
Abstract
Background
Apolipoprotein D (ApoD) is a lipocalin involved in several processes including lipid transport, but its modulation during human pregnancy was never examined.
Methods
We investigated the changes in the levels of ApoD in the plasma of pregnant women at the two first trimesters of gestation and at delivery as well as in the placenta and in venous cord blood. These changes were studied in 151 women classified into 9 groups in relation to their prepregnancy body mass index (BMI) and gestational weight gain (GWG).
Results
Plasma ApoD levels decrease significantly during normal uncomplicated pregnancy. ApoD is further decreased in women with excessive GWG and their newborns. In these women, the ApoD concentration was tightly associated with the lipid parameters. However, the similar ApoD levels in low cholesterol (LC) and high cholesterol (HC) women suggest that the plasma ApoD variation is not cholesterol dependant. A tight regulation of both placental ApoD transcription and protein content is most probably at the basis of the low circulating ApoD concentrations in women with excessive GWG. After delivery, the plasma ApoD concentrations depended on whether the mother was breast-feeding or not, lactation favoring a faster return to baseline values.
Conclusion
It is speculated that the decrease in plasma ApoD concentration during pregnancy is an adaptive response aimed at maintaining fetal lipid homeostasis. The exact mechanism of this adaptation is not known.
Similar content being viewed by others

Background
Human pregnancy is associated with profound changes in the maternal lipid, carbohydrate and protein metabolisms. These changes are aimed at favoring the maintenance of pregnancy, sustaining fetal growth and brain development, and facilitating parturition [1]. Maternal metabolism is intimately linked with prepregnancy body mass index (BMI) and gestational weight gain (GWG), which greatly influence the outcome of pregnancy [2]. In association with an unhealthy lifestyle, suboptimal prepregnancy BMI and GWG also increase the risk of birth defects and chronic health problems in the children [3].
The maternal lipid metabolism during pregnancy is characterized by progressive increases in plasma cholesterol and triglyceride levels accompanied by increases in low density lipoprotein (LDL) and very low density lipoprotein (VLDL), leading to maternal hyperlipidemia during late pregnancy [4]. Cholesterol is essential for optimal embryonic and fetal development. It is an important component of plasma membranes, required for cell proliferation, differentiation and morphogenesis modulation [5]. It is also used by the placenta for the synthesis of steroid hormones [6]. Triglycerides are also crucial as they are used as a source of essential fatty acids for the fetus, although they do not directly cross the placental barrier [7].
Plasma lipid metabolism is regulated in part by the specific apolipoprotein constituents of the various lipoprotein classes. The pregnancy induced hyperlipidemia is accompanied by a rise in the plasma levels of some apolipoproteins, namely ApoA-1, ApoB, ApoC-II and ApoC-III. Apolipoprotein D (ApoD) is a secreted lipocalin assigned with many putative functions including lipid transport. Its macromolecular distribution extends from VLDL to very high density lipoproteins (VHDL) with a maximum concentration in high density lipoproteins 3 (HDL3) [8]. It is considered an atypical apolipoprotein as both its structure and major sites of synthesis differ from the other apolipoproteins. Indeed, in human, ApoD is poorly expressed in the liver and intestine while it is highly expressed in adrenal glands, spleen, kidneys, pancreas, placenta, nervous system, lungs, ovaries and testes [[9], Rassart et al., unpublished results]. Several hydrophobic molecules were identified as its potential ligands including cholesterol [9], bilirubin [10], pregnenolone, progesterone, estrogens [11, 12] and arachidonic acid [13].
ApoD expression is modulated in many situations (for review see [14, 15]), namely cellular growth and differentiation [16–19], cancer [19, 20], nervous system pathologies [21–24] inflammation [25, 26] and oxidative stress [27–29]. ApoD is also involved in gestation and fetus development. In human, it is up-regulated in the endometrium during the window of uterine receptivity for embryonic implantation [30], is highly expressed in placenta [9] and is found in colustrum and milk [31]. Its levels are also increased in fallopian tubes and ovaries of gestating compared to non-gestating guinea pigs [32] but are decreased in lactating compared to virgin mouse mammary gland [33]. During mouse development, ApoD expression is selectively modulated from embryonic day 8.5 (E8.5) to birth [34] and in brain, its expression coincides with the period of active myelination and synaptogenesis [35]. The role of ApoD in embryogenesis is not limited to mammals as it is found in the yolk of the rapidly growing chicken oocyte, where it might transport lipids or regulatory molecules such as vitamin A and thyroid hormones [36, 37], and expressed during late chicken embryogenesis [38].
In spite of the important role of ApoD in lipid transport, its expression in gestation-related tissues and during fetus development, and also despite numerous studies on other apolipoproteins, there is no available information concerning ApoD modulation throughout human pregnancy.
To address this question, we measured ApoD levels in plasma at each trimester of pregnancy, in cord blood, two months after delivery and in placenta. We also examined how ApoD levels are modified by factors affecting lipid metabolism such as maternal prepregnancy BMI, gestational weight gain and hypercholesterolemia.
