
Abstract
Recent advances in molecular biology have made possible the identification of genetic defects responsible for Wilson's disease, Indian childhood cirrhosis and copper toxicosis in Long Evans Cinnamon rats, toxic milk mice, and Bedlington terriers. The Wilson's disease gene is localized on human chromosome 13 and codes for ATP7B, a copper transporting P-type ATPase. A genetic defect similar to that of Wilson's disease occurs in Long Evans Cinnamon rats and toxic milk mice. Familial copper storage disorders in Bedlington and West Highland white terriers are associated with early subclinical disease, and copper accumulation with subsequent liver injury culminating in cirrhosis. The canine copper toxicosis locus in Bedlington terriers has been mapped to canine chromosome region CFA 10q26. Recently, a mutated MURR1 gene was discovered in Bedlington terriers affected with the disease. Idiopathic childhood cirrhosis is biochemically similar to copper toxicosis in Bedlington terriers, but clinically much more severe. Both conditions are characterized by the absence of neurologic damage and Kayser-Fleisher rings, and normal ceruloplasmin levels. A recent study added North Ronaldsay sheep to the list of promising animal models to study Indian childhood cirrhosis. Morphologic similarities between the two conditions include periportal to panlobular copper retention and liver changes varying from active hepatitis to panlobular pericellular fibrosis, and cirrhosis. Certain copper-associated disorders, such as chronic active hepatitis in Doberman pinschers and Skye terrier hepatitis are characterized by copper retention secondary to the underlying disease, thus resembling primary biliary cirrhosis in humans. Copper-associated liver disease has increasingly being recognized in Dalmatians. Copper-associated liver diseases in Dalmatians and Long Evans Cinnamom rats share many morphologic features. Fulminant hepatic failure in Dalmatians is characterized by high serum activities of alanine aminotransferase and aspartate aminotransferase, and severe necrosis of centrilobular areas (periacinar, zone 3) hepatocytes. Macrophages and surviving hepatocytes contain copper-positive material. Liver disease associated with periacinar copper accumulation has also been described in Siamese cats. Many questions regarding copper metabolism in mammals, genetic background, pathogenesis and treatment of copper-associated liver diseases remain to be answered. This review describes the similarities between the clinico-pathological features of spontaneous copper-associated diseases in humans and domestic animals.
Similar content being viewed by others


Introduction
Copper-associated diseases are increasingly being reported in both man and animals [1–6]. Wilson's disease is an autosomal recessive disorder that results from pathological accumulation of copper predominantly in the liver and brain [1]. Copper also has a role in fatal, non-Wilson's liver diseases affecting young children with a genetic abnormality of copper metabolism [3, 7]. Excess accumulation of copper also occurs as a consequence of chronic liver diseases such as primary biliary cirrhosis, and chronic hepatitis in both humans [8] and animals [9]. A genetic defect similar to that of Wilson's disease has been discovered in the Long Evans Cinnamon (LEC) rat [10], and the toxic milk mouse [11]. Animal models play an important role in the study of copper homeostasis, mechanisms (pathogenesis) of copper-associated liver diseases, and in the implementation of new therapeutic approaches such as gene therapy [12].
Copper homeostasis in mammals
The proximal small intestine is recognized as the main site of dietary copper absorption in mammals [13]. Transport from the intestinal lumen into intestinal mucosa is a carrier-mediated process involving a saturable transport component [14]. The overall intestinal copper uptake is influenced by amino acids, ascorbic acid, and other dietary factors [14]. Once in mucosal cells, approximately 80% of the newly absorbed copper is in the cytosol, mainly bound to metallothioneins (MT). These are low-molecular weight inducible proteins with many functions including homeostasis, storage, transport and detoxification of metals [15, 16]. Metallothioneins bind to many metals, but in normal circumstances only Zn, Cu and Cd binding is significant [17]. After passage through the enterocytes, copper enters the portal circulation where it is bound to carrier proteins (primarily albumin), peptides and amino acids and is transported to the liver [18], with lesser amounts entering the kidney [17].
Copper transport in hepatocytes can be divided into three discernible but interrelated steps: copper uptake, intracellular copper distribution and utilization, and copper export. At the hepatocellular cellular level copper uptake is likely mediated by hCtr1, a copper transporter [19]. Uptake of copper is competitively inhibited by divalent metal ions such as cadmium, manganese, zinc, and cobalt [17]. Once within the hepatocyte, cytoplasmic copper chaperones (hCOX17, HAH1/Atox1, hCCS) distribute the metal to specific cellular compartments for its incorporation into copper-requiring proteins. HAH1/Atox1 [20] may function to bind copper and supply it to the Wilson's disease protein (ATP7B) in the trans-Golgi network. The ATP7B gene encodes the Wilson's disease p-type ATPase [21]. The ATP7B protein is required for incorporation of copper into ceruloplasmin in the liver and for biliary excretion of copper [22–24]. ATP7B may also be involved in the transport of copper to a vesicular compartment [25]. Copper from these vesicles may be delivered to lysosomes [26]. Within hepatocytes, free copper would likely be toxic to cells. However, it appears that copper is complexed by reduced glutathione (GSH) soon after the metal enters the cell [27]. The importance of GSH in metal detoxification is supported by its role in the removal of toxic oxygen species [28]. Following entry to the hepatocyte, in addition to GSH copper interacts with MT, and ceruloplasmin [17]. The copper chaperone for MT has not been identified [27]. Copper is secreted into plasma as a complex with ceruloplasmin [29, 30]. This complex accounts for 90% to 95% of plasma copper [31]. In most mammals, copper is excreted easily, and the main route of excretion of copper is the bile [13, 32]. Urinary copper excretion is minimal under normal conditions since most of the copper in circulating blood is bound to ceruloplasmin or confined within the erythrocytes and very little copper crosses the glomerular capillaries [14, 33]. The process of hepatobiliary copper secretion is still poorly understood. Two independent pathways have been identified for the elimination of copper from hepatocytes into bile [34]. The first appears to be a vesicular pathway that involves the delivery of lysosomal contents, including copper into bile [32]. Reduction of copper excretion by microtubular disruption from colchicine administration supports the notion of a vesicular pathway [34]. A second pathway may involve canalicular membrane transport of copper-glutathione, and it functions when copper loads beyond physiological levels are presented to liver cells [34]. Copper transport into bile correlates well with the biliary excretion of glutathione [28], and the canalicular multispecific organic anion transporter (cMOAT) may contribute to biliary copper excretion [26], but the mechanism of normal biliary copper excretion is poorly understood.
Disruption of the normal copper homeostasis or accumulation of copper in excess of metabolic requirements can lead to copper toxicity. Copper toxicosis can be classified as primary when it results from an inherited metabolic defect, and as secondary when it is the consequence of an abnormally high intake, increased absorption, or reduced excretion of copper due to underlying pathologic processes.
