
Abstract
Background
Stem cell therapy is a promising treatment for cerebral palsy, which refers to a category of brain diseases that are associated with chronic motor disability in children. Autologous MSCs may be a better cell source and have been studied for the treatment of cerebral palsy because of their functions in tissue repair and the regulation of immunological processes.
Methods
To assess neural stem cell–like (NSC-like) cells derived from autologous marrow mesenchymal stem cells as a novel treatment for patients with moderate-to-severe cerebral palsy, a total of 60 cerebral palsy patients were enrolled in this open-label, non-randomised, observer-blinded controlled clinical study with a 6-months follow-up. For the transplantation group, a total of 30 cerebral palsy patients received an autologous NSC-like cells transplantation (1-2 × 107 cells into the subarachnoid cavity) and rehabilitation treatments whereas 30 patients in the control group only received rehabilitation treatment.
Results
We recorded the gross motor function measurement scores, language quotients, and adverse events up to 6 months post-treatment. The gross motor function measurement scores in the transplantation group were significantly higher at month 3 (the score increase was 42.6, 95% CI: 9.8–75.3, P=.011) and month 6 (the score increase was 58.6, 95% CI: 25.8–91.4, P=.001) post-treatment compared with the baseline scores. The increase in the Gross Motor Function Measurement scores in the control group was not significant. The increases in the language quotients at months 1, 3, and 6 post-treatment were not statistically significant when compared with the baseline quotients in both groups. All the 60 patients survived, and none of the patients experienced serious adverse events or complications.
Conclusion
Our results indicated that NSC-like cells are safe and effective for the treatment of motor deficits related to cerebral palsy. Further randomised clinical trials are necessary to establish the efficacy of this procedure.
Similar content being viewed by others


Background
Childhood cerebral palsy is a non-progressive brain disease that results from various cerebral insults that can occur before birth and 1 month after birth. Patients primarily present with motor developmental delay or motor dysfunction and possible mental retardation, epilepsy, behavioural disorders, and sensory and perceptual disturbances. Hypoxic ischemic encephalopathy and premature cerebral palsy are the most common causes of cerebral palsy [1, 2]. A census conducted in six cities in 1998 revealed that the prevalence of cerebral palsy in children 1 to 6 years of age was 1.92% [3]. The incidence of cerebral palsy in pre-schoolers in the United States has ranged from 3%–4% [4]. Children with cerebral palsy may impart a heavy burden on their families and society. Conventional therapies for treating cerebral palsy include physical therapy, motor function training, language training, orthomorphia, neurotomy, and intramuscular injections of botulinum toxin A. However, these methods have not improved cerebral injuries in patients with moderate-to-severe cerebral palsy [5, 6].
Stem cell transplantation is a novel and promising treatment for cerebral palsy [7, 8]. However, this procedure is still in the initial stages of investigation [9], and there have not been any published results from clinical trials to date [10]. Several types of stem cells are candidates for the treatment of cerebral palsy, such as human embryonic neural stem cells, olfactory ensheathing cells, umbilical mesenchymal stem cells, and bone marrow MSCs [7, 8, 11, 12]. However, human embryonic neural stem cells and olfactory ensheathing cells are difficult to apply in clinical practice due to the potential immunological rejection of xenogenic cells, ethical arguments, a high risk of transplantation within the brain, and the difficulty of repeated transplantations [9]. Autologous MSCs may be a better cell source and have been studied for the treatment of cerebral palsy because of their functions in tissue repair and the regulation of immunological processes [13]. In addition, previous studies have demonstrated that human bone marrow MSCs exhibit neural phenotypes and can differentiate into NSC-like cells in vitro [14–16]. Moreover, intraspinal cell therapy has led to better outcomes for neurological disorders in animal-based studies [17, 18] and clinical trails [19, 20]. Therefore, we hypothesized that an intraspinal infusion of autologous MSCs-derived NSC-like cells may be a novel treatment for patients with moderate-to-severe cerebral palsy. In a controlled clinical study, we investigated the clinical outcomes of 30 cerebral palsy patients who underwent transplantation with NSC-like cells and who were followed up for 6 months.