Methods
Population
The women participating in the study were recruited at their first prenatal visit, before their tenth week of pregnancy, at the Clinique Fidès of Montréal (Montréal, QC, Canada) and at the Saint-Luc Hospital's Perinatology Service of the Centre Hospitalier de l'Université de Montréal (CHUM, Montréal, QC, Canada), from 2002-2006. This study included 151 pregnant women of similar socio-economic situation. The study was approved by the ethical committee of CHUM and Université du Québec à Montréal (Montréal, QC, Canada). All subjects provided written informed consent. The exclusion criteria were gestational or type 2 diabetes, preeclampsia, hypertension, consumption of drugs interfering with lipid metabolism and complications during pregnancy or at delivery. A group of 5 non-pregnant women of similar age than the pregnant subjects examined, having a BMI of 20-26 kg/m2 and with plasma biochemistry within the expected normal ranges was also included.
Population classification
The study population was classified into 9 groups according to their prepregnancy BMI, confirmed at their first prenatal visit, and GWG. In accordance with Health Canada recommendations (2002), the normal values for BMI were established at 20-26 kg/m2. In order to facilitate the analysis, the normal values for GWG were established at 11-18 kg independently of the BMI [39–41]. The normal control group was defined as: BMI 20-26 kg/m2, GWG 11-18 kg. Women with a BMI under 20 or above 26 kg/m2 were designated as low and high BMI, respectively, while women with a GWG under 11 or above 18 kg were designated as low and high GWG, respectively. A classification based on the median plasmatic total cholesterol level at delivery (6,85 mM) was also established. Women with a cholesterol concentration inferior to 7 mM (n = 38) were referred to as the low cholesterol group (LC) while women with a cholesterol concentration superior to 8 mM (n = 29) were considered as the non-pathologic high cholesterol group (HC) [42–44].
Blood and tissue samples
Blood samples were collected at first (10-17 weeks) and second (22-28 weeks) trimesters of gestation and at delivery (36-40 weeks). Newborn blood samples were retrieved from the umbilical cord (venous cord blood). Blood samples were also collected two months after parturition (postpartum) from lactating and non-lactating women. The blood samples were centrifuged 15 min at 3,500 × g and plasma samples were kept at -20°C until analysis. The placentas, from vaginal delivery, were obtained from the Saint-Luc Hospital of CHUM (Montréal, QC, Canada) and were immediately immersed in Dulbecco's Modified Eagle Medium (DMEM) (Sigma, Oakville, ON, Canada) supplemented with antibiotics (penicillin, streptomycin and neomycin, Invitrogen, Burlington, ON, Canada) and NaHCO3. After the removal of the amnion, the chorion and the decidual layer, the placental tissue was randomly cut in 5 cm2 sections, immediately frozen in liquid nitrogen and kept at -80°C until analysis.
Plasma biochemistry
The plasma levels of total cholesterol, LDL-cholesterol, HDL-cholesterol and triglycerides were individually measured using the UniCel 36 DX600 Synchron Clinical System (Beckman-Coulter, Mississauga, ON, Canada) at the Clinical Biochemistry Service of Saint-François d'Assise Hospital (Québec, QC, Canada). Total plasma fatty acids were measured by gas phase chromatography. ApoA-1 and ApoB-100 levels were measured by RIA or ELISA methods at the Centre Hospitalier Universitaire de Québec (Québec, QC, Canada). ApoD levels were measured by competitive ELISA using the human ApoD monoclonal antibody 2B9 as previously described [22]. Briefly, microtiter plates were coated with antigen (1 μg ApoD/ml) overnight at 4°C in 5 mM glycin buffer (pH 9.2). Unreacted sites were blocked with PBS-BSA 1% for 1 h. A mixture containing diluted plasma and 2B9 antibody in PBS-BSA 1% then replaced the saturation solution. Bound 2B9 antibody was detected by peroxidase labeled anti-mouse IgG (KPL, Gaithersburg, MD) and revealed with ABTS substrate (2,2'-azino-bis(3-ethylbenzthiazoline-6-sulphonic acid; KPL). Optical density was measured at 410 nm. All quantifications were performed in triplicate.
RNA isolation and quantitative Real-Time PCR (qRT-PCR)
Total RNA was prepared from 25 mg of placental tissue using the High Pure RNA Tissue Kit (Roche Diagnostics, Laval, QC, Canada) according to the manufacturer's instructions. Subsequently, cDNA was obtained by reverse transcription of total RNA using the Omniscript RT kit (Qiagen, Mississauga, ON, Canada). The quantification of ApoD and 18S transcripts were assessed by qRT-PCR using the LightCycler 480 SYBR Green I Master and the LightCycler 480 instrument and software (Roche Diagnostics). For each gene, diluted amounts of known templates provided quantitative standard curves from which cDNA copy number in clinical samples could be determined. ApoD transcript expression was then normalized versus the housekeeping gene 18S. The following primers were used in qRT-PCR: ApoD forward, 5'-CAT CTT GGG AAG TGC CCC AA-3'; ApoD reverse, 5'-CCA TCA GCT CTC AAC TCC TGG TTT-3'; 18S forward, 5'-CGC CGC TAG AGG TGA AAT TC-3'; 18S reverse, 5'-TTG GCA AAT GCT TTC GCT C-3'.