Spontaneous Copper toxicosis in humans and animals
Familial copper storage disorders occur in Wilson disease in humans [35], LEC rats [36], toxic milk mouse [11, 37], Bedlington terriers [38, 39], and in West Highland White Terrier dogs [40]. Excess copper can accumulate within the liver as a consequence of chronic cholestatic liver diseases [8], particularly in diseases such as primary biliary cirrhosis [8, 41], and chronic hepatitis [42]. Similar conditions occur in certain breeds of dogs [5, 9, 43, 44].
Wilson's disease
Wilson's disease is an autosomal recessive inherited disorder of copper metabolism [35, 45, 46]. Wilson's disease results in copper accumulation in the liver, cornea and brain [1]. The worldwide incidence of Wilson's disease, independent of ethnic and geographic origin, is approximately 1 in 30,000 [47]. However, it has been noted that the disease may be more common than previously expected, because most incidence estimations are based on adolescent or adults presenting with neurologic symptoms, which occur only in about half of the patients [48]. The Wilson's disease gene is localized on human chromosome 13 and codes for ATP7B, a copper transporting P-type ATPase [21]. The Wilson's disease mutations occur throughout the whole gene and include missense and nonsense mutations, deletions and insertions [49]. Most of the more than 80 mutations are present at a low frequency, and mutations differ between ethnic groups [50]. Thus, diagnosis of Wilson's disease is challenging and requires a battery of tests, including morphologic evaluation and copper analysis of liver tissue [51, 52]. Liver disease may mimic various forms of common liver conditions, ranging from fulminant hepatic failure, chronic hepatitis, and cirrhosis [1].
Animal models of Wilson's disease
The LEC rat [36] and the toxic milk mouse are the only known valid animal models of Wilson's disease [11, 37].
Animal models of Wilson's disease – LEC rat
The LEC rat with a hooded dilute agouti coat is a mutant inbred strain, which was established from a closed colony of randomly bred Long-Evans rats [36]. Long Evans Cinnamon rats suffer from fulminant hepatitis and severe jaundice at about 4 months of age and show similarities to Wilson's disease in many clinical and biochemical features [10, 36]. This mutant has a deletion in the copper transporting ATPase gene (Atp7b) homologous to the human Wilson's disease gene (ATP7B) [10, 53], and the mode of inheritance of hepatitis is also autosomal recessive [54].
Similar to the condition in Wilson's disease, LEC rats manifest elevated hepatic copper levels, defective incorporation of copper into ceruloplasmin, and reduced biliary excretion of copper [55]. LEC rats develop intravascular haemolysis secondary to the release of large amounts of non-ceruloplasmin copper into the bloodstream [56], as it has been described in patients with Wilson's disease [14].
The hepatic copper concentration can rise to 2,126 ppm dry weight [57]. It is also known that LEC rats may accumulate as much iron as copper in the liver as a result of hemolysis [56]. This mutant strain also possesses reduced hepatic selenium [58]. Both accumulation of iron and depletion of selenium in the liver may contribute to the development of fulminant hepatitis, hepatic fibrosis, and subsequent hepatocarcinogenesis in LEC rats by increasing the process of oxidative damage with copper, and a reduction in the antioxidant capacity against copper-induced free-radical damage [56, 58].
It has been suggested that an immune-mediated mechanism may play a role in the development of acute lethal hepatitis in LEC rats. Autoimmune antibodies to liver microsomal proteins have been demonstrated 3–7 weeks before death in these rats [59]. Protein disulfide isomerase and calreticulin have been identified as antigens in liver microsomes of this mutant [60], and treatment with immunosuppressant drugs such as cyclosporin-A reduced the mortality in LEC rats [61]. However, a recent study showed that the development of antimicrosomal antibodies does not precede the development of severe liver damage in the LEC rat model [62].
The clinical signs of hepatitis include severe jaundice, a bleeding tendency, oliguria, lethargy, and loss of body weight. During this period, activities of serum enzymes, lactate dehydrogenase (LDH), alanine aminotransferase (ALT) [63], aspartate aminotransferase (AST), and γ-glutamyltransferase (GGT), as well as bilirubin levels, are increased significantly [36, 54, 62]. While the serum levels of ceruloplasmin remain reduced all the time [60], the copper concentration in serum increases mainly after the onset of jaundice [63]. About half of the animals die within a week of the onset of jaundice [36].
Histological changes of acute hepatitis in LEC rats occur prior to 8 weeks of age, and the most drastic changes occur from 17 to 20 weeks of age [36]. A recent study utilizing female LEC rats reports biochemical and morphological evidence of severe liver damage at 12 weeks of age [62]. Histological changes are characterized by hepatocellular karyomegaly, large numbers of Councilman bodies, submassive necrosis [54], mitosis of hepatocytes [36], and apoptosis [56]. After this stage, surviving rats develop chronic hepatitis, cholangiofibrosis, preneoplastic foci and nodules, and hepatocellular carcinomas [46, 54, 56]. Histochemical examination of LEC rat liver for copper reveals that copper accumulates preferentially in hepatocytes and distributes diffusely throughout the cytoplasm. Copper accumulates in virtually all hepatocytes throughout the entire liver lobule, but shows a tendency to localize in the periportal areas [64]. LEC rats that survive the stage of fulminant hepatitis develop cirrhosis [65], and are highly susceptible to the development of hepatocellular carcinoma [64]. This is an interesting feature of this particular animal model because hepatocellular carcinoma is rarely diagnosed in Wilson's disease patients [66].
Animal models of Wilson's disease – Toxic milk mice
Toxic milk is an autosomal recessive mutation which alters copper homeostasis in mice [37]. Offspring of mutant females are born copper-deficient and since their mother's milk is also low in copper, babies die at 2 weeks of age. The progeny of affected dams fostered to lactating normal females survive but with age copper accumulate in their livers [67]. By 6 months of age, liver changes are characterized by nodular fibrosis, bile duct hyperplasia and portal lymphocytic inflammatory cell infiltration [67]. Toxic milk mice share some biochemical abnormalities with Wilson's disease for example concentration of serum copper and ceruloplasmin are decreased. The genetic defect in toxic milk mice is similar to that of Wilson's disease [11]. Although gross and histologic changes in the liver in both rodent models (i.e. LEC rat and toxic milk mice) resemble Wilson's disease [67], same differences have been noted. Neither of the rodent models has neurologic symptoms, and in the toxic milk mice model affected dams produce Cu-deficient milk, whereas there are no reports of Cu-deficient milk in humans mothers with Wilson's disease [68].
Indian childhood cirrhosis
Indian childhood cirrhosis and its analogues endemic Tyrolean infantile cirrhosis, and idiopathic copper toxicosis, are fatal liver diseases seen in young children due to genetic susceptibility to minimal excess in dietary copper [2–4, 7]. The gene for Indian childhood cirrhosis diagnosed in North America has recently been identified [69].
North Ronaldsay sheep
This primitive breed has adapted to copper impoverished environment and display an abnormal sensitivity to copper toxicity when transferred to copper adequate location [70]. A recent study reports the remarkable similarities between the condition in North Ronaldsay sheep and Indian childhood cirrhosis, whereby affected sheep exhibited liver changes varying from active hepatitis to panlobular pericellular fibrosis, and cirrhosis. Histochemical stains demonstrated periportal to panlobular histochemical copper retention [6].
