serotype 2 (SS2) infection, and the mortality rate of coinfected pigs is significantly higher than that of PRRSV infected pigs. While the clinical symptoms of both PRRSV infected and coinfected pigs were similar, the incidence of fever in coinfected pigs was higher than that in monoinfected pigs [6].
Since 2006, an unprecedented epidemic of porcine high fever syndrome (PHFS) has spread through the Chinese swine industry, resulting in the culling of an estimated 20 million pigs annually. This disease is characterized by high fever, high incidence rate, and high mortality rate [7]. After extensive epidemiological investigations, highly pathogenic PRRSV (HP-PRRSV) was first isolated from China; many reports suggested that an NSP2 and GP5 gene deletion mutant of PRRSV was the causative agent of the PHFS epidemic [7–10]. Since SS7 has been isolated from pigs exhibiting clinical symptoms of PHFS, some researchers also believe that PHFS is caused by coinfection of HP-PRRSV and S. suis. SS7 is more prevalent than other S. suis serotypes in several provinces of China [11, 12], and SS7 exacerbates PHFS when accompanied by PRRSV infection. Other researchers have suggested that SS7 is less virulent than SS2 and cannot induce serious effects. We established a porcine model of single and mixed infection using veterinary clinical isolates of PRRSV strain HuN4 and SS7 strain WC0711 isolated from China, based on the protocol for coinfection model establishment proposed by Harms et al. [13]. Our aim was to characterize the interaction of SS7 with HP-PRRSV and to elucidate the causes of PHFS epidemic.
Results
Clinical Observation
The pigs in HP-PRRSV-infected group and coinfected group had rectal temperatures > 40.5°C for more duration than control pigs and SS7-infected pigs. Among the coinfected pigs, 8 died of acute illness and the remaining 2 survived. The mortality and morbidity rates of pigs in all groups are summarized in Table 1. The severity of respiratory disease in HP-PRRSV-infected and coinfected pigs was significantly higher (P < 0.05) than in control or SS7 monoinfected pigs. The HP-PRRSV-infected and coinfected pigs with respiratory disease had cough and sneezing in the early phase and asthma and abdominal breathing thereafter. The SS7-infected pigs exhibited mild and moderate cough and sneezing symptoms in the early phase, but they recovered within 2 or 3 days. The HP-PRRSV-infected (4/12) and coinfected pigs (8/10) showed signs of central nervous system (CNS) disease, including muscle tremors, head tilt, nystagmus, and posterior limb paralysis. Only 1 pig in the coinfected group exhibited joint swelling. These signs of CNS disease were not observed in SS7-infected pigs. Unlike SS7-infected pigs, all pigs in the HP-PRRSV-infected and coinfected groups exhibited athrepsia. Further, conjunctivitis was observed in HP-PRRSV-infected pigs and coinfected pigs and diarrhea was observed in HP-PRRSV-infected pigs (severe), SS7-infected pigs (temporary), and coinfected pigs (severe). The relevant clinical data are shown in Table 2.
Macroscopic and microscopic lesions
No macroscopic lesions were observed in the control pigs. The pigs in HP-PRRSV-infected and coinfected groups developed macroscopic brain lesions mainly due to meningitis, meningeal congestion and hemorrhage, swallowed gyri, and brain tissue colliquation. The lung lesions showed multifocal distribution. The affected lung parenchyma appeared mottled, tan, and rubbery, and failed to collapse. Several pigs in the coinfected group had pleuritis or purulent airway exudates. The severity of the lung lesions in SS7-infected pigs was lower than that in HP-PRRSV-infected and coinfected pigs. Pigs in all the 3 experimental groups showed lymph node lesions, including intumescentia and hemorrhage. The scores of lung and lymph nodes were evaluated in detail at necropsy, and are summarized in Figure 1. Kidney lesions in HP-PRRSV-infected and coinfected pigs included punctiform hemorrhage in the cortex, inner hemorrhage, shrunken or disappeared substantia medullaris, and change of color to cinnamon. Macroscopic lesions were also detected in other organs in HP-PRRSV-infected and coinfected pigs; these pigs had grayish-white spots in the liver, and trichocardia, hydrops pericardial, tonsillitis, hemorrhage of the stomach fundus, and spleen infarcts. The SS7-infected pigs had macroscopic lesions mainly in the lungs and lymph nodes with few lesions in other organs. Peritonitis was observed in SS7-infected pigs (2/10) and coinfected pigs (4/10). There was no evidence of arthritis in any of the pigs. The representative images of the macroscopic lesions are presented in Figure 2.

