
Abstract
Background
Diabetes is a chronic medical condition accompanied by a considerable health-related quality of life (HRQL) burden. The purpose of this analysis was to use generic measures of HRQL to describe HRQL deficits associated with varying degrees of severity of type 2 diabetes.
Methods
The RAND-12 physical and mental health composites (PHC and MHC, respectively) and Health Utilities Index Mark 3 (HUI3) were self-completed by 372 subjects enrolled in a prospective, controlled study of an intervention to improve care for individuals with type 2 diabetes in rural communities. Analysis of covariance was used to assess differences in HRQL according to disease severity and control of blood glucose. Disease severity was defined in terms of treatment intensity, emergency room visits and absenteeism from work specifically attributable to diabetes. To control for potential confounding, the analysis was adjusted for important sociodemographic and clinical characteristics.
Results
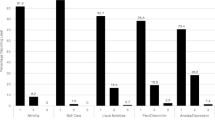
The PHC and MHC were significantly lower for individuals treated with insulin as compared to diet alone (PHC: 41.01 vs 45.11, MHC: 43.23 vs 47.00, p < 0.05). Individuals treated with insulin had lower scores on the vision, emotion and pain attributes of the HUI3 than individuals managed with oral medication or diet. The PHC, MHC, pain attribute and overall score on the HUI3 captured substantial decrements in HRQL associated with absenteeism from work due to diabetes, while the burden associated with emergency room utilization for diabetes was seen in the PHC and HUI3 pain attribute.
Conclusions
We concluded that generic measures of HRQL captured deficits associated with more severe disease in type 2 diabetes.
Similar content being viewed by others


Explore related subjects
Find the latest articles, discoveries, and news in related topics.Background
Severity of diabetes has been associated with increased burden and impairment on many dimensions of health-related quality of life (HRQL), including social functioning, cognition, role functioning, physical functioning, emotional well-being, general perceptions of health and pain [1–14]. Diabetic complications, such as retinopathy, nephropathy, neuropathy, cardiovascular disease, stroke and peripheral vascular disease, result in significant morbidity and mortality [1–9]. Self-reported HRQL is an important outcome to assess in diabetes because clinical parameters, such as glycated hemoglobin (HbA1c), a measure of average blood glucose control over the previous three months, often fail to capture the overall impact of the disease.
Commonly used indicators of disease advancement or severity have included treatment intensity of diabetes, duration of diabetes, number and severity of complications associated with diabetes. The presence and severity of complications relate to clinical depression, anxiety and impairment on both generic and disease-specific measures of health status and HRQL in individuals with type 1 or type 2 diabetes [2–5, 15]. There is evidence that longer duration of diabetes is associated with deficits in HRQL [2, 6, 16, 17], but some studies have failed to find this association [18, 19].
The purpose of this analysis was to describe HRQL deficits associated with varying degrees of disease severity and poor control of blood glucose in type 2 diabetes, using the RAND-12 and Health Utilities Index Mark 3 (HUI3), two generic measures of HRQL. The prevalence of comorbidities in type 2 diabetes is relatively high. Past research suggests disease-specific measures may better capture the dimensions of HRQL most affected by diabetes, but these measures are not designed to capture the deficits associated with comorbidities, i.e. they are specific to diabetes. Generic measures may be useful for capturing the additional HRQL deficits associated with comorbidities, such as cardiovascular disease and depression, as they encompass a broad range of dimensions or attributes of HRQL. Further, using generic measures often enables comparisons to be made between the study sample and available population norms. Finally, preference-based measures, such as the HUI3, can provide utility scores for varying degrees of disease severity, which may be incorporated into cost utility analyses. We hypothesized that generic measures would capture increasing HRQL deficits according to disease severity, and that the HUI3 may be more sensitive than the RAND-12, as the HUI3 has attributes that may be directly affected by diabetic complications.
Methods
Study Design
This analysis was conducted using baseline, cross-sectional data from a prospective, controlled study of an intervention to improve care for individuals with type 2 diabetes [20]. Two comparable and geographically adjacent rural health regions in Northern Alberta were included in the intervention study. The intervention region had a population of 20,000 residents, 17 physicians, and one full-time and two part-time diabetes educators, while the control region had a population of 25,000 residents, 22 physicians, and one part-time diabetes educator. Both regions were about a six hour drive from the nearest secondary or tertiary care referral centres. In both regions approximately 75% of the population was white and 25% was First Nations (aboriginal). Ethical approval for the study was obtained through the University of Alberta Health Research Ethics Board Panel A.
