
Abstract
Background
Although malignancy has been reported in thyroglossal cysts, synchronous occurrence of two malignancies is extremely rare.
Case Report
A case of concurrent papillary and squamous carcinoma arising in the thyroglossal cyst is presented here.
Conclusions
Papillary and squamous carcinoma simultaneously occurring in a thyroglossal cyst is rarely diagnosed prior to surgery and pose a therapeutic dilemma. In view of the extreme rarity of the condition, controversies do exist regarding the optimal strategy to be adopted. The ideal procedure needs to be individually tailored and involve a combination of surgery, radio ablation, thyroid suppression and external radiotherapy.
Similar content being viewed by others


Introduction
Malignant neoplasms rarely arise in thyroglossal cysts [1, 2]. Papillary carcinoma predominates among them. Squamous carcinoma accounts for only 5 % of the cases [3]. Only two cases of concurrent papillary and squamous carcinoma have been reported so far [4, 5]. Lack of an accurate preoperative diagnosis, rarity of the condition, and the possibility of an associated thyroid malignancy duly contribute to the confusion regarding the optimal management of this condition. We present one such case and discuss the various therapeutic options.
Case Report
A 48-year-old man presented with a swelling in the front of neck for past one year associated with a recent increase in size and hoarseness of voice. On examination, he was found to have a 5 × 6 cm cystic, non-transilluminant swelling below the hyoid, which moved with deglutition and protrusion of tongue but had restricted intrinsic mobility. Indirect laryngoscopic examination was unremarkable. Fine needle aspiration cytology was carried out which revealed thyroglossal cyst. Routine hematological and biochemical investigations and chest X roentgenogram were normal.
With a preoperative diagnosis of thyroglossal cyst, Sistrunk's procedure was planned. On exploration of the neck at surgery he was found to have two cystic swellings intimately related to each other, one was in the midline and the other was laterally placed. The latter was intimately related to the thyroid gland and adherent to the carotid sheath, strap muscles and the laryngeal apparatus. There was no regional lymphadenopathy. The swelling was meticulously dissected free from the carotid sheath and the laryngeal apparatus and was excised along with a portion of the strap muscles. A near total thyroidectomy was also performed. The right recurrent laryngeal nerve could not be identified at surgery and was presumed sacrificed during the procedure. The patient developed stridor in the immediate postoperative period, which necessitated endotracheal re-intubation but resolved later with conservative measures.
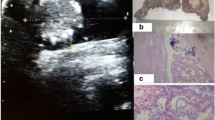
Histopathology of the resected specimen showed distinct foci of papillary carcinoma ([Figure 1) and squamous carcinoma (Figure 2) in the lateral cystic swelling and a normal thyroid gland. The midline swelling was found to have inflammatory tissue only. The patient was put on suppressive dose of thyroxin. Thyroid scintigraphy, radioiodine ablation of remnant thyroid and external beam radiotherapy to the tumor bed was planned however; the patient was lost to follow-up.

photomicrograph showing tumor cells with uniform opened out nucleus arranged in a papillary pattern. Psammoma bodies are seen. [Hematoxylin and Eosin ×200]