Placental ApoD quantification
Placental tissues were rinsed 3-4 times in cold 0,9% NaCl solution containing a mixture of anti-proteases (Complete protease inhibitors-EDTA free, Roche Diagnostics) to remove blood from tissue. Placental tissues (1 g) were then homogenized in 1 ml cold lysis buffer (125 mM Tris-HCl, pH 8,0, 2 mM CaCl2, 1,4% (v/v) Triton X-100, 2% Complete protease inhibitors-EDTA free, 1 mM phenylmethylsulphonylfluoride) using a Polytron tissue homogenizer 3000 (Brinkman, Westbury, NY, USA). The homogenates were centrifuged at 10,000 × g for 25 min at 4°C. The protein concentration of the supernatant was determined using the BCA (bicinchoninic acid) assay (Pierce, Brockville, ON, Canada). Supernatants were kept at -80°C until analysis. The ApoD levels were measured by competitive ELISA as described above.
Statistical analyses
Data were expressed as means ± SEM and analyzed with unpaired Student's t-test or Mann-Whitney U test. Results were considered significant at p < 0.05. The association between two variables of the same population was assessed using Pearson's correlation coefficient. All statistical analyses were performed using Prism 4.0 (GraphPad Software, San Diego, CA, USA).
Results
Population characteristics
As shown in Additional file 1, the 151 pregnant women participating to this study were classified into 9 groups according to their prepregnancy BMI and GWG. It was first observed that GWG had a greater influence on group characteristics at delivery than BMI. For example, in the high BMI group, suboptimal GWG, i.e. inferior or superior to the normal range of 11-18 kg, significantly reduced the pregnancy duration (Additional file 1). Nevertheless, only the normal BMI, low GWG group had smaller newborns (Additional file 2). Suboptimal GWG had an even larger impact on lipid parameters, mainly in the high BMI but also in the normal BMI group. Unexpectedly, however, both low and high GWG resulted in decreased lipid levels (Additional file 1). These changes however had a low incidence on the newborn lipid parameters (Additional file 2).
Plasma ApoD levels decrease during pregnancy
Plasma ApoD levels were measured in women at each trimester of pregnancy. In the control group (BMI 20-26 kg/m2, GWG 11-18 kg), plasma ApoD concentration declined early in pregnancy as its levels were already reduced by 40% at the first trimester of pregnancy compared to non-pregnant women (Figure 1). ApoD levels continued to progressively decrease at the second trimester and until delivery where they reached 30% of the levels in non-pregnant women (Figure 1). A similar significant decrease of ApoD during gestation was also observed in our 8 other groups (data not shown). Interestingly, ApoD levels in the venous cord blood were similar to the levels in the mother plasma at delivery in all groups, except for the normal BMI (20-26 kg/m2), low GWG (< 11 kg) group where cord blood had inferior ApoD levels than the mother's blood (Figure 1 and Table 1). In spite of this, by using the Pearson's correlation coefficient, no correlation was found between ApoD plasma levels in the mother and the venous cord blood (Table 2 and Additional file 3).

Plasma ApoD levels during pregnancy. ApoD levels were measured in women with a BMI of 20-26 kg/m2 and a GWG of 11-18 kg at the two first trimesters of pregnancy (1st and 2nd) and at delivery. ApoD levels in the venous cord blood were also measured. Data are expressed as means ± SEM. * indicates significant differences compared to the first trimester (p < 0.001). # indicates significant differences compared to the second trimester (p < 0.001). & indicates significant differences compared to the pregnant groups and to cord blood (p < 0.001).
Influence of prepregnancy BMI and GWG on plasma ApoD levels
Maternal prepregnancy BMI did not present an impact on plasma ApoD levels at delivery (Table 1). However, a GWG superior to 18 kg caused a decrease in maternal ApoD levels in the normal and low BMI groups but not in the high BMI group (Table 1). Similarly, GWG but not BMI also affected venous cord blood ApoD concentration. Newborns from mothers having a GWG superior to 18 kg had lower cord blood ApoD levels than newborns from the other groups (Table 1).
Association between plasma ApoD levels and pregnancy parameters
The correlation between ApoD concentration at delivery and the other pregnancy-related parameters was explored using Pearson's correlation coefficient. In the control group, ApoD levels correlated only with total-cholesterol, in a positive manner (Additional file 3). In the other groups, ApoD correlations were different and specific to each group (Additional file 3). Then, since only GWG had an impact on ApoD values (Table 1), we created 3 new groups containing all women with similar GWG, regardless of their BMI (Table 2). In women with low GWG, ApoD values were directly correlated with GWG and inversely correlated with the newborn weight. Moreover, in women with normal GWG, ApoD was inversely correlated with ApoA-I. In contrast, in women with high GWG, which present lower ApoD levels, ApoD was correlated with most of the parameters. ApoD was strongly negatively correlated with most of the lipid parameters except triglycerides with which ApoD was directly correlated. ApoD was also negatively correlated with gestational age, GWG and newborn height and directly correlated with mother's age and BMI (Table 2). However, although many of the lipid parameters in women with high GWG are significantly different from the normal GWG group, all newborns displayed similar lipid parameters independently of maternal GWG (data not shown).
ApoD and cholesterol
To verify if the low ApoD level in women with excessive GWG was attributable to their lower cholesterol levels (Additional file 1), and because of the correlation between plasma ApoD and cholesterol levels in the control group (Additional file 3), we compared the ApoD levels between low cholesterol (LC) and high cholesterol (HC) women (Table 3). The HC group had higher total and LDL-cholesterol, triglycerides, ApoA-I and ApoB-100 levels but lower GWG (Table 3). However, both groups displayed similar ApoD levels. The 2 groups were also different from the control group described in Additional file 1. As expected, the LC group had lower while the HC group had higher levels of total cholesterol, LDL-cholesterol and ApoB-100. In this aspect, the LC group was similar to the high GWG groups (Additional files 1 and 3). The HC group also showed lower GWG and higher triglycerides levels than the control group (Additional files 1 and 3). In spite of this, all newborns displayed similar lipid parameters independently of maternal cholesterol levels (data not shown).