Sample
Three hundred and ninety-three individuals with type 2 diabetes were enrolled in the main study. In order to be included in the study, subjects had to have type 2 diabetes, live within the control or intervention region, consent to baseline measurements, be sufficiently literate in English to answer surveys and be willing to participate in follow-up visits. Subjects were excluded if they were discovered to not have type 2 diabetes, had a foreshortened life-expectancy, declined enrollment or were unable or unwilling to give informed consent. Subjects were recruited and enrolled by local diabetes health care professionals (registered dieticians, certified diabetes educators, registered diabetes nurses), diabetes education programs, community pharmacists or primary care physicians.
Measures
The RAND-12 and HUI3 were used to measure the HRQL deficits experienced by patients. Both HRQL measures were self-administered, self-completed at the time of the baseline visit or were submitted via mail. For both HRQL measures, we used the standard four week recall.
The HUI3 is a preference-based index measure of HRQL that uses a multi-attribute utility function to assign valuations to different health states [21]. Using the multi-attribute approach, health states are defined by a classification system that includes a set of dimensions or attributes of HRQL, with a number of different levels of functioning for each attribute. In the HUI3 system, eight attributes, including vision, hearing, speech, ambulation, dexterity, emotion, cognition and pain and discomfort, define health status. Each attribute has five or six levels, which creates 972,000 unique HUI3 health states. Within each attribute, levels range from highly impaired (e.g. blind for vision) to normal. Overall utility scores on the HUI3 range from -0.36 to 1.0, with -0.36 representing the utility of the worst possible HUI3 health state, 0.0 representing dead and 1.0 representing perfect health [21]. Differences of greater than 0.03 on the overall HUI3 score are considered clinically important [22, 23].
In addition to overall scores, single attribute utility scores (SAU) can be obtained for each attribute of the HUI3 [21]. For the single attribute utilities, scores range from 0.0 to 1.0, with a score of 0.0 representing the lowest level of functioning on an attribute and a score of 1.0 representing full functional capacity on an attribute. Differences in SAU scores of 0.05 may be considered clinically important [23]. The HUI3 may be particularly useful in studying HRQL in diabetes because several of the single attributes would likely be affected by severity of diabetes and diabetic complications. Thus, we focused on the vision, ambulation, dexterity, cognition and pain attributes in the analysis.
The RAND-12 contains 12 items taken from the eight scales of the RAND-36 Health Status Inventory (RAND-36) [24] and measures physical and mental dimensions of health status. Six of the 12 items create the Physical Health Composite (PHC) and the remaining six items create the Mental Health Composite (MHC). Scoring of each scale uses a one-parameter Rasch model, based on item response theory. The PHC and MHC are norm-based standardized scores, with a mean of 50 and standard deviation of 10 (i.e. T-scores) in the general United States population [24]. The RAND-12 uses the same 12 items of the commonly recognized SF-12 [25], but applies a different scoring algorithm. We found the RAND-12 scoring approach performed better than the SF-12 in discriminating known groups in this sample [26]. While a minimally clinically important difference on the RAND-12 has not been clearly defined, a difference between groups of 5.0 would represent a moderate effect size (0.50) (mean difference = 5.0 / S.D. = 10.0 = 0.50), which may be considered clinically important.
Severity at the time of the survey was defined in terms of treatment intensity of diabetes, self-reported emergency room utilization specifically related to diabetes in the previous six months, and self-reported absenteeism from work specifically related to diabetes in the previous six months. Management of diabetes with diet alone was defined as the least intense treatment, followed by oral medications, while the most intense treatment was with insulin alone or in combination with oral medications. Data on treatment intensity, duration of diabetes, emergency room visits and absenteeism from work were self-reported.
Control of blood glucose was assessed using glycated hemoglobin (HbA1c), a measure of average control of blood glucose over the previous three months. For HbA1c, we categorized individuals according to targets from the clinical practice guidelines for diabetes management in Canada that were current during the time of the study [8]. Glycated hemoglobin of less than 0.070 was the optimal target goal, 0.071 to 0.084 to indicative of less-than optimal control possibly warranting action, and greater than 0.084 was indicated inadequate control and that action should be taken [8]. Blood samples for glycated hemoglobin levels were all drawn in labs in Northern Alberta and the analysis of samples was carried out in a central lab, where the range of normal values for this measure was 0.043 to 0.061.