Methods
Study design and patient enrolment
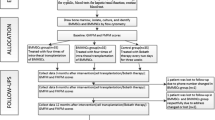
An open-label, non-randomised, observer-blinded controlled clinical study was conducted. The study was approved by the Ethics Committee and the Science Committee of the Armed Police General Hospital of Zhejiang Province, China and was registered in the China Clinical Trial Registry (ChiCTR-TRC-12002056). Informed consent was obtained from all of the patients or their parents. A total of 60 patients with cerebral palsy with Gross Motor Function Classification System (GMFCS, corresponding to GMFCS E&R 2007) levels III-V were enrolled in this study from June 2010 to June 2011. Overall, 30 patients were treated with conventional methods and stem cell transplantation and were included in the transplantation group. An additional 30 patients with cerebral palsy were only treated with conventional methods and were included in the control group. The study protocol is shown in Figure 1.

Study protocol. A total of 60 patients with cerebral palsy with Gross Motor Function Classification System (GMFCS) levels III-V were enrolled in this study. For the transplantation group, a total of 30 cerebral palsy patients received the autologous NSC-like cell transplantation and rehabilitation treatments whereas 30 patients in the control group only received rehabilitation treatment. The study protocol is shown. Motor ability was assessed using the Gross Motor Function Measure questionnaire-88. Language ability was measured using the Gesell questionnaire. All of the assessments were conducted by a specifically assigned person, and the assessment results were recorded in the case report. A safety evaluation was performed during the 6-month follow-up to detect instances of death, any serious clinical events, abnormal electroencephalogram results, and neuroimaging complications.
The patients were enrolled according to the following inclusion criteria [3]: (1) the presence of non-progressive, neurological disorders that appeared in infancy or early childhood; (2) the appearance of retardation including the lack of development or ability in sporting activities and the persistence of posture obstacles, which may be associated with lesions that affect feeling, perception, cognition, communication, and behaviour, epilepsy or secondary musculoskeletal problems; (3) no diagnosis of other diseases, such as metabolic or degenerative diseases, that could induce central paralysis and transient retardation in a normal person; and (4) negative serological markers for AIDS, hepatitis, and syphilis. Patients with severe anaphylactic or autoimmune diseases were excluded from the transplantation group.
Autologous MSC cultures
Patients fasted for 4–6 hours and went without water 1 hour before the collection of autologous bone marrow specimens. The patients were injected with 5 mg/kg phenobarbital, 0.01 mg/kg atropine, and 4 mg/kg ketamine in the aseptic collecting room 30 minutes before specimen collection. In addition, 8–25 mL of bone marrow (0.6-1.0 mL/kg of body weight) was collected from the right posterior superior iliac spine according to conventional bone marrow aspiration procedures. A total of 100 U/mL heparin was added to the collecting tube as an anticoagulant. Following current manufacturing best practices, mononuclear bone marrow cells were isolated by Percoll (1.073 g/mL) centrifugation and were allowed to adhere to a flask for 72 hours in low glucose Dulbecco’s Modified Eagle’s Medium (Gibco-Invitrogen) at 5% CO2 and 37°C, and the media were changed every 3 days. The cells with a strong positive signal for the multipotential marker Oct 4 and Nanog were screened for further cloning and culturing (Additional file 1: Figure S1A). The cell phenotypes were assessed by flow cytometry. The results indicated that CD34 and CD45 were negative, and the positive rates of CD29 and CD44 were above 95% (Additional file 1: Figure S1B). The ability of the cells to differentiate into adipocytes and osteocytes in culture was confirmed in vitro following the criteria of the 2006 International Society of Cellular Therapy [21]. At 70%–80% confluence, the cells were detached and replated at 5 × 106/175 cm2 in culture to process for neural differentiation and confirm negativity for endotoxin, hepatitis C virus, hepatitis B virus, HIV, syphilis, fungus, Myco plasma species, and Chlamydia before infusion. A G-banding karyotype analysis was performed to confirm the absence of chromosomal aberrations in the final cellular product. The MSCs were continuously cultured without cryopreservation and were thawed before transplantation. Supplementary methods were shown in more detail (see Additional file 1).
