
Abstract
Background
Currently applied indicator organism systems, such as coliforms, are not fully protective of public health from enteric viruses in water sources. Waterborne disease outbreaks have occurred in systems that tested negative for coliforms, and positive coliform results do not necessarily correlate with viral risk. It is widely recognized that bacterial indicators do not co-occur exclusively with infectious viruses, nor do they respond in the same manner to environmental or engineered stressors. Thus, a more appropriate indicator of health risks from infectious enteric viruses is needed.
Presentation of the hypothesis
Torque teno virus is a small, non-enveloped DNA virus that likely exhibits similar transport characteristics to pathogenic enteric viruses. Torque teno virus is unique among enteric viral pathogens in that it appears to be ubiquitous in humans, elicits seemingly innocuous infections, and does not exhibit seasonal fluctuations or epidemic spikes. Torque teno virus is transmitted primarily via the fecal-oral route and can be assayed using rapid molecular techniques. We hypothesize that Torque teno virus is a more appropriate indicator of viral pathogens in drinking waters than currently used indicator systems based solely on bacteria.
Testing the hypothesis
To test the hypothesis, a multi-phased research approach is needed. First, a reliable Torque teno virus assay must be developed. A rapid, sensitive, and specific PCR method using established nested primer sets would be most appropriate for routine monitoring of waters. Because PCR detects both infectious and inactivated virus, an in vitro method to assess infectivity also is needed. The density and occurrence of Torque teno virus in feces, wastewater, and source waters must be established to define spatial and temporal stability of this potential indicator. Finally, Torque teno virus behavior through drinking water treatment plants must be determined with co-assessment of traditional indicators and enteric viral pathogens to assess whether correlations exist.
Implications of the hypothesis
If substantiated, Torque teno virus could provide a completely new, reliable, and efficient indicator system for viral pathogen risk. This indicator would have broad application to drinking water utilities, watershed managers, and protection agencies and would provide a better means to assess viral risk and protect public health.
Similar content being viewed by others


Background
The connection between fecal contamination of drinking water and outbreaks of disease from waterborne pathogens has been established for more than a century [1]. Because it would not be feasible to monitor directly for every known pathogen, indicator organisms, which correlate with fecal contamination and suggest health risk, are used instead [2, 3]. In water supply systems, monitoring for total coliforms, fecal coliforms, and E. coli is regulated under the Total Coliform Rule (TCR) [4]. However, these bacterial indicators are not always 100% protective of public health, particularly from enteric viruses. Waterborne disease outbreaks of viral etiology have occurred in systems in which coliforms were absent, and instances of coliform presence in violation of the TCR are not always associated with adverse public health outcomes [5–7].
The use of coliforms as indicators of viral pathogen risk is problematic for several reasons:
-
1)
There is a lack of association between coliforms and human enteric viruses in the environment. Bacterial indicators have low predictive ability for enteric viruses [8, 9] and low or no correlation to viruses [10–16].
-
2)
The fate of coliforms and viral pathogens in environmental systems is disparate. Coliform bacteria are more susceptible than enteric viruses to extremes in pH, salinity, and temperature [9, 17–19]. In addition, bacteria are more easily removed by filtration through natural aquifer systems [13, 20–22]. Overall, virus persistence and mobility generally exceed that of bacteria in environmental waters [9, 23].
-
3)
Coliforms and viral pathogens have distinct resistance patterns in engineered treatment processes [24]24, and infectious viruses have been found in finished waters that are coliform negative [25, 26]. Physical removal of viruses through treatment systems, for instance by ultrafiltration or microfiltration membranes, is more challenging than removal of bacteria [27–32]. In addition, many enteric viruses are more resistant than bacteria to disinfection with chlorine and ultraviolet radiation [8, 33–36].
Several alternatives to bacterial indicators have been proposed. Coliphages exhibit similarities to enteric viruses regarding environmental transport and survival [37, 38]. However, coliphage survival characteristics vary by season [39] and by coliphage group [12, 40–43]. In addition, coliphages may continue to replicate in surviving bacterial hosts after being shed in feces, thus exhibiting much greater persistence than human enteric viruses in receiving waters [9, 44]. Alternatively, only a small percentage of human or animal fecal samples test positive for coliphages [45, 46] so these viruses may be too sparse to detect in some environmental waters.
