
Abstract
Background
Parkinson's disease (PD) is the second most common neurodegenerative disorder. Recently, mutations in the PINK1 (PARK6) gene were shown to rarely cause autosomal-recessively transmitted, early-onset parkinsonism. In order to evaluate whether PINK1 contributes to the risk of common late-onset PD we analysed PINK1 sequence variations. A German (85 patients) and a Norwegian cohort (90 patients) suffering from late-onset PD were screened for mutations and single nucleotide polymorphisms (SNPs) in the PINK1 gene. Both cohorts consist of well-characterized patients presenting a positive family history of PD in ~17%. Investigations were performed by single strand conformation polymorphism (SSCP), denaturating high performance liquid chromatography (DHPLC) and sequencing analyses. SNP frequencies were compared by the χ2 test
Results
Several common SNPs were identified in our cohorts, including a recently identified coding variant (Q115L) in exon 1. Genotyping of the Q115L variation did not reveal significant frequency differences between patients and controls. Pathogenic mutations in the PINK1 gene were not identified, neither in the German nor in the Norwegian cohort.
Conclusion
Sequence variation in the PINK1 gene appears to play a marginal quantitative role in the pathogenesis of the late-onset form of PD, in German and Norwegian cohorts, if at all.
Similar content being viewed by others


Background
PD is the second most common neurodegenerative disorder after Alzheimer disease affecting more than 1% of the population by the age of 65 years. Mutations in the alpha-synuclein (PARK1), Parkin (PARK2) and DJ-1 (PARK7) gene cause fairly rare familial forms of PD characterized by an early age of onset. Mutations in the recently identified LRRK2 (PARK8) gene, especially the common mutation G2019S, occur more frequently in patients suffering from early as well as late-onset PD [1, 2]. Recently, mutations in the PINK1 (PARK6) gene were shown to cause autosomal recessively transmitted early-onset parkinsonism [3, 4]. The PINK1 (PTEN-induced kinase 1) gene encodes a putative protein kinase. The protein is targeted to mitochondria and shows a serine-threonine kinase domain with homology to kinases of the Ca2+/calmodulin family[3]. It appears to exert protective effects against cellular stress within mitochondria[3]. These findings link mitochondria directly to the pathogenesis of PD [3, 5]. An additional link between mitochondrial dysfunction and PD is obvious via the identification of disease causing mutations in the Omi/HtrA2 gene [6]. The hypothesis of mitochondrial impairment was further emphasized by postmortem studies of PD brains [7] and observation of PD syndromes after intoxication with mitochondrial complex I inhibitors, such as MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine) and rotenone [8]. Mutations in the PINK1 gene are the second most common cause of autosomal-recessively inherited early-onset PD after mutations in the Parkin gene. On the other hand, strong evidence was reported for a possible role of Parkin gene variations in the late-onset form of PD (age of onset >45 years): Parkin mutations appear to contribute to the common late-onset form and mutations, especially in exon 7 in heterozygous state, may play a role as susceptibility alleles for sporadic PD[9, 10]. The question arises as to whether the PINK1 gene is also a candidate gene for late-onset forms of Parkinson's disease, similar to the suggested role of the Parkin gene.
Here we report of a population-based analysis of sequence variations within the PINK1 gene. The German cohort includes 85 patients suffering from late-onset form of PD and represents a modern urban population with a genetic heterogeneity. In contrast, the Norwegian cohort represents a more homogeneous population [11] and includes 90 patients suffering from late-onset form of PD.
Results
All 8 coding exons of the PINK1 gene were screened for sequence variation using SSCP and sequencing analyses. Several SNPs were identified in our cohorts (L63L, Q115L, Ivs4-5A>G het, Ivs6+43C>T het, N521T, c.1783A>T). Allelic frequencies of several SNPs differed significantly between the two European cohorts confirming homogeneity of the Norwegian cohort (Table 1). Patients and controls were genotyped for the recently identified variation Q115L [12] using DHPLC analysis (Table 2). The observed frequencies did not differ significantly between patients and controls, neither in the German (p = 0.27) nor in the Norwegian cohort (p = 0.8). This screening did not reveal any disease-relevant mutation in our cohorts.