Autologous NSC-like cells induction and differentiation
At 30%-40% confluence, a combination of 20 ng/ml recombinant human FGF basic (bFGF) and 10 nM retinoic acid was added to the medium for 12 hours to transform the MSCs, and the differentiation capacity was evaluated after 14 days [14]. Growth curves were drawn to assess the proliferation ability of the MSCs and the transformed cells (Figure 2A). In total, 1 × 104 of the transformed cells were collected to prepare slices for immunofluorescence staining, and 50%–70% of the cells expressed Nestin and Tuj-1 (Figure 2B). A total of 1 × 106 cells were co-labelled with antibodies against Nestin (BD Pharmingen) and Tuj-1 (Abcam) , Sox2 (Abcam) or Sox1 (Santa Cruz). According to the flow cytometry analysis, 66.83%, 90.92% and 64.71% of the induced cells expressed both Nestin and Tuj-1, Sox2 and Sox1, respectively (Figure 2B). These results suggest that the MSCs differentiated into NSC-like cells. The NSC-like cells were detached, washed three times in saline, re-suspended in saline with 5% human albumin and filtered in a 100-μm nylon filter. Approximately 100 μl of this solution was used for safety and viability tests. No chromosomal aberrations or increased telomerase activity was found for the induced NSC-like cells. In addition, a high cell viability (>90%) and the negative microbiological results ensured the quality of the cells before the transplantations. To determine whether the induced NSC-like cells could differentiate into different neural lineages, MSCs were induced for 14 days under the same conditions and were stained using antibodies against Tuj-1 (Abcam), NeuN (Abcam), Tau (Abcam), Nestin (Santa Cruz), CD44 (Santa Cruz) and GFAP (Santa Cruz). The induced cells expressed both neuron- and glial cell-specific proteins (Figure 2C).

MSCs can be induced to differentiate into NSC-like cells and exhibit multipotency by generating progenies of different neural lineages in vitro. (A) During differentiation, MSCs develop the properties of neural stem cells (NSCs). The induced cells were observed in the bright fields after 0.5 days and after 14 days. The growth curves of the MSCs and the NSC-like cells, which were obtained by enumerating the cells at each time point under a haemocytometer, are shown (n=3; the calculated doubling times were 20 hours and 40 hours, respectively). (B) After induction, the NSC-like cells were fixed, and immunofluorescence was used to detect the expression of Nestin and Tuj-1. The cells were counterstained using DAPI. The scale bar is 10 μm. To assess the induction efficiency, the cells were co-labelled with antibodies against Nestin and Tuj-1, Sox-2 or Sox1, and the proportions of double-positive cells were 66.83%, 90.92% and 64.71%, respectively. The tests were repeated three times. (C) To determine whether the induced NSC-like cells could differentiate into both neurons and glia cells, MSCs were induced for 14 days under the same conditions and stained using antibodies against neuron- and glial cell-specific proteins. The scale bar is 10 μm.
Safety evaluation of NSC-like cells in vivo in a mouse model
The MSC-derived NSC-like cells (1.0 × 106) were implanted subcutaneously into the flanks of nude mice or were transplanted intraspinally into the subarachnoid space of nude mice. No tumour formation or other adverse events were observed in mice after 3 months. The animal studies were approved by the Institutional Animal Care and Use Committee of the Second Military Medical University in Shanghai, China.
Cell transplantation therapy
Before the lumbar puncture, the patients fasted without food and water. The patients were injected with phenobarbital sodium, atropine, and ketamine according to the dose and usage guidelines before the collection of bone marrow. When the patients fell asleep, a local anaesthetic was infiltrated under the skin and a spinal needle was inserted between the lumbar vertebrae L3/L4 or L4/L5 and pushed in until the needle traversed the dura mater and the thin arachnoid membrane into the subarachnoid space. The stylet from the spinal needle was withdrawn, and drops of cerebrospinal fluid (up to 5 ml) were collected. Then, 5 ml cell suspension, which contained 1-2 × 107 of NSC-like cells, was gently injected into the subarachnoid cavity through the spinal needle. The opening pressure of the cerebrospinal fluid was measured during specimen collection using a simple column manometer. The procedure ended by withdrawing the needle while placing pressure on the puncture site. The cell transplantation was administered at intervals of 3 weeks for two cycles. In addition, the patients in the transplantation group received rehabilitation treatments at the same time.
Observation indices
As the primary measurement, the motor and language abilities of the patients were observed before treatment and at 1, 3, and 6 months post-treatment. Motor ability was assessed using the Gross Motor Function Measure (GMFM-88 or GMFM) [22] questionnaire. An example was shown in Additional file 1. Language ability was measured using the Gesell questionnaire. The language developmental quotient (LDQ) was determined using the following formula: language developmental age/present age × 100. All of the assessments were conducted by a specifically assigned person. For the observer-blinded design of the study, the patients were randomly arranged before the tests, and the examiner was blinded to the names and the grouping of patients. The assessment results were recorded in the case reports.