Some researchers have suggested enteroviruses or noroviruses as indicators of other enteric viruses [47, 48]. However, these viruses exhibit seasonal fluctuations and epidemic spikes [16, 49]. In addition, quantification of infectious noroviruses in vitro has only recently been accomplished using 3-D cell culture [50], which is well beyond the analytical capabilities of typical water testing laboratories. Adenovirus has been proposed as an indicator because of its remarkable resistance characteristics and lack of seasonal variability. However, this virus did not correlate with hepatitis A virus or enteroviruses in urban waterways [51].
We hypothesize that Torque teno virus (TTV) is a superior indicator of enteric viruses compared to traditional bacterial indicators and proposed viral indicators. TTV is an enterically transmitted human virus, but it exhibits characteristics that distinguish it from other enteric viruses. Recent studies toward understanding the biology and occurrence of TTV provide preliminary support for our hypothesis.
Presentation of the hypothesis
TTV is a recently discovered non-enveloped virus with a single-stranded, circular DNA genome [52–54]. TTV isolates are remarkably variable with 47–70% divergence at the amino acid level [55, 56]. TTV divergence is unevenly distributed across the genome; hypervariable regions exist within the coding region [57], and the untranslated region contains conserved regulatory sequences [58].
Initially, TTV was described as a novel hepatitis virus [52], but it was later determined that TTV circulates in a large proportion of healthy individuals [59–61] with an average worldwide prevalence estimated at 80% [62, 63]. The virus appears to elicit both persistent and transient infections [52]. Transmission of TTV is primarily by the fecal-oral route [63], but it is detected in a variety of human tissues and fluids, including plasma and serum [64–68]. Many attempts have been made to assign a pathology to TTV, but none have been substantiated. In fact, Griffiths [69] and Simmonds et al. [70] have suggested that TTV may constitute the first known commensal human virus.
A few investigators have tracked TTV in the environment or in treatment systems. Their results suggest that TTV may co-locate with various enteric viruses. Currently, little is known about the environmental stability of TTV, although Takayama et al. [71] demonstrated that TTV infectivity was not lost after 95 hours of dry heat treatment. Investigators suspect that TTV particles are highly resistant to environmental stressors [72].
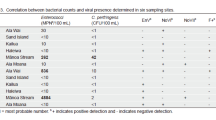
In polluted streams of Brazil, TTV was found to be spatially and temporally constant [61], and the TTV positivity rate of 92.3% paralleled the positivity rate reported by de Paula et al. [73] for hepatitis A virus in the same geographic region. In Italy, river water samples receiving waste treatment effluent were found to contain TTV and other enteric viruses [72]. TTV and rotavirus occurred either simultaneously or within 1 month's sampling period of each other. In addition, TTV occurred 1–2 months after enterovirus was detected and simultaneously or within 2 months of noroviruses g1 and g2 in all but one case.
Vaidya et al. [59] compared sewage treatment plant influent and effluent concentrations of TTV and hepatitis A and E viruses via PCR and observed that raw sewage prevalence of TTV DNA was statistically similar to the prevalence of hepatitis E virus RNA and hepatitis A virus RNA. Following treatment, hepatitis A virus RNA was significantly reduced, but the reductions in TTV and hepatitis E virus genetic material were not statistically significant. When TTV was monitored through activated sludge wastewater treatment plants in Japan, researchers reported that the TTV genome was detected with 97% frequency in influent, 18% in secondary effluent after activated sludge but before chlorination, 24% in final effluent after chlorination, and 0% in effluent for reuse following filtration and ozonation [60]. In contrast, coliforms decreased sequentially with each step in the treatment process, and the concentration of coliforms did not correlate with the number of positive TTV samples collected at any step.
As a putative indicator, TTV should be abundant where water is not adequately treated and diarrheal disease is common and should exist at low or undetectable levels where water treatment leads to clean, potable water. Poor sanitation may increase TTV transmission by the fecal-oral route, as the countries of Bolivia and Burma – both with high risks of waterborne disease – have TTV incidences of 82% and 96%, respectively, among otherwise healthy individuals [74]. In contrast, TTV prevalence in the United States is estimated to be 10% [75]. It is hypothesized that at this prevalence, TTV would be present in most environmental samples at levels high enough to be detected using PCR [63] with the exception of contamination resulting from single septic systems.
Testing the hypothesis
A three-phased plan of research is necessary to determine the value of TTV as an indicator for viral pathogens.