Mean value (standard deviation) of lesion scores. (a) Scores of macroscopic lung lesion, (b) Scores of macroscopic lymph node lesion, (c) Scores of microscopic lung lesion, and (d) Scores of microscopic lymph node lesion at different times after inoculation.

Macroscopic lesions in the coinfected group. (a) Kidney and pelvic hemorrhage; (b) Trichocardia and hydropericardium; (c) Stomach hemorrhage; (d) Bacterial infection in the thoracic cavity; (e) Lymph node intumescentia and hemorrhage; (f) Lung consolidation.
The control pigs showed no pathological lesions. The pathological lung lesions in HP-PRRSV-infected pigs showed the following characteristics: widened interval of alveolar and mild interstitial pneumonia on day 7; interstitial pneumonia associated with purulent lesions and small vessel thrombosis on day 14; suppurative pneumonia and purulent bronchitis on day 21; and localized interstitial pneumonia on day 28. The pathological lung lesions in SS7-infected pigs showed the following characteristics: widened alveolar septa with neutrophil suppurative lesions and small vessel thrombosis on day 14 (7 days after inoculation); widened alveolar septa accompanied by a small number of lymphoid cells, eosinophil infiltration with some fibrin deposition, and mild interstitial pneumonia with neutrophil infiltration on day 21; and small amount of lymphocytic infiltration, fibroplasia, small vessel thrombosis and extensive localized interstitial lymphoid cell infiltration around the bronchi on day 28. The pathological lung lesions in all of the 8 deceased pigs (death occurred between days 10 and 15) exhibited suppurative pneumonia, purulent bronchitis, thrombosis, blood stasis, and widened alveolar septa with fibrin deposition. The severity of the lesions in the deceased pigs was significantly higher (P < 0.01) than that in HP-PRRSV-infected pigs on day 14. The 2 surviving pigs showed localized interstitial pneumonia on day 28. Their lymph nodes exhibited marked lymphocyte necrosis and disintegration, which was sometimes combined with plasma cell hyperplasia or eosinophil infiltration, elevated nodule volume, nodule cavitation, and paracortical hemorrhage. The lymph nodes of HP-PRRSV-infected and coinfected pigs showed a considerable degree of injury with no significant difference, but were obviously more serious (P < 0.01) than those in the SS7-infected pigs. The specific pathology scores of microscopic lung and lymph nodes are summarized in Figure 1. The pathological examination of the brain of PRRSV- and SS7-infected pigs mainly revealed small vessel thrombosis, mild edema, neuron liquefaction necrosis, and glial cell infiltration and perivascular cuffing in some pigs. However, serious perivascular cuffing and thrombosis were observed in the pathological specimens of coinfected pigs. The representative images of the microscopic lesions are presented in Figure 3.

Microscopic lesions in the coinfected group. (a) Perivascular cuffs in brain; (b) Suppurative pneumonia and purulent bronchitis; (c) Lymphocyte necrosis and disintegration in submaxillary lymph nodes; (d) Severe congestion of kidney and renal tubular necrosis and collapse; (e) Moderate sinusoidal congestion with a small number of lymphoid cells and macrophage infiltration in the lung; (f) Lymphoid cell necrosis and collapse around the ellipsoid arterioles and in the white pulp and red pulp of the spleen.
Bacteremia and viremia
Bacteremia was observed in all 10 pigs of the coinfected group, 2 of which showed persistent bacteremia during the experiment. No bacteremia was observed in SS7-infected pigs. At 3 days after HP-PRRSV infection, viremia was observed in all pigs of the HP-PRRSV-infected and coinfected groups, and 9 pigs had viremia even on day 1. Except 5 pigs, all pigs had viremia throughout the study.
