
Abstract
Background
Ethiopia is the second most populous country in Africa with high fertility and fast population growth rate. It is also one of the countries with high maternal and child mortality rate in sub-Saharan Africa Family planning is a crucial strategy to halt the fast population growth, to reduce child mortality and improve maternal health (Millennium Development Goal 4 and 5). Therefore, this study aimed to assess the prevalence and determinants of modern contraceptive utilization among married women of reproductive age group.
Methods
A community based cross-sectional study was conducted from August 15 to September 1, 2010 among married women aged 15–49 years in Debre Birhan District. Multistage sampling technique was used to select a total of 851 study participants. A pre-tested structured questionnaire was used for gathering data. Bivariate and multivariate logistic regression analyses were performed using SPSS version 16.0 statistical package.
Results
Modern contraceptive prevalence rate among currently married women was 46.9%. Injectable contraceptives were the most frequently used methods (62.9%), followed by intrauterine device (16.8%), pills (14%), norplant (4.3%), male condom (1.2%) and female sterilization (0.8%). Multiple logistic regression model revealed that the need for more children (AOR 9.27, 95% CI 5.43-15.84), husband approve (AOR 2.82, 95% CI 1.67-4.80), couple’s discussion about family planning issues (AOR 7.32, 95% CI 3.60-14.86). Similarly, monthly family income and number of living children were significantly associated with the use of modern contraceptives.
Conclusion
Modern contraceptive use was high in the district. Couple’s discussion and husband approval of contraceptives use were significantly associated with the use of modern contraceptives. Therefore, district health office and concerned stakeholders should focus on couples to encourage communication and male involvement for family planning.
Similar content being viewed by others



Background
In 2011, world population stood at 7 billion. Africa accounts more than 1 billion of world population of which, Ethiopia, the second populous country in Africa contributes 87.1 million people [1]. The average total fertility rate worldwide ranges from 1.7 children per woman in more developed countries to 4.6 in the least developed countries. Total fertility rate in Ethiopia is 5.3 children per woman [1]. This puts Ethiopia among countries with highest total fertility rates in the world. For fertilities to fall to those low levels, increases the use of family planning methods plays a significant contribution especially in less developed countries including Ethiopia [1, 2].
At present, family planning service which is free of cost is provided in both governmental and NGO health facilities in Ethiopia, including hospitals, clinics, health centers, and health stations [3]. But , Ethiopia is among countries with low contraceptive prevalence rate, with only 14% and 16%, national and Amhara National Regional State contraceptive prevalence rate among married women, respectively [2, 4]. This was resulted high total fertility rate and unwanted pregnancy which intern affects the maternal and child health status [5].
The factors that influence contraceptive practice are multifaceted and challenging. Several studies evident that most women’s knowledge and use of contraception is associated with socio-demographic, socio-cultural, socio economic, source of information and family planning factors. For instance, according to different study findings socio-demographic and economic, obstetric and media exposure related factors were found to contribute on the use of modern contraceptive [6–24].
Considering the present lower utilization of contraceptives achieving the MDGs will be a major challenge for Ethiopia. Therefore, the identification of the prevalence and possible factors that determine the utilization of contraceptives in the study area will have greater input to program managers for designing programs, proper implementation and evaluation of their contribution regarding family planning.
Methods
Study design and setting
A community based cross-sectional study was conducted from August 15 to September 1, 2010 in Debre Birhan district, North Shoa Administrative Zone, Amhara National Regional State (ANRS), Ethiopia. The district has 9 administrative kebeles. The district/Debre Birhan town is located at 130 km North of Addis Ababa, capital city of Ethiopia. Based on the 2007 population and housing census, the total population size of the district estimated to be 72,097 [19]. The number of households in the district was estimated to be 16,767 at the time of the study. According to the information obtained from District Health Office; in the district there are 1 hospital, 1 health center, 18 clinics and 4 health posts which render health services for the community. Family planning service is available in most of the health facilities including health posts.