Primary biliary cirrhosis
Primary biliary cirrhosis is a chronic progressive, often fatal liver disease, characterized by the eventual development of cirrhosis and liver failure [31, 41]. Middle-aged females are predisposed to the condition [71]. The immunological abnormalities and morphologic features observed in primary biliary cirrhosis, favour the hypothesis of an immune-mediated mechanism [72, 73]. However, the nature of the initiating factor(s) and of the sensitizing antigen is unknown. The only effective treatment for this disease is liver transplantation [74]. Indeed, primary biliary cirrhosis is one of the five most frequent causes of liver transplantation [75]. Although copper accumulation is a secondary event [76], therapeutic approaches have included attempts to remove excess hepatic copper in order to avoid possible synergism between the initiating factor(s) and release of copper into the liver [77].
Animal models of primary biliary cirrhosis
Certain disorders, such as chronic active hepatitis in Doberman pinschers and Skye terrier hepatitis are characterized by copper retention secondary to the underlying disease, thus resembling primary biliary cirrhosis in humans [44]. Copper values are never so elevated as in the familial storage diseases.
Animal models of primary biliary cirrhosis – Chronic hepatitis in Doberman Pinschers
Doberman hepatitis is a disorder associated with histologic features of chronic active hepatitis, cholestasis, and cirrhosis. Middle aged, spayed female dogs are predisposed to the disease [9, 43, 78]. The cause of the disease remains undetermined, but histopathological changes support the idea of immune-mediated disorder [79]. Copper accumulates in centroacinar (portal) areas [9, 80]. The present knowledge on the role of copper in this disorder is incomplete; however, the presence of copper in liver biopsies constitutes one of the essential diagnostic criteria for subclinical Doberman hepatitis [80].
Animal models of primary biliary cirrhosis – Skye terrier hepatitis
This condition appears to be an unusual lesion characterized by intracanalicular cholestasis, with copper accumulation and hepatocellular degeneration culminating in cirrhosis [44]. Copper accumulation occurs primarily in the periacinar area, which is inconsistent with other disorders associated with cholestasis and subsequent tissue copper retention [81]. The cause is unknown, but an inheritable metabolic defect involving membrane transfer and transport systems in the periacinar zone, resulting in disturbed bile secretion and excessive copper accumulation have been suggested [44].
Animal models of primary biliary cirrhosis – Feline cholangiohepatitis complex
This condition has three well-characterized histopathologic lesions, but the etiology and pathogenesis of the condition is poorly understood [82]. The non-suppurative type has been compared to primary biliary cirrhosis in humans [83, 84]. Non-suppurative cholangitis in cats is characterized by lymphocytic and plasmacytic portal infiltration, bile duct hyperplasia, and portal fibrosis. Histochemical stains demonstrate copper positive granules within portal hepatocytes (ICF personal observation). The value of this model in the study of primary biliary cirrhosis has not been thoroughly assessed.
Other copper associated disease in dogs
In general, naturally occurring canine genetic diseases resemble human diseases more faithfully than their rodent counterpart, as there is a higher degree of DNA sequence identity between humans and dogs than between humans and rodents [85]. Familial copper storage disorders in Bedlington and West Highland white terriers are usually associated with early subclinical disease during which copper accumulates with subsequent liver injury culminating in cirrhosis [40, 86]. Occasionally however, there may be a copper-induced hemolytic crisis in Bedlington terriers [86, 87]. Bedlington Terrier copper toxicosis has generated much interest as a possible animal model for Wilson's disease. However, it has been proven that Wilson's disease and Bedlington Terrier copper toxicosis do not share the same genetic defect [88]. The canine copper toxicosis locus in Bedlington terriers has been mapped to canine chromosome region CFA 10q26 [88] and in addition to ATPB, ATOX 1 [89, 90], ATP6H [91] have been excluded as candidate genes underlying copper toxicosis in Bedlington terriers [89, 90]. Recently, a mutated MURR1 gene was discovered in Bedlington terriers affected with the disease [85].
Some similarities have been noted between Bedlington terriers and idiopathic childhood cirrhosis. Idiopathic childhood cirrhosis is biochemically similar to copper toxicosis in Bedlington terriers [85], but clinically much more severe [7]. Both conditions are characterized by the absence of neurologic damage and Kayser-Fleisher rings [92, 93], and normal ceruloplasmin levels [47].
Liver copper values can be as high as 12,000 ppm dry weight in Bedlington terriers [94] whereas the highest copper value recorded in West Highland white terriers is 6,800 ppm dry weight [95]. In Bedlington terriers older than 1 year of age, there is a progressive increase in the accumulation of tissue copper until 8 years of age [81]. There is no relationship between age, histomorphological changes and hepatic copper concentration in West Highland white terriers. The clinical signs vary widely, depending on the stage of the disease. Affected animals in the early stages usually are asymptomatic. Depression, anorexia, lethargy, vomiting, and increased ALT are usually associated with an acute onset of hepatic necrosis. Microscopically, there is a spectrum of recognizable changes. In the least affected or subclinical cases, accumulation of intracytoplasmic refractile, light-brown granules in vacuolated parenchymal cells of the periacinar zones are observed which stain histochemically positive for copper. This is followed by the development of foci of hepatocellular degeneration and necrosis with scattered inflammatory response of neutrophils, lymphocytes and plasma cells. Fine fibrous septa extend from the portal areas into the lobules. More advanced stages are characterized by periportal infiltrates of inflammatory cells and prominent piecemeal necrosis (resembling chronic active hepatitis). Piecemeal necrosis has not been described in West Highland white terriers toxicosis. Finally, there is a complete architectural disorganization of the liver with variable sized nodules of hepatocytes (with focal degeneration and aggregates of neutrophils) separated by bands of fibrous connective tissue with portal-central bridging [94, 96]. Contrary to Wilson's disease, hepatocytes with Mallory bodies have not been identified [97].
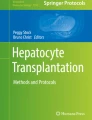
Copper-associated liver disease has increasingly being recognized in Dalmatians [98, 99] (Figs. 1,2). Fulminant hepatic failure characterized by high serum activities of ALT and AST. Histologically, there is severe necrosis of hepatocytes involving the centrilobular areas. Macrophages and surviving hepatocytes contain copper-positive material [98]. Primary copper storage disease was suspected on the basis of histologic findings and high copper concentration in the liver [99]. Morphologic changes observed in Dalmatians are strikingly similar to those observed in LEC rats (ICF personal observation) suggesting that copper toxicosis in Dalmatians is a promising spontaneous animal model of Wilson's disease.

Dalmatian dog liver. Dissecting hepatitis with marked mononuclear inflammation. P = portal. HE stain. Bar = 50 μm.

Dalmatian dog liver. Prominent copper-positive granules. P = Portal. Rhodanine stain. Bar = 50 μm.