Statistical Significance Testing
Analysis of covariance (ANCOVA) was used to assess differences in HRQL associated with varying degrees of disease severity and control of blood glucose. For treatment intensity, individuals treated with insulin were presumed to have the most severe disease and largest disease burden, while individuals managed using diet alone were presumed to be the least burdened by diabetes. Among those subjects who indicated they were employed, individuals who attributed an absenteeism from work to diabetes were anticipated to have greater disease burden than individuals who did not. Similarly, individuals who visited an emergency room due to diabetes were expected to have a greater burden. It was anticipated that the relationship between control of blood glucose and HRQL, if present at all, would be weak.
In order to control for potential confounding, age, sex, level of education, annual household income, body mass index, and ethnicity (aboriginal or First Nations versus caucasian) were entered as covariates in all analyses. Duration of diabetes was controlled for in the analyses for emergency room visits, days off work, and control of blood glucose, but was not controlled for in the analysis for treatment intensity. A high correlation between treatment intensity and duration of diabetes suggested collinearity would be a problem in the analysis; therefore, duration of diabetes was excluded from this analysis. For all comparisons, a p-value of less than 0.05 (two-tailed) was considered to be statistically significant.
For interpreting clinically important differences on the PHC and MHC of the RAND-12, Cohen's guidelines for effect sizes were used as no established guidelines were available. Effect sizes of greater than 0.80 were considered large, while effect sizes between 0.50 and 0.79 were considered moderate and effect sizes between 0.20 and 0.49 were considered small [27].
Statistical analyses were performed using SPSS Version 11.5 with the available cases. No data was imputed for this cross-sectional analysis.
Results
Of the 393 subjects originally enrolled in the original study, 372 (94.7%) completed baseline HRQL questionnaires. No statistically significant differences in age, sex, level of education, income, BMI and duration of diabetes were noted between individuals who did (n = 372) and did not (n = 21) complete baseline HRQL data.
The percentage of the study sample with HRQL data missing ranged from a low of 1.9% (n = 7) for the emotion and dexterity attributes of the HUI3 to a high of 14.8% (n = 55) for the overall HUI3 score. If an individual's level was missing for any of the HUI attributes, the overall score would be missing. Of those who had completed the baseline surveys (N = 372), individuals missing the PHC, MHC and overall HUI3 scores were statistically significantly older and had lower incomes than individuals with complete data. In addition, individuals with missing HRQL data were more likely to be widowed. For the variables used to separate the sample into known groups, individuals with missing HUI3 scores tended to have more intensive treatment of their diabetes, i.e. they were more likely to use insulin and/or oral medications than to be managed on diet alone.
The majority of the sample was female (53.3%), currently married (68.3%), and had not completed high school (67.2%). A considerable proportion of the sample was retired (43.5%), which is not surprising as the average age of the sample was 62.3 ± 12.53 years. Approximately one-quarter (26.6%) of the study sample was First Nations (aboriginal). The average duration of diabetes was 8.0 ± 8.5 years, with the most common treatment for diabetes being oral medications, although a substantial proportion of the sample (27.2%) was treated with insulin. Overall, the unadjusted mean PHC (43.48 ± 10.81) was slightly lower than the MHC (44.84 ± 10.24) for the study sample, though both composites were approximately one-half of a standard deviation below the general United States population norm of 50. The average unadjusted overall HUI3 score was 0.64 ± 0.30.
When demographic and clinical variables were compared according to treatment intensity, the groups were similar for the most part. Differences were not statistically significant for most variables, with the exception of duration of diabetes, control of blood glucose, and main activity (Table 1). The average duration of diabetes of individuals whose diabetes was managed using insulin with or without oral medication was almost five times that of individuals whose diabetes was managed with diet alone (Table 1).
Burden Associated with Disease Severity
The burden associated with severity of type 2 diabetes was reflected in both physical and mental dimensions of HRQL (Table 2 and Table 3). In comparing those managed with diet alone to those using insulin, a statistically significant difference (p < 0.05) of 4.10 units (95% CI: 0.49–7.72) was observed in the PHC, representing a small to moderate effect size, after adjusting mean scores for the covariates. As well, the difference in overall HUI3 score between management with diet alone and insulin was clinically important and statistically significant (0.68 vs 0.61, p < 0.05, 95% CI for difference: -0.04 – 0.17). Statistically significant and clinically important differences were also observed for the vision and pain attributes of the HUI3, both of which reflect the physical dimension of HRQL. The difference in vision scores between individuals managed with diet alone compared to insulin was 0.07, while the difference in the pain attribute between individuals whose treatment regimen included insulin as compared to oral medication was 0.08.