Organ-wise distribution of virus and bacteria
The HP-PRRSV strain HuN4 and SS7 strain WC0711 were not detected in the organs of the control pigs. The distribution status of HuN4 and WC0711 strains in 9 organs at different time points after inoculation is summarized in Tables 3 and 4. WC0711 strain detection rates in the 9 organs of the 8 deceased pigs in the coinfected group were significantly higher (P < 0.05) than those in SS7-infected pigs at all time points after inoculation, except in the liver and tonsils on day 28. HuN4 strain detection rates in the brains and stomachs of coinfected pigs were significantly higher (P < 0.05) than those in HP-PRRSV-infected pigs, while the detection rate in other organs was identical for both the groups. Secondary infection with SS7 improved the distribution of the strain HuN4. The strain HuN4 was detected in all the 9 examined organs in the 8 deceased pigs; the detection rate of HuN4 in the brain of coinfected pigs was up to 50%, which was much higher than that in the monoinfected groups.
PRRSV RNA quantification
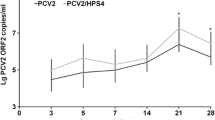
The control and SS7-infected pigs did not contain PRRSV RNA in the lungs and brain. However, all pigs in the HP-PRRSV-infected and coinfected groups contained PRRSV in the lungs, and 4 pigs in the coinfected group and 1 pig in HP-PRRSV-infected group contained PRRSV in the brain. The lungs of HP-PRRSV-infected and coinfected pigs contained similar amount of PRRSV RNA; however, the amount of PRRSV RNA in the brain of coinfected pigs was significantly higher (P < 0.01) than that in HP-PRRSV-infected pigs. The PRRSV levels in the lung and brain are shown in Figure 4.

PRRSV RNA. (a) PRRSV RNA levels in the lungs of all pigs in HP-PRRSV-infected and coinfected groups either after necropsy or death. The data from the coinfected group at 14 days post-inoculation (DPI) is the mean value of 8 pigs of the coinfected group that died between 10 and 15 DPI; no pigs from the coinfected group were necropsied on 21 DPI. (b) The PRRSV RNA levels in the brains of HP-PRRSV-infected and coinfected pigs.
Discussion
HP-PRRSV has been a great threat to pigs since 2006 [7]. However, in this study, we found that PRRSV alone cannot cause extensive damage to the host. Pigs coinfected with PRRSV and SS7 showed symptoms similar to those characteristic of PHFS: high fever, high mortality and morbidity, severe respiratory disease, red coloration of the body, and blue colored ears. The SS7 strain WC0711, an isolate obtained from a PHFS endemic area, was weakly pathogenic in pigs; the severity of the clinical symptoms of the SS7-infected pigs was low and there were no fatalities. This result was consistent with the findings of previous reports regarding the weak virulence of SS7. The SS7 strain WC0711 is an attenuated strain; it can cause mild or moderate respiratory symptoms in pigs, but self-healing may start within a short duration [14]. However, the condition of pigs coinfected with HP-PRRSV (HuN4) and SS7 (WC0711) deteriorated rapidly, with deaths occurring continuously after day 10. The rectal temperature of the 8 deceased pigs of the coinfected group reached 41°C, and in 3 of the 8 pigs the temperature reached 41.5°C, and the number of neurologic symptoms in these pigs increased significantly. Secondary infection with the strain WC0711 increased the mortality of PRRSV-infected pigs from 16.7% to 80% and their progression to the acute stage. We suggest that even SS7, which is a weak virulent serotype, can cause significantly more damage when coinfected with HP-PRRSV. Our results were consistent with those of Feng et al., who reported that after uterine infection of PRRSV in sows, the pigs were markedly more susceptible to SS2 at birth [6].