Excess copper accumulation occurs as a consequence of chronic liver disease in other canine breeds dogs [5, 9, 43, 44], particularly Cocker Spaniels and Poodles [9]. Similarly, secondary copper accumulation has been described in chronic hepatitis in humans [42].
Spontaneous copper-associated liver disease in other mammalian species
Sheep are particularly susceptible to copper poisoning [100, 101]. The condition occurs when sheep are accidentally fed rations prepared for other species (i.e. bovine or swine) [100, 102]. Copper poisoning in sheep is commonly diagnosed. In contrast, copper toxicosis in other farm animals is rarely reported [103].
Spontaneous copper-associated liver disease in other mammalian species – Copper toxicosis in sheep
Chronic copper poisoning in sheep results from the accumulation of copper in hepatic tissue over a period of a few weeks to more than a year [100, 101], and is considered to have two distinct phases [104]. During the accumulation or pre-hemolytic phase, animals may be clinically normal, even with liver copper concentrations of 1,000 ppm, so long as increasing mitotic rate produces enough new hepatocytes to take up the copper released by dying cells [94]. However, liver damage does occur during this period as indicated by increased levels of lactic dehydrogenase and AST [100]. The second phase, or hemolytic crisis, lasts from hours to days and is characterized by the sudden onset of severe intravascular hemolysis and hemoglobinemia associated with increased blood copper levels, with resulting liver [104, 105], kidney, and brain damage [106].
During the hemolytic phase, elevated serum values of AST, GGT, ALP, copper, urea nitrogen (BUN), bilirubin [100, 107], and ceruloplasmin [108] have been observed. Elevation of blood copper occurs prior to and during the hemolysis; the ceruloplasmin levels tend to fluctuate but in most instances there is a two-fold or more increase immediately before and during the hemolytic crisis [108]. The histologic changes are present in the liver in the preclinical stages and can be somewhat obscured by the periacinar (centrilobular) necrosis of hypoxemia and the bile accumulations of hemolytic disease [94]. Copper can be demonstrated histochemically with rubeanic acid or rhodanine as fine granules within the cytoplasm of parenchymal and Kupffer cells [104, 108]. Copper in hepatocytes is mostly located within lysosomes [109]. It has been demonstrated that copper deposition begins in the periacinar areas extending to the mid and periportal zones with progressive copper-loading [109].
Spontaneous copper-associated liver disease in other mammalian species – Copper-associated liver disease in cats
Liver disease associated with centrilobular (periacinar, zone 3) copper accumulation was described in a Siamese cat [110]. One of the authors (ICF) has examined cases of copper-associated liver disease in cats, with morphologic characteristics similar to those reported in Siamese cats (Figs. 3,4), suggesting that metabolic defects of copper metabolism occur with relative frequency in the feline specie and may have been overlooked in the past.

Liver from a cat with severe hepatic lipidosis. Diffuse severe hepatocellular vacuolation. P = Portal. HE stain. Bar = 50 μm.

Liver from a cat with severe hepatic lipidosis. Prominent copper-positive granules. P = Portal. Rhodanine stain. Bar = 50 μm.
Spontaneous copper-associated liver disease in other mammalian species – Copper-associated liver disease in ferrets
Two cases have been described in ferrets [111]. One case was characterized by chronic hepatopathy, with diffuse hepatocellular vacuolation, and the second case had centrilobular degeneration and necrosis. In both ferrets, liver copper concentration was markedly elevated and special staining revealed copper pigment in hepatocytes and macrophages. An inherited defect of copper metabolism was suspected in these ferrets based on the lack of related illness in 11 other ferrets housed in the same environment and receiving the same diet.
Treatment of Cu-associated disease in animal models
D-penicillamine has been effective in the treatment of Bedlington Terrier toxicosis [81]. However, copper is only slowly removed from the liver and clinical improvement generally requires years of treatment [112]. Side effects seen with D-penicillamine therapy in humans include fever, anorexia, pyridoxine deficiency, leukopenia, thrombocytopenia [113, 114], rashes and proteinuria [47]. In dogs, treatment with D-penicillamine often is associated with anorexia, nausea and vomiting [92, 112, 115].
Alternate agents such as trientine [116], tetrathiomolybdate (TTM) [117, 118], and zinc [119, 120] have been employed in the treatment of Wilson's disease. Zinc [121] have been used for the treatment of copper toxicosis in sheep and dogs [119]. In sheep, ammonium tetrathiomolybdate lowers liver concentrations and prevents the development of hemolysis, however, the kidneys accumulate large amounts of copper [122, 123]. It also appears that TTM is not fully excreted after treatment but molybdenum is widely distributed and retained in many organs including brain and pituitary [124].
Conclusions
Recent advances in molecular biology have made possible the identification of genetic defects responsible for Wilson's disease, Indian childhood cirrhosis, and copper toxicosis in LEC rats, toxic milk mice, and Bedlington terriers. However, many questions regarding copper metabolism in mammals, and pathogenesis and treatment of copper-associated liver diseases remain to be answered. Studies designed to identify genetic defects of copper metabolism and to implement new therapeutic approaches to cure these conditions will greatly contribute to the knowledge of the pathogenesis of copper-associated diseases. This review demonstrates that there are numerous spontaneous animal models of copper-associated liver diseases. Based on the clinical presentation and morphological features, copper-associated liver disease in Dalmatians dogs has the potential to be a good model of Wilson's disease. North Ronaldsay sheep is a promising model to study Indian Childhood cirrhosis and its analogues, and Bedlington Terrier copper toxicosis may share many similarities with Indian childhood cirrhosis. In the future, increased research collaboration between basic and applied scientists will be needed to link molecular defects to their morphologic and clinical implications.
Methods
The following methods are routinely used in our laboratory for qualitative and quantitative detection of copper.
Rhodanine method for histochemical detection of copper
Liver sections are dewaxed and hydrated to distilled water. Then, sections are placed in rhodanine working solution at 37°C for 18 hours. Rhodanine working solution is prepared using 3.0 ml of 0.2% Rhodanine stock solution (0.2 g rhodanine in 100 ml 100% ethanol) and 50 ml buffer acetate (5.0 ml 40% formalin, 20 g sodium acetate in 1000 ml distilled water).
Slides are rinsed in 3 changes of acetate buffer solution, counterstained in Mayer's hematoxylin solution, rinsed in acetate buffer, dehydrated, cleared and mounted.