Sample size and sampling techniques
The source population was all currently married women found in the district, and the study population was currently married women who live in the selected kebeles of each stratum. Currently married women age 15 to 49 years in selected kebeles in each stratum were included.
Assuming 29% modern CPR, 95% confidence level, 4.5% margin of error and design effect of 2, the total sample size required was determined to be 869. A multi-stage sampling technique was employed for the selection of the sampling units. In the district there were 9 kebeles, of which a total of 5 kebeles were selected using simple random sampling method.
The sample size for each of the selected kebeles was determined proportionally to the size of the women age 15–49 years of each kebele. Then, systematic sampling method was employed to select the households from each kebele. The first household interviewed was determined from the kebele house number register using simple random sampling method. The next household was identified systematically (H/h)th by going in a clockwise direction. In cases of selected household with more than one eligible respondent, only one respondent was chosen by lottery method.
Data collection procedures
Data were collected on utilization of modern contraceptive (female sterilization, male sterilization, the pill, the intrauterine device (IUD), injectables, implants, male condom, female condom, and diaphragm/foam/jelly) and traditional methods (rhythm (periodic abstinence), withdrawal, and folk), socio-demographic characteristics, reproductive and FP factors, and Programmatic factors.
First, a structured and pre-tested questionnaire was prepared in English and then translated into Amharic, the Local language. A questionnaire interview, which was prepared in the Amharic language, was used for data collection. The data was collected by 5 female diploma nurses. The data collectors were supervised daily by two supervisors. The filled questionnaires were checked daily by the supervisors and principal investigator.
Data collectors approached and interviewed the selected respondents after informed consent had been obtained. The women, who were not available in the first visit, were revisited for two more times. During the revisit, the women in the next household were interviewed in place of those women who were not found.
Data processing and analysis
The data gathered through the structured questionnaire were entered and analyzed using SPSS version 16. Besides, the data were checked and cleaned for their completeness and errors in data entering. Frequency was run and double data entry on 10% of the questionnaires was performed to check data entry errors. To explain the study population in relation to the relevant variables, descriptive statistics were used. Association between dependent and independent variables was assessed and its strength was presented using odds ratios and 95% confidence intervals. Bivariate followed by multivariate logistic regression analysis were also carried out to control confounding effects of variables.
Ethical consideration
Primarily, ethical clearance was obtained from the Institutional Review Board of the University of Gondar, School of Public Health. Later on, formal letter of cooperation was written for District Health Office. Consent from District Health Office and respective kebeles was also obtained. The data collectors collected the information after obtaining verbal consent from each participant. Respondents were informed that they could refuse or discontinue participation at any time they wanted and they were also informed that they could ask anything about the study. Information was recorded anonymously and confidentiality was assured throughout the study period. A woman who did not practice was advised about the benefits of contraceptive usage and encouraged to communicate with health workers in the district for some more information on it.
Results
-
A.
Socio-demographic characteristics of the respondents
A total of 851 currently married women responded to the questionnaire, which yields a response rate of 97.9%. Six hundred fifty two (76.6%) of the respondents were from urban areas and the remaining 199 (23.4%) were from the rural areas. The mean age of the respondents was 29.49 years (29.49 ± 6.57 SD). Concerning educational status, 190 (22.3%) of the respondents were unable to read and write, 77 (9%) and 100 (11.8%) of the women and husbands were able to read and write, respectively. Two hundred eighty (32.9%) of the women had attended primary education, 225 (26.6%), were educated to the level of secondary education and the rest 79 (9.3%), attended to college or university level (Table 1).
Table 1 Socio-demographic and economic characteristics of currently married women in Debre Birhan District, August 2010 -
B.
Women’s knowledge and practice of modern contraceptive methods
Eight hundred thirty eight (98.5%) of the respondents heard about family planning and were able to mention at least one method. The most commonly reported modern family planning methods were Injectable 815 (98.9%). Regarding the advantages, 591 (70.5%) and 407 (48.6%) of women reported that contraceptive methods have advantage of spacing children and limiting the number of children respectively (Figure 1 and Table 2).