Several reports have confirmed that the main characteristic of PRRSV is its damaging effects on the host immune system, which facilitates the invasion of other pathogens [5, 15–17]. The immunosuppressive effects are most potent 1 week after infection with PRRSV [18]. The lymph node injury in coinfected pigs was more severe than that in PRRSV (HuN4)-infected pigs. Therefore, we speculated that HP-PRRSV and PRRSV have similar destructive effects on the immune system, and allow secondary infection by SS7, thereby further exacerbating the damage to the immune system. In addition, neurotoxicity is an important feature of PRRSV infection in pigs [19]. Brain injury caused by other pathogens is aggravated after coinfection with PRRSV [20]. In our study, CNS diseases did not develop in the SS7-infected pigs, but the incidence of CNS diseases was doubled in the coinfected pigs as compared to that in the HP-PRRSV-infected pigs. Therefore, coinfection of HP-PRRSV and SS7 may damage the nervous system or induce HP-PRRSV to aggravate nervous system injuries. This effect may be due to the fact that HP-PRRSV infection increases the permeability of the blood-brain barrier. SS7 caused bacteremia immediately after HP-PRRSV infection and rapidly spread to each organ, aggravating the pathological injury to the lungs, brain, and lymph nodes; the combined effect of coinfection markedly increased host mortality. Moreover, SS7 infection improved the distribution of the virus, thereby causing damage to more organs. Therefore, secondary infection with SS7 enhances the pathogenicity of HP-PRRSV in pigs.
Conclusions
We have shown that the clinical manifestations of the coinfection model are similar to those observed during the "high fever" epidemic in China since 2006. The SS7 epidemic may have played a role in the occurrence and development of PRRS. The general level of importance of SS7 has always been less than SS2 because of the characteristic low virulence of the former. However, pigs coinfected with HP-PRRSV and SS7 exhibited serious clinical symptoms affecting multiple organs, such as the lungs, brain, and lymph nodes, which reduced the production and increased mortality, particularly in the case of newborn pigs. Therefore, it is necessary to control bacterial infection by adopting measure to prevent and control HP-PRRS infection. Further characterization of PHFS of pigs under laboratory and natural conditions will be necessary to understand the mechanisms underlying the enhanced susceptibility of HP-PRRSV-infected pigs to SS7.
Methods
Animals
We brought 42 crossbred early-weaned pigs of approximately 3 weeks of age to our research facility. The pigs were purchased from a herd determined to be free of PRRSV and SS7 based on regular serological testing. On the day of arrival, the pigs were randomly assigned to 4 groups: 8, control group; 12, HP-PRRSV-infected group and coinfected group; and 10, SS7-infected group. The care and treatment of pigs in our study were conducted in accordance with the guidelines on animal experimentation of Chinese Academy of Agricultural Sciences (CAAS).
Experimental design and inoculations
Eight pigs served as uninoculated controls. The pigs in the HP-PRRSV-infected group and coinfected group were intranasally (IN) (2 ml) and intramuscularly (IM; 1 ml) inoculated with the representative strain of HP-PRRSV, namely, HuN4 on day 0 [21]. The pigs in the SS7-infected group and coinfected group were IN (2 ml) and IM inoculated with the SS7 strain WC0711, which was isolated from a sample of PHFS, on day 7. The experimental design is summarized in Table 5. The HP-PRRSV strain HuN4 isolated at passage 25 was used as the inoculum for virus challenge. The titer of the virus was calculated as 104.97 TCID50/2 ml. The WC0711 strain was isolated from a pure culture on sheep blood agar plates (BAPs) by overnight incubation at 37°C, and was subsequently cultured in Todd-Hewitt broth (Bacto, Liverpool, UK) with 5% horse serum for 12 h at 37°C. The culture was centrifuged at 3,000 rpm for 15 min and the bacteria were resuspended in phosphate buffered saline (PBS). The bacterial inoculum contained approximately 109 colony-forming units (CFU)/ml.
Clinical observation
The pigs were monitored daily and scored for the severity of clinical respiratory disease by using a scoring system ranging from 0 (normal) to 6 (severe dyspnea and abdominal breathing) [22]. In addition, the pigs were observed daily for other clinical signs, including CNS disease, joint swelling, lameness, sneezing, and jaundice. The rectal temperature, muscle wasting, and behavioral changes, such as lethargy were recorded daily.
