
Abstract
Background
The objective of this study was to determine the concordance rate between core needle biopsy (CNB) and surgical excision of invasive breast cancer regarding the oestrogen receptor (ER) and Progesterone receptor (PgR) status as determined by Immunohistochemistry (IHC).
Methods
Hormone receptor status was established using IHC (using quickscore system 0–8) on preoperative CNB and subsequent surgical excision in 93 patients with invasive breast cancer. Results were compared taking into account tumour's size, grade, and patient's age.
Results
The ER concordance rate between CNB and surgical excisions was 95%. The PgR concordance rate was 89%. This shows that CNB has a sensitivity of 97% for ER and 95% for PgR.
There is a positive correlation of ER and PgR between CNB and surgical excision (p < 0.000001). There was no significant difference in the number of core biopsies between concordant and discordant cases.
Conclusion
Preoperative core biopsy is highly sensitive for the IHC detection of ER and PgR in invasive breast cancer. The concordance rate is higher for ER than PgR, which could be due to the fact that ER is more homogeneously distributed.
Similar content being viewed by others

Introduction
The core needle biopsy (CNB) is technique increasingly used for the preoperative assessment of breast lesions [1]. Image guidance increases accuracy and reduces the number of false negative cases [2]. The presence of malignancy and tumour's type and grade are routinely reported.
There is an increasing need to provide prognostic data on CNB in order to improve treatment outcome [3, 4].
Hormone receptor status, and especially ER, provides valuable prognostic information and predicts the response to adjuvant and neo-adjuvant systemic treatment [5].
Traditionally, the hormone receptor status was determined by enzyme immunoassay of ER and PgR proteins. However, this has been replaced gradually by immunohistochemistry (IHC), which has shown an equal reliability [6].
Previous studies that examined the reliability of preoperative CNB using enzyme immunoassay showed conflicting results [7–9].
This retrospective study examines the correlation between CNB and surgical excision in regards to the ER ad PgR status of invasive breast cancer using IHC.
Patients and Methods
In this retrospective study we looked at consecutive 95 cases of invasive breast carcinoma in 93 patients. All patients underwent CNB at their clinic appointment and proceeded for breast surgery subsequently 2–3 weeks later. Preoperative CNBs and surgical excision specimens were analysed for ER and PgR status using IHC (DAKO mab) after antigen retrieval at high temperature. All specimens were analysed using semi quantitative IHC "quick score" system (0 – 8) by the same breast pathologist. With this method, the intensity of the immunohistochemical reaction as viewed under the light microscope was recorded 0–4 (0 indicated no staining of any nuclei even at high magnification). The proportion of cells staining positively at any intensity was scored as 0 (no cell staining), 1 (1–25% cells stained), 2 (26–50% cells stained), 3 (51–75% cells stained) or 4 (when >75% cells stained). The proportion and intensity scores were added together to obtain a total score ranging from 0 to 8.
We also examined other parameters including: tumour size, grade, and patient's age.
ER/PgR status was considered positive if quick score was 2 – 8. Results were re-assessed when quick score was raised to 4 – 8 to label ER/PgR status as positive. The number of biopsies taken on each occasion was also recorded.
Results
The mean and median age of this study group was 59.2 and 59 respectively (range 32 – 92 years). The mean tumour size was 20 mm (3.2 – 110 mm), and the median grade was 2 (1 – 3). The median number of CNBs taken at preoperative assessment was 2.6 (1 – 9). The mean IHC score for ER was 6.7 (range 0 – 8).
All patients had either mastectomy or lumpectomy as their definitive surgical treatment.
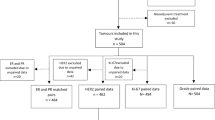
Firstly, ER/PgR status was considered positive if quick score was 2 – 8. The concordance for tumour grade was 65%. The concordance rate for ER was 95% between CNB and surgical excision. There were 2 false negative and 3 false positive cases. PgR concordance rate was 89% with 4 false negative and 6 false positive cases. According to the above results the sensitivity of CNB for ER and PgR was 97% and 95% respectively. Furthermore, to re-examine our findings, we analysed the results considering ER/PgR to be positive if quick score was 4 – 8. We found a concordance rate for ER to be 93% (3 false negative and 5 false positive cases). The concordance rate for PgR was 92% (3 false negative and 6 false positive cases) (figure 1). This gives CNB sensitivity of 98% for positive ER status and 96% for positive PgR status (table 1).

Graphic Results, 1: ER in CNB, 2: ER in surgical excision.
ER in CNB positively correlated with ER in surgical excision (r: 0.61, p < 0.000001). PgR in CNB also positively correlated with PgR in surgical excision (r: 0.66, p < 0.000001)
There was no significant difference in the number of CNBs between concordant and discordant cases.
Discussion
Core needle biopsies offer a reliable and accurate assessment of hormone receptor status.