Figure 1 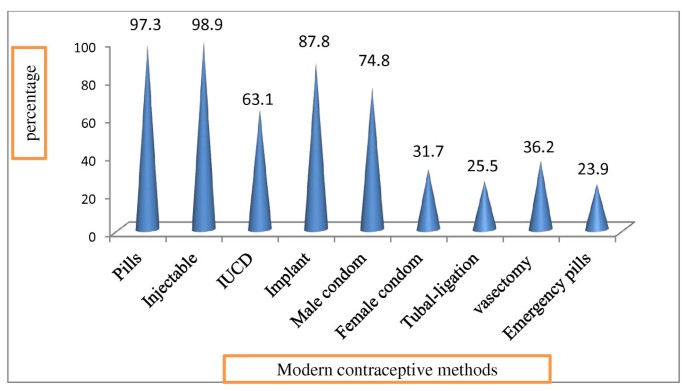
Bar graph showing respondent’s Knowledge of each of modern contraceptive methods in Debre Birhan District, August 2010.
Table 2 Knowledge and practice of modern family planning methods among currently married women in Debre Birhan District, August 2010 In this study, 448 (52.6%) of women had ever used family planning methods. Three hundred ninety nine (46.9%) [317/652 (48.62%) urban and 82/199 (41.21%) rural] of married women were currently using modern family planning methods. Concerning the types of methods, majority of the respondents were using injectable which is 251 (62.9%) (Table 2).
Among women who had ever used contraceptives, 49 (10.94%) discontinued taking contraceptives. Study participants were forwarded many different reasons for discontinuing or never using modern contraceptives. One hundred sixty (35.5%) need to have more children, 82 (9.6%) due to use of traditional methods, 56 (12.4%) were due to religious prohibition, 56 (12.4%) husband disapproval, 66 (14.6%) fear or/and perceived side effects of contraceptives, like being infertile and developing medical illness such as hypertension were the commonest side effects which perceived by this study participants, 16 (3.9%) due to little pregnancy risk related with being older reproductive age group (45–49) and 13 (2.9%) were related to low awareness about modern family planning (Figure 2).
Figure 2 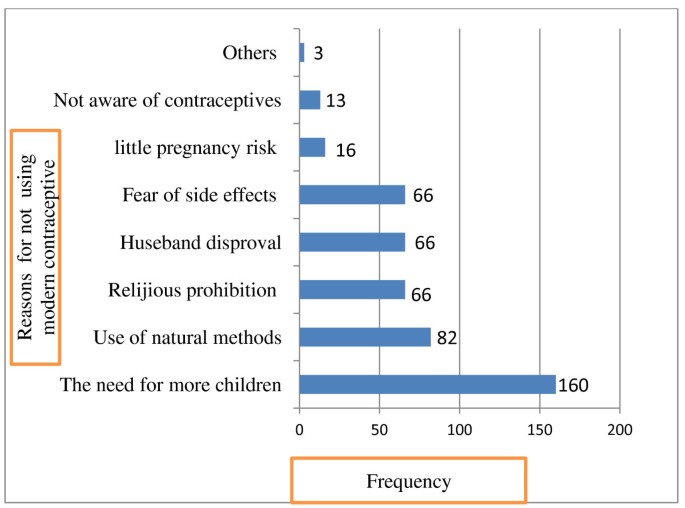
Bar graphs showing reasons for not use or discontinuation of modern contraceptive among currently married women in Debre Birhan District, August 2010.
-
C.
Determinants of modern contraceptive use among currently married women in the district
In the bivariate analysis, educational status of women and husband, desire for more children, number of living children, discussion with health extension workers, discussion of wives with their husband, approval of modern contraceptive use by husband and status of decision making on modern contraceptives were found to be significantly associated with the use of contraceptives with P-value <0.01.