Postmortem examination
We randomly selected 2 pigs each from the control group, HP-PRRSV-infected group, and coinfected group and performed necropsy on day 7 of the study. Then, 4 randomly selected pigs from all the 3 experimental groups and 2 from the control group were necropsied on day 14 and 21, respectively. The remaining pigs were necropsied on day 28. If the pigs died or became moribund before schedule, they were necropsied immediately. Organ samples (brain, tonsils, lymph nodes, heart, liver, spleen, lungs, kidneys, and stomach) were collected and analyzed for the presence of SS7 by polymerase chain reaction (PCR). Reverse transcriptase (RT)-PCR [5] and real-time PCR [23] for HP-PRRSV and immunofluorescent antibody (IFA) assays for both SS7 and HP-PRRSV [24] were performed. The distribution of virus and bacteria was investigated.
An estimated percentage of the lung affected by pneumonia was visibly determined for each pig based on a scoring system [22]. The sections of heart, liver, and kidney were evaluated for the presence of lymphohistiocytic inflammation and scored from 0 (none) to 3 (severe). Lymphoid tissues, including lymph nodes, tonsils, and spleen, were evaluated for lymphoid depletion ranging from 0 (normal) to 3 (severe) and histiocytic inflammation and replacement of follicles ranging from 0 (normal) to 3 (severe) [25]. The macroscopic and microscopic scores were evaluated by 4 different researchers.
Bacteremia and viremia
To monitor bacteremia and viremia, blood was collected on days 0, 1, 3, 5, 7, 8, 10, 12, 15, 19, 23, and 28. Whole blood was cultured in Todd-Hewitt broth for the detection of SS7 by PCR. The presence of PRRSV in the sera was determined by RT-PCR using previously described methods [13]. DNA was extracted from whole blood using a TIANamp bacteria DNA kit (TIANGEN) and RNA was extracted from the sera using a QIAamp viral RNA mini kit (QIAGEN). The emergence and persistence times of bacteremia and viremia were recorded. The primers used for the detection of bacteremia were cps7a: 5'-AGTCTAACACGAAATAAGGC-3' and cps7b: 5'-GTCAAACACCCTGGATAGCCG-3'. The primers used for the detection of viremia were HP-PRRSVVU: 5'-GAGGGAAGGGGATTGCCAGCCAG-3' and HP-PRRSVVL: 5'-CTCACCCCCACACGGTCGCCCTAA-3'.
Statistical analysis
Before data analysis, descriptive statistics were performed to assess the overall quality of the data. Continuous data were analyzed by one-way analysis of variance (ANOVA). If the results of one-way ANOVA showed significant difference (P < 0.05), pairwise testing using Tukey's adjustment was performed. Discrete data (macroscopic and microscopic lesions and clinical observations) were analyzed by the nonparametric Kruskal-Wallis one-way ANOVA. If the results of nonparametric ANOVA showed significant difference (P < 0.05), Wilcoxon tests were performed for pairwise analysis. Response feature analysis was performed to account for clinical observations. The results obtained after HP-PRRSV challenge were combined, and the averages for each pig and differences among groups were compared by nonparametric Kruskal-Wallis ANOVA. Fisher's exact test was used to evaluate the differences in the incidence of infection.
References
Elvander M, Larsson B, Engvall AB, Gunnarsson A: Nationwide surveys of TGE/PRCV, CSF, PRRS, SDV, L. Pomona and B. suis in pigs in Sweden. J Epidemiol Sante Anim. 1997, 39: 31-32.
Canon N, Audige L, Denac H, Hofmann M, Griot C: Evidence of freedom from porcine reproductive and respiratory syndrome virus infection in Switzerland. Vet Rec. 1998, 142: 142-143. 10.1136/vr.142.6.142.
Motha J, Stark K, Thompson J: New Zealand is free from PRRS, TGE and PRRSV. J Surveillance. 1997, 24: 10-11.