Measurement of copper in tissue by flame atomic absorption spectroscopy
Liver samples are placed in plastic bags, frozen at -80°C and stored for 24 hours. Tissues are then processed for atomic absorption spectrophotometry. Briefly, approximately 1 gram of tissue from each sample is weighed and placed in a Teflon container for microwave digestion. All samples are weighed in duplicate. Control samples with known amounts of copper are also included. To each vessel, including a blank containing no tissue, 1.0 ml of deionized, distilled water and 2.5 ml full strength, trace metal free nitric acid (10.95 M HNO3) is added. Vessels are capped and placed in a MDS-200 microwave oven and digested. The digested contents are poured off and diluted to 10 ml with distilled water and thoroughly mixed. Copper concentrations are measured using a spectrophometer equipped with a copper hollow cathode lamp, with the following instrument settings: wavelength 324.8 nm, slit width 0.7 nm, lamp current 17 mA. Standards used are 3, 6 and 12 ppm prepared from 1000 ppm stock standard in 0.2 M HNO3. Peak area is read with a read delay of 0 s, and a read time of 5 s. Standard reference materials are used as quality control substances, and are processed with each batch of liver samples. Samples are not corrected for recovery if the he recovery of the quality control samples is 95% or more. Cu concentrations are recorded in μg/g wet weight tissue.
References
Loudianos G, Gitlin JD: Wilson's disease. Semin Liver Dis. 2000, 20: 353-364. 10.1055/s-2000-9389.
Dieter HH, Schimmelpfennig W, Meyer E, Tabert M: Early childhood cirrhoses (ECC) in Germany between 1982 and 1994 with special consideration of copper etiology. Eur J Med Res. 1999, 4: 233-242.
Tanner MS: Role of copper in Indian childhood cirrhosis. Am J Clin Nutr. 1998, 67: 1074S-1081S.
Muller T, van De Sluis B., Muller W, Pearson P, Wijmenga C: Non-Indian childhood cirrhosis. Eur J Med Res. 1999, 4: 293-297.
Thornburg LP: A perspective on copper and liver disease in the dog. J Vet Diagn Invest. 2000, 12: 101-110.
Haywood S, Muller T, Muller W, Heinz-Erian P, Tanner MS, Ross G: Copper-associated liver disease in North Ronaldsay sheep: a possible animal model for non-Wilsonian hepatic copper toxicosis of infancy and childhood. J Pathol. 2001, 195: 264-269. 10.1002/path.930.
Muller T, Muller W, Feichtinger H: Idiopathic copper toxicosis. Am J Clin Nutr. 1998, 67: 1082S-1086S.
Elmes ME, Clarkson JP, Mahy NJ, Jasani B: Metallothionein and copper in liver disease with copper retention--a histopathological study. J Pathol. 1989, 158: 131-137.
Fuentealba C, Guest S, Haywood S, Horney B: Chronic hepatitis: a retrospective study in 34 dogs. Can Vet J. 1997, 38: 365-373.
Wu J, Forbes JR, Chen HS, Cox DW: The LEC rat has a deletion in the copper transporting ATPase gene homologous to the Wilson disease gene. Nat Genet. 1994, 7: 541-545.
Theophilos MB, Cox DW, Mercer JF: The toxic milk mouse is a murine model of Wilson disease. Hum Mol Genet. 1996, 5: 1619-1624. 10.1093/hmg/5.10.1619.
Terada K, Aiba N, Yang XL, Iida M, Nakai M, Miura N, Sugiyama T: Biliary excretion of copper in LEC rat after introduction of copper transporting P-type ATPase, ATP7B. FEBS Lett. 1999, 448: 53-56. 10.1016/S0014-5793(99)00319-1.
Cousins RJ: Absorption, transport, and hepatic metabolism of copper and zinc: special reference to metallothionein and ceruloplasmin. Physiol Rev. 1985, 65: 238-309.
DiDonato M, Sarkar B: Copper transport and its alterations in Menkes and Wilson diseases. Biochim Biophys Acta. 1997, 1360: 3-16. 10.1016/S0925-4439(96)00064-6.
Kagi J: Overview of metallothionein. Methods Enzymol. 1991, 205: 613-626.
Miles AT, Hawksworth GM, Beattie JH, Rodilla V: Induction, regulation, degradation, and biological significance of mammalian metallothioneins. Crit Rev Biochem Mol Biol. 2000, 35: 35-70.
Linder MC, Hazegh-Azam M: Copper biochemistry and molecular biology. Am J Clin Nutr. 1996, 63: 797S-811S.
Harris ED: Copper transport: an overview. Proc Soc Exp Biol Med. 1991, 196: 130-140.
Zhou B, Gitschier J: hCTR1: a human gene for copper uptake identified by complementation in yeast. Proc Natl Acad Sci U S A. 1997, 94: 7481-7486. 10.1073/pnas.94.14.7481.
Klomp LW, Lin SJ, Yuan DS, Klausner RD, Culotta VC, Gitlin JD: Identification and functional expression of HAH1, a novel human gene involved in copper homeostasis. J Biol Chem. 1997, 272: 9221-9226. 10.1074/jbc.272.14.9221.
Bull PC, Thomas GR, Rommens JM, Forbes JR, Cox DW: The Wilson disease gene is a putative copper transporting P-type ATPase similar to the Menkes gene. Nat Genet. 1993, 5: 327-337.
Dijkstra M, Vonk RJ, Kuipers F: How does copper get into bile? New insights into the mechanism(s) of hepatobiliary copper transport. J Hepatol. 1996, 24 Suppl 1: 109-120.
Nagano K, Nakamura K, Urakami KI, Umeyama K, Uchiyama H, Koiwai K, Hattori S, Yamamoto T, Matsuda I, Endo F: Intracellular distribution of the Wilson's disease gene product (ATPase7B) after in vitro and in vivo exogenous expression in hepatocytes from the LEC rat, an animal model of Wilson's disease. Hepatology. 1998, 27: 799-807.
Schaefer M, Roelofsen H, Wolters H, Hofmann WJ, Muller M, Kuipers F, Stremmel W, Vonk RJ: Localization of the Wilson's disease protein in human liver. Gastroenterology. 1999, 117: 1380-1385.
Schilsky ML, Stockert RJ, Sternlieb I: Pleiotropic effect of LEC mutation: a rodent model of Wilson's disease. Am J Physiol. 1994, 266: G907-G913.
Bacon BR, Schilsky ML: New knowledge of genetic pathogenesis of hemochromatosis and Wilson's disease. Adv Intern Med. 1999, 44: 91-116.
Pena MM, Lee J, Thiele DJ: A delicate balance: homeostatic control of copper uptake and distribution. J Nutr. 1999, 129: 1251-1260.
Freedman JH, Ciriolo MR, Peisach J: The role of glutathione in copper metabolism and toxicity. J Biol Chem. 1989, 264: 5598-5605.
Dameron CT, Harris ED: Regulation of aortic CuZn-superoxide dismutase with copper. Caeruloplasmin and albumin re-activate and transfer copper to the enzyme in culture. Biochem J. 1987, 248: 669-675.
Harris ZL, Gitlin JD: Genetic and molecular basis for copper toxicity. Am J Clin Nutr. 1996, 63: 836S-841S.
Crawford JM: The liver and the biliary tract. Basic Pathology. Edited by: KumarV, CotranRS and RobbinsSL. 1997, Philadelphia, WB Saunders, 516-555.
