
Abstract
Background
The purpose of this study was to determine the effect of stress reduction via the Transcendental Meditation program on school rule infractions in adolescents.
Methods
Forty-five African American adolescents (ages 15–18 years) with high normal systolic blood pressure were randomly assigned to either Transcendental Meditation (n = 25) or health education control (n = 20) groups. The meditation group engaged in 15-min sessions at home and at school each day for 4 months. The control group was presented 15-min sessions of health education at school each day for 4 months. Primary outcome measures were changes in absenteeism, school rule infractions and suspension days during the four-month pretest period prior to randomization compared with the four-month intervention period.
Results
Comparing the pretest and intervention periods, the meditation group exhibited a mean decrease of 6.4 absentee periods compared to an increase of 4.8 in the control group (p < .05). The meditation group exhibited a mean decrease of 0.1 infractions over the four months compared to an increase of 0.3 in the control group (p < .03). There was a mean reduction of 0.3 suspension days due to behavior-related problems in the meditation group compared to an increase of 1.2 in the control group (p < .04).
Conclusion
These findings demonstrate that the Transcendental Meditation program conducted in the school setting has a beneficial impact upon absenteeism, rule infractions, and suspension rates in African American adolescents.
Similar content being viewed by others


Background
The prevalence of negative school behaviors remains a significant health problem in the U.S [1]. For example, with respect to behaviors that contribute to intentional injuries, according to the Youth Risk Behavior Surveillance Survey, 36.6% of high school students reported having been in a physical fight in the past month, with 14.8% of the fights occurring on school property, 3.5% were injured in a physical fight and five percent of students missed school because of feeling unsafe [1]. Results of studies attempting to reduce such aggressive behaviors in schools have been mixed. A school-based violence prevention curriculum reportedly reduced self-reported aggressive behaviors among middle school boys in 2 of 6 classes only [2]. On the other hand, an 18-session violence-prevention curriculum [3], resulted in decreased frequency of self-reported violence and other problem behaviors in 6th grade boys, but not in girls [4]. Few studies have focused on observable behavioral outcomes and findings have been mixed [5]. 'Students for Peace', a multi-component violence prevention project with 9000 middle school students, failed to reduce fights at school and absenteeism due to feeling unsafe at school [6]. Violence prevention education has been reported to reduce suspension rates [7].
It has been hypothesized that the high prevalence of negative school behaviors is in part due to greater exposure to chronic psychosocial stress, e.g., inadequate economic resources, family disintegration, information overload, media violence [8–11]. Self-reported feelings of anger have been shown to be predictive of aggression in youth [12]. The escalating prevalence of anger and violence in youth has been associated in part with increased levels of anxiety and stress [13].
School systems are increasingly interested in reducing negative school behaviors, however, they have had difficulty identifying programs that are effective and easy to implement on a broad scale [14]. Given the urgent need and the readiness of school boards to address these needs, the testing and implementation of promising intervention programs is of great urgency. One approach to the growing problem of school-related conduct problems may be to provide skills in stress reduction. Few studies have examined whether stress reduction programs improve school behavior in youth.
Research suggests that behavioral stress reduction via the Transcendental Meditation® (TM) program may hold promise in the improvement of school-related behaviors in youth. Research has demonstrated that TM produces improvements in mental health, including reduction of various forms of psychological distress, such as depression, anxiety, hostility and emotional instability [15–21]. TM has been shown to reduce aggression [22], and to increase overall relaxation in adults [23].
Black college students and adults increased significantly on an overall mental health factor and showed a greater reduction in self-reported anxiety and neuroticism after one year of TM practice [24]. Although findings have not been entirely consistent [25], improved academic performance has been reported in high school students practicing TM [26], and in African American college students practicing a simple meditation process [27]. In a medium-sized chemical manufacturing company, with employees practicing TM over a six-year period, days lost through illness or injury decreased by 50 per cent and absenteeism declined by 89 per cent [28]. These findings suggest that examination of the effects of TM on improving school-related behaviors in youth is warranted.
This study was part of a larger study examining the impact of stress reduction via TM on high normal blood pressure levels in adolescents. The results of this study on blood pressure have been reported previously and indicated a beneficial impact of TM on cardiovascular functioning at rest and during stress [29]. This is the first report of a controlled trial of stress reduction via TM as a means of improving school-related conduct behaviors. In the present study, African American youth with high normal blood pressure (BP) were randomly assigned to either a 4-month TM program experimental group or a health education control group. Based on previous findings it was predicted that youth who practiced TM would exhibit greater decreases in school absenteeism, rule infractions, and days suspended from pre-test to 4 month post-test than controls.