Scores on the MHC of the RAND-12 and the HUI3 emotion attribute were both highest for subjects whose diabetes was managed with diet alone. The magnitude of the difference in MHC for individuals managed with diet alone compared to insulin was 3.77 units (effect size = 0.38, p < 0.05), which was slightly smaller than the difference in PHC between these groups. Also clinically important and statistically significant was the difference in scores on the HUI3 emotion attribute (0.07, p < 0.05) for individuals being managed with insulin compared to diet alone.
The HRQL burden of individuals who required an absenteeism from work due to diabetes was substantial (Table 3). Differences between individuals who were and were not absent from work for the PHC and MHC were 13.07 (p < 0.001, effect size = 1.3) and 6.29 (p = 0.084, effect size = 0.63), respectively, representing moderate to large effect sizes. Clinically important and statistically significant differences in overall HUI3 scores were also observed between individuals who were and were not absent from work due to diabetes (0.23, p < 0.001). The difference in the pain attribute of the HUI3 was considerable (0.28, p < 0.001), further demonstrating the physical health burden associated with greater disease severity.
The PHC was significantly lower for individuals who reported one or more emergency room visits for diabetes (37.68) compared to individuals who reported no emergency room visits (44.28, p < 0.05) (Table 3). The effect size for this difference was moderate to large (0.66). The HUI3 pain attribute was also affected; the difference between groups was 0.16 (p < 0.05), three times the threshold of what would be considered clinically important. In contrast to missing work due to diabetes, the need to visit an emergency room for diabetes was not associated with a significant mental health burden on the HUI3, which assesses happiness or depression. While the difference in scores on the MHC of the RAND-12 between subjects who did and did not have an emergency room visit for diabetes did not reach statistical significance, the effect size was moderate (0.53) (Table 3).
Burden Associated with Poor Control of Blood Glucose
As hypothesized, differences in HRQL between individuals in the three categories of control of blood glucose (optimal target goal, less-than optimal control possibly warranting action, and inadequate control that requires action) were negligible for the most part, after adjusting for the covariates in the model. A clinically important difference on the pain attribute, however, was observed between individuals who had acceptable control (adjusted mean = 0.83, 95% CI: 0.78–0.87) or whose control of blood glucose suggested that action may be required (adjusted mean = 0.83, 95% CI: 0.77–0.88) and those whose control of blood glucose suggested action was required (adjusted mean = 0.77, 95% CI: 0.69–0.83). These differences failed to reach statistical significance.
Discussion
Type 2 diabetes is a progressive disease in which advancing condition or severity is generally presumed to have an increasing burden on overall health. In this study, we found the burden associated with severity of type 2 diabetes generally affected physical and mental dimensions of health status and HRQL, as measured by the RAND-12 and HUI3. As anticipated, control of blood glucose, measured using HbA1c, was not a significant indicator of the self-reported HRQL burden of type 2 diabetes, regardless of its association with the development of long-term microvascular complications.
We were confident that treatment intensity of diabetes could be used as a marker of disease severity in type 2 diabetes as the Canadian Diabetes Association, until its December 2003 Guidelines, had recommended a step-wise approach to the management of type 2 diabetes starting with diet alone, then progressing to oral medications and, finally, to insulin with or without oral medications [8]. Further supporting the use of treatment intensity as a marker of disease severity in our data was the observation that individuals who were treated with insulin were also treated, on average, with a larger number of antihypertensive medications (p = 0.008) and were more difficult to control adequately (i.e. higher HbA1c) (p < 0.001). As well, a larger proportion of individuals taking oral medications for diabetes (23.8%) or insulin alone or in combination with oral medication (29.9%) received a lipid lowering medication (specifically HMG-CoA Reductase Inhibitors), compared to individuals whose diabetes was managed by diet alone (13.0%) (p = 0.036). This suggests higher rates of comorbidity or more aggressive treatment in the higher treatment intensity groups.
Treatment with insulin, as a marker for disease severity, was associated with increased physical and mental health burden. Individuals treated with insulin were almost one standard deviation below population norms on the PHC, suggesting a large effect. Further, insulin use was associated with nearly a seven point deficit on the MHC relative to the population norm, representing a moderate to large effect. Deficits in health status were smaller in less intense treatment groups relative to the population norms for each composite (i.e. the T-Score of 50).