Gross J.B.,Jr., Myers BM, Kost LJ, Kuntz SM, LaRusso NF: Biliary copper excretion by hepatocyte lysosomes in the rat. Major excretory pathway in experimental copper overload. J Clin Invest. 1989, 83: 30-39.
Luza SC, Speisky HC: Liver copper storage and transport during development: implications for cytotoxicity. Am J Clin Nutr. 1996, 63: 812S-820S.
Schilsky ML: In vitro modeling of liver membrane copper transport. Hepatology. 1995, 22: 1340-1342.
Subramanian I, Vanek ZF, Bronstein JM: Diagnosis and Treatment of Wilson's Disease. Curr Neurol Neurosci Rep. 2002, 2: 317-323.
Kasai N, Osanai T, Miyoshi I, Kamimura E, Yoshida MC, Dempo K: Clinico-pathological studies of LEC rats with hereditary hepatitis and hepatoma in the acute phase of hepatitis. Lab Anim Sci. 1990, 40: 502-505.
Rauch H, Wells AJ: The toxic milk mutation, tx, which results in a condition resembling Wilson disease in humans, is linked to mouse chromosome 8. Genomics. 1995, 29: 551-552. 10.1006/geno.1995.9968.
Johnson GF, Gilbertson SR, Goldfischer S, Grushoff PS, Sternlieb I: Cytochemical detection of inherited copper toxicosis of Bedlington terriers. Vet Pathol. 1984, 21: 57-60.
Haywood S, Fuentealba IC, Foster J, Ross G: Pathobiology of copper-induced injury in Bedlington terriers: ultrastructural and microanalytical studies. Anal Cell Pathol. 1996, 10: 229-241.
Thornburg LP, Shaw D, Dolan M, Raisbeck M, Crawford S, Dennis GL, Olwin DB: Hereditary copper toxicosis in West Highland white terriers. Vet Pathol. 1986, 23: 148-154.
Kaplan MM: Primary biliary cirrhosis. N Engl J Med. 1996, 335: 1570-1580. 10.1056/NEJM199611213352107.
Miyamura H, Nakanuma Y, Kono N: Survey of copper granules in liver biopsy specimens from various liver abnormalities other than Wilson's disease and biliary diseases. Gastroenterol Jpn. 1988, 23: 633-638.
Johnson GF, Zawie DA, Gilbertson SR, Sternlieb I: Chronic active hepatitis in Doberman pinschers. J Am Vet Med Assoc. 1982, 180: 1438-1442.
Haywood S, Rutgers HC, Christian MK: Hepatitis and copper accumulation in Skye terriers. Vet Pathol. 1988, 25: 408-414.
Schilsky ML: Wilson disease: genetic basis of copper toxicity and natural history. Semin Liver Dis. 1996, 16: 83-95.
Nanji MS, Nguyen VT, Kawasoe JH, Inui K, Endo F, Nakajima T, Anezaki T, Cox DW: Haplotype and mutation analysis in Japanese patients with Wilson disease. Am J Hum Genet. 1997, 60: 1423-1429.
Scheinberg IH, Sternlieb I: Wilson disease and idiopathic copper toxicosis. Am J Clin Nutr. 1996, 63: 842S-845S.
Ferenci P: Wilson's disease. Ital J Gastroenterol Hepatol. 1999, 31: 416-425.
Thomas GR, Forbes JR, Roberts EA, Walshe JM, Cox DW: The Wilson disease gene: spectrum of mutations and their consequences. Nat Genet. 1995, 9: 210-217.
Roberts EA, Cox DW: Wilson disease. Baillieres Clin Gastroenterol. 1998, 12: 237-256.
Steindl P, Ferenci P, Dienes HP, Grimm G, Pabinger I, Madl C, Maier-Dobersberger T, Herneth A, Dragosics B, Meryn S, Knoflach P, Granditsch G, Gangl A: Wilson's disease in patients presenting with liver disease: a diagnostic challenge. Gastroenterology. 1997, 113: 212-218.
Pilloni L, Lecca S, Van Eyken P, Flore C, Demelia L, Pilleri G, Nurchi AM, Farci AM, Ambu R, Callea F, Faa G: Value of histochemical stains for copper in the diagnosis of Wilson's disease. Histopathology. 1998, 33: 28-33. 10.1046/j.1365-2559.1998.00455.x.
Bingham MJ, Ong TJ, Summer KH, Middleton RB, McArdle HJ: Physiologic function of the Wilson disease gene product, ATP7B. Am J Clin Nutr. 1998, 67: 982S-987S.
Masuda R, Yoshida MC, Sasaki M, Dempo K, Mori M: Hereditary hepatitis of LEC rats is controlled by a single autosomal recessive gene. Lab Anim. 1988, 22: 166-169.
Cuthbert JA: Wilson's disease: a new gene and an animal model for an old disease. J Investig Med. 1995, 43: 323-336.
Kato J, Kobune M, Kohgo Y, Sugawara N, Hisai H, Nakamura T, Sakamaki S, Sawada N, Niitsu Y: Hepatic iron deprivation prevents spontaneous development of fulminant hepatitis and liver cancer in Long-Evans Cinnamon rats. J Clin Invest. 1996, 98: 923-929.
Sternlieb I, Quintana N, Volenberg I, Schilsky ML: An array of mitochondrial alterations in the hepatocytes of Long-Evans Cinnamon rats. Hepatology. 1995, 22: 1782-1787.
Downey JS, Bingle CD, Cottrell S, Ward N, Churchman D, Dobrota M, Powell CJ: The LEC rat possesses reduced hepatic selenium, contributing to the severity of spontaneous hepatitis and sensitivity to carcinogenesis. Biochem Biophys Res Commun. 1998, 244: 463-467. 10.1006/bbrc.1998.8296.
Yokoi T, Nagayama S, Kajiwara R, Kawaguchi Y, Aizawa T, Otaki Y, Aburada M, Kamataki T: Occurrence of autoimmune antibodies to liver microsomal proteins associated with lethal hepatitis in LEC rats: effects of TJN-101 ((+)-(6S,7S,R-biar)- 5,6,7,8-tetrahydro-1,2,3,12-tetramethoxy-6,7-dimethyl-10,11- methylenedioxy-6-dibenzo[a,c]cyclooctenol) on the development of hepatitis and the autoantibodies. Toxicol Lett. 1995, 76: 33-38. 10.1016/0378-4274(94)03190-8.
Li Y, Togashi Y, Sato S, Emoto T, Kang JH, Takeichi N, Kobayashi H, Kojima Y, Une Y, Uchino J: Spontaneous hepatic copper accumulation in Long-Evans Cinnamon rats with hereditary hepatitis. A model of Wilson's disease. J Clin Invest. 1991, 87: 1858-1861.
Yokoi T, Nagayama S, Kajiwara R, Kawaguchi Y, Kamataki T: Effects of cyclosporin-A and D-penicillamine on the development of hepatitis and the production of antibody to protein disulfide isomerase in LEC rats. Res Commun Mol Pathol Pharmacol. 1994, 85: 73-81.