The cholesterol level greatly affected the association of ApoD with maternal and newborn characteristics, ApoD being more associated with pregnancy-related characteristics in LC than in HC women (Table 3). These associations differed from the ones described for the control group (Additional file 3) but showed similarities to those in high GWG groups (Table 2).
ApoD in placenta
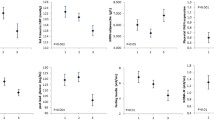
Because of the high levels of ApoD mRNA in human placenta and the importance of this tissue in fetal development, we examined placental ApoD transcript and protein content in relation to maternal BMI and GWG. Besides its influence on plasma ApoD levels (Table 1), maternal GWG also affected placental ApoD transcription (Figure 2A). However, in contrast to plasma, ApoD transcript levels were decreased in both low and high GWG compared with normal GWG groups. This pattern was mostly noticed in women with normal or low BMI but, although not significant, this tendency was also observed in women with high BMI (Figure 2A). Interestingly, the placental ApoD protein content diverged from the mRNA levels and was affected both by GWG and by BMI (Figure 2B). High BMI with suboptimal GWG groups contained the lower levels of ApoD whereas the higher levels of ApoD were observed in low BMI groups having suboptimal GWG. Low levels of ApoD were also detected in the normal BMI, low GWG group. Nevertheless, ApoD levels were similar in normal GWG groups, independently of BMI.

ApoD levels in placenta according to pre-pregnancy BMI and GWG. (A) The level of apoD mRNA expression was measured by qRT-PCR using specific primers for apoD. Data are expressed as the normalized ratio of apoD mRNA to 18S RNA (means ± SEM). (B) The placental ApoD protein content was measured by ELISA. The values (means ± SEM) were normalized by the total protein content. * indicates significant differences (p < 0.01) from the normal control group (BMI 20-26 kg/m2, GWG 11-18 kg). # indicates significant differences (p < 0.01) from the group of similar GWG and normal BMI (20-26 kg/m2).
Postpartum plasma ApoD levels
Given that plasma ApoD levels were decreased by 70% at the end of pregnancy, we examined if, in control women, ApoD levels returned to baseline values two months after delivery and whether these levels were affected by lactation (Figure 3). Breast-feeding (lactating) women had plasma ApoD levels similar to non-pregnant women. However, in bottle-feeding (non-lactating) women, ApoD concentration remained comparable to the levels at delivery.

The effect of breast- and bottle-feeding on plasma ApoD levels. ApoD concentration was measured in mothers two months after delivery (women with a BMI of 20-26 kg/m2 and a GWG of 11-18 kg) and compared with levels at delivery and in non-pregnant women (BMI 20-26 kg/m2). Data are expressed as means ± SEM. * indicates significant differences compared to non-pregnant women (p < 0.001). # indicates significant differences compared to breast-feeding women (p < 0.001).
Discussion
To our knowledge, this study is the first to demonstrate that plasma ApoD levels decrease during pregnancy. Plasma ApoD levels were already significantly lower during first trimester of pregnancy than values detected in non-pregnant women and continued to decrease until the end of pregnancy. The mechanisms governing this decrease are currently unknown, but many potential reasons could explain it.
As for albumin, which concentration is lowered by 30% during pregnancy [45], the decrease in plasma ApoD levels could be explained in part by hemodilution. Maternal blood volume increases until term and although dependant on many factors, the average increase in volume at term is 45-50% [46]. Still, although it could explain the decrease in plasma ApoD levels at the first and second trimesters of pregnancy, hemodilution alone cannot explain the observed 70% decrease of plasma ApoD at delivery.
Low levels of plasma ApoD could also result from decreased ApoD synthesis or secretion. Plasma ApoD can originate from many sources, one of which being the placenta. Since ApoD mRNA levels are almost as high in placenta as in adrenal glands and spleen, major sources of ApoD in non-pregnant humans [9], decreased ApoD transcription is unlikely the origin of low plasma ApoD concentration. Another argument against ApoD transcriptional downregulation is the presence of oxidative and inflammatory markers mostly in complicated but also in normal pregnancies [47]. Oxidative stress [26–29] and inflammation [25, 26] were both reported as intensifying ApoD mRNA production. ApoD decrease could also be caused by the inhibition of its translation or the increase of its degradation rate. More likely, the decline in ApoD levels could be imputable to its reduced secretion by placenta and other tissues during pregnancy. In addition, as prolonged exposure to physiological concentrations of 17 beta-estradiol inhibited markedly (70-90%) ApoD secretion in human breast cells [19], high estrogen concentrations, as seen during gestation [48, 49], could be the root of plasma ApoD decrease.
Assuming that ApoD synthesis and degradation rates remain unchanged, a reduced secretion will result in ApoD accumulation inside tissues. In the placenta, in collaboration with other molecules, ApoD could play a key role in the transport of essential nutrients, regulation factors and toxic metabolites between the mother and the fetus. Those could include cholesterol [9], arachidonic acid [13, 50], steroids [11, 12], vitamin A and thyroid hormones [37] as well as the removal of bilirubin [10].