Although the comparison between diet alone and the insulin treatment groups was statistically significant for both the PHC and MHC, the effect size was small to moderate. For the HUI3, however, differences in the overall, vision, pain and emotion single attribute scores were relatively large and exceeded the difference that would be considered clinically important. The difference between individuals managed with diet alone compared to oral medication were relatively small for the PHC and MHC of the RAND-12, but the difference in overall HUI3 score achieved clinical importance. Thus, the HUI3 may be more sensitive than the RAND-12 to the burden associated with increased severity of type 2 diabetes.
Our findings for treatment intensity are consistent with previous research in that increased intensity of treatment (i.e. progressing from diet to oral medications and finally to insulin) in individuals with type 2 diabetes has been associated with lower levels of HRQL in previous cross-sectional studies [3, 4, 6]. However, when the UKPDS examined treatment intensity of type 2 diabetes longitudinally, it was found that intensive policies to manage blood glucose did not adversely affect HRQL [28]. Thus, the relationship between increased intensity of treatment and decreased HRQL could be attributable to increased treatment burden, but may also reflect the fact that more intense treatment is associated with more advanced or severe disease.
It was hypothesized that emergency room visits and days off work attributable to diabetes would be related to a diabetic complication or comorbidity, and, thus, these variables could be used as additional markers for varying degrees of disease severity as no direct measures were available in the data. The physical and mental health burden associated with emergency room visits and time off work for diabetes was significantly larger than the burden seen for treatment regimen. The effect size of the difference in disease burden was large according to absenteeisms from work and emergency room visits for diabetes. The need for time off work or an emergency room visit was associated with MHC scores approximately 1.0 and PHC scores approximately 1.2 to 1.4 standard deviations below the population norms of 50 for each composite. This suggests having severe disease was associated with substantial burden, both physical and mentally, relative to the population from which the norms for the RAND-12 were derived.
Emergency room visits due to diabetes were associated with a larger physical health deficit than mental health burden for the RAND-12. The deficits observed on overall HUI3 scores associated with emergency room visits and absenteeism from work appeared to be driven mainly by the pain attribute. Differences in the remaining single attributes were small, with the exception of the differences in the emotion attribute according to absenteeism from work, which was clinically important and statistically significant.
Only small variations in HRQL scores were seen for individuals according to the three Hb1Ac groups, with the exception of the pain attribute. Thus, the burden associated with poor control of blood glucose was not captured by cross-sectional assessment of HRQL using the RAND-12 PHC, MHC, overall HUI3 or any of the remaining single attributes. This may suggest that the generic measures of health status that were used were not sensitive enough to detect differences between these groups, a result similar to previous research using other generic measures of HRQL in diabetes [28–31]. Generally, generic measures have failed to demonstrate an association between HRQL and HbA1c, while specific measures of HRQL have more frequently demonstrated a significant relationship between HRQL and control of blood glucose [15, 32, 33]. The failure to demonstrate a relationship between HRQL and control of blood glucose in this study could attributable to other factors unrelated to the instruments. The lack of an observed relationship could be due to a weak relationship between control of glucose and HRQL or due to the use of average control over three months (HbA1c), rather than episodes of hyperglycemia or hypoglycemia [33]. Indicators of unstable control may better reflect the overall disease burden of diabetes rather than average control of blood glucose over a three month period. While HbA1c is associated with complications and microvascular complications are associated with HRQL, evidence for the direct association between HbA1c and HRQL cross-sectionally is not strong.
After controlling for a number of important determinants of health that would likely affect health status and HRQL (e.g. sex, education, income, body mass index), we demonstrated important differences in HRQL for different levels of diabetes severity. We also demonstrated the ability of these widely used HRQL measures to pick up these differences. Generic, utility-based HRQL scores, such as the HUI3, are important in that they can be incorporated into quality-adjusted life years and economic evaluations of health care interventions. Unfortunately, the use of preference-based measures in diabetes has been limited. In fact, a review of the literature only produced a limited number of studies which used a preference-based measure [27–30]. The majority of these studies derived utility scores from the EQ-5D [27–29], while one study used the Quality of Well-Being Index [30]. Utility scores vary between instruments, likely due to differences in the range of possible scores, method by which preferences are elicited and the content of the instruments (i.e. the attributes of health status captured, the number of levels for assessing degree of impairment, and the weight given to each attribute in calculating overall scores). Such differences have the potential to affect the manner in which the instruments behave in populations with diabetes, making some instruments more sensitive to the health deficits specifically associated with diabetes. It is necessary to assess the construct validity of each preference-based measure, as results from one instrument cannot be generalized to others. This study provides the first evidence that the HUI3 captures the HRQL burden of disease severity in type 2 diabetes.