Bedard K, Fuentealba IC, Cribb A: The Long Evans Cinnamon (LEC) rat develops hepatocellular damage in the absence of antimicrosomal antibodies. Toxicology. 2000, 146: 101-109. 10.1016/S0300-483X(00)00169-4.
Rui M, Suzuki KT: Copper in plasma reflects its status and subsequent toxicity in the liver of LEC rats. Res Commun Mol Pathol Pharmacol. 1997, 98: 335-346.
Mori M, Hattori A, Sawaki M, Tsuzuki N, Sawada N, Oyamada M, Sugawara N, Enomoto K: The LEC rat: a model for human hepatitis, liver cancer, and much more. Am J Pathol. 1994, 144: 200-204.
Betto H, Kaneda K, Yamamoto T, Kojima A, Sakurai M: Development of intralobular bile ductules after spontaneous hepatitis in Long-Evans mutant rats. Lab Invest. 1996, 75: 43-53.
Cheng WS, Govindarajan S, Redeker AG: Hepatocellular carcinoma in a case of Wilson's disease. Liver. 1992, 12: 42-45.
Biempica L, Rauch H, Quintana N, Sternlieb I: Morphologic and chemical studies on a murine mutation (toxic milk mice) resulting in hepatic copper toxicosis. Lab Invest. 1988, 59: 500-508.
Llanos RM, Mercer JF: The molecular basis of copper homeostasis copper-related disorders. DNA Cell Biol. 2002, 21: 259-270. 10.1089/104454902753759681.
Betard C, Rasquin-Weber A, Brewer C, Drouin E, Clark S, Verner A, Darmond-Zwaig C, Fortin J, Mercier J, Chagnon P, Fujiwara TM, Morgan K, Richter A, Hudson TJ, Mitchell GA: Localization of a recessive gene for North American Indian childhood cirrhosis to chromosome region 16q22-and identification of a shared haplotype. Am J Hum Genet. 2000, 67: 222-228. 10.1086/302993.
MacLachlan GK, Johnston WS: Copper poisoning in sheep from North Ronaldsay maintained on a diet of terrestrial herbage. Vet Rec. 1982, 111: 299-301.
Zhang F, Jia J, Wang B, Qian L, Yin S, Wang Y, Cui Y, You H, Ma H, Wang H, Zhang C: [Clinical characteristics of primary biliary cirrhosis: a report of 45 cases]. Zhonghua Nei Ke Za Zhi. 2002, 41: 163-167.
Dienes HP, Erberich H, Dries V, Schirmacher P, Lohse A: Autoimmune hepatitis and overlap syndromes. Clin Liver Dis. 2002, 6: 349-62, vi.
Strassburg CP, Manns MP: Autoimmune tests in primary biliary cirrhosis. Baillieres Best Pract Res Clin Gastroenterol. 2000, 14: 585-599. 10.1053/bega.2000.0105.
Markus BH, Dickson ER, Grambsch PM, Fleming TR, Mazzaferro V, Klintmalm GB, Wiesner RH, Van Thiel DH, Starzl TE: Efficiency of liver transplantation in patients with primary biliary cirrhosis. N Engl J Med. 1989, 320: 1709-1713.
Bjoro K, Friman S, Hockerstedt K, Kirkegaard P, Keiding S, Schrumpf E, Olausson M, Oksanen A, Isoniemi H, Hjortrup A, Bergan A, Ericzon BG: Liver transplantation in the Nordic countries, 1982-1998: changes of indications and improving results. Scand J Gastroenterol. 1999, 34: 714-722. 10.1080/003655299750025930.
Kowdley KV, Knox TA, Kaplan MM: Hepatic copper content is normal in early primary biliary cirrhosis and primary sclerosing cholangitis. Dig Dis Sci. 1994, 39: 2416-2420.
LaRusso NF: The Fifth Carlos E. Rubio Memorial Lecture. Sclerosing cholangitis: pathogenesis, pathology, and practice. P R Health Sci J. 1999, 18: 11-17.
Crawford MA, Schall WD, Jensen RK, Tasker JB: Chronic active hepatitis in 26 Doberman pinschers. J Am Vet Med Assoc. 1985, 187: 1343-1350.
Thornburg LP: Histomorphological and immunohistochemical studies of chronic active hepatitis in Doberman Pinschers. Vet Pathol. 1998, 35: 380-385.
Speeti M, Eriksson J, Saari S, Westermarck E: Lesions of subclinical doberman hepatitis. Vet Pathol. 1998, 35: 361-369.
Center SA: Chronic hepatitis, cirrhosis, breed-specific hepatophathies, copper storage hepatopathy, suppurative hepatitis, granulomatous hepatitis, and idiopathic hepatic fibrosis. Strombeck's Small Animal Gastroenterology. Edited by: GuilfordWG, CenterSA, StrombeckDR, WilliamsDA and MeyerDJ. 1996, Philadelphia, WB Saunders, 705-765.
Day DG: Feline cholangiohepatitis complex. Vet Clin North Am Small Anim Pract. 1995, 25: 375-385.
Kaplan MM: Primary biliary cirrhosis. Adv Intern Med. 1987, 32: 359-377.
Prasse KW, Mahaffey EA, DeNovo R, Cornelius L: Chronic lymphocytic cholangitis in three cats. Vet Pathol. 1982, 19: 99-108.
B. van de Sluis, Rothuizen J, Pearson PL, van Oost BA, Wijmenga C: Identification of a new copper metabolism gene by positional cloning in a purebred dog population. Hum Mol Genet. 2002, 11: 165-173. 10.1093/hmg/11.2.165.
Herrtage ME, Seymour CA, Jefferies AR, Blakemore WF, Palmer AC: Inherited copper toxicosis in the Bedlington terrier: a report of two clinical cases. J Small Anim Pract. 1987, 28: 1127-1140.
Center SA: Pathophysiology, laboratory diagnosis, and diseases of the liver. Textbook of Veterinary Internal Medicine. Edited by: EttingerSJ. 1995, Philadelphia, WB Saunders, 1261-1371.
van de Sluis BJ, Breen M, Nanji M, van Wolferen M, de Jong P, Binns MM, Pearson PL, Kuipers J, Rothuizen J, Cox DW, Wijmenga C, van Oost BA: Genetic mapping of the copper toxicosis locus in Bedlington terriers to dog chromosome 10, in a region syntenic to human chromosome region 2p13-p16. Hum Mol Genet. 1999, 8: 501-507. 10.1093/hmg/8.3.501.
Dagenais SL, Guevara-Fujita M, Loechel R, Burgess AC, Miller DE, Yuzbasiyan-Gurkan V, Brewer GJ, Glover TW: The canine copper toxicosis locus is not syntenic with ATP7B or ATX1 and maps to a region showing homology to human 2p21. Mamm Genome. 1999, 10: 753-756. 10.1007/s003359901085.
Nanji MS, Cox DW: The copper chaperone Atox1 in canine copper toxicosis in Bedlington terriers. Genomics. 1999, 62: 108-112. 10.1006/geno.1999.5983.