The secondary measurement was patient survival and the incidence of the following adverse events: (1) fever, headache, allodynia, vomiting, infection, or other reactions; (2) clinical seizures and/or epileptic discharges on a serial electroencephalogram (EEG) at any time during hospitalization; (3) new lesions in the skull according to MRI at 6 months post-procedure; and (4) other clinically significant complications from the procedure during the long-term folow-up.
Statistical analysis
The data were expressed as the mean ± S.E.M. The statistical significance of the patient ages, GMFM scores and language developmental quotients was detected using the one-way ANOVA analysis, LSD test and two-tailed Student’s t-test. The statistical significance of gender and the GMFCS levels was detected using the chi-squared test. The statistical analysis was performed using SPSS 11.0.
Results
Baseline characteristics of the patients
A total of 30 patients with cerebral palsy in GMFCS levels III-V were enrolled in this study and were included in the transplantation group. The group consisted of 14 males and 16 females with a mean age of 5.53 ± 1.20 years (range, 1–32 years). An additional 30 patients with cerebral palsy were treated with conventional methods and were included in the control group, which consisted of 14 males and 16 females with a mean age of 4.66 ± 1.31 years (range, 1–35 years). The baseline characteristics of the patients in the two groups at the study onset are shown in Tables 1–2. In addition, a comparison of the patient ages, LDQs and GMFM scores in the two groups are shown in Figure 3. No significant differences were found.

A comparison of the baseline characteristics of the patients in the two groups. (A) A comparison of the number of patients according to the Gross Motor Function Classification System (GMFCS) levels in the transplantation (Trans) and control groups. Statistically significant differences were detected using the chi-squared test. (B-D): A comparison of the mean ages (B), mean baseline Gross Motor Function Measure (GMFM) scores (C) and mean baseline language developmental quotients (LDQs) (D) of the patients in the transplantation (Trans) and control groups is shown. Statistically significant differences were detected between the groups using a Student t-test.
The MRI results from the skulls of patients with cerebral palsy can show a periventricular white matter injury (PWMI), and the pathological findings can include periventricular leukomalacia and diffused dysmyelination [23, 24]. Prasad [25] studied 102 children 1–3 years of age with cerebral palsy and found that 47.1% had a PWMI in the skull based on MRI findings. In this study, 16 of the 30 patients (54.5%) in the transplantation group had white matter injuries according to MRI.
Functional outcomes of motor development among the two groups
The motor functions of the patients were observed and evaluated using the GMFM scores before treatment and at 1, 3, and 6 months post-treatment (Table 1). The GMFM scores of all of the patients in the two groups gradually increased during the 6 months post-treatment, however, there were no significant differences in the control group. In contrast, the GMFM scores in the transplantation group at months 3 and 6 post-treatment were significantly higher compared with the baseline scores (P= 0.011 and 0.001), whereas there were no significant changes in the GMFM scores at month 1 post-treatment (P= 0.265). The GMFM score increase from baseline to month 6 post-treatment was 58.6 (95% CI: 25.8-91.4) in the transplantation group. This finding suggests that there was a significant recovery effect in motor function after the transplantation treatment. Additional movie files were shown in more detail (see Additional file 2 and 3). In addition, we found that the GMFM scores at months 3, and 6 post-treatment were significantly higher in the transplantation group compared with those in the control group (P= 0.003 and P< 0.001, respectively). However, there were no differences in the GMFM scores at month 1 post-treatment between the two groups (P= 0.089) (Figure 4A). To evaluate the impact of NSC transplantation in patients with different levels of cerebral palsy, we divided the patients according to their GMFCS levels. The results indicated that patients in the transplantation group with levels IV and V had a better recovery of motor function (Figure 4B-D).

A comparison of the kinetic Gross Motor Function Measure (GMFM) scores of the patients in the two groups. (A) A comparison of the mean GMFM scores before treatment (0 months) and at 1, 3, and 6 months post-treatment for the patients in the transplantation (Trans) and control groups. (B-D) A comparison of the mean GMFM scores for the patients with GMFCS levels III (B), IV(C) and V(D) in the transplantation (Trans) and control groups. The data were expressed as the mean ± S.E.M. Statistically significant differences were detected between the groups using a two-tailed Student’s t-test, * P< 0.05, ** P< 0.01, *** P<0.001. (E-F) Changes in the GMFM scores of the patients in the transplantation (Trans) group (E) and in the control group (F) before and after treatment. Each line indicates the kinetic scores of an individual patient.