Multivariate analysis was employed to assess the net effect of selected socio-demographic, reproductive, family planning knowledge, perception and program related explanatory variables on the use of modern contraceptive methods. The result of multiple logistic regression model revealed that respondents desire for more children, number of living children, husband approval of use of modern contraceptive methods, husband-wife communication and family monthly income were significantly associated with use of contraceptives methods.
Women who desire another children after two years were 5.71 times more likely to use modern contraceptive than those who desire another child within two years (AOR 5.71, 95% C.I = 3.48-9.37) and those women who do not desire more children at all were 9.27 times more likely to use modern contraceptive methods than those who desire another child within two years (AOR 9.27, 95% C.I. = 5.43-15.84). In addition, those women who perceive/report their husband approve or accept their use of modern contraceptive were almost three times more likely to use modern contraceptive than those who perceive/report their husband would disprove/not accept the use of modern contraceptives (AOR 2.82, 95% C.I 1.67-4.80).
This study also showed that as the number of husband–wife communication increase the use of modern contraceptive also increased when compared with those women who did not communicate with their husband. Those women who had discussion with their husband once were 4.50 times more likely to use modern contraceptives than those women not discussed (AOR 4.50, 95% C.I 2.15–9.42), and those women discussed more than three times were 7.32 times more likely to use modern contraceptives than those women not discussed with their husbands at all about family planning use (AOR 7.32, 95% C.I 3.60–14.86).
Furthermore, the study revealed that family monthly income was significant associated with the use of modern contraceptives. But variables like educational status of the women and husband, residence, women and husband occupation, discussion with health extension workers and some others which are significant or/and P-value < 0.2 in bivariate analysis were not statistically significant with the use of modern contraceptives in the multiple logistic regression model (Table 3).
Discussion
This study assessed the prevalence and determinants of modern contraceptive utilization among married women of reproductive age in Debre Birhan district. Nearly half (46.9%) of participants were currently using modern contraceptive methods. This finding was similar with the study done in Adama Town (47%) and also the 51.6% CPR in Ethiopia [20, 21]. But this finding is higher than the previous studies conducted in Dembia District, Northwest Ethiopia, in 2004 which showed 14% CPR [15]. The reason for this could be the fact that 76.6% of the study participants were from urban areas in this study while only 41% from the study in Dembia [15]. In addition, increase in the availability and accessibility of different family planning services in both urban and rural areas of Debre Birhan district with active involvement of health extension worker on provision of FP education and service might have increased the use of contraceptive methods.
Most of the study participants were using injectable type of contraceptive methods. This choice could be due to its convenience of not being taken on daily basis and having comfortable ways of administration on top of the availability of this method than others. Child spacing was the main reason for women to use modern contraceptives. On the other hand the need for more children was the main reason for not using modern contraceptive methods. This is in line with findings from northwest Ethiopia and Sudan, Bangladesh and Pakistan [6, 10, 12, 14, 15].
In this study, those women who desire another child after two years were nearly six times more likely to use modern contraceptives than those women who desire another child within two years. This finding is in line with the study conducted in Bangladesh and Pakistan [6, 16]. Women’s internal motivations to achieve their child spacing goal could be the possible reason for higher level of contraceptive use.
Women who had one or more children were more likely to use modern contraceptives than those who had no children. In contrast, women who had more than 5 children were almost three times less likely to use modern contraceptives compared with women who had no children. This could be for the reason that those women who had more than 5 children were at the older age of reproduction and they might have perceived not to be at risk of pregnancy. Secondly, older women are more likely to practice sex infrequently. This finding is similar to previous reports from Bangladesh, Pakistan, and Tanzania which reported that as the number of living children increases, use of modern contraceptives increase [6, 8, 16].
This study revealed that women who discussed with their husband about modern contraceptives were about seven times more likely to use modern contraceptive methods than women who did not discuss at all. This is in line with studies conducted from Jimma (south west Ethiopia), Kenya, Tanzania, Nigeria and Bangladesh [6, 8, 9, 13, 14, 17].