Methods
Procedures
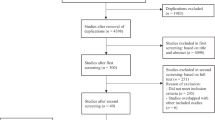
A blood pressure screening was conducted on 677 youth in two inner-city public high schools. These schools were chosen on the basis of being representative of the broader population of African American high school students in Richmond County. Forty-five African American adolescents (ages 15–18 years) were eligible on the basis of resting systolic blood pressure ≥ 85th percentile on 3 consecutive occasions with respect to age, gender and height [30]. None of the students declined to participate. Each school was alternately assigned to either TM (n = 25, 6 females, 19 males) or a health education control (CTL, n = 20, 7 females, 13 males). The study was conducted over 2 semesters with two 4-month interventions per semester. In order to control for differences between the schools, the order of interventions was counterbalanced between schools with both schools receiving both the TM or CTL interventions by the completion of the study. The students were assigned to only one intervention. The sample size variation was due to a disparity in subject recruitment between the schools. The blood pressure findings have been reported previously [29].
The TM group engaged in 15-min sessions as a group at school and individually at home, each school day, as well as 15-min twice-daily individual home practice on weekends for 4 months. The students self-reported that they typically meditated in their bedrooms at home, where they were not interrupted. The CTL group was presented with 4 months of daily 15-min school sessions of lifestyle education. These sessions were intended to provide comparable time and attention from the intervention leader to the CTL subjects. Attendance was monitored for all sessions at school and weekly 'participation cards' were completed by the subjects to document meditations at home.
After four months of intervention both groups' data were collected from the school records of grades, school disciplinary actions (i.e., rule infractions such as dress code violations, excess tardies, disruptive classroom behavior, fighting, etc.), numbers of absentee and tardy periods, and suspension days for behavior-related problems for the 4 months preceding the intervention and for the 4 months of the intervention.
Measurements
Permission to conduct the study was granted by the Superintendent of Richmond County Public Schools and the Medical College of Georgia Human Assurance Committee. All pre- and post intervention assessments testing was conducted at the Georgia Prevention Institute of the Medical College of Georgia. After consent and assent forms were signed, subjects completed an expectation of benefits questionnaire, and parents completed a demographic information form. Subjects completed the Spielberger Anger Expression Scale [31], as well as measures of lifestyle and environmental stress, including television viewing, before and after the 4 month intervention period [32]. A Detecto CN220 scale with height rod (Cardinal Scale Manufacturing Corp, Webb City, MO) was used to measure the height and weight according to standard protocol [33].
Suspension rates
The number of days suspended before and during the 4-month intervention was determined from school records. The change in the number of days suspended between the period 4 months before intervention and the 4 months during the intervention period was the primary outcome measure. Suspension categories specific to violence included fighting, classroom disruption, as well as other categories involving high-risk behaviors such as illegal absences, disregarding commands, excessive tardies and leaving campus without permission.
Tardies and Absenteeism
The accumulated numbers of tardy and absentee class periods in the 4-month intervention period were compared with the 4-month pre-intervention period.
Grades
The grade percentage achieved at the end of the 4-month intervention period was compared with that of the 4-month pre-intervention period.
Rule infractions
A separate measure of rule infractions (total number of infractions as defined by the Augusta Richmond County Board of Education, such as dress violations, excess tardies, disruptive classroom behavior, fighting) was determined from the school records. The number of rule infractions during the 4-month intervention period was compared with the number of rule infractions during the 4-month period before the intervention.
Interventions
Stress reduction
The rationale for the selection of TM rather than a standard meditation technique is that TM is by far the most studied mental relaxation technique [23]. The TM technique has been described as a simple mental procedure practiced for 15 min twice a day while sitting comfortably with eyes closed [34]. The TM technique has its origin in the ancient Vedic approach to health [35], and does not require changes in personal belief, lifestyle, or philosophy [36]. No mental effort is required toward intentionally altering physiological processes (e.g., respiration rate, muscle relaxation, etc.). The ordinary thinking process becomes quiescent and a distinctive state of psycho-physiological 'restful alertness', a wakeful but deeply restful state, is gained [37, 38]. The TM technique was taught by a certified TM instructor using the standard seven-step program presented on consecutive days. The first and second steps are introductory and preparatory lectures presented in a group. The third and fourth steps are conducted individually and consist of a personal interview, and instruction. The remaining three steps are verification and validation of the practice and are presented in a group format.