Galina L, Pijoan C, Sitjar M, Christianson WT, Rossow K, Collins JE: Interaction between Streptococcus suis serotype 2 and porcine reproductive and respiratory syndrome virus in specific pathogen-free piglets. Vet Rec. 1994, 134: 60-64. 10.1136/vr.134.3.60.
Wei TC, Tian ZJ, An TQ, Zhou YJ, Xiao Y, Jiang YF, Hao XF, Zhang SR, Peng JM, Qiu HJ, Tong GZ: Development and application of Taq Man-MGB fluorescence quantitative RT-PCR assay for detection of porcine reproductive and respiratory syndrome virus. Chinese Journal of Preventive Veterinary Medicine. 2008, 30: 944-948.
Feng WH, Laster SM, Tompkins M, Brown T, Xu JS, Altier C, Gomez W, Benfield D, McCaw MB: In utero infection by porcine reproductive and respiratory syndrome virus is sufficient to increase susceptibility of piglets to challenge by Streptococcus suis type II. Journal of Virology. 2001, 75: 4889-4895. 10.1128/JVI.75.10.4889-4895.2001.
Tian KG, Yu XL, Zhao TZ, Feng YJ, Cao Z, Wang CB, Hu Y, Chen XZ, Hu DM, Tian XS, et al: Emergence of Fatal PRRSV Variants: Unparalleled Outbreaks of Atypical PRRS in China and Molecular Dissection of the Unique Hallmark. Plos One. 2007, 2: e526-10.1371/journal.pone.0000526.
Tong GZ, Zhou YJ, Hao XF, Tian ZJ, An TQ, Qiu HJ: Highly pathogenic porcine reproductive and respiratory syndrome, China. Emerg Infect Dis. 2007, 13: 1434-1436.
Li Y, Wang X, Bo K, Tang B, Yang B, Jiang W, Jiang P: Emergence of a highly pathogenic porcine reproductive and respiratory syndrome virus in the Mid-Eastern region of China. Vet J. 2007, 174: 577-584. 10.1016/j.tvjl.2007.07.032.
Zhou YJ, Hao XF, Tian ZJ, Tong GZ, Yoo D, An TQ, Zhou T, Li GX, Qiu HJ, Wei TC, Yuan XF: Highly virulent porcine reproductive and respiratory syndrome virus emerged in China. Transboundary and Emerging Diseases. 2008, 55: 152-164. 10.1111/j.1865-1682.2008.01020.x.
Zhen Y, Kaicheng W, Weixing F, Ping J: Epidemiological investigation on the carrier status of Streptococcus suis in healthy pigs. Chinese journal of Zoonoses. 2009, 25: 977-979.
Ping S, Manxiang L: Analysis on Resistance of Separation Plant of Streptococcus suis Type 2 # and type 7 # to Antibiotic. Journal of Anhui Agri Sci. 2009, 37: 140-141.
Harms PA, Sorden SD, Halbur PG, Bolin SR, Lager KM, Morozov I, Paul PS: Experimental reproduction of severe disease in CD/CD pigs concurrently infected with type 2 porcine circovirus and porcine reproductive and respiratory syndrome virus. Veterinary Pathology. 2001, 38: 528-539. 10.1354/vp.38-5-528.
Tian Y, Aarestrup FM, Lu CP: Characterization of Streptococcus suis serotype 7 isolates from diseased pigs in Denmark. Veterinary Microbiology. 2004, 103: 55-62. 10.1016/j.vetmic.2004.07.009.
Solano GI, Segales J, Collins JE, Molitor TW, Pijoan C: Porcine reproductive and respiratory syndrome virus (PRRSv) interaction with Haemophilus parasuis. Vet Microbiol. 1997, 55: 247-257. 10.1016/S0378-1135(96)01325-9.
Thacker EL, Halbur PG, Ross RF, Thanawongnuwech R, Thacker BJ: Mycoplasma hyopneumoniae potentiation of PRRSV-induced pneumonia. J Clin Microbiol. 1998, 37: 620-627.
