
Abstract
Background
Malignant gastrointestinal stromal tumors (GIST) are rare mesenchymal tumors originating in the wall of the gastrointestinal tract. Myogenic gastrointestinal stromal tumor, a distinctive morphologic variant is characterized by an unusually prominent myxoid stromal background.
Case presentation
We report a case of myxoid variant of GIST in a 42 years old woman presenting as an epigastric mass associated to an ovarian cyst and elevated CA-125. Histologically, the lesions was composed of a proliferation of spindle cells in an abundant myxoid stroma, without evidence of atypia or anaplasia. Immunohistochemical stains showed strong positive staining with muscle actin, positive staining with CD34 and weak positive staining with CD117, while showed negative for S-100.
Conclusion
At surgery every effort should be made to identify the origin of the tumor. A complete surgical removal of the tumor should be obtained, as this is the only established treatment that offers long term survival.
Similar content being viewed by others


Background
Gastrointestinal stromal tumors (GIST) are rare tumors that may arise anywhere in the tubular gastrointestinal tract, but stomach is the most common site of localization. Surgery is the main stay of treatment and complete resection is achieved in most of cases [1]. The 5 year overall survival ranges from 21% to 88% in different series, depending from risk grading and completeness of surgical resection [1–4]. In light of the tendency of these tumors to pursue an indolent clinical course with a significant risk of late relapse, a brisk follow-up is advocated for all patients [5]. Imatinib mesylate is proposed as therapy for high risk GISTs after surgery [6]. A distinctive morphologic variant of gastrointestinal stromal tumor has been described, characterized by a prominent myxoid stromal background reminiscent of a neural neoplasm but lacking the immunohistochemical or ultrastructural features of peripheral nerve sheath or ganglionic differentiation. This variant is more frequent in women and mostly occurs in the stomach. These lesions are described grossly as well circumscribed, unencapsulated, with a prominently myxoid and often cystic cut surface [7]. We report a case of myxoid variant GIST, occurring in a 42 year old woman.
Case presentation
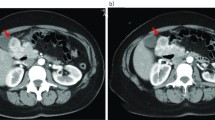
A 42-year-old woman presented with pelvic pain, palpable pelvic mass extended to the epigastric region, and elevated CA-125 (61.8 U/ml). Computed tomography (CT) imaging showed a left 6 × 5 cm cystic ovarian lesion and a 12 × 9.5 cm solid mass in the epigastric region (figure 1, 2). A preoperative diagnosis of metastatic ovarian malignancy or FIGO stage III ovarian malignancy was made. At laparotomy, a left ovarian cyst was seen along with a solid mass attached to the greater curvature of stomach which was easily dissected from it. Histologically, the lesions was composed of a proliferation of spindle cells embedded in an abundant myxoid stroma, without evidence of frank atypia or anaplasia. Histochemical stains showed strong positive staining with muscle actin, positive staining with CD34 and weak positive staining with CD117, while it was negative for S-100. The histological work up was conclusive for a low malignancy GIST – myxoid variant, being the mass volume the only risk factor [3, 5], the ovarian mass on the other hand was a follicular cyst. Due to the lack of clear risk factors for recurrence, and to complete surgical tumor resection, the patient was advised follow-up only.

Computed tomography imaging of upper abdomen showing solid mass lesion in epigastric area.