Nanji M, Coronado VA, Cox DW: ATP6H, a subunit of vacuolar ATPase involved in metal transport: evaluation in canine copper toxicosis. Mamm Genome. 2001, 12: 617-621. 10.1007/s00335-001-2059-1.
Twedt DC, Sternlieb I, Gilbertson SR: Clinical, morphologic, and chemical studies on copper toxicosis of Bedlington Terriers. J Am Vet Med Assoc. 1979, 175: 269-275.
Hunt DM, Wake SA, Mercer JF, Danks DM: A study of the role of metallothionein in the inherited copper toxicosis of dogs. Biochem J. 1986, 236: 409-415.
Kelly WR: The liver and biliary system. Pathology of Domestic Animals. Edited by: JubbKVF, KennedyPC and PalmerN. 1993, San Diego, Academic Press, 319-406.
Thornburg LP, Rottinghaus G, McGowan M, Kupka K, Crawford S, Forbes S: Hepatic copper concentrations in purebred and mixed-breed dogs. Vet Pathol. 1990, 27: 81-88.
Kelly DF, Haywood S, Bennett AM: Copper toxicosis in Bedlington terrier in the United Kingdom. J Small Anim Pract. 1984, 25: 293-298.
Ludwig J, Owen C.A.,Jr., Barham SS, McCall JT, Hardy RM: The liver in the inherited copper disease of Bedlington terriers. Lab Invest. 1980, 43: 82-87.
Cooper VL, Carlson MP, Jacobson J, Schneider NR: Hepatitis and increased copper levels in a dalmatian. J Vet Diagn Invest. 1997, 9: 201-203.
Noaker LJ, Washabau RJ, Detrisac CJ, Heldmann E, Hendrick MJ: Copper associated acute hepatic failure in a dog. J Am Vet Med Assoc. 1999, 214: 1502-6, 1495.
Lewis NJ, Fallah-Rad AH, Connor ML: Copper toxicity in confinement-housed ram lambs. Can Vet J. 1997, 38: 496-498.
Soli NE: Chronic copper poisoning in sheep. A review of the literature. Nord Vet Med. 1980, 32: 75-89.
Maiorka PC, Massoco CO, de Almeida SD, Gorniak SL, Dagli ML: Copper toxicosis in sheep: a case report. Vet Hum Toxicol. 1998, 40: 99-100.
Auza N: [Copper in ruminants. Review]. Ann Rech Vet. 1983, 14: 21-37.
Ishmael J, Gopinath C, Howell JM: Experimental chronic copper toxicity in sheep. Histological and histochemical changes during the development of the lesions in the liver. Res Vet Sci. 1971, 12: 358-366.
Gooneratne SR, Howell JM, Cook RD: An ultrastructural and morphometric study of the liver of normal and copper-poisoned sheep. Am J Pathol. 1980, 99: 429-449.
Gopinath C, Howell JM: Experimental chronic copper toxicity in sheep. Changes that follow the cessation of dosing at the onset of haemolysis. Res Vet Sci. 1975, 19: 35-43.
Sargison ND, Scott PR, Penny CD, Pirie RS: Polioencephalomalacia associated with chronic copper poisoning in a Suffolk ram lamb. Vet Rec. 1994, 135: 556-557.
Ishmael J, Gopinath C, Howell JM: Experimental chronic copper toxicity in sheep. Biochemical and haematological studies during the development of lesions in the liver. Res Vet Sci. 1972, 13: 22-29.
Kumaratilake JS, Howell JM: Histochemical study of the accumulation of copper in the liver of sheep. Res Vet Sci. 1987, 42: 73-81.
Haynes JS, Wade PR: Hepatopathy associated with excessive hepatic copper in a Siamese cat. Vet Pathol. 1995, 32: 427-429.
Fox JG, Zeman DH, Mortimer JD: Copper toxicosis in sibling ferrets. J Am Vet Med Assoc. 1994, 205: 1154-1156.
Twedt DC, Hunsaker HA, Allen KG: Use of 2,3,2-tetramine as a hepatic copper chelating agent for treatment of copper hepatotoxicosis in Bedlington terriers. J Am Vet Med Assoc. 1988, 192: 52-56.
Sass-Kortsak A: Wilson's disease. A treatable liver disease in children. Pediatr Clin North Am. 1975, 22: 963-984.
Scheinberg IH: Toxicity of penicillamine. Postgrad Med J. 1968, Suppl-4.
Rolfe DS, Twedt DC: Copper-associated hepatopathies in dogs. Vet Clin North Am Small Anim Pract. 1995, 25: 399-417.
Scheinberg IH, Jaffe ME, Sternlieb I: The use of trientine in preventing the effects of interrupting penicillamine therapy in Wilson's disease. N Engl J Med. 1987, 317: 209-213.
Brewer GJ, Dick RD, Yuzbasiyan-Gurkin V, Tankanow R, Young AB, Kluin KJ: Initial therapy of patients with Wilson's disease with tetrathiomolybdate. Arch Neurol. 1991, 48: 42-47.
Brewer GJ, Dick RD, Johnson V, Wang Y, Yuzbasiyan-Gurkan V, Kluin K, Fink JK, Aisen A: Treatment of Wilson's disease with ammonium tetrathiomolybdate. I. Initial therapy in 17 neurologically affected patients. Arch Neurol. 1994, 51: 545-554.
Brewer GJ, Dick RD, Schall W, Yuzbasiyan-Gurkan V, Mullaney TP, Pace C, Lindgren J, Thomas M, Padgett G: Use of zinc acetate to treat copper toxicosis in dogs. J Am Vet Med Assoc. 1992, 201: 564-568.
Hoogenraad TU: Zinc treatment of Wilson's disease. J Lab Clin Med. 1998, 132: 240-241.
Van Ryssen JB: The effectiveness of using supplementary zinc and molybdenum to reduce the copper content in the liver of hypercuprotic sheep. J S Afr Vet Assoc. 1994, 65: 59-63.
Gooneratne SR, Howell JM, Aughey E: An ultrastructural study of the kidney of normal, copper poisoned and thiomolybdate-treated sheep. J Comp Pathol. 1986, 96: 593-612.
Gooneratne SR, Howell JM, Gawthorne JM: Intravenous administration of thiomolybdate for the prevention and treatment of chronic copper poisoning in sheep. Br J Nutr. 1981, 46: 457-467.
Haywood S, Dincer Z, Holding J, Parry NM: Metal (molybdenum, copper) accumulation and retention in brain, pituitary and other organs of ammonium tetrathiomolybdate-treated sheep. Br J Nutr. 1998, 79: 329-331.
Author information
Authors and Affiliations
Corresponding author
Additional information
I Carmen Fuentealba and Enrique M Aburto contributed equally to this work.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Fuentealba, I.C., Aburto, E.M. Animal models of copper-associated liver disease. Comp Hepatol 2, 5 (2003). https://doi.org/10.1186/1476-5926-2-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-5926-2-5