Discussion
As recently shown, mutations in the PINK1 gene rarely cause autosomal-recessively transmitted PD [3]. Besides an early age of onset, the observed clinical symptoms in PD caused by PINK1 are similar to symptoms in idiopathic PD.
In this population-based study, we investigated whether sequence variations in the PINK1 gene play a role in the late-onset form of PD. A recently described variation (Q115L) of the PINK1 gene [12] was identified in the German and the Norwegian cohorts. We calculated allele frequencies in cases and controls and show here that the Q115L variant was not associated with late-onset PD in our study. These findings correspond to previously published data of no leading association of other coding SNPs within the PINK1 gene and PD [13]. In addition, several common SNPs were identified. We did not find any pathogenic mutation of the PINK1 in our cohorts composed of patients suffering from late-onset form of PD. The risk to miss potential mutations was minimized by a well established and optimized SSCP analyses.
The most likely reason to explain the absence of mutations in our cohorts is the lack of influence of the PINK1 gene in the pathogenesis of late-onset PD. Individual tagging SNPs and tag-defined haplotypes in 500 PD patients likewise did not reveal associations with PD [14]. Future investigations should include screening of potential promoter as well as enhancer/silencer regions of the gene to finally exclude any lack of influence of PINK1 variation on PD manifestation. Yet, functional investigations of the PINK1 protein are necessary to identify potential interaction partners as candidates for additional mutation screening.
Conclusion
Investigations of other genes involved in the mitochondrial pathway of the PINK1 gene are necessary to evaluate the exact role of mitochondrial impairment for common forms of PD.
Materials and methods
Patients and controls
The Norwegian cohort (n = 90) consists of patients suffering from late-onset PD (median age of onset 64.4 years, range from 49 to 78 years, standard deviation 7.9) originated from the Stavanger area of Western Norway. This population is known to be genetically quite homogeneous [11] and has previously been described in several clinical PD studies [15, 16]. 16.7% of the patients presented a positive family history for PD concerning first degree relatives (siblings or parents). All patients meet the criteria for PD [15, 17] and were thoroughly clinically examined. An ethnically matched control group of healthy blood donors was recruited in Bergen, Norway. The German cohort (n = 85) consists of patients of the Ruhr area suffering from late-onset PD (median age of onset 58.7 years, range from 45 to 79 years, standard deviation 8.7) diagnosed according to the UK Brain Bank criteria [18]. 16.5% of the patients presented a positive family history for PD concerning first degree relatives (siblings or parents). Ethnically matched control samples from senior healthy blood donors (median age 57.2 years, range from 42 to 68 years, standard deviation 5.7) were recruited at the neighbouring University Hospital of Essen (Germany). Population stratification was excluded for the controls by multiple microsatellites analyses. After receiving informed consent from the patients, peripheral blood samples were taken and genomic DNA was extracted following standard protocols. German (Bochum and Düsseldorf) and Norwegian (Bergen) ethics committees approved this study.
SSCP, DHPLC, sequencing
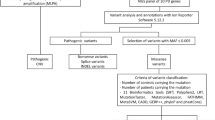
The 8 coding exons of the PINK1 gene were amplified by polymerase chain reaction (PCR) in all patients using designed primer pairs adapted to the SSCP technique (Table 3). SSCP analysis according to standard procedure [19] was used to identify mutations and SNPs. In order to optimize mutation screening by SSCP analyses, PCR products were digested with different restriction enzymes depending on the lengths of their fragments [19] and screened in two different conditions. Selected samples with band shifts evidenced in SSCP analyses were confirmed by direct sequencing. The sequence reactions were run on an automated DNA sequencer (Applied Biosystems 377 XL, Foster City, USA) and analyzed with the ABI Prism™ 377 XL collection and convenient sequencing analysis software. SNP frequencies of the Q115L variation in patients and controls were determinated by using DHPLC analyses (WAVE® system, Cheshire, UK, using software Wavemaker 4.1) according to established procedures.