Computed tomography imaging of the pelvis showing cystic ovarian lesion
Discussion
Fletcher et al., [5] classified these tumors in to very low, low, intermediate and high risk, categories according to tumor size and mitotic count. Tumors <2 cm and mitotic count <5/50 high power field (HPF) were categorized as very low risk; tumor size 2–5 cm and mitotic count <5/50 HPF as low risk; tumor size <5 cm and mitotic count 6–10/50 HPF or tumor size 5–10 cm and mitotic count <5/50 HPF as intermediate risk; tumor size >5 cm and mitotic count >5/50 HPF or tumor size >10 cm and any mitotic rate or tumor any size and mitotic rate >10/50 HPF as high risk. As reported by others [8–10], GIST may mimic a pelvic masses. In such circumstances they are first noticed by gynecologists and are often diagnosed, prior to surgery, as ovarian tumors, either as metastatic from, or metastatizing to gastrointestinal tract. Only at surgery their nature is fully understood. The same was true in our case as a solid epigastric mass was associated to an ovarian cystic lesion similar to that in Krukenberg tumor. Therefore, in presence of a pelvic mass, especially if other unusual signs are present, the possibility of other than a gynecologic tumor has to be considered. At surgery, every effort should be made to identify the origin of the tumor and related anatomic structures. In the case of GIST, a complete surgical removal of the tumor should be obtained, as despite significant advances in new chemotherapic regimens have been radical surgical removal only offers chance of long term survival.
References
Besana-Ciani I, Boni L, Dionigi G, Benevento A, Dionigi R: Outcome and long-term results of surgical resection for gastrointestinal stromal tumors (GIST). Scand J Surg. 2003, 92: 195-199.
Liberati G, Lucchetta MC, Petraccia L, Nocchi S, Rosentzwig R, De Matteis A, Grassi M: Meta-analytical study of gastrointestinal stromal tumors (GIST). Clin Ter. 2003, 154: 85-91.
Singer S, Rubin BP, Lux ML, Chen CJ, Demetri GD, Fletcher CD, Fletcher JA: Prognostic value of KIT mutation type, mitotic activity, and histologic subtype in gastrointestinal stromal tumors. J Clin Oncol. 2002, 20: 3898-3905. 10.1200/JCO.2002.03.095.
Crosby JA, Catton CN, Davis A, Couture J, O'Sullivan B, Kandel R, Swallow CJ: Malignant gastrointestinal stromal tumors of the small intestine: a review of 50 cases from a prospective database. Ann Surg Oncol. 2001, 8: 50-59. 10.1245/aso.2001.8.1.50.
Fletcher CD, Berman JJ, Corless C, Gorstein F, Lasota J, Longley BJ, Miettinen M, O'Leary TJ, Remottí H, Rubin BP, Shmookler B, Sobin LH, Weiss SW: Diagnosis of gastrointestinal stromal tumors: a consensus approach. Int J Surg Pathol. 2002, 10: 81-89.
DeMatteo RP: The GIST of targeted cancer therapy: a tumor (gastrointestinal stromal tumor), a mutated gene (c-kit), and a molecular inhibitor (ST1571). Ann Surg Oncol. 2002, 9: 831-839.
Suster 9, Sorace D, Moran CA: Gastrointestinal stromal tumors with prominent myxoid matrix. Clinicopathologic, immunohistochemical, and ultrastructural study of nine cases of a distinctive morphologic variant of myogenic stromal tumor. Am J Surg Pathol. 1995, 19: 59-70.
Zighelboim I, Henao G, Kunda A, Gutierrez C, Edwards C: Gastrointestinal stromal tumor presenting as a pelvic mass. Gynecol Oncol. 2003, 91: 630-635. 10.1016/j.ygyno.2003.08.025.
Belics Z, Csapo Z, Szabo I, Papay J, Szabo J, Papp Z: Large gastrointestinal stromal tumor presenting as an ovarian tumor. A case report. J Reprod Med. 2003, 48: 655-658.
Foti MA, Currao AA, Palano AD, Nuciforo G: GIST in ginecologia: aspetti clinici. In Atti della Società Italiana di Ginecologia e Ostetricia, Congresso di Catania Ottobre 2003 v. 2, CIC Edizioni Internazionali, Roma. 2003, 496-499.
Acknowledgements
Written consent was obtained from the patient or their relative for publication of study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contributions
All authors conceived of the study, and participated in its design and coordination. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Carlomagno, G., Beneduce, P. A gastrointestinal stromal tumor (GIST) masquerading as an ovarian mass. World J Surg Onc 2, 15 (2004). https://doi.org/10.1186/1477-7819-2-15
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7819-2-15