Functional outcomes of language development among the two groups
The language abilities of the patients were observed before treatment and at 1, 3, and 6 months post-treatment. The means of the language developmental quotients of the patients in the two groups gradually increased during the 6 months post-treatment (Figure 5). However, no significant differences in the language developmental quotients were observed at months 1, 3, and 6 post-treatment when compared with the baseline quotients in both groups (P>0.05 for all). In addition, we did not find any significant differences in the language developmental quotients at months 1, 3, and 6 post-treatment between the two groups (P= 0.751, 0.522 and 0.304, respectively). This finding suggests that the recovery of language functions was not accelerated in the transplantation group.

A comparison of the kinetic language developmental quotients of the patients in the two groups. (A) A comparison of the mean language developmental quotients before (0 months) and after treatment for the patients in the transplantation (Trans) and control groups. (B-D) A comparison of the mean language developmental quotients for the patients with GMFCS levels III (B), IV(C) and V (D) in the transplantation (Trans) and control groups. No statistically significant differences were detected between the groups using a two-tailed Student’s t-test.
Adverse reactions in the transplantation group
No new neurological deficits were immediately identified after NSC treatment. All of the patients in this study were observed for more than 6 months after treatment. None of the 60 patients experienced fever, headache, allodynia, vomiting, or other serious adverse events that were related to the experimental procedure. Follow-up MRI evaluations did not show any significant anatomical or structural changes that could indicate adverse events. There was no evidence of any new ischemic, haemorrhagic, or neoplastic lesions. However, an increase in the frequency of crying was reported in one patient but resolved spontaneously 2 days after the treatment without any intervention. Other possible adverse effects or complications in the control and transplantation groups were evaluated, but no differences were observed in the frequency of new-onset morbidities between the groups.
Discussion
Improvements in perinatal emergency medicine have decreased the neonatal mortality rate, however, the incidence of hypoxic ischemic encephalopathy and premature cerebral palsy have increased over time [1]. Conventional rehabilitation treatment for cerebral palsy cannot improve the motor function of patients with moderate-to-severe chronic cerebral palsy [5, 6]. In this study, we did not find any significant improvement in the motor functions of the patients in the control group. However, in the transplantation group, our data indicated that the GMFM scores post-treatment were significantly higher after 3 months compared with the baselines scores, which suggests that the motor recovery effects were accelerated in the transplantation group. In addition, we found that patients in the transplantation group with GMFCS levels IV and V had a better recovery of motor functions. These results provide strong clinical support for MSC-derived NSC-like cells transplantation for the treatment of cerebral palsy, especially for moderate-to-severe chronic cerebral palsy.
The mechanism by which NSCs contribute to motor function recovery remains controversial. Experiments have demonstrated that transplanted NSCs exhibit strong plasticity, can easily integrate with host cells and can establish a stable synaptic connection and become functional substituting nerve cells [26–28]. Additionally, NSCs may produce neurotrophic factors that facilitate the recovery of impaired tissues in the diseased brain region [29–32]. Consistent with these findings, we found that autologous NSC-like cells derived from MSCs could differentiate into neuronal and glial lineages in vitro. Our study was not designed to address the mechanism of NSC functions in vivo, and future experiments are necessary to define the exact mechanism of therapeutic cerebral repair by NSCs.
The safety of the NSC-based cell therapy is another urgent problem. The risk for chromosomal aberrations, neoplastic transformation, increased telomerase activity, or both has been reported for human MSCs following several passages in culture in experimental settings [33]. We used early cultured MSCs (3–4 passage) that displayed normal karyotypes and telomerase activity to induce NSC-like cells. Before each treatment, we confirmed the safety of induced NSC-like cells by telomerase activity evaluation, karyotype analysis and microbiological detection. To our knowledge, there are no clinical data that support the development of neoplasms that are directly related to an autologous MSC inoculum [34, 35]. In this study, we evaluated the safety of MSCs and NSC-like cells in nude mice, and no tumour formation or other complications were found in a long-term (more than 3 months) study. Moreover, allodynia was reported to be a risk of intraspinal neural stem cell transplantation [30]. In this study, we did not find any cases of allodynia or other adverse events during the 6-month follow-up. Therefore, we confirmed that the cells in our study were safe for the patients, however, more long-term follow-up studies may be necessary to further confirm the safety of NSC-like cells.