Health Education Control
A didactic series of lessons was presented focusing upon the role of weight management, diet and physical activity in the prevention of essential hypertension and their beneficial influence upon blood pressure and other CVD risk factors based on National Institutes of Health guidelines on weight loss, diet (reducing salt and sodium intake) and increasing physical activity. See: http://www.nhlbi.nih.gov/health/prof/heart/index.htm. Subjects attended daily 15-minute school sessions during the 4-month intervention period.
Statistical analyses
The comparability between the two groups at pre- and post-intervention on all sociodemographic and anthropometric variables (e.g., age, weight, height) was assessed via a series of 2 (intervention group: TM vs. CTL) by 2 (time: pre- vs. post-intervention) repeated measures analyses of variance (ANOVA) with time as the repeated measure.
Absentee periods, grade point average, tardies, and days suspended were analyzed as dependent variables using 2 (intervention: TM vs. CTL) by 2 (time: pre- vs. post-intervention) repeated measures ANOVAs. Anger in, anger out, and anger control were analyzed as dependent variables using 2 (sex: male vs. female) by 2 (intervention: TM vs. CTL) by 2 (time: pre- vs. intervention period) repeated measures ANOVAs. Gender was included in the analysis due to previous reports of gender differences in self-reports of anger coping styles [39].
Results
Descriptive characteristics
Descriptive characteristics of the TM and CTL groups are presented in Table 1. There were no significant main (i.e., group, time) or interaction effects for any parameter (all ps > .10) indicating the groups did not differ significantly at pre-intervention in any anthropometric or demographic parameters. The groups did not differ at pre-intervention in expectation of benefits (p > .10).
Compliance
From the attendance monitored at sessions at school and self reports to document meditations at home, which included 240 possible school and home meditation sessions, a determination of average compliance of the TM group for twice daily practice was calculated as 71.6%. Compliance ranged from 5.8 to 97.4%, with 15/25 subjects determined to be greater than 70% compliant.
Rule Infractions and Suspension Rates
As depicted in Table 2, the TM group exhibited a mean total reduction of 0.1 rule infractions over the four months of intervention compared to an increase of 0.3 infractions in the CTL group (F 1,38 = 5.4, p < .03). There was a mean total reduction of 0.3 suspension days due to behavior-related problems in the TM group compared to an increase of 1.2 suspension days in the CTL group (F 1,39 = 4.7, p < .04).
Tardy and Absentee Periods
Comparing the pre-intervention and intervention periods, the TM group exhibited a mean total reduction of 6.4 absentee class periods compared to an increase of 4.8 in the CTL group (F 1,33 = 4.2, p < .05, see Table 2 for means). Comparing the pre-intervention and intervention periods, the TM group exhibited a non-significant decrease of 0.5 tardies compared to an increase of 0.6 tardies in the CTL group (F 1,39 = 0.3, p = ns).
Grades
Non-significant changes were observed in grade point average between the TM group which increased by 0.2% and CTL group which decreased by 1.1% (F 1,36 = 0.75, p > .10).
Anger
A group x sex x time interaction was observed for anger-in such that the TM group females exhibited greater decreases compared to slight increases among the CTL group females while no significant changes were observed in males (F 1,36 = 5.7, p < .03). No significant main or interaction effects were observed for anger-out and anger control (all ps > .21). Regarding other psychosocial variables, no significant main or interaction effects were observed between the groups on measures of lifestyle and environmental stress (all ps > .10).
Discussion
To our knowledge this is the first clinical trial examining the impact of a behavioral stress-reduction intervention on a quality of life-related issue (school behavior) in youth. This study examined the impact of a four-month participation in the TM program on absenteeism, rule infractions, and suspension rates in adolescents with high normal BP. The findings were not attributable to baseline differences in anthropometrics since the TM and control groups were similar on these parameters at pre- and post-intervention, and both groups were similar in their expectations of health benefits at pre-intervention. Evaluation of impact of possible moderators, such as exposure to environmental stress, i.e., neighborhood stress, showed no differences between the groups. All subjects resided in the same geographical locale (i.e., lower socioeconomic status neighborhoods), and none participated in any formal lifestyle programs during the intervention period, besides school sports and/or physical education.