Statistical analyses
SNP frequencies were compared by the χ2 test. We considered P-values < 0.05 as significant.
References
Gilks WP, Abou-Sleiman PM, Gandhi S, Jain S, Singleton A, Lees AJ, Shaw K, Bhatia KP, Bonifati V, Quinn NP, Lynch J, Healy DG, Holton JL, Revesz T, Wood NW: A common LRRK2 mutation in idiopathic Parkinson's disease. Lancet. 2005, 365: 415-416.
Di Fonzo A, Rohe CF, Ferreira J, Chien HF, Vacca L, Stocchi F, Guedes L, Fabrizio E, Manfredi M, Vanacore N, Goldwurm S, Breedveld G, Sampaio C, Meco G, Barbosa E, Oostra BA, Bonifati V: A frequent LRRK2 gene mutation associated with autosomal dominant Parkinson's disease. Lancet. 2005, 365: 412-415.
Valente EM, Abou-Sleiman PM, Caputo V, Muqit MM, Harvey K, Gispert S, Ali Z, Del Turco D, Bentivoglio AR, Healy DG, Albanese A, Nussbaum R, Gonzalez-Maldonado R, Deller T, Salvi S, Cortelli P, Gilks WP, Latchman DS, Harvey RJ, Dallapiccola B, Auburger G, Wood NW: Hereditary early-onset Parkinson's disease caused by mutations in PINK1. Science. 2004, 304: 1158-1160. 10.1126/science.1096284.
Rogaeva E, Johnson J, Lang AE, Gulick C, Gwinn-Hardy K, Kawarai T, Sato C, Morgan A, Werner J, Nussbaum R, Petit A, Okun MS, McInerney A, Mandel R, Groen JL, Fernandez HH, Postuma R, Foote KD, Salehi-Rad S, Liang Y, Reimsnider S, Tandon A, Hardy J, St George-Hyslop P, Singleton AB: Analysis of the PINK1 gene in a large cohort of cases with Parkinson disease. Arch Neurol. 2004, 61: 1898-1904. 10.1001/archneur.61.12.1898.
Shen J, Cookson MR: Mitochondria and dopamine: new insights into recessive parkinsonism. Neuron. 2004, 43: 301-304. 10.1016/j.neuron.2004.07.012.
Strauss KM, Martins LM, Plun-Favreau H, Marx FP, Kautzmann S, Berg D, Gasser T, Wszolek Z, Muller T, Bornemann A, Wolburg H, Downward J, Riess O, Schulz JB, Kruger R: Loss of function mutations in the gene encoding Omi/HtrA2 in Parkinson's disease. Hum Mol Genet. 2005
Beal MF: Mitochondria, oxidative damage, and inflammation in Parkinson's disease. Ann N Y Acad Sci. 2003, 991: 120-131.
Dauer W, Przedborski S: Parkinson's disease: mechanisms and models. Neuron. 2003, 39: 889-909. 10.1016/S0896-6273(03)00568-3.
Foroud T, Uniacke SK, Liu L, Pankratz N, Rudolph A, Halter C, Shults C, Marder K, Conneally PM, Nichols WC, Parkinson Study G: Heterozygosity for a mutation in the parkin gene leads to later onset Parkinson disease. Neurology. 2003, 60: 796-801.
Oliveira SA, Scott WK, Martin ER, Nance MA, Watts RL, Hubble JP, Koller WC, Pahwa R, Stern MB, Hiner BC, Ondo WG, Allen FHJ, Scott BL, Goetz CG, Small GW, Mastaglia F, Stajich JM, Zhang F, Booze MW, Winn MP, Middleton LT, Haines JL, Pericak-Vance MA, Vance JM: Parkin mutations and susceptibility alleles in late-onset Parkinson's disease.[see comment]. Annals of Neurology. 2003, 53: 624-629. 10.1002/ana.10524.