Previous studies on a smaller case sample have suggested similar findings regarding ER [10–12]. However, results on PgR were less consistent.
The concordance rate in our study for ER was higher than for PgR. Homogenous distribution of ER through out the tumour is a possible explanation. Heterogeneity of the ER in tumour cell populations may have important implications for analytic cell selection and for prognosis in ER-positive carcinomas. Previous studies have shown homogenous geographic distribution of ER in the tumour cell population [13, 14].
These results indicate that the hormone receptor status as determined by CNB can be reliably used to guide neo-adjuvant and adjuvant systemic therapy in patients with invasive breast cancer.
In summary, preoperative CNB is highly sensitive for the IHC detection of ER and PgR in invasive breast cancer.
References
Sharifi S, Peterson MK, Baum JK, et al: Assessment of pathologic prognostic factors in breast core needle biopsies. Mod Pathol. 1999, 12 (10): 941-945.
Shah VI, Raju U, Chitale D, et al: False-negative core needle biopsies of the breast: an analysis of clinical, radiologic, and pathologic findings in 27 concecutive cases of missed breast cancer. Cancer. 2003, 97 (8): 1824-31. 10.1002/cncr.11278. 15
Harris GC, Denley HE, Pinder SE, et al: Correlation of histologic prognostic factors in core biopsies and therapeutic excisions of invasive breast carcinoma. Am J Surg Pathol. 2003, 27 (1): 11-5. 10.1097/00000478-200301000-00002.
King TA, Cederbom GJ, Champaign JL, et al: A core breast biopsy diagnosis of invasive carcinoma allows for definitive surgical treatment planning. Am J Surg. 1998, 176 (6): 497-501. 10.1016/S0002-9610(98)00250-5.
Colditz GA, Rosner BA, Chen WY, et al: Risk factors for breast cancer according to estrogen and progesterone receptor status. J Natl Cancer Inst. 2004, 96 (3): 218-28. 4
Ferrero-Pous M, Trassard M, Le Doussal V, et al: Comparison of enzyme immunoassay and immunohistochemical measurements of estrogen and progesterone receptors in breast cancer patients. Appl Immunohistochem Mol Morphol. 2001, 9 (3): 267-75. 10.1097/00022744-200109000-00012.
Bridges KG, Keshgegian AA, Kumar H, et al: Influence of surgical technique on estrogen and progesterone receptor determination in breast cancer. Cancer. 1983, 51: 2317-20.
Sharoni T, Feldman B, Inhar I, et al: Estrogen and progesterone receptor levels are lower in specimens taken from previously biopsied breast tumour tissue. J Surg Oncol. 35: 197-200.
Day T, Yeoman RR, Nelson G, et al: Influence of mastectomy technique on sex steroid receptor analysis. Am J Surg. 1988, 156: 446-9.
Connor CS, Tawfik OW, Joyce AJ, et al: comparison of prognostic tumor markers obtained on image-guided breast biopsies and final surgical specimens. Am J Surg. 2002, 184 (4): 322-4. 10.1016/S0002-9610(02)00953-4.
Jacobs TW, Siziopikou KP, Prioleau J, et al: Do prognostic marker studies on core needle biopsy specimens of breast carcinoma accurately reflect the marker status of the tumor?. Mod Pathol. 1998, 11 (3): 259-64.
Railo M, Nordling S, Krogerus L, et al: Preoperative assessment of proliferative activity and hormonal receptor status in carcinoma of the breast: a comparison of needle aspiration and needle-core biopsies to the surgical specimen. Diagn Cytopathol. 1996, 15 (3): 205-10. 10.1002/(SICI)1097-0339(199609)15:3<205::AID-DC6>3.0.CO;2-F.
Layfield LJ, Saria E, Mooney EE, et al: Tissue heterogeneity of immunohistochemically detected estrogen receptor. Implications for image analysis quantification. Am J Clin Pathol. 1998, 110 (6): 758-64.
Charpin C, Martin PM, De Victor B, et al: Multiparametric study (SAMBA 200) of estrogen receptor immunocytochemical assay in 400 human breast carcinomas: analysis of estrogen receptor distribution heterogeneity in tissues and correlations with dextran coated charcoal assays and morphological data. Cancer Res. 1988, 48 (6): 1578-86. 15
Author information
Authors and Affiliations
Corresponding author
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
Open Access This is an open access article distributed under the terms of the Creative Commons Attribution Noncommercial License ( https://creativecommons.org/licenses/by-nc/2.0 ), which permits any noncommercial use, distribution, and reproduction in any medium, provided the original author(s) and source are credited.
About this article
Cite this article
Al Sarakbi, W., Salhab, M., Thomas, V. et al. Is preoperative core biopsy accurate in determining the hormone receptor status in women with invasive breast cancer?. Int Semin Surg Oncol 2, 15 (2005). https://doi.org/10.1186/1477-7800-2-15
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7800-2-15