It was already reported that ApoD levels in newborns represent about 37% of the levels found in adults [51, 52]. Accordingly, we observed that the concentration of circulating ApoD in the venous cord blood was very similar to that of the mother at delivery, which is about 30% of the levels in non-pregnant women, although the levels found in the cord blood and in the mother were not statistically correlated. This lack of correlation suggests that ApoD does not pass through the placental barrier. Since ApoD mRNA expression occurs as early as E8.5 during mouse embryogenesis [34], the fetus might not be dependent on a maternal ApoD supply. Furthermore, the similarity in mother and venous cord blood ApoD concentrations suggests that even if maternal plasma ApoD does not directly cross the placental barrier, both might be subjected to the same regulatory mechanisms.
We also observed that, while prepregnancy maternal BMI had no incidence on plasma ApoD concentrations on both mother and cord blood, high GWG (> 18 kg) significantly decreased ApoD values. This decrease is very likely multifactorial. In this particular case, it could, among others, be related to defects in lipid metabolism. Indeed, high GWG groups displayed lower levels of total cholesterol, LDL-cholesterol, and ApoB-100. This was present in normal and high BMI groups but the tendency, although not significant, was also observed in the low BMI group. This was also observed in the group composed of all women with high GWG regardless of their BMI. In addition, in this group, ApoD and lipid markers were strongly correlated. An involvement of ApoD in lipid metabolism was already suggested. Because of its capacity to bind cholesterol and its presence on lipoprotein fractions [8], ApoD, in collaboration with ApoA-I, lecithin-cholesterol acyltransferase (LCAT) and cholesteryl ester transfer protein (CETP) [53], may participate in the cholesterol transport pathway. Furthermore, genetic variation in ApoD affects the serum lipid levels [54].
Nevertheless, lipid levels are probably not the major factors responsible for low ApoD levels in these groups. Indeed, high GWG groups are not the only ones presenting levels of total cholesterol, LDL-cholesterol, and ApoB-100 different from the control group as well as correlations between ApoD and lipid levels. In addition, the low BMI group does not show a significant decrease of these lipid parameters. Finally, the ApoD concentration is similar in the control, HC and LC groups, the latter showing similarities with the high GWG groups.
Our results also suggest that a tight regulation of placental ApoD transcription and secretion is probably involved in the lower circulating ApoD concentrations in women with excessive GWG. In the view that ApoD may play a key role in the control of fetal homeostasis, the regulation of ApoD levels becomes vital for the pregnancy outcome and the health of the newborn. Thus, in women with high GWG, a decrease in circulating ApoD is desirable in order to reduce lipid transfer to fetus. This could be achieved both by reducing the ApoD transcription and by preventing ApoD from leaving the placenta. Consistently, high GWG have low ApoD mRNA levels and normal or high placental ApoD content. According to this hypothesis, the lower production of ApoD in low GWG women is disadvantageous. It would then be compensated by an increased secretion or lower degradation by the placenta and possibly other tissues resulting in adequate ApoD protein concentration in the circulation. In overweight women (high BMI), this control is probably altered, as evidenced by the high ApoD mRNA and low ApoD protein levels in the placenta independently of the GWG. This may explain why the plasma ApoD levels are similar in high GWG and in the control group. Still, plasma ApoD levels are not solely dependent on placental regulation as high BMI groups, in spite of high ApoD mRNA and low ApoD protein levels in the placenta, did not show higher plasma ApoD concentration than the control group. Similarly, despite low ApoD transcript levels and high protein content in the placenta, the low BMI, low GWG group had plasma ApoD levels similar to the control group. This suggests that other tissues have the ability to secrete or trap ApoD and that they may not be subjected to the same regulatory pathways than the placenta.
After delivery, the return to basal, non-pregnant, plasma ApoD levels, such as observed in breast-feeding women was expected. However, the fact that bottle-feeding women still have the same plasma ApoD levels than at delivery is intriguing and suggests again that the regulation of ApoD levels is complex. A possible explanation of this discrepancy is that breast-feeding mothers have high levels of prolactin. Prolactin was reported to exert an antagonistic action on estrogen production in order to maintain lactation [48, 55] and could thus favor ApoD production. In addition, breast-feeding induces the production of cytokines [56, 57], which may contribute to the higher levels of circulating ApoD.
Conclusion
Plasma ApoD levels decrease during normal uncomplicated human pregnancy. ApoD is further decreased in women with excessive GWG and their newborns. The cause of this decrease, controlled in part at the transcriptional level in the placenta, is probably multi-factorial and may be related to pregnancy-induced changes in lipids and hormone levels. Still, the connection between lipids, estrogen and apoD levels is speculative and requires further studies.
References
DeCherney A, Pernoll ML: Current Obstetric & Gynecologic Diagnosis & Treatment. 1994, East Norwalk: McGraw-Hill Companies, 8
Nohr EA, Vaeth M, Baker JL, Sørensen TIa, Olsen J, Rasmussen KM: Combined associations of prepregnancy body mass index and gestational weight gain with the outcome of pregnancy. Am J Clin Nutr. 2008, 87: 1750-1759.
Kaiser L, Allen LH: American Dietetic Association. Position of the American Dietetic Association: nutrition and lifestyle for a healthy pregnancy outcome. J Am Diet Assoc. 2008, 108: 553-561. 10.1016/j.jada.2008.01.030.
Potter JM, Nestel PJ: The hyperlipidemia of pregnancy in normal and complicated pregnancies. Am J Obstet Gynecol. 1979, 133: 165-170.