Counterbalancing interventions between schools controlled for school-to-school variations in which unknown characteristics of a particular school population or policies of operation could have differentially impacted implementation of the protocol. A previously reported beneficial impact on cardiovascular functioning was shown by decreases in systolic blood pressure from pre- to post-intervention in the TM group compared to controls [29]. The TM group also exhibited greater decreases in systolic blood pressure reactivity to acute laboratory behavioral stressors [29]. These physiological benefits are corroborated with behavioral and psychological benefits in the present study.
The present findings compare favorably with the results of another skills-based approach upon conduct related behaviors. Changes in suspension status among 1523 high school students was compared across groups exposed to school-based violence prevention. Those exposed in a class-specific violence prevention education intervention showed a 71% reduction in suspension rate [7]. The present study showed a reduction in suspensions of 83% during the 4-month intervention. Improvement in overall mental health factor and reduction in anxiety and neuroticism in African American college students was previously shown after one year of TM practice [24]. These findings are encouraging and indicate a combination of anger management, conflict resolution skills testing and stress reduction may be particularly beneficial and need to be examined.
The present study extends previous findings, with incorporation of a randomized controlled study design and use of documented records of behavior rather than typical self-report data which are open to the problem of social desirability. Counterbalancing treatment assignment by school decreased likelihood of within-school intervention contamination owing to potential inter-subject interactions, and unanticipated between-school differences. Efforts were made to provide comparable instruction time and attention at school to both groups. Similar to the present findings, previous findings using health education as a control, reportedly did not impact the attitudinal or behavioral preferences for non-aggressive conflict resolution among 6th grade students [40].
One strength of the intervention is that the TM technique was taught in a standardized manner by a qualified TM instructor. Subjective meditation experiences were monitored by the TM instructor via self-reports and additional instruction was provided when necessary. Daily group TM practice in the presence of the instructor facilitated successful practice. The present findings are supported by other TM studies which have shown reductions in aggression [22], anxiety [41], stress-related neuromodulators, such as cortisol [42], and blood pressure [43] in Caucasian American adults. Since the present study was conducted in inner-city public high schools, with African American students with high normal blood pressure, empirical evaluation is needed to determine if the findings may be generalizable to other students.
Although the present findings are promising, there are several limitations of the study. First, the limited sample size and duration of evaluation was not long enough to provide sufficient frequencies of occurrences for several measures such as specific categories of suspension rates such as physical fighting, weapon carrying and drug possession. A similar sample size of 34 subjects was sufficient to demonstrate the impact of TM on blood pressure and cardiovascular reactivity to stress in adolescents [29]. Second, a follow-up evaluation beyond that of the 4-month intervention to determine whether the TM effect was sustained or if students reverted to negative behaviors was not conducted. Future studies should attempt to determine the mechanisms responsible for the impact of TM on school-related conduct problems and attendance by assessing possible changes in perceived negative affective and/or behavioral impact of stressors and/or utilizing mock conflict-evoking scenarios to determine possible changes in behavioral response patterns.
Conclusions
The TM group exhibited a decrease in absentee periods, rule infractions and suspension days due to behavior-related problems compared to the CTL group. The findings also indicate a potential beneficial impact upon anger expression in African American females. The successful implementation of the intervention suggests the feasibility of school-based stress reduction programs in efforts to improve both physical and behavioral risk factors in youth.
Author contribution
VB and FT designed the study, secured funding and supervised the execution of the study. VB recruited subjects and supervised the intervention. VB, LB and FT analyzed the data. All authors contributed the manuscript preparation and approved the final paper.
References
Brener ND, Simon TR, Krug EG, Lowry R: Recent trends in violence-related behaviors among high school students in the United States. JAMA 1999, 282: 440–446. 10.1001/jama.282.5.440
Orpinas P, Parcel GS, McAlister A, Frankowski R: Violence prevention in middle schools: a pilot evaluation. J Adolesc Health 1995, 17: 360–371. 10.1016/1054-139X(95)00194-W
Farrell AD, Meyer AL, Dahlberg LL: Richmond youth against violence: a school-based program for urban adolescents. Am J Prev Med 1996, 12: 13–21.
Farrell AD, Meyer AL: The effectiveness of a school-based curriculum for reducing violence among urban sixth-grade students. Am J Public Health 1997, 87: 979–984.
