
Abstract
Background
Metastases to the breast from extramammary tumours are uncommon, and metastatic renal cell carcinoma to the breast is extremely rare. We report a metastasis to the breast from a renal primary with the radiological and histopathological features.
Case presentation
An 81-year-old lady was seen in the breast clinic for a right breast mass after sustaining a fall. Clinical examination and investigations revealed a metastatic cancer from a renal primary. She received surgical treatment only and is under regular follow-up in the oncology clinic.
Conclusion
The treatment strategy for metastatic breast diseases is based on a proper assessment of such cases by surgeons, radiologists and histopathologists.
Similar content being viewed by others


Background
Metastases to the breast from extramammary tumours are uncommon, and metastatic renal cell carcinoma to the breast is extremely rare [1]. We report a metastasis to the breast from a renal primary with the radiological and histopathological features.
Case presentation
An 81 years old lady had a right radical nephrectomy in 1999 for conventional renal cell cancer (RCC). She was discharged from the urology and oncology clinics in 2004 after 5 1/2 years follow-up with no signs of local or regional recurrence.
In December 2004, she noticed a lump in the right breast after sustaining a fall. She was referred to the breast clinic in July 2005 for further assessment.
Clinically, she had a mass in the upper outer quadrant of the right breast. The left breast was normal and there was no axillary lymphadenopathy. Abdominal examination was normal.
Radiology confirmed a 17 × 13 × 9 mm well circumscribed hypoechoic mass in the right upper quadrant of the right breast (Figure 1). The mass was core biopsied.

Ultrasonography showing hypoechoic mass in the right breast.
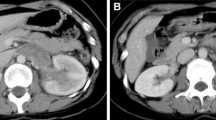
The histopathological examination revealed tumour growth consistent with conventional renal cell carcinoma. Tumour cells strongly expressed vimentin. CT scan of the chest and abdomen showed a 12 mm mass in the right breast and a 2.7 cm metastatic deposit at the right renal bed (Figures 2 and 3). The lungs and the liver were normal. The lump was excised in October 2005.

Computed tomography showing well-defined, round mass in the right breast (arrow).

Computed tomography showing tumour mass in the renal bed (arrow points to surgical clips).
The gross examination of the specimen confirmed metastasis from a renal primary (Figure 4). There was no evidence of in situ ductal or lobular disease.

Photomicrograph showing islands of tumour cells with clear cytoplasm, lying in fibrovascular stroma (Hematoxylin & Eosin, 10×).
The patient was offered Interferon treatment, but she preferred to hold on therapy as an alternative. She is under regular follow-up in the oncology clinic.
Discussion
Metastases to the breast from extramammary primary malignancies are rare. The incidence of metastasis to the breast in various clinical autopsy studies ranges from 5%–6.6% [3]. Both breasts are equally affected and bilateral involvement is not uncommon. Solitary discrete lesions occur in 85% [4].
The primitive neoplasms that most frequently metastasise to the breast are malignant melanoma, lymphoma, lung cancer and in men, prostatic cancer [1–3]. Breast metastasis from a renal tumour is extremely rare, accounting for 3% of the cases.
Clinically, metastatic lesions in the breast present as painless swellings with rapid growth [1, 4]. Unlike primary tumours, the skin is not involved and the axillary node involvement is variable [1, 4].
Mammogram shows well-circumscribed lesions, which lack microcalcifications [1, 4]. The course of renal cell carcinoma is extremely variable and unpredictable both in its clinical development and metastasis [1]. Most patients with renal cell carcinoma following nephrectomy develop multiple metastases and die within 10 years [2].
A preceding history of extramammary carcinoma can be helpful in suspecting a mass as a possible metastasis, as radical surgery can be avoided and appropriate chemotherapy or radiation therapy can be ensured [3, 4].
Conclusion
A treatment strategy for metastatic breast diseases is based on a proper assessment of such cases by surgeons, radiologists and histopathologists.
References
Forte A, Peronace MI, Gallinaro LS, Bertagni A, Prece V, Montesano G, Palumbo P, Nasti AG: Metastasis to the breast of a renal carcinoma: a clinical case. Eur Rev Medical Pharmacological Sci. 1999, 3: 115-118.
Hardy SC, Benson EA: Solitary breast metastasis from a hypernephroma. Eur J Surg Oncol. 1987, 4: 365-366.
Kannan V: Fine-needle aspiration of metastatic renal-cell carcinoma masquerading as primary breast carcinoma. Diag Cytopath. 1998, 5: 343-345. 10.1002/(SICI)1097-0339(199805)18:5<343::AID-DC7>3.0.CO;2-B.
Chieng DC, Cohen JM, Waisman J, Fernandez G: Fine-needle aspiration cytology of renal cell carcinoma metastatic to the breast: A report of three cases. Diag Cytopath. 1999, 5: 324-327. 10.1002/(SICI)1097-0339(199911)21:5<324::AID-DC5>3.0.CO;2-Q.
Acknowledgements
Written consent of the patient was obtained for publication of this case report.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
AA performed literature review, drafted and revised manuscript
AV evaluated histopathological features, edited and revised the manuscript
HM evaluated radiological images
MS contributed to the conception of the report
NS contributed to collection of the clinical data
All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Alzaraa, A., Vodovnik, A., Montgomery, H. et al. Breast metastasis from a renal cell cancer. World J Surg Onc 5, 25 (2007). https://doi.org/10.1186/1477-7819-5-25
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7819-5-25