Porter JA, Young KE, Beachy PA: Cholesterol modification of hedgehog signaling proteins in animal development. Science. 1996, 274: 255-259. 10.1126/science.274.5285.255.
Kallen CB: Steroid hormone synthesis in pregnancy. Obstet Gynecol Clin North Am. 2004, 31: 795-816. 10.1016/j.ogc.2004.08.009.
Herrera E: Metabolic adaptations in pregnancy and their implications for the availability of substrates to the fetus. Eur J Clin Nutr. 2000, 54: S47-S51.
McConathy WJ, Alaupovic P: Studies on the isolation and partial characterization of apolipoprotein D and lipoprotein D of human plasma. Biochemistry. 1976, 15: 515-520. 10.1021/bi00648a010.
Drayna D, Fielding C, McLean J, Baer B, Castro G, Chen E, Comstock L, Henzel W, Kohr W, Rhee L, Wion K, Lawn R: Cloning and expression of human apolipoprotein D cDNA. J Biol Chem. 1986, 261: 16535-16539.
Peitsch MC, Boguski MS: Is apolipoprotein D a mammalian bilin-binding protein?. New Biol. 1990, 2: 197-206.
Dilley WG, Haagensen DE, Cox CE, Wells SA: Immunologic and steroid binding properties of the GCDFP-24 protein isolated from human breast gross cystic disease fluid. Breast Cancer Res Treat. 1990, 16: 253-260. 10.1007/BF01806333.
Simard J, Veilleux R, de Launoit Y, Haagensen DE, Labrie F: Stimulation of apolipoprotein D secretion by steroids coincides with inhibition of cell proliferation in human LNCaP prostate cancer cells. Cancer Res. 1991, 51: 4336-4341.
Morais Cabral JH, Atkins GL, Sánchez LM, López-Boado YS, López-Otin C, Sawyer L: Arachidonic acid binds to apolipoprotein D: implications for the protein's function. FEBS Lett. 1995, 366: 53-56. 10.1016/0014-5793(95)00484-Q.
Rassart E, Bedirian A, Do Carmo S, Guinard O, Sirois J, Terrisse L, Milne R: Apolipoprotein D. Biochim Biophys Acta. 2000, 1482: 185-198.
Van Dijk W, Do Carmo S, Rassart E, Dahlbäck B, Sodetz JM: The plasma lipocalins α1-acid glycoprotein, apolipoprotein D, apolipoprotein M and complement protein C8γ. Lipocalins. Edited by: Akerström B, Borregaard N, Flower DR, Salier J-P. 2006, Georgetown: Landes Bioscience, 140-166.
Do Carmo S, Séguin D, Milne R, Rassart E: Modulation of apolipoprotein D and apolipoprotein E mRNA expression by growth arrest and identification of key elements in the promoter. J Biol Chem. 2002, 277: 5514-5523. 10.1074/jbc.M105057200.
López-Boado YS, Tolivia J, López-Otín C: Apolipoprotein D gene induction by retinoic acid is concomitant with growth arrest and cell differentiation in human breast cancer cells. J Biol Chem. 1994, 269: 26871-26878.
Provost PR, Marcel YL, Milne RW, Weech PK, Rassart E: Apolipoprotein D transcription occurs specifically in nonproliferating quiescent and senescent fibroblast cultures. FEBS Lett. 1991, 290: 139-141. 10.1016/0014-5793(91)81244-3.
Simard J, Dauvois S, Haagensen DE, Lévesque C, Mérand Y, Labrie F: Regulation of progesterone-binding breast cyst protein GCDFP-24 secretion by estrogens and androgens in human breast cancer cells: a new marker of steroid action in breast cancer. Endocrinology. 1990, 126: 3223-3231. 10.1210/endo-126-6-3223.
Hunter S, Young A, Olson J, Brat DJ, Bowers G, Wilcox JN, Jaye D, Mendrinos S, Neish A: Differential expression between pilocytic and anaplastic astrocytomas: identification of apolipoprotein D as a marker for low-grade, non-infiltrating primary CNS neoplasms. J Neuropathol Exp Neurol. 2002, 61: 275-281.
Boyles JK, Notterpek LM, Anderson LJ: Accumulation of apolipoproteins in the regenerating and remyelinating mammalian peripheral nerve. Identification of apolipoprotein D, apolipoprotein A-IV, apolipoprotein E, and apolipoprotein A-I. J Biol Chem. 1990, 265: 17805-17815.
Terrisse L, Poirier J, Bertrand P, Merched A, Visvikis S, Siest G, Milne R, Rassart E: Increased levels of apolipoprotein D in cerebrospinal fluid and hippocampus of Alzheimer's patients. J Neurochem. 1998, 71: 1643-1650.
Terrisse L, Séguin D, Bertrand P, Poirier J, Milne R, Rassart E: Modulation of apolipoprotein D and apolipoprotein E expression in rat hippocampus after entorhinal cortex lesion. Brain Res Mol Brain Res. 1999, 70: 26-35. 10.1016/S0169-328X(99)00123-0.
Thomas EA, Dean B, Pavey G, Sutcliffe JG: Increased CNS levels of apolipoprotein D in schizophrenic and bipolar subjects: implications for the pathophysiology of psychiatric disorders. Proc Natl Acad Sci USA. 2001, 98: 4066-4071. 10.1073/pnas.071056198.