Webster DW: The unconvincing case for school-based conflict resolution programs for adolescents. Health Aff 1993, 12: 126–141. 10.1377/hlthaff.12.4.126
Orpinas P, Kelder S, Frankowski R, Murray N, Zhang Q, McAlister A: Outcome evaluation of a multi-component violence-prevention program for middle schools: the Students for Peace project. Health Educ Res 2000, 15: 45–58. 10.1093/her/15.1.45
Hausman A, Pierce G, Briggs L: Evaluation of comprehensive violence prevention education: effects on student behavior. J Adolesc Health 1996, 19: 104–110. 10.1016/1054-139X(96)00128-0
Weist MD, Paskewitz DA, Jackson CY, Jones D: Self-reported delinquent behavior and psychosocial functioning in inner-city teenagers: a brief report. Child Psychiatry Hum Dev 1998, 28: 241–248. 10.1023/A:1022684031414
Rosella JD, Albrecht SA: Toward an understanding of the health status of black adolescents: an application of the stress-coping framework. Issues Compr Pediatr Nurs 1993, 16: 193–205.
Guerra NG, Huesmann LR, Tolan PH, Van Acker R, Eron LD: Stressful events and individual beliefs as correlates of economic disadvantage and aggression among urban children. J Consult Clin Psychol 1995, 63: 518–528. 10.1037//0022-006X.63.4.518
Spencer MB, Dobbs B, Swanson DP: African American adolescents: adaptational processes and socioeconomic diversity in behavioral outcomes. J Adolesc 1988, 11: 117–137.
Cornell DG, Peterson CS, Richards H: Anger as a predictor of aggression among incarcerated adolescents. J Consult Clin Psychol 1999, 67: 108–115. 10.1037//0022-006X.67.1.108
Lowry R, Cohen LR, Modzeleski W, Kann L, Collins JL, Kolbe LJ: School violence, substance use, and availability of illegal drugs on school property among US high school students. J Sch Health 1999, 69: 347–355.
Everett SA, Kann L, McReynolds L: The Youth Risk Behavior Surveillance System: policy and program applications. J Sch Health 1997, 67: 333–335.
Brooks JS, Scarano T.: Transcendental Meditation in the treatment of post-Vietnam adjustment. Journal of Counseling and Development 1985, 65: 212–215.
Alexander CN, Swanson GC, Rainforth MV, Carlisle TW, Todd CC, Oates RM: Effects of the Transcendental Meditation program on stress reduction, health, and employee development: A prospective study in two occupational settings. Anxiety, Stress and Coping: An International Journal 1993, 6: 245–262.
Haratani T, Hemmi T: Effects of Transcendental Meditation (TM) on the mental health of industrial workers. Japanese Journal of Industrial Health 1990, 32: 656.
Davis L: Management of depression in general practice. British Medical Journal 1986, 292: 64.
Eppley K, Abrams AI, Shear J: Differential effects of relaxation techniques on trait anxiety: A meta-analysis. Journal of Clinical Psychology 1989, 45: 957–974.
Abrams AI, Siegel LM: The Transcendental Meditation program and rehabilitation at Folsom State Prison: A cross-validation study. Criminal Justice and Behavior 1978, 5: 3–20.
Aron A, Orme-Johnson DW, Brubaker P: The Transcendental Meditation program in the college curriculum: A 4-year longitudinal study of effects on cognitive and affective functioning. College Student Journal 1981, 15: 140–146.
Shapiro J: The relationship of the TM program to self-actualization and negative personality characteristics. In: Scientific research on the Transcendental Meditation program: Collected papers (Edited by: Orme-Johnson DW, Farrow JT). Rheinweiler, W. Germany: Maharishi European Research University Press; 1976, 1: 462–467.
Alexander CN, Robinson P, Orme-Johnson DW, Schneider RH, Walton KG: Effects of Transcendental Meditation compared to other methods of relaxation and meditation in reducing risk factors, morbidity and mortality. Homeostasis 1994, 35: 243–264.
Gaylord C, Orme-Johnson D, Travis F: The effects of the Transcendental Meditation technique and progressive muscle relaxation on EEG coherence, stress reactivity, and mental health in black adults. International Journal of Neuroscience 1989, 46: 77–86.
Carsello CJ, Creaser JW: Does transcendental meditation training affect grades? J Appl Psychol 1978, 63: 644–645. 10.1037//0021-9010.63.5.644
Nidich SI, Nidich RJ: Increased academic achievement at Maharishi School of the Age of Enlightenment: A replication study. Education 1989, 109: 302–304.