In this study, we did not find any evidence of accelerated recovery of language function in the transplantation group. Language disorders in children with cerebral palsy are categorized as asophia, anarthria and language developmental delays [36], which are caused by a motor disturbance of the speech organs due to brain injury. Language recovery is affected by multiple factors [37]. The time period from 7–24 months after birth is important for establishing brain language signal pathways. In this study, all of the patients missed this key phase of language training. Therefore, stem cells combined with language training at an earlier stage may improve the language ability of these patients.
The main limitations of this study include the small sample size and the lack of a randomised, double-blinded, placebo-controlled design. However, we employed an observer-blinded, controlled design to minimize measurement bias. As shown in Figure 3, the baseline characteristics of the patients from the two groups are well matched, and no significant differences were found between the two groups in the comparison of the patient ages, LDQs and GMFM scores at the study onset. This study is the first reported controlled clinical trial of NSC-like cells therapy for chronic cerebral palsy, and our study provides strong clinical evidence that supports stem cell transplantation for the treatment of motor deficits related to cerebral palsy. Further randomised clinical trials are necessary to establish the efficacy of this procedure.
Conclusion
Our data indicates that the transplantation of MSC-derived NSC-like cells is safe and effective for the treatment of chronic cerebral palsy. Motor function, but not the language quotient, indicated optimal improvement 3 months after transplantation.
References
An T, Guo XQ, Pu XH: Study progress in early intervention of high- risk infants for the prevention and treatment of cerebral palsy. Clin Pediatr. 2006, 24: 696-698.
Moster D, Lie RT, Markestad T: Long-term medical and social consequences of preterm birth. N Engl J Med. 2008, 359: 262-273. 10.1056/NEJMoa0706475.
Hu YM: Jiang ZF. 2002, Zhu FT: Practice of pediatrics. People’s medical publishing house
Yeargin-Allsopp M, Van Naarden Braun K, Doernberg NS, Benedict RE, Kirby RS, Durkin MS: Prevalence of cerebral palsy in 8-year-old children in three areas of the United States in 2002: a multisite collaboration. Pediatrics. 2008, 121: 547-554. 10.1542/peds.2007-1270.
Koman LA, Smith BP, Shilt JS: Cerebral palsy. Lancet. 2004, 363: 1619-1631. 10.1016/S0140-6736(04)16207-7.
Holt RL, Mikati MA: Care for child development: basic science rationale and effects of interventions. Pediatr Neurol. 2011, 44: 239-253. 10.1016/j.pediatrneurol.2010.11.009.
Luan Z, Yin GC, Hu XH, Qu SQ, Wu NH, Yan FQ, Qian YM, Jin HY, Gong XJ: [Treatment of an infant with severe neonatal hypoxic-ischemic encephalopathy sequelae with transplantation of human neural stem cells into cerebral ventricle]. Zhonghua Er Ke Za Zhi. 2005, 43: 580-583. discussion 580
Chen GJ, Fang F, Tang YH: Cell Therapy of cerebral diseases in China: a meta-analysis. Med J Chin PAPF. 2011, 22: 216-218.
Carroll JE, Mays RW: Update on stem cell therapy for cerebral palsy. Expert Opin Biol Ther. 2011, 11: 463-471. 10.1517/14712598.2011.557060.
Trounson A, Thakar RG, Lomax G, Gibbons D: Clinical trials for stem cell therapies. BMC Med. 2011, 9: 52-10.1186/1741-7015-9-52.
Du K, Luan Z, Qu SQ: Clinical outcome of bone marrow mesenchymal stem cells transplantation in children with severe cerebral palsy. Clin Pediatr. 2011, 29: 55-58.
Wang XD, Yang J, Li M: Effects of bone marrow mesenchymal stem cell graft on gross motor function in children with cerebral. Journal of China-Japan Friendship Hospital. 2010, 24: 337-342.
Bartley J, Carroll JE: Stem cell therapy for cerebral palsy. Expert Opin Biol Ther. 2003, 3: 541-549.
Long X, Olszewski M, Huang W, Kletzel M: Neural cell differentiation in vitro from adult human bone marrow mesenchymal stem cells. Stem Cells Dev. 2005, 14: 65-69. 10.1089/scd.2005.14.65.