Maher JE, Goldenberg RL, Tamura T, Cliver SP, Hoffman HJ, Davis RO, Boots L: Albumin levels in pregnancy: a hypothesis-decreased levels of albumin are related to increased levels of alpha-fetoprotein. Early Hum Dev. 1993, 34: 209-215. 10.1523/JNEUROSCI.2644-08.2008.
Do Carmo S, Levros LC, Rassart E: Modulation of apolipoprotein D expression and translocation under specific stress conditions. Biochim Biophys Acta. 2007, 1773: 954-969. 10.1016/j.bbamcr.2007.03.007.
Charron JB, Ouellet F, Houde M, Sarhan F: The plant Apolipoprotein D ortholog protects Arabidopsis against oxidative stress. BMC Plant Biol. 2008, 8: 86-10.1186/1471-2229-8-86.
Ganfornina MD, Do Carmo S, Lora JM, Torres-Schumann S, Vogel M, Allhorn M, González C, Bastiani MJ, Rassart E, Sanchez D: Apolipoprotein D is involved in the mechanisms regulating protection from oxidative stress. Aging Cell. 2008, 7: 506-515. 10.1111/j.1474-9726.2008.00395.x.
Muffat J, Walker DW, Benzer S: Human ApoD, an apolipoprotein up-regulated in neurodegenerative diseases, extends lifespan and increases stress resistance in Drosophila. Proc Natl Acad Sci USA. 2008, 105: 7088-7093. 10.1073/pnas.0800896105.
Kao LC, Tulac S, Lobo S, Imani B, Yang JP, Germeyer A, Osteen K, Taylor RN, Lessey BA, Giudice LC: Global gene profiling in human endometrium during the window of implantation. Endocrinology. 2002, 143: 2119-2138. 10.1210/en.143.6.2119.
Palmer DJ, Kelly VC, Smit AM, Kuy S, Knight CG, Cooper GJ: Human colostrum: identification of minor proteins in the aqueous phase by proteomics. Proteomics. 2006, 6: 2208-2216. 10.1002/pmic.200500558.
Provost PR, Tremblay Y, el-Amine M, Bélanger A: Guinea pig apolipoprotein D RNA diversity, and developmental and gestational modulation of mRNA levels. Mol Cell Endocrinol. 1995, 109: 225-236. 10.1016/0303-7207(95)03506-3.
Cofer S, Ross SR: The murine gene encoding apolipoprotein D exhibits a unique expression pattern as compared to other species. Gene. 1996, 171: 261-263. 10.1016/0378-1119(96)00099-6.
Sánchez D, Ganfornina MD, Martínez S: Expression pattern of the lipocalin apolipoprotein D during mouse embryogenesis. Mech Dev. 2002, 110: 225-229. 10.1016/S0925-4773(01)00578-0.
Ong WY, Lau CP, Leong SK, Kumar U, Suresh S, Patel SC: Apolipoprotein D gene expression in the rat brain and light and electron microscopic immunocytochemistry of apolipoprotein D expression in the cerebellum of neonatal, immature and adult rats. Neuroscience. 1999, 90: 913-922. 10.1016/S0306-4522(98)00507-7.
Vieira AV, Lindstedt K, Schneider WJ, Vieira PM: Identification of a circulatory and oocytic avian apolipoprotein D. Mol Reprod Dev. 1995, 42: 443-446. 10.1002/mrd.1080420411.
Yao Y, Vieira A: Comparative 17beta-estradiol response and lipoprotein interactions of an avian apolipoprotein. Gen Comp Endocrinol. 2002, 127: 89-93. 10.1016/S0016-6480(02)00032-1.
Ganfornina MD, Sánchez D, Pagano A, Tonachini L, Descalzi-Cancedda F, Martínez S: Molecular characterization and developmental expression pattern of the chicken apolipoprotein D gene: implications for the evolution of vertebrate lipocalins. Dev Dyn. 2005, 232: 191-199. 10.1002/dvdy.20193.
Johnson JW, Longmate JA, Frentzen B: Excessive maternal weight and pregnancy outcome. Am J Obstet Gynecol. 1992, 167: 353-370.
Ogunyemi D, Hullett S, Leeper J, Risk A: Prepregnancy body mass index, weight gain during pregnancy, and perinatal outcome in a rural black population. J Matern Fetal Med. 1998, 7: 190-193. 10.1002/(SICI)1520-6661(199807/08)7:4<190::AID-MFM5>3.0.CO;2-D.
Zhou W, Olsen J: Gestational weight gain as a predictor of birth and placenta weight according to pre-pregnancy body mass index. Acta Obstet Gynecol Scand. 1997, 76: 300-307.
Ethier-Chiasson M, Duchesne A, Forest JC, Giguère Y, Masse A, Mounier C, Lafond J: Influence of maternal lipid profile on placental protein expression of LDLr and SR-BI. Biochem Biophys Res Commun. 2007, 359: 8-14. 10.1016/j.bbrc.2007.05.002.
Ethier-Chiasson M, Forest JC, Giguère Y, Masse A, Marseille-Tremblay C, Lévy E, Lafond J: Modulation of placental protein expression of OLR1: implication in pregnancy-related disorders or pathologies. Reproduction. 2008, 136: 491-502. 10.1530/REP-08-0082.