Phase I – Develop reliable TTV assay
PCR indicates the presence/absence of a target sequence and would yield a positive result for a non-infectious viral particle if the particle's genetic material was intact. The presence of viral nucleic acid at a site nevertheless indicates that contamination occurred in the recent past and suggests that the site is susceptible to future contamination [76]. The rapid nature of PCR makes it an ideal tool for periodic monitoring of water sources.
Because viruses are present in low concentrations in environmental waters, it is necessary to concentrate water samples by several orders of magnitude prior to PCR analysis. However, sample concentration also may concentrate inhibitors of DNA polymerase. The use of hollow fiber ultrafiltration is proposed. This method is effective for concentrating MS2 coliphage, noroviruses, and adenoviruses for subsequent enumeration or PCR detection [[77]; Sibley SD, personal communication]. The selection of primers against conserved regions of the TTV genome is crucial for accurately detecting all TTV isolates. In addition to amplifying a conserved sequence, nested or seminested PCR is proposed; this technique approaches a resolution of one TTV genome/sample [53, 62, 78].
If TTV is to be used as an indicator – particularly in a treatment system in which viral particles may be inactivated but not removed – a method must be available to determine TTV infectivity. In vitro infection by TTV has been demonstrated in activated peripheral blood mononuclear cells and the Chang liver cell line [79–81]. Either of these may be candidates for infectivity assessment. Chang liver cells exhibit cytopathic effects 2–3 days after inoculation with TTV [81] so this cell line may be useful for rapid identification of infectivity.
Phase II – Monitor TTV in sources
In order to determine the utility of TTV as an indicator, the occurrence, density, and persistence of TTV in feces, wastewater, and environmental waters need to be evaluated. Geographically diverse samples should be collected during all seasons to assess both spatial and temporal stability. The persistence of the TTV genome has not been described in environmental waters, but researchers have reported that TTV DNA from fecal extracts degrades by approximately 3 log10 within 1 week when monitored by real-time PCR at 37°C [81]. Once these data are gathered, the results can be compared to coliforms, coliphages, and total culturable viruses to determine whether TTV co-locates with other enteric viruses and/or other indicators.
Phase III – Monitor TTV through drinking water treatment
The fate of TTV through drinking water treatment processes needs to be assessed. Prior research has demonstrated removal/inactivation of TTV through wastewater treatment [60], but data are lacking for municipal drinking waters. As with source monitoring, spatial and temporal diversity of the sampling protocol is necessary. Co-monitoring coliforms, coliphages, and total culturable viruses should be performed to demonstrate the relative resistance of TTV to treatment effects and to determine relationships, if any, among TTV, enteric viruses, and indicators.
Implications of the hypothesis
Because of the shortcomings of traditional bacterial indicator organisms to accurately indicate viral risk, novel indicator or monitoring systems are needed. If the indicator potential of TTV is substantiated, a TTV indicator system could complement or replace traditional bacterial indicators for the detection of human enteric viruses in environmental samples. The ability to assess viral pathogen risk would be enhanced, and ultimately, public health would be better protected.
Authors' information
JSG is a graduate student at WPI with expertise in molecular, biochemical, and virologic techniques. JSG is well versed in PCR, including real-time and endpoint PCR. Her technical skills include mammalian, yeast, and bacterial cell culture; genetic engineering; viral protein biochemistry; and basic viral infection, propagation, and storage techniques. JDP is a faculty member in Environmental Engineering with 15 years experience in source water protection, microbial source tracking, and physical/chemical water treatment. SCL is a faculty member in Soil Science and Director of Microbiology at a State Hygiene Laboratory. She has over 20 years of expertise in watershed management, water quality analysis, indicator organism microbiology and public health issues.
References
Snow J: On the mode of communication of cholera. 2nd edition. London: J. Churchill; 1855.
Toranzos GA, McFeters GA: Detection of indicator microorganisms in environmental freshwaters and drinking waters. In Manual of Environmental Microbiology. Edited by: Hurst CJ, Knudsen GR, McInerney MJ, Stetzenbach LD, Walter M. Washington, DC: American Society for Microbiology Press; 1997:184-194.
National Research Council: Indicators for waterborne pathogens. Washington, DC: National Academy Press; 2004.
U.S. Environmental Protection Agency: National Primary Drinking Water Regulations: Total Coliform Rule, Final Rule. Federal Register 1989, 54: 27544-27568.