photomicrograph showing sheets of tumor cells with eosinophilic cytoplasm and hyperchromatic nucleus. Keratin pearl formation is seen. [Hematoxylin and Eosin ×200]
Discussion
Thyroglossal cysts are the most common non-odontogenic cyst in the neck and are presents in approximately 7% of the general population [1, 6]. Primary carcinoma, on the other hand, is rare and is seen in less than 1% of cases [1, 2]. Although rapid increase in size, dysphagia, hoarseness of voice and pain may be harbingers of malignancy, the diagnosis is usually based on pathological examination of the cyst [1, 7–12]. Preoperative evaluation of thyroglossal duct cyst includes a thorough head and neck examination, palpation of thyroid gland, thyroid function tests and a thyroid scan if there is a suspicion of an ectopic thyroid gland or a mass is palpable within the cyst, thyroid gland or in the neck [9]. An ultrasound examination may aid in the diagnosis of malignancy by demonstrating a mural nodule, calcification or lymph node metastases [13]. Computerized tomography has also been used for the same purpose but a previously infected cyst with thickened walls, presence of ectopic thyroid tissue within the cyst as well as a congenital dermoid cyst with debris may mimic malignancy [14]. Papillary carcinoma accounts for more than 90% of all cases and squamous carcinoma is seen in only 5% of cases [3]. Concurrent papillary and squamous carcinoma arising in thyroglossal cyst is extremely rare and only two cases have been reported so far [4, 5]. In the case described, as the foci of papillary and squamous carcinoma are separate and distinct, it is unlikely that the latter arose from squamous metaplasia of the papillary carcinomatous component.
The prognosis of papillary carcinoma arising in a thyroglossal cyst is good and is similar to that of papillary carcinoma of thyroid gland having cure rates in excess of 95 % [9, 15]. Sistrunk's procedure is preferred to simple excision and would suffice if the thyroid gland was found to be normal and negative margins can be achieved [16]. If the thyroid and lymph nodes are grossly normal during the procedure, a postoperative thyroid scan is recommended. However, if thyroid nodules are palpable peroperatively, or the pre or postoperative thyroid scan is abnormal, thyroidectomy is warranted [17, 18]. In the present case, as the lesion was intimately related to the thyroid gland and given the 10 – 14 % risk of another focus of carcinoma in the thyroid gland, we decided to carry out a near total thyroidectomy. Lymphadenopathy on the other hand is found only in 8% of the cases, hence only the significant involvement of regional lymph nodes necessitates a modified radical neck dissection [3, 10]. Central compartment dissection should also be considered in view of the fact that these lymph nodes may be involved in the absence of concomitant foci of malignancy in the thyroid gland [13]. Recurrence rates are lowest when total ablation of thyroid tissue is achieved and therefore thyroidectomy followed by radioiodine ablation should be considered especially if tumor recurrence or metastasis occurs [9]. Ultrasound examination of the neck as well as plasma thyroglobulin estimation may be helpful in detecting recurrence. Thyroid suppression is recommended for all patients with papillary carcinoma of thyroglossal cyst regardless of the presence of a normal thyroid scan or whether the patient had a thyroidectomy or not [9, 11, 19, 20].
Patients with squamous carcinoma arising in a thyroglossal cyst have a poorer prognosis and therefore should be treated with Sistrunk's procedure and postoperative external beam radiotherapy to both sides of the neck even in the absence of regional lymphadenopathy [9, 21].
This case is reported in view of the extreme rarity and to highlight the therapeutic options in the management of malignancies arising in thyroglossal cysts.
References
Allard RHB: The thyroglossal cyst. Head Neck Surg. 1982, 5: 134-146.
Nussbaum M, Buchwald RP, Ribner A, Mori K, Litwins J: Anaplastic carcinoma arising from median ectopic thyroid (thyroglossal duct remnant). Cancer. 1981, 48: 2724-2728.
Renard TH, Choucair RJ, Stevenson WD, Brooks WC, Poulos E: Carcinoma of the thyroglossal duct. Surg Gynecol Obstet. 1990, 171: 305-308.
Ronan SG, Deutsch E, Ghosh L: Thyroglossal duct carcinoma: light and electron microscopic studies. Head Neck Surg. 1986, 8: 222-225.
Kwan WB, Liu FF, Banerjee D, Rotstein LE, Tsang RW: Concurrent papillary and squamous carcinoma in a thyroglossal duct cyst: A case report. Can J Surg. 1996, 39: 328-332.
Ellis P, van Nostrand AW: The applied anatomy of thyroglossal tract remnants. Laryngoscope. 1977, 87: 765-770.
Bhagavan VS, Rao DR, Weinberg T: Carcinoma of thyroglossal duct cyst: Case report and review of the literature. Surgery. 1970, 67: 281-292.
Yildiz K, Koksal H, Ozpran Y, Muhtar H, Telatar M: Papillary carcinoma in a thyroglossal duct remnant with normal thyroid gland. J Laryngol Otol. 1993, 107: 1174-1176.
LaRouere MJ, Drake AF, Baker SR, Richter HJ, Magielski JE: Evaluation and management of a carcinoma arising in a thyroglossal duct cyst. Am J Otolaryngol. 1987, 8: 351-355.
Martin Perez M, Burguno Garcia M, Echevarria Iturbe C, Martinez Perez D: Papillary carcinoma arising in a thyroglossal duct cyst: Report of two cases. J Oral Maxillofac Surg. 1993, 51: 89-93.
Hilger AW, Thompson SD, Smallman LA, Watkinson JC: Papillary carcinoma arising in a thyroglossal duct cyst: A case report and literature review. J laryngol Otol. 1995, 109: 1124-1127.
Jacques DA, Chambers RG, Oertel JE: Thyroglossal tract carcinoma: A review of the literature and addition of eighteen cases. Am J Surg. 1970, 120: 439-446.
Cignarelli M, Ambrosi A, Marino A, Lamacchia O, Cincione R, Neri V: Three cases of papillary carcinoma and three of adenoma in thyroglossal duct cysts: clinical – diagnostic comparison with benign thyroglossal duct cysts. J Endocrinol Invest. 2002, 25: 947-954.
Branstetter BF, Weismann JL, Kennedy TL, Whitaker M: The CT appearance of thyroglossal duct carcinoma. Am J Neuroradiol. 2000, 21: 1547-1550.
Schlumberger MJ: Papillary and follicular thyroid carcinoma. N Engl J Med. 1998, 338: 297-306. 10.1056/NEJM199801293380506.
McNicoll MP, Hawkins DB, England K, Penny R, Maceri DR: Papillary carcinoma arising in a thyroglossal duct cyst. Otolaryngol Head Neck Surg. 1989, 99: 50-54.
Chen F, Sheridan B, Nankervis J: Carcinoma of the thyroglossal duct: Case reports and a literature review. Aust NZ J Surg. 1993, 63: 614-616.
Weiss SD, Orlich CC: Primary papillary carcinoma of a thyroglossal duct cyst: Report of a case and a literature review. Br J Surg. 1991, 78: 87-89.
Kum CK, Goh P, Teh M: Papillary carcinoma arising in a thyroglossal cyst. Aust NZ J Surg. 1993, 63: 738-740.
Maziak D, Borowy ZJ, Deitel M, Jaksic T, Ralph-Edwards A: Management of papillary carcinoma arising in thyroglossal duct anlage. Can J Surg. 1992, 35: 522-525.
Bosch K, Kummer E, Hohmann F: Carcinoma of the thyroglossal duct. Neth J Surg. 1986, 38: 36-40.
Author information
Authors and Affiliations
Corresponding author
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Vijay, R., Rajan, K.K. & Feroze, M. Inapparent twin malignancy in thyroglossal cyst: Case Report. World J Surg Onc 1, 15 (2003). https://doi.org/10.1186/1477-7819-1-15
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7819-1-15