It has been argued that generic measures of HRQL have an advantage over specific measures in that they permit comparisons across disease states. Such information could potentially be useful to assist with resource allocation and policy decision making. Utility values obtained using different methods and different instruments vary considerably for the reasons outlined previously, but may also vary between study samples due to differences in demographics, clinical characteristics, etc. That said, it still may be useful to compare utility values of other diseases (obtained using the same instrument) to provide a frame of reference for community preferences for the health states associated with type 2 diabetes. For example, in a population-based study using the HUI3, it was found that the average overall HUI3 score for individuals with stroke was 0.54 and arthritis was 0.77 [22]. In this study the average overall HUI3 score was 0.64 ± 0.30, suggesting the average preference for health states associated with type 2 diabetes was less than stroke, but more than arthritis. Direct comparisons are limited, however, as we did not control for the number of additional comorbid medical conditions while Grootendorst et al. did; other demographic differences between samples could be important as well [22].
A number of limitations in this study should be recognized. First, the number of individuals for which HRQL data was missing was relatively large for some HRQL measures and statistically significant differences between individuals with complete and missing data for the various HRQL measures were found. It is unclear how these differences would affect study results. Individual missing HRQL data were older and had lower socio-economic status. It is possible that this systematic absence of data would weaken several of the observed relationships and understate the burden of diabetes. Further assessment of the impact of missing data and imputation methods are planned. As well, in carrying out a multivariate analysis, individuals with missing data on covariates were excluded from the analysis. For most analyses, no differences were found in HRQL scores for individuals included in and missing from the multivariate analyses. The exception to this was the analysis according to absenteeism from work due to diabetes. As no association was found between the probability of being excluded and the grouping variable (i.e. being absent from work), it is unlikely that the effect of excluding subjects missing covariates biased the between groups comparisons. However, since the excluded individuals were healthier, the burden in both groups may have been overstated for this particular analysis.
Data on treatment for diabetes, emergency room visits and absenteeism from work were based on self-report and this could potentially be a study limitation. However, a high level of agreement was observed between self-reported treatment of diabetes and data obtained through a formal medication history taken by research coordinators for these patients, so data on treatment regimen is likely reliable [34]. An additional limitation of the study was the lack of direct data on the presence of complications, which has been shown in past research to be associated with HRQL in diabetes [28]. Instead, this study used treatment intensity, emergency room visits and time off work for diabetes, with the assumption that these variables were accurate markers for disease severity. It was then assumed that more severe diabetes would be associated with more complications. Unfortunately, data on complications was not collected as part of the larger study and was not available. Another limitation of the study was the relatively small number of individuals who reported being absent from work or visiting an emergency room for diabetes. Finally, it was not clear how representative this sample was of the general population of individuals with type 2 diabetes, although generalizing the study findings beyond rural Albertans with type 2 diabetes was not the purpose of this study. Rather, it was our objective to capture the disease burden of type 2 diabetes in rural Albertans. As we are reasonably confident that our study sample was representative of the target population [20], we feel that this objective has been accomplished.
Conclusions
The PHC and MHC of the RAND-12, the overall HUI3 and diabetes relevant single attributes captured differences in burden associated with treatment regimen, emergency room visits and absenteeism from work due to diabetes. Glycated hemoglobin (HbA1c), a physiologic measure of average glycemic control, was not related to the majority of the generic HQRL scores and did not adequately reflect individuals' overall physical and mental health. We believe that HBA1c is a nonspecific and insensitive measure of disease burden in diabetes, despite it being an important prognostic physiologic parameter. We would encourage the use of HRQL measures to capture the disease burden of type 2 diabetes, rather than focusing on physiological parameters.
Authors Contributions
SRM, ET, and JAJ conceived the DOVE study and its design, and participated in its coordination.
DHF, JAJ and SLM conceived the HRQL sub-analysis of the DOVE study.
SLM carried out the data analysis and drafted the manuscript.
All authors contributed to the writing and editing of the final manuscript.
Conflict of Interest
David Feeny is an owner of Health Utilities Incorporated
Abbreviations
- PHC:
-
Physical Heath Composite
- MHC:
-
Mental Health Composite
- HUI3:
-
Health Utilities Index Mark 3
- HRQL:
-
Health related quality of life
- HbA1c:
-
Glycated hemoglobin
- BMI:
-
Body Mass Index
- HMG-CoA:
-
hydroxymethyglutaryl co-enzyme A reductase
- UKPDS:
-
United Kingdom Prospective Diabetes Study
- SAU:
-
Single attribute utility
References
Ahroni JH, Boyko EJ, Davignon DR, Pecoraro RE: The health and functional status of veterans with diabetes. Diabetes Care 1994,17(4):318–321.