D'Antonio RG, Winn RE, Taylor JP, Gustafson TL, Current WL, Rhodes MM, Gary GW Jr, Zalac RA: A waterborne outbreak of cryptosporidiosis in normal hosts. Ann Int Med 1985, 103: 886-888.
Craun GF, Berger PS, Calderon RL: Coliform bacteria and waterborne disease outbreaks. JAWWA 1997, 89: 96-104.
Hrudey SE, Hrudey EJ: Safe Drinking Water: Lessons from Recent Outbreaks in Affluent Nations. London: IWA Publishing; 2004.
Bosch A, Lucena F, Diez JM, Gajardo R, Blasi M, Jofre J: Waterborne viruses associated with hepatitis outbreak. JAWWA 1991, 83: 80-83.
Nasser AM, Oman SD: Quantitative assessment of the inactivation of pathogenic and indicator viruses in natural water sources. Water Res 1999, 33: 1748-1752.
Gerba CP, Goyal SM, LaBelle RL, Cech I, Bogdan GF: Failure of indicator bacteria to reflect occurrence of enteroviruses in marine waters. Am J Pub Health 1979, 69: 1116-1119.
LaBelle RL, Gerba CP, Goyal SM, Melnick JL, Cech I, Bogdan GF: Relationships between environmental factors, bacterial indicators, and the occurrence of enteric viruses in estuarine sediments. Appl Environ Microbiol 1980,39(3):586-596.
Nasser AM, Tchorch Y, Fattal B: Comparative survival of E. coli, F+ bacteriophages, HAV and poliovirus 1 in wastewater and groundwater. Water Sci Technol 1993, 27: 401-407.
Scandura JE, Sobsey MD: Viral and bacterial contamination of groundwater from on-site sewage treatment systems. Water Sci Technol 1997, 35: 141-146.
Borchardt M, Haas NL, Hunt RJ: Vulnerability of drinking-water wells in La Crosse, Wisconsin, to enteric-virus contamination from surface water contributions. Appl Environ Microbiol 2004, 70: 5937-5946.
Jiang SC, Chu W: PCR detection of pathogenic viruses in southern California urban rivers. J Appl Microbiol 2004, 97: 17-28.
Skraber S, Gassilloud B, Gantzer C: Comparison of coliforms and coliphages as tools for assessment of viral contamination in river water. Appl Environ Microbiol 2004, 70: 3644-3649.
Springthorpe VS, Loh CL, Robertson WJ, Sattar SA: In situ survival of indicator bacteria, MS-2 phage and human pathogenic viruses in river water. Water Sci Technol 1993, 27: 413-420.
Bosch A: Human enteric viruses in the water environment: a minireview. Int Microbiol 1998, 1: 191-196.
Fong TT, Lipp EK: Enteric viruses of humans and animals in aquatic environments: health risks, detection, and potential water quality assessment tools. Microbiol Mol Biol Rev 2005, 69: 357-371.
Macler BA, Merkle JC: Current knowledge on groundwater microbial pathogens. Hydrol J 2000, 8: 29-40.
Azadpour-Keeley A, Faulkner BR, Chen JS: Movement and longevity of viruses in the subsurface. EPA Ground Water Issue 2003, 1-24.
Reynolds KA, Mena KD, Gerba CP: Risk of waterborne illness via drinking water in the United States. Rev Environ Contam Toxicol 2008, 192: 117-158.
Bitton G, Farrah SR, Ruskin RH, Butner J, Chou YJ: Survival of pathogenic and indicator organisms in groundwater. Ground Water 1983, 21: 405.
Payment P, Armon R: Virus removal by drinking water treatment processes. CRC Crit Rev Environ Contr 1989, 19: 15-31.
Keswick BH, Gerba CP, DuPont HL, Rose JB: Detection of enteric viruses in treated drinking water. Appl Environ Microbiol 1984, 47: 1290-1294.
Payment P, Trudel M, Plante R: Elimination of viruses and indicator bacteria at each step of treatment during preparation of drinking water at seven water treatment plants. Appl Environ Microbiol 1985, 49: 1418-1428.
Jacangelo JG, Laine JM, Carns KE, Cummings EW, Mallevaille J: Low-pressure membrane filtration for removing Giardia and microbial indicators. JAWWA 1991, 83: 97-106.