This study also indicated that those women whose husband’s approve using modern contraceptives were almost three times more likely to use modern contraceptives. This is in line with the previous studies in Pakistan and Ethiopia [9, 15, 22, 23]. This implies that male involvement has an important role on the use of modern contraceptives.
The main strength of this study is that, being community based, it could reflect the actual experience of the married women during the study period. As limitations of this study, information about the husband were indirectly obtained from women. Additionally, similarities of living standards in some rural and urban areas might have underestimated the rural–urban difference in the use of contraceptive methods. On the other hand, being most of the residences in the district were live in urban areas might not able to identify factors which associate with the use of modern contraceptive in the rural areas.
This study were tried to see the strength of the association between the outcome and explanatory variables beyond simply identifying those variables which are statistically significant for the use of modern contraceptive specifically in the study area.
In conclusion, the modern contraceptive use in this district among currently married women of reproductive age group is high. Couple’s communication/discussion and husband’s approval about contraceptives were significantly associated with modern contraceptive use. However, women’s demand for more children has a negative effect on the use of modern contraceptive methods. Improvement in family income or socio-economic status to the higher level has an important role in upgrading usage of modern contraceptive.
Health service programs and strategies of the country at each level of health care delivery system need to consider the involvement of males for modern contraceptives utilization. Hence, governmental and nongovernmental organizations, health facilities and other stakeholders need to ensure availability, accessibility and sustained advocacy for use of available contraceptive methods for married couples. Lastly, we recommend that researchers to investigate husbands’ perception and acceptance toward contraceptive use by their couples.
Abbreviations
- ANRS:
-
Amhara National Regional State
- CPR:
-
Contraceptive prevalence rate
- EDHS:
-
Ethiopian demographic health survey
- FGAE:
-
Family guidance association of ethiopia
- FP:
-
Family planning
- HEW:
-
Health extension worker
- IUCD:
-
Intrauterine contraceptive device
- MDG:
-
Millennium development goal
- NGO:
-
Non-governmental organization
- RH:
-
Reproductive health
- SD:
-
Standard deviation
- WHO:
-
World Health Organization.
References
Population Reference Bureau: World population data sheet. 2011, [http://www.prb.org/pdf11/2011population-data-sheet_eng.pdf]
Central Statistical Agency: ICF International: Ethiopian Demographic and Health Survey. 2006, Addis Ababa, Ethiopia, Calverton, Maryland, USA: Central Statistical Agency and ORC Macro, [http://www.etharc.org/amhara/Asset/Dowloadables/DHS%202005%20Ethiopia.pdf]
United Nations (UN): World Contraceptive Use 2007. 2008, New York: UN Department of Economic and Social Affairs, Population Division
Korra A: Community based family planning services: a performance assessment of the jimma FPCBD project. Ethiop J Health Dev. 1997, 11 (1): 17-22.
Hailemariam A, Mekbib T, Fantahun M: Family Planning in Ethiopia. Epidemiology and Ecology of Health and Disease in Ethiopia. Edited by: Berhane Y, Hailemariam D, Kloos H. 2006, Addis Ababa: Shama Books, 267-285.
Mostafa K, Aynul I: Contraceptive Use: socioeconomic correlates and method choices in rural Bangladesh. Asia Pac J Public Health. 2010, 22 (4): 436-450. 10.1177/1010539510370780.
Timothy C, Nelson W, Tom K: Contraceptive Use among women of reproductive Age in Kenya’s city slums. Int J Bus Soc Sci. 2011, 2 (1): 22-43.
Lwelamira J, Mnyamagola G, Msaki MM: Knowledge, attitude and practice (KAP) towards modern contraceptives among married women of reproductive Age in mpwapwa district, central Tanzania. Curr Res J Soc Sci. 2012, 4 (3): 235-245.