Peyrot M, Rubin RR: Levels and risks of depression and anxiety symptomology among diabetic adults. Diabetes Care 1997, 20: 585–590.
Jacobson AM, de Groot M, Samson JA: The evaluation of two measures of quality of life in type 1 and type 2 diabetes. Diabetes Care 1994, 17: 267–274.
Keinanenn-Kiukaanniemi S, Ohinma A, Pjunpaa H, Koivukangas P: Health related quality of life in diabetic patients measured by the Nottingham Health Profile. Diabetic Medicine 13: 382–388. 10.1002/(SICI)1096-9136(199604)13:4<382::AID-DIA14>3.0.CO;2-Y
Anderson RM, Fitzgerald JT, Wisdom K, Davis WK, Hiss RG: A comparison of global versus disease-specific quality-of-life measures in patients with NIDDM. Diabetes Care 1997, 20: 299–305.
Glasgow RE, Ruggiero L, Eakin EG, Dryfoos J, Chobanian L: Quality of life and associated characteristics in a large national sample of adults with diabetes. Diabetes Care 1997, 20: 562–567.
Luscombe FA: Health-related quality of life measurement in type 2 diabetes. Value in Health 2000,3(1):S15-S28. 10.1046/j.1524-4733.2000.36032.x
Clinical practice guidelines for the management of diabetes in Canada Can Med Assoc J 1998,159(Suppl 8):S1-S29.
The Diabetic Control and Complications Trial Research Group: The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. New Engl J Med 1993, 329: 977–986. 10.1056/NEJM199309303291401
Wandell PE, Brorsson B, Aberg H: Quality of life in diabetic patients registered with primary health care services in Sweden. Scand J Soc Health Care 1997, 15: 97–102.
Aalto AM, Uutemla A, Kangas T: Health behavior, social integration, perceived health and dysfunction. A comparison between type 1 and 2 diabetes and controls. Scand J Soc Med 1996, 24: 272–281.
Gafvels G, Borjesson B, Lithner F: The social consequences of insulin-treated diabetes mellitus in patients 20–50 years of age. An epidemiological case-control study. Scand J Soc Med 1991, 19: 86–93.
Anderson RJ, Freedland KE, Clouse RE, Lustman PJ: The prevalence of comorbid depression in adults with diabetes. Diabetes Care 2001,24(6):1069–1078.
Bourdel-Marchasson I, Dubroca B, Manciet G, Deschamps A, Emeriau JP, Dartigues JF: Prevalence of diabetes and effect on quality of life in older French living in the community: the PAQUID Epidemiological Survey. J Am Geriatr Soc 1997, 45: 295–301.
Rubin RR, Peyrot M: Quality of life and diabetes. Diabetes Metab Res Rev 1999, 15: 205–218. 10.1002/(SICI)1520-7560(199905/06)15:3<205::AID-DMRR29>3.0.CO;2-O
Aalto M, Uutela A, Aro AR: Health related quality of life among insulin dependent diabetics: disease-related and psychosocial correlates. Patient Educat Couns 1997, 30: 215–225. 10.1016/S0738-3991(96)00963-9
Klein BE, Klein R, Moss SE, Self-rated health and diabetes of long duration: The Wisconsin Epidemiologic Study of Diabetic Retinopathy. Diabetes Care 1998, 21: 236–240.
Wredling R, Stalhammar J, Adamson U, Berne C, Larsson Y, Oestman J: Well-being and treatment satisfaction in adults with diabetes: a Swedish population-based study. Qual Life Res 1995, 5: 515–522.
Parkerson GR, Connis RT, Broadhead WE, Patrick DL, Taylor TR, Chiu-Kit JT: Disease-specific versus generic measurement of health related quality of life in insulin-dependent diabetic patients. Med Care 1993, 31: 629–639.
Majumdar SR, Guirguis LM, Toth EL, Lewanczuk RZ, Lee TK, Johnson JA: Controlled trial of a multifaceted intervention for improving quality of care for rural patents with type 2 diabetes. Diabetes Care 2003, 26: 3061–3066.