Jacangelo JG, Adham SS, Laine JM: Mechanism of Cryptosporidium, Giardia, and MS2 virus removal by MF and UF. JAWWA 1995, 87: 107.
Nasser A, Weinberg D, Dinoor N, Fattal B, Adin A: Removal of hepatitis virus (HAV), poliovirus and MS2 coliphage by coagulation and high rate filtration. Water Sci Technol 1995, 31: 63-68.
Yoo S, Brown DR, Pardini RJ, Bentson GD: Microfiltration: a case study. JAWWA 1995, 87: 38-49.
Hagen K: Removal of particles, bacteria and parasites with ultrafiltration for drinking water treatment. Desalination 1998, 119: 85-91.
Harrington GW, Xagoraraki I, Assavasilavasukul P, Standridge JH: Effect of filtration conditions on removal of emerging waterborne pathogens. JAWWA 2003, 95: 95-104.
Melnick JL, Gerba CP, Wallis C: Viruses in water. Bull World Health Organ 1978, 56: 499-508.
Keswick BH, Satterwhite TK, Johnson PC, DuPont HL, Secor SL, Bitsura JA, Gary GW, Hoff JC: Inactivation of Norwalk virus in drinking water by chlorine. Appl Environ Microbiol 1985, 50: 261-264.
Chang JCH, Ossoff SF, Lobe DC, Dorfman MH, Dumais CM, Qualls RG, Johnson JD: UV inactivation of pathogenic and indicator organisms. Appl Environ Microbiol 1985, 49: 1361-1365.
Gerba CP, Gramos DM, Nwachuku N: Comparative inactivation of enteroviruses and adenovirus 2 by UV light. Appl Environ Microbiol 2002, 68: 5167-5169.
Osawa S, Furuse K, Watanabe I: Distribution of ribonucleic acid coliphages in animals. Appl Environ Microbiol 1981, 41: 164-168.
Furuse K: Distribution of coliphages in the environment: general considerations. In Phage Ecology. Edited by: Goyal SM, Gerba CP, Bitton G. New York: Wiley-Interscience; 1987:87-123.
Chung H, Sobsey MD: Comparative survival of indicator viruses and enteric viruses in seawater and sediment. Water Sci Technol 1993, 27: 425-428.
San Martin C, Burnett RM, de Haas F, Heinkel R, Rutten T, Fuller SD, Butcher SJ, Bamford DH: Combined EM/X-ray imaging yields a quasi-atomic model of the adenovirus-related bacteriophage PRD1 and shows key capsid and membrane interactions. Structure 2001, 9: 917-930.
U.S. Environmental Protection Agency: Method 1601: male-specific (F+) and somatic coliphage in water by two-step enrichment procedure. In EPA 821-R-01-030. Office of Water, Washington, DC; 2001.
U.S. Environmental Protection Agency: Method 1602: Male-specific (F+) and somatic coliphage in water by single agar layer procedure. In EPA 821-R-01-029. Office of Water, Washington, DC; 2001.
Long SC, Sobsey MD: A comparison of the survival of F+RNA and F+DNA coliphages in lake water microcosms. J Water Health 2004, 2: 15-22.
Pang L, Close M, Goltz M, Sinton L, Davies H, Hall C, Stanton G: Estimation of septic tank setback distances based on transport of E. coli and F-RNA phages. Environ Int 2004, 29: 907-921.
Long SC, Mahar EJ, Pei R, Arango C, Shafer E, Schoenberg TH: Development of source-specific indicator organisms for drinking water. In Technical Report. American Water Works Association Research Foundation, Denver, CO; 2002.
Long SC, El-Khoury SS, Oudejans S, Sobsey MD, Vinje J: Assessment of sources and diversity of male-specific coliphages for source tracking. Environ Eng Sci 2005, 22: 367-377.
Kopecka H, Dubrou S, Prevot J, Marechal J, Lopez-Pila JM: Detection of naturally occurring enteroviruses in waters by reverse transcription, polymerase chain reaction, and hybridization. Appl Environ Microbiol 1993, 59: 1213-1219.
Metcalf TG, Melnick JL, Estes MK: Environmental virology: from detection of virus in sewage and water by isolation to identification by molecular biology – a trip of over 50 years. Annu Rev Microbiol 1995, 49: 461-487.