Wills RW, Fedorka-Cray PJ, Yoon KJ, Gray JT, Stabel T, Zimmerman JJ: Synergism between porcine reproductive and respiratory syndrome virus (PRRSV) and Salmonella choleraesuis. Proc Am Assoc Swine Pract. 1997, 1997: 459-462.
Thanawongnuwech R, Brown GB, Halbur PG, Roth JA, Royer RL, Thacker BJ: Pathogenesis of porcine reproductive and respiratory syndrome virus-induced increase in susceptibility to Streptococcus suis infection. Vet Pathol. 2000, 37: 143-152. 10.1354/vp.37-2-143.
Rossow KD, Shivers JL, Yeske PE, Polson DD, Rowland RRR, Lawson SR, Murtaugh MP, Nelson EA, Collins JE: Porcine reproductive and respiratory syndrome virus infection in neonatal pigs characterised by marked neurovirulence. Veterinary Record. 1999, 144: 444-448. 10.1136/vr.144.16.444.
Narita M, Ishii M: Encephalomalacic lesions in pigs dually infected with porcine reproductive and respiratory syndrome virus and pseudorabies virus. Journal of Comparative Pathology. 2004, 131: 277-284. 10.1016/j.jcpa.2004.05.001.
Tong GZ, Zhou YJ, Hao XF, Tian ZJ, Qiu HJ, Peng JM, An TQ: Identification and molecular epidemiology of the very virulent porcine reproductive and respiratory syndrome virus emerged in China. Chinese Journal of Preventive Veterinary Medicine. 2007, 29: 323-326.
Halbur PG, Paul PS, Frey ML, Landgraf J, Eernisse K, Meng XJ, Lum MA, Andrews JJ, Rathje JA: Comparison of the pathogenicity of two US porcine reproductive and respiratory syndrome virus isolates with that of the Lelystad virus. Vet Pathol. 1995, 32: 648-660. 10.1177/030098589503200606.
Inoue R, Tsukahara T, Sunaba C, Itoh M, Ushida K: Simple and rapid detection of the porcine reproductive and respiratory syndrome virus from pig whole blood using filter paper. Journal of Virological Methods. 2007, 141: 102-106. 10.1016/j.jviromet.2006.11.030.
Shibata I, Mori M, Uruno K: Experimental infection of maternally immune pigs with porcine reproductive and respiratory syndrome (PRRS) virus. Journal of Veterinary Medical Science. 1998, 60: 1285-1291. 10.1292/jvms.60.1285.
Opriessnig T, Thacker EL, Yu S, Fenaux M, Meng XJ, Halbur PG: Experimental reproduction of postweaning multisystemic wasting syndrome in pigs by dual infection with Mycoplasma hyopneumoniae and porcine circovirus type 2. Vet Pathol. 2004, 41: 624-640. 10.1354/vp.41-6-624.
Acknowledgements
The work was supported by a grant from the Ministry of Sciences and Technology, the State Key Project of Basic Research (Project 973, No. 2006CB504401).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
Xu Min carried out the animal experiments, participated in the sequence alignment and drafted the manuscript. Wang Shujie and Liu Yonggang cultured the virus and bacteria. Shi Wenda, Li Liqin, and Wu Jiabin were responsible for the molecular genetic studies. Rong Fulong carried out the immunoassays. Xu Mingming participated in the sequence alignment. Sun Guanli, Li Linxi and Xiang Hua participated in the design of the study and performed the statistical analysis. Cai Xuehui and Lei Liancheng conceived of the study, participated in its design and coordination, and helped to draft the manuscript. All authors read and approved the final manuscript.
Shujie Wang, Liancheng Lei and Xuehui Cai contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Xu, M., Wang, S., Li, L. et al. Secondary infection with Streptococcus suis serotype 7 increases the virulence of highly pathogenic porcine reproductive and respiratory syndrome virus in pigs. Virol J 7, 184 (2010). https://doi.org/10.1186/1743-422X-7-184
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1743-422X-7-184