Feeny DH, Furlong WJ, Torrance GW, Goldsmith CH, Zhu Z, DePauw S, Denton M, Boyle M: Health Utilities Index. Multiattribute and single-attribute utility functions for the Health Utilities Index Mark 3 system. Med Care 2002,40(2):113–128. 10.1097/00005650-200202000-00006
Grootendorst P, Feeny D, Furlong W: Health Utilities Index Mark 3: Evidence of construct validity for stroke and arthritis in a population health survey. Med Care 2000,38(3):290–299. 10.1097/00005650-200003000-00006
Horsman JR, Furlong WJ, Feeny DH, Torrance GW: The Health Utilities Index (HUI® ): concepts, measurement properties and applications. Health and Quality of Life Outcomes 2003, 1: 54. 10.1186/1477-7525-1-54
Hays RD: RAND-36 Health Status Inventory. The Psychological Corporation. San Antonio 1998.
Ware JE, Kosinski M, Keller SD: A 12-item short form health survey: construction of scales and preliminary tests of reliability and validity. Med Care 1996, 34: 220–233. 10.1097/00005650-199603000-00003
Johnson JA, Maddigan SL: Performance of RAND-12 and SF-12 in type 2 diabetes. Qual Life Res Forthcoming
Cohen J: A power primer. Psychological Bulletin 1992, 112: 155–159. 10.1037//0033-2909.112.1.155
U.K. Prospective Diabetes Study Group: Quality of life in type 2 diabetic patients is affected by complications but not by intensive policies to improve blood glucose or blood pressure control (UKPDS 37). Diabetes Care 1999,22(7):1125–1136.
Holmes J, McGill S, Kind P, Bottomley J, Gillam S, Murphy M: Health-related quality of life in type 2 diabetes (T2 ARDIS-2). Value in Health 2000,3(Suppl 1):S47-S51. 10.1046/j.1524-4733.2000.36028.x
Redekop WK, Koopmanschap MA, Stolk RP, Rutten GEM, Wolffenbuttel BHR, Nielssen LW: Health-related quality of life and treatment satisfaction in Dutch patients with type 2 diabetes. Diabetes Care 2002,25(3):458–463.
Coffey JT, Brandle M, Zhou H, Marriott D, Burke R, Tabaei BP, et al.: Valuing health-related quality of life in diabetes. Diabetes Care 2002,25(12):2238–2243.
Van der Does FE, de Neeling JN, Snoek FJ, et al.: Symptoms and well-being in relation to glycemic control in type II diabetes. Diabetes Care 1993, 19: 204–210.
Testa MA, Simonson D: Health economic benefits and quality of life during improved glycemic control in patients with type 2 diabetes mellitus: A randomized, controlled, double-blind trial. J Am Med Assoc 1998,280(17):1490–1496. 10.1001/jama.280.17.1490
Schapansky LA, Johnson JA, Majumdar S, Lewanczuk R, Lee TK, Toth EL: The burden of pharmacotherapy for patients with type 2 diabetes in rural Alberta: data from the DOVE Study [abstract]. Can J Clin Pharmacol 2001, 8: 22.
Acknowledgements
Dr. Johnson and Dr. Majumdar are Population Health Investigators with the Alberta Heritage Foundation for Medical Research (AHFMR). Dr. Johnson holds a Canada Research Chair in Diabetes Health Outcomes. Ms. Maddigan holds a Full-time Studentship in Health Research with AHFMR.
The authors acknowledge useful suggestions made by three reviewers from the Institute of Health Economics.
The DOVE Investigators are Dr. Ellen Toth (Principal Investigator), Dr. Jeffrey A. Johnson, Dr. Sumit R. Majumdar, Dr. Richard Lewanczuk, Dr. TK Lee, Ms. Lisa Guirguis (Project Officer).
Funding for the DOVE Study was provided by the Canadian Diabetes Association, Caritas Health Group, and the Institute of Health Economics.
This work was supported by a New Emerging Team (NET) grant to the Alliance for Canadian Health Outcomes Research in Diabetes (ACHORD). The ACHORD NET grant is sponsored by the Canadian Diabetes Association, the Heart and Stroke Foundation of Canada, The Kidney Foundation of Canada, the CIHR – Institute of Nutrition, Metabolism and Diabetes and the CIHR – Institute of Circulatory and Respiratory Health.
Author information
Authors and Affiliations
Consortia
Corresponding author
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Maddigan, S.L., Majumdar, S.R., Toth, E.L. et al. Health-related quality of life deficits associated with varying degrees of disease severity in type 2 diabetes. Health Qual Life Outcomes 1, 78 (2003). https://doi.org/10.1186/1477-7525-1-78
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7525-1-78