Borg A DAHKMLHEMP: BRCA1 1675delA and 1135insA account for one third of Norwegian familial breast-ovarian cancer and are associated with later disease onset than less frequent mutations. Dis Markers. 1999, Oct;15(1-3):79-84.:
Klein C, Djarmati A, Hedrich K, Schafer N, Scaglione C, Marchese R, Kock N, Schule B, Hiller A, Lohnau T, Winkler S, Wiegers K, Hering R, Bauer P, Riess O, Abbruzzese G, Martinelli P, Pramstaller PP: PINK1, Parkin, and DJ-1 mutations in Italian patients with early-onset parkinsonism. Eur J Hum Genet. 2005
Groen JL, Kawarai T, Toulina A, Rivoiro C, Salehi-Rad S, Sato C, Morgan A, Liang Y, Postuma RB, St George-Hyslop P, Lang AE, Rogaeva E: Genetic association study of PINK1 coding polymorphisms in Parkinson's disease. Neurosci Lett. 2004, 372: 226-229. 10.1016/j.neulet.2004.09.043.
Healy DG, Abou-Sleiman PM, Ahmadi KR, Muqit MM, Bhatia KP, Quinn NP, Lees AJ, Latchmann DS, Goldstein DB, Wood NW: The gene responsible for PARK6 Parkinson's disease, PINK1, does not influence common forms of parkinsonism. Ann Neurol. 2004, 56: 329-335. 10.1002/ana.20206.
Kurz M, Alves G, Aarsland D, Larsen JP: Familial Parkinson's disease: a community-based study. European Journal of Neurology. 2003, 10: 159-163. 10.1046/j.1468-1331.2003.00532.x.
Tandberg E, Larsen JP, Nessler EG, Riise T, Aarli JA: The epidemiology of Parkinson's disease in the county of Rogaland, Norway. Movement Disorders. 1995, 10: 541-549. 10.1002/mds.870100503.
Larsen JP, Dupont E, Tandberg E: Clinical diagnosis of Parkinson's disease. Proposal of diagnostic subgroups classified at different levels of confidence. Acta Neurologica Scandinavica. 1994, 89: 242-251.
Hughes AJ, Daniel SE, Kilford L, Lees AJ: Accuracy of clinical diagnosis of idiopathic Parkinson's disease: a clinico-pathological study of 100 cases. J Neurol Neurosurg Psychiatry. 1992, 55: 181-184.
Jaeckel S, Epplen JT, Kauth M, Miterski B, Tschentscher F, Epplen C: Polymerase chain reaction-single strand conformation polymorphism or how to detect reliably and efficiently each sequence variation in many samples and many genes. Electrophoresis. 1998, 19: 3055-3061. 10.1002/elps.1150191802.
Acknowledgements
We sincerely thank all the participants in this study. We also thank Dr. O.-B. Tysnes (Department of Neurology, Haukeland University Hospital, Bergen, Norway) for providing control samples. AMS gratefully acknowledges an Alma and Heinrich Vogelsang Foundation fellowship.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors' contributions
AMS carried out the molecular genetic studies, performed the statistical analysis and drafted the manuscript. MK participated in devising the study based on thoroughly clinical analysis of the patients. JPL supervised data collection and diagnosis of the Norwegian cohort. DW and TM provided the samples and performed clinical diagnostics of the German patient group. JTE conceived of the study, and participated in its design and coordination and helped to draft the manuscript. GD supervised AMS, especially the molecular studies. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Schlitter, A.M., Kurz, M., Larsen, J.P. et al. Exclusion of PINK1 as candidate gene for the late-onset form of Parkinson's disease in two European populations. J Negat Results BioMed 4, 10 (2005). https://doi.org/10.1186/1477-5751-4-10
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1477-5751-4-10