Hermann A, Gastl R, Liebau S, Popa MO, Fiedler J, Boehm BO, Maisel M, Lerche H, Schwarz J, Brenner R, Storch A: Efficient generation of neural stem cell-like cells from adult human bone marrow stromal cells. J Cell Sci. 2004, 117: 4411-4422. 10.1242/jcs.01307.
Deng J, Petersen BE, Steindler DA, Jorgensen ML, Laywell ED: Mesenchymal stem cells spontaneously express neural proteins in culture and are neurogenic after transplantation. Stem Cells. 2006, 24: 1054-1064. 10.1634/stemcells.2005-0370.
Zhao ZM, Li HJ, Liu HY, Lu SH, Yang RC, Zhang QJ, Han ZC: Intraspinal transplantation of CD34+ human umbilical cord blood cells after spinal cord hemisection injury improves functional recovery in adult rats. Cell Transplant. 2004, 13: 113-122.
Enzmann GU, Benton RL, Talbott JF, Cao Q, Whittemore SR: Functional considerations of stem cell transplantation therapy for spinal cord repair. J Neurotrauma. 2006, 23: 479-495. 10.1089/neu.2006.23.479.
Mazzini L, Mareschi K, Ferrero I, Vassallo E, Oliveri G, Nasuelli N, Oggioni GD, Testa L, Fagioli F: Stem cell treatment in Amyotrophic Lateral Sclerosis. J Neurol Sci. 2008, 265: 78-83. 10.1016/j.jns.2007.05.016.
Mazzini L, Ferrero I, Luparello V, Rustichelli D, Gunetti M, Mareschi K, Testa L, Stecco A, Tarletti R, Miglioretti M: Mesenchymal stem cell transplantation in amyotrophic lateral sclerosis: A Phase I clinical trial. Exp Neurol. 2010, 223: 229-237. 10.1016/j.expneurol.2009.08.007.
Dominici M, Le Blanc K, Mueller I, Slaper-Cortenbach I, Marini F, Krause D, Deans R, Keating A, Prockop D, Horwitz E: Minimal criteria for defining multipotent mesenchymal stromal cells. The International Society for Cellular Therapy position statement. Cytotherapy. 2006, 8: 315-317. 10.1080/14653240600855905.
Lundkvist Josenby A, Jarnlo GB, Gummesson C, Nordmark E: Longitudinal construct validity of the GMFM-88 total score and goal total score and the GMFM-66 score in a 5-year follow-up study. Phys Ther. 2009, 89: 342-350. 10.2522/ptj.20080037.
Back SA, Craig A, Luo NL, Ren J, Akundi RS, Ribeiro I, Rivkees SA: Protective effects of caffeine on chronic hypoxia-induced perinatal white matter injury. Ann Neurol. 2006, 60: 696-705. 10.1002/ana.21008.
Back SA, Craig A, Kayton RJ, Luo NL, Meshul CK, Allcock N, Fern R: Hypoxia-ischemia preferentially triggers glutamate depletion from oligodendroglia and axons in perinatal cerebral white matter. J Cereb Blood Flow Metab. 2007, 27: 334-347. 10.1038/sj.jcbfm.9600344.
Prasad R, Verma N, Srivastava A, Das BK, Mishra OP: Magnetic resonance imaging, risk factors and co-morbidities in children with cerebral palsy. J Neurol. 2011, 258: 471-478. 10.1007/s00415-010-5782-2.
Park KI, Himes BT, Stieg PE, Tessler A, Fischer I, Snyder EY: Neural stem cells may be uniquely suited for combined gene therapy and cell replacement: Evidence from engraftment of Neurotrophin-3-expressing stem cells in hypoxic-ischemic brain injury. Exp Neurol. 2006, 199: 179-190. 10.1016/j.expneurol.2006.03.016.
Chamberlain G, Fox J, Ashton B, Middleton J: Concise review: mesenchymal stem cells: their phenotype, differentiation capacity, immunological features, and potential for homing. Stem Cells. 2007, 25: 2739-2749. 10.1634/stemcells.2007-0197.
Iwanami A, Kaneko S, Nakamura M, Kanemura Y, Mori H, Kobayashi S, Yamasaki M, Momoshima S, Ishii H, Ando K: Transplantation of human neural stem cells for spinal cord injury in primates. J Neurosci Res. 2005, 80: 182-190. 10.1002/jnr.20436.