Haramoto E, Katayama H, Oguma K, Yamashita H, Tajima A, Nakajima H, Ohgaki S: Seasonal profiles of human noroviruses and indicator bacteria in a wastewater treatment plant in Tokyo, Japan. Water Sci Technol 2006, 54: 301-308.
Straub TM, Bentrup KH, Orosz-Coghlan P, Dohnalkova A, Mayer BK, Bartholomew RA, Valdez CO, Bruckner-Lea CJ, Gerba CP, Abbaszadegan M, Nickerson CA: In vitro cell culture infectivity assay for human noroviruses. Emerg Infect Dis 2007, 13: 396-403.
Jiang SC: Adenovirus as an index of human viral contamination. U.S. EPA Workshop on Microbial Source Tracking: 5 February 2002; Irvine 2002, 75-78.
Nishizawa T, Okamoto H, Konishi K, Yoshizawa H, Miyakawa Y, Mayumi M: A novel DNA virus (TTV) associated with elevated transaminase levels in posttransfusion hepatitis of unknown etiology. Biochem Biophys Res Commun 1997, 241: 92-97.
Okamoto H, Nishizawa T, Kato N, Ukita M, Ikeda H, Iizuka H, Miyakawa Y, Mayumi M: Molecular cloning and characterization of a novel DNA virus (TTV) associated with posttransfusion hepatitis of unknown etiology. Hepatol Res 1998, 10: 1-16.
Miyata H, Tsunoda H, Kazi A, Yamada A, Khan MA, Murakami J, Kamahora T, Shiraki K, Hino S: Identification of a novel GC-rich 113-nucleotide region to complete the circular, single-stranded DNA genome of TT virus, the first human circovirus. J Virol 1999, 73: 3582-3586.
Biagini P, Gallian P, Attoui H, Cantaloube JF, de Micco P, de Lamballerie X: Determination and phylogenetic analysis of partial sequences from TT virus isolates. J Gen Virol 1999, 80: 419-424.
Luo K, He H, Liu Z, Liu D, Xiao H, Jiang X, Liang W, Zhang L: Novel variants related to TT virus distributed widely in China. J Med Virol 2002, 67: 118-126.
Nishizawa T, Okamoto H, Tsuda F, Aikawa T, Sugai Y, Konishi K, Akahane Y, Ukita M, Tanaka T, Miyakawa T, Mayumi M: Quasispecies of TT virus (TTV) with sequence divergence in hypervariable regions of the capsid protein in chronic TTV infection. J Virol 1999, 73: 9604-9608.
Leary TP, Erker JC, Chalmers ML, Desai SM, Mushahwar IK: Improved detection systems for TT virus reveal high prevalence in humans, non-human primates and farm animals. J Gen Virol 1999, 80: 2115-2120.
Vaidya SR, Chitambar SD, Arankalle VA: Polymerase chain reaction-based prevalence of hepatitis A, hepatitis E and TT viruses in sewage from an endemic area. J Hepatol 2002, 37: 131-136.
Haramoto E, Katayama H, Oguma K, Yamashita H, Nakajima E, Ohgaki S: One-year monthly monitoring of Torque teno virus (TTV) in wastewater treatment plants in Japan. Water Res 2005, 39: 2008-2013.
Diniz-Mendes L, de Paula VS, Luz SLB, Niel C: High prevalence of human Torque teno virus in streams crossing the city of Manaus, Brazilian Amazon. J Appl Microbiol 2008, 105: 51-58.
Springfeld C, Bugert JJ, Schnitzler P, Tobiasch E, Kehm R, Darai G: TT virus as a human pathogen: significance and problems. Virus Genes 2000, 20: 35-45.
Bendinelli M, Pistello M, Maggi F, Fornai C, Freer G, Vatteroni L: Molecular properties, biology, and clinical implications of TT virus, a recently identified widespread infectious agent of humans. Clin Microbiol Rev 2001, 14: 98-113.
Ross RS, Viazov S, Runde V, Schaefer UW, Roggendorf M: Detection of TT virus DNA in specimens other than blood. J Clin Virol 1999, 13: 181-184.
Okamoto H, Takahashi M, Nishizawa T, Tawara A, Sugai Y, Sai T, Tanaka T, Tsuda F: Replicative forms of TT virus DNA in bone marrow cells. Biochem Biophys Res Comm 2000, 270: 657-662.