Marseille-Tremblay C, Ethier-Chiasson M, Forest JC, Giguère Y, Masse A, Mounier C, Lafond J: Impact of maternal circulating cholesterol and gestational diabetes mellitus on lipid metabolism in human term placenta. Mol Reprod Dev. 2008, 75: 1054-1062. 10.1002/mrd.20842.
Maher JE, Goldenberg RL, Tamura T, Cliver SP, Hoffman HJ, Davis RO, Boots L: Albumin levels in pregnancy: a hypothesis-decreased levels of albumin are related to increased levels of alpha-fetoprotein. Early Hum Dev. 1993, 34: 209-215. 10.1016/0378-3782(93)90178-W.
Hytten F: Blood volume changes in normal pregnancy. Clin Haematol. 1985, 14: 601-612.
Fialová L, Malbohan I, Kalousová M, Soukupová J, Krofta L, Stípek S, Zima T: Oxidative stress and inflammation in pregnancy. Scand J Clin Lab Invest. 2006, 66: 121-127. 10.1080/00365510500375230.
Alvarez JJ, Montelongo A, Iglesias A, Lasunción MA, Herrera E: Longitudinal study on lipoprotein profile, high density lipoprotein subclass, and postheparin lipases during gestation in women. J Lipid Res. 1996, 37: 299-308.
Soldin OP, Guo T, Weiderpass E, Tractenberg RE, Hilakivi-Clarke L, Soldin SJ: Steroid hormone levels in pregnancy and 1 year postpartum using isotope dilution tandem mass spectrometry. Fertil Steril. 2005, 84: 701-710. 10.1016/j.fertnstert.2005.02.045.
Lafond J, Moukdar F, Rioux A, Ech-Chadli H, Brissette L, Robidoux J, Masse A, Simoneau L: Implication of ATP and sodium in arachidonic acid incorporation by placental syncytiotrophoblast brush border and basal plasma membranes in the human. Placenta. 2000, 21: 661-669. 10.1053/plac.2000.0561.
Lane DM, McConathy WJ: Factors affecting the lipid and apolipoprotein levels of cord sera. Pediatr Res. 1983, 17: 83-91. 10.1203/00006450-198302000-00001.
McConathy WJ, Lane DM: Studies on the apolipoproteins and lipoproteins of cord serum. Pediatr Res. 1980, 14: 757-761. 10.1203/00006450-198005000-00009.
Francone OL, Gurakar A, Fielding C: Distribution and functions of lecithin:cholesterol acyltransferase and cholesteryl ester transfer protein in plasma lipoproteins. Evidence for a functional unit containing these activities together with apolipoproteins A-I and D that catalyzes the esterification and transfer of cell-derived cholesterol. J Biol Chem. 1989, 264: 7066-7072.
Desai PP, Bunker CH, Ukoli FA, Kamboh MI: Genetic variation in the apolipoprotein D gene among African blacks and its significance in lipid metabolism. Atherosclerosis. 2002, 163: 329-338. 10.1016/S0021-9150(02)00012-6.
Wang C, Hsueh AJ, Erickson GF: Prolactin inhibition of estrogen production by cultured rat granulosa cells. Mol Cell Endocrinol. 1980, 20: 135-144. 10.1016/0303-7207(80)90077-5.
Shimaoka Y, Hidaka Y, Tada H, Nakamura T, Mitsuda N, Morimoto Y, Murata Y, Amino N: Changes in cytokine production during and after normal pregnancy. Am J Reprod Immunol. 2000, 44: 143-147. 10.1111/j.8755-8920.2000.440303.x.
Shimaoka Y, Hidaka Y, Tada H, Takeoka K, Morimoto Y, Amino N: Influence of breast-feeding on the production of cytokines. Am J Reprod Immunol. 2001, 45: 100-102. 10.1111/j.8755-8920.2001.450206.x.
Acknowledgements
We are thankful to Dr. Catherine Mounier for helpful discussions and to Maude Éthier-Chiasson and Fée-Ann McNabb for technical assistance. This work was supported by Canadian Institutes for Health Research grants (MOP-15677 and NET-54002). SDC was supported by FRSQ, NSERC and UQAM studentships.
Author information
Authors and Affiliations
Corresponding authors
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
SDC carried out the laboratory work, participated in conceiving and designing of the study, performed the statistical analysis and drafted the manuscript. J-CF, YG and AM were involved in data acquisition and analysis. ER and JL conceived and design the study, analyzed the results and edited the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
12958_2009_564_MOESM1_ESM.doc
Additional file 1: Table 4: Population characteristics at delivery. Plasma biochemistry of the mother at delivery organized according to maternal body mass index and gestational weight gain. (DOC 79 KB)
12958_2009_564_MOESM2_ESM.doc
Additional file 2: Table 5: Newborn characteristics at birth. Plasma biochemistry of the newborn at birth organized according to maternal body mass index and gestational weight gain. (DOC 69 KB)
12958_2009_564_MOESM3_ESM.doc
Additional file 3: Table 6: Association of plasma ApoD levels with clinical and biochemical characteristics in women at delivery. The data provided represent the Pearson correlations coefficients (r) between plasma ApoD levels and maternal characteristics at delivery. (DOC 81 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Do Carmo, S., Forest, JC., Giguère, Y. et al. Modulation of Apolipoprotein D levels in human pregnancy and association with gestational weight gain. Reprod Biol Endocrinol 7, 92 (2009). https://doi.org/10.1186/1477-7827-7-92
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7827-7-92