World Health Organization (WHO): Global and Regional Estimates of the Incidence of Unsafe Abortion and Associated Mortality in 2000. 2004, Geneva: WHO
Mekonnen W, Worku A: Determinants of low family planning use and high unmet need in butajira district. South central Ethiopia. Reprod Health. 2011, 8: 37-10.1186/1742-4755-8-37.
Ali S, Rozi S, Mahmood M: Prevalence and factors associated with practice of modern contraceptive methods among currently married women in district naushahro feroze Karachi Pakistan. JPMA. 2004, 54: 461-465.
Ibnouf A, Van Den Born H, Maarse J: Utilization of family planning services by married Sudanese women of reproductive age. East Mediterr Health J. 2007, 13 (6): 1372-1381.
Olugbenga-Bello A, Abodunrin O, Adeomi A: Contraceptive practices among women in rural communities in south-western Nigeria. Glob J Med Res. 2011, 11 (2): 1-
Beekle A, Mccabe C: Awareness and determinants of family planning practice in Jimma, Ethiopia. Int Nurs Rev. 2006, 53: 269-276. 10.1111/j.1466-7657.2006.00492.x.
Kebede Y: Contraceptive prevalence in dembia district, northwest Ethiopia. Ethiop J Health Dev. 2006, 20 (1): 32-38.
Stephenson R, Hennink M: Opportunities and choices working paper number 2 February 2004. Barriers to family planning service use among the urban poor in Pakistan. [http://www.socstats.soton.ac.uk/choices/Pakistan%20barriers%20WP2.PDF]
Haile A, Enqueselassie F: Influence of women’s autonomy on couple’s contraception use in Jimma town Ethiopia. Ethiop J Health Dev. 2006, 20 (3): 145-151.
Mon M, Liabsuetrakul T: Factors influencing married youths’ decisions on contraceptive use in a rural area of Myanmar, Thailand. Southeast Asian J Trop Med Public Health. 2009, 40 (5): 1057-1064.
Federal Democratic Republic of Ethiopia population and census commission: Summary and Statistical Report of the 2007 Population and Housing Census Results. 2008, Addis Ababa, Ethiopia
Biruk T, Assefa H, Georges R: The prevalence of Covert use of contraceptives in Nazareth/Adama town. Eur J Contracept Reprod Health Care. 2008, 13 (2): 63-
Mulu W, Tilahun H: Modeling trends of health and health related indicators in Ethiopia (1995–2008): a time-series study. Bio-Med Cent Health Res Policy Syst. 2009, 7: 29-46. 10.1186/1478-4505-7-29.
Pandey S, Karki S, Pradhan A: Practice of contraceptives. J Inst Med. 2009, 31 (3): 3-9.
Abraham W, Adamu A, Deresse D: The involvement of Men in family planning an application of Tran-theoretical model in wolaita soddo town south Ethiopia. Asian J Med Sci. 2010, 2 (2): 44-50.
Mekonnen A, Sophie A, Dramaix M, Bantayehu A: Factors affecting continuity and success of community–based reproductive health service program in rural community of northeast Ethiopia. East Afr Med J. 2008, 85 (10): 478-499.
Acknowledgments
The authors are indebted to the College of Medicine and Health Sciences, University of Gondar for funding this research project. Our sincere gratitude also goes to all supervisors, data collectors, study participants, Debre Birhan District Health Office and respective kebele administrations for their cooperation and support during the study period.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
AM designed the study, participated in the data collection, performed analysis and interpretation of data and drafted the paper and prepared the manuscript. BM, AF and DW assisted in the design, approved the proposal with some revisions, participated in data analysis and revised subsequent drafts of the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an open access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Mohammed, A., Woldeyohannes, D., Feleke, A. et al. Determinants of modern contraceptive utilization among married women of reproductive age group in North Shoa Zone, Amhara Region, Ethiopia. Reprod Health 11, 13 (2014). https://doi.org/10.1186/1742-4755-11-13
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1742-4755-11-13