Ma H, Yu B, Kong L, Zhang Y, Shi Y: Neural stem cells over-expressing brain-derived neurotrophic factor (BDNF) stimulate synaptic protein expression and promote functional recovery following transplantation in rat model of traumatic brain injury. Neurochem Res. 2012, 37: 69-83. 10.1007/s11064-011-0584-1.
Hofstetter CP, Holmstrom NA, Lilja JA, Schweinhardt P, Hao J, Spenger C, Wiesenfeld-Hallin Z, Kurpad SN, Frisen J, Olson L: Allodynia limits the usefulness of intraspinal neural stem cell grafts; directed differentiation improves outcome. Nat Neurosci. 2005, 8: 346-353. 10.1038/nn1405.
Lim JY, Park SI, Kim SM, Jun JA, Oh JH, Ryu CH, Jeong CH, Park SH, Park SA, Oh W: Neural Differentiation of Brain-derived Neurotrophic Factor-expressing Human Umbilical Cord Blood-derived Mesenchymal Stem Cells in Culture via TrkB-mediated ERK and beta-catenin Phosphorylation and following Transplantation into the Developing Brain. Cell Transplant. 2011, 20: 1855-1866. 10.3727/096368910X557236.
Chekhonin VP, Lebedev SV, Volkov AI, Pavlov KA, Ter-Arutyunyants AA, Volgina NE, Savchenko EA, Grinenko NF, Lazarenko IP: Activation of expression of brain-derived neurotrophic factor at the site of implantation of allogenic and xenogenic neural stem (progenitor) cells in rats with ischemic cortical stroke. Bull Exp Biol Med. 2011, 150: 515-518. 10.1007/s10517-011-1180-8.
Momin EN, Mohyeldin A, Zaidi HA, Vela G, Quinones-Hinojosa A: Mesenchymal stem cells: new approaches for the treatment of neurological diseases. Curr Stem Cell Res Ther. 2010, 5: 326-344. 10.2174/157488810793351631.
Centeno CJ, Schultz JR, Cheever M, Freeman M, Faulkner S, Robinson B, Hanson R: Safety and complications reporting update on the re-implantation of culture-expanded mesenchymal stem cells using autologous platelet lysate technique. Curr Stem Cell Res Ther. 2011, 6: 368-378. 10.2174/157488811797904371.
Tan J, Wu W, Xu X, Liao L, Zheng F, Messinger S, Sun X, Chen J, Yang S, Cai J: Induction therapy with autologous mesenchymal stem cells in living-related kidney transplants: a randomized controlled trial. JAMA. 2012, 307: 1169-1177. 10.1001/jama.2012.316.
Parkes J, Hill N, Platt MJ, Donnelly C: Oromotor dysfunction and communication impairments in children with cerebral palsy: a register study. Dev Med Child Neurol. 2010, 52: 1113-1119. 10.1111/j.1469-8749.2010.03765.x.
Pennington L, Miller N, Robson S, Steen N: Intensive speech and language therapy for older children with cerebral palsy: a systems approach. Dev Med Child Neurol. 2010, 52: 337-344. 10.1111/j.1469-8749.2009.03366.x.
Acknowledgement
This study was supported by the National Key Basic Research and Development Project (Beijing, China) (No. 2011CB965101). We would also like to thank all of the patients whose participation made this study possible.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
HQL conceived of the study, participated in its design, and drafted and revised the manuscript. GJC and YLW participated in the design of the study, collected and analysed the data, and drafted the manuscript. ZYX participated in the design of the study, analysed the data, drafted and revised the manuscript and performed the immunoassays. FF and RMX collected and analysed the data. YW drafted and revised the manuscript and performed the statistical analysis. XLH and LXF participated in the coordination of the study and helped draft the manuscript. All of the authors read and approved the final manuscript.
Guojun Chen, Yali Wang, Zhenyu Xu contributed equally to this work.
Electronic supplementary material
12967_2012_1407_MOESM2_ESM.wmv
Additional file 2: The motor ability of patient No. 4 in the transplantation group before and after treatment. (WMV 4 MB)
12967_2012_1407_MOESM3_ESM.wmv
Additional file 3: The motor ability of patient No. 5 in the transplantation group before and after treatment. (WMV 3 MB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Chen, G., Wang, Y., Xu, Z. et al. Neural stem cell-like cells derived from autologous bone mesenchymal stem cells for the treatment of patients with cerebral palsy. J Transl Med 11, 21 (2013). https://doi.org/10.1186/1479-5876-11-21
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1479-5876-11-21