Hall PD: The effect of meditation on the academic performance of African American college students. Journal of Black Studies 1999, 29: 408–415.
Swanson G: Enlightened Management: Building High Performance People Fairfield, Iowa: MIU Press 1989.
Barnes VA, Treiber FA, Davis H: Impact of Transcendental Meditation on cardiovascular function at rest and during acute stress in adolescents with high normal blood pressure. J Psychosom Res 2001, 51: 597–605. 10.1016/S0022-3999(01)00261-6
National High Blood Pressure Education Program Working Group on Hypertension Control in Children and Adolescents: Update on the 1987 Task Force Report on High Blood Pressure in Children and Adolescents: a working group report from the National High Blood Pressure Education Program. Pediatrics 1996, 98: 649–658.
Spielberger CD, Johnson EH, Russell SF, Crane RJ, Jacobs GA, Worden TJ: The experience and expression of anger: Construction and validation of an anger expression scale. In: Anger and Hostility in Cardiovascular and Behavioral Disorders (Edited by: Chesney MA, Rosenman RH). New York: Hemisphere/McGraw-Hill 1985, 5–30.
Kann L, Kinchen SA, Williams BI, Ross JG, Lowry R, Hill CV, Grunbaum JA, Blumson PS, Collins JL, Kolbe LJ: Youth risk behavior surveillance – United States, 1997. Mor Mortal Wkly Rep CDC Surveill Summ 1998, 47: 1–89.
National Center for Health Statistics: NHANES III Anthropometric procedures (video),. In: Book NHANES III Anthropometric procedures (video) City: US Dept of Health and Human Services, US Government Printing Office 1988.
Roth R: Maharishi Mahesh Yogi's Transcendental Meditation Washington, DC: Primus 1994.
Maharishi Mahesh Yogi: Maharishi's Vedic Approach to Health Vlodrop, Holland: Maharishi Vedic University Press 1995.
Nader T: Human Physiology – Expression of Veda and the Vedic Literature Vlodrop, Holland: Maharishi Vedic University Press 1994.
Jevning R, Wallace RK, Biedebach M: The physiology of meditation: A review. A wakeful hypometabolic integrated response. Neuroscience and Biobehavioral Reviews 1992, 16: 415–424.
Wallace KR: The Physiology of consciousness Fairfield: Maharishi International University Press 1993.
Casper RC, Belanoff J, Offer D: Gender differences, but no racial group differences, in self-reported psychiatric symptoms in adolescents. J Am Acad Child Adolesc Psychiatry 1996, 35: 500–508. 10.1097/00004583-199604000-00016
Petchers MK, Hirsch EZ, Bloch BA: A longitudinal study of the impact of a school heart health curriculum. J Community Health 1988, 13: 85–94.
Dillbeck MC: The effect of Transcendental Meditation on anxiety level. Journal of Clinical Psychology 1977, 33: 1076–1078.
MacLean CR, Walton KG, Wenneberg SR, Levitsky DK, Mandarino JV, Waziri R, Schneider RH: Altered responses of cortisol, GH, TSH and testosterone to acute stress after four months' practice of Transcendental Meditation (TM). Annals of the New York Academy of Sciences 1994, 746: 381–384.
Wenneberg SR, Schneider RH, Walton KG, MacLean CRK, Levitsky DK, Salerno JW, Wallace RK, Mandarino JV, Rainforth MV, Waziri R: A controlled study on the effects of Transcendental Meditation on cardiovascular reactivity and ambulatory blood pressure. International Journal of Neuroscience 1997, 89: 15–28.
Acknowledgements
This study was supported in part by National Institutes of Health Grant #HL62976 to Dr. Treiber and an American Heart Association Scientist Development Grant #9930073N to Dr. Barnes. We would like to thank Dr. Charles Larke, Superintendent; Dr. Vivian Pennamon, and Mr. Quentin Motley, Principals, Richmond County Public Schools in Augusta, Georgia for their cooperation in providing the facilities for this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing Interests
None declared.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Barnes, V.A., Bauza, L.B. & Treiber, F.A. Impact of stress reduction on negative school behavior in adolescents. Health Qual Life Outcomes 1, 10 (2003). https://doi.org/10.1186/1477-7525-1-10
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-7525-1-10