Okamoto H, Ukita M, Nishizawa T, Kishimoto J, Hoshi Y, Mizuo H, Tanaka T, Miyakawa Y, Mayumi M: Circular double-stranded forms of TT virus DNA in the liver. J Virol 2000, 74: 5161-5167.
Okamoto H, Nishizawa T, Takahashi M, Asabe S, Tsuda F, Yoshikawa A: Heterogeneous distribution of TT virus of distinct genotypes in multiple tissues from infected humans. Virology 2001, 288: 358-368.
Pollicino T, Raffa G, Squadrito G, Costantino L, Cacciola I, Brancatelli S, Alafaci C, Florio MG, Raimondo G: TT virus has ubiquitous diffusion in human body tissues: analyses of paired serum and tissue samples. J Viral Hepat 2003, 10: 95-102.
Griffiths P: Time to consider the concept of a commensal virus? Rev Med Virol 1999, 9: 73-74.
Simmonds P, Prescott LE, Logue C, Davidson F, Thomas AE, Ludlam CA: TT virus – part of the normal human flora? J Infect Dis 1999, 180: 1748-1750.
Takayama S, Miura T, Matsuo S, Taki M, Sugh S: Prevalence and persistence of a novel DNA TT virus (TTV) infection in Japanese hemophiliacs. Br J Haematol 1999, 104: 626-629.
Verani M, Casini B, Battistini R, Pizzi F, Rovini E, Carducci A: One-year monthly monitoring of Torque teno virus (TTV) in river water in Italy. Water Sci Technol 2006, 54: 191-195.
de Paula VS, Diniz-Mendes L, Villar LM, Luz SL, Silva LA, Jesus MS, da Silva NM, Gaspar AM: Hepatitis A virus in environmental water samples from the Amazon Basin. Water Res 2007, 41: 1169-1176.
Abe K, Inami T, Asano K, Miyoshi C, Masaki N, Hayashi S, Ishikawa K-I, Takebe Y, Win KM, El-Zayadi AR, Han K-H, Zhang DY: TT virus infection is widespread in the general populations from different geographic regions. J Clin Microbiol 1999, 37: 2703-2705.
Desai SM, Muerhoff AS, Leary TP, Erker JC, Simons JN, Chalmers ML, Birkenmeyer LG, Pilot-Matias TJ, Mushahwar IK: Prevalence of TT virus infection in US blood donors and populations at risk for acquiring parenterally transmitted viruses. J Infect Dis 1999, 179: 1242-1244.
Yates MV: Classical indicators in the 21st century – far and beyond the coliform. Water Environ Res 2007, 79: 279-286.
Hill VR, Kahler AM, Jothikumar N, Johnson TB, Hahn D, Cromeans TL: Multistate evaluation of an ultrafiltration-based procedure for simultaneous recovery of enteric microbes in 100-liter tap water samples. Appl Environ Microbiol 2007,73(13):4218-4225.
Okamoto H, Akahane Y, Ukita M, Fukuda M, Tsuda F, Miyakawa Y, Mayumi M: Fecal excretion of an nonenveloped DNA virus (TTV) associated with posttransfusion non-A-G hepatitis. J Med Virol 1998, 56: 128-132.
Maggi F, Fornai C, Zaccaro L, Morrica A, Vatteroni ML, Isola P, Marchi S, Ricchiuti A, Pistello M, Bendenelli M: TT virus (TTV) loads associated with different peripheral blood cell types and evidence for TTV replication in activated mononuclear cells. J Med Virol 2001, 64: 190-194.
Mariscal LF, Lopez-Alcorocho JM, Rodriguez-Inigo E, Ortiz-Movilla N, de Lucas S, Bartolome J, Carreno V: TT virus replicates in stimulated by not in nonstimulated peripheral blood mononuclear cells. Virology 2002, 301: 121-129.
Desai M, Pal R, Deshmukh R, Banker D: Replication of TT virus in hepatocyte and leucocyte cell lines. J Med Virol 2005, 77: 136-143.
Acknowledgements
This material is based upon work supported under a National Science Foundation Graduate Research Fellowship.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
All authors contributed equally to this manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Griffin, J.S., Plummer, J.D. & Long, S.C. Torque teno virus: an improved indicator for viral pathogens in drinking waters. Virol J 5, 112 (2008). https://doi.org/10.1186/1743-422X-5-112
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1743-422X-5-112