
Abstract
Background
The efficacy and safety of plant stanols added to food products as serum cholesterol lowering agents have been demonstrated convincingly, but their effects on cholesterol metabolism and on serum non-cholesterol sterols is less evaluated. The aim of this study was to assess the validity of serum non-cholesterol sterols and squalene as bioindices of cholesterol synthesis and absorption, and to examine how the individual serum non-cholesterol sterols respond to consumption of plant stanols.
Methods
We collected all randomized, controlled plant stanol ester (STAEST) interventions in which serum cholestanol, plant sterols campesterol and sitosterol, and at least two serum cholesterol precursors had been analysed. According to these criteria, there was a total of 13 studies (total 868 subjects without lipid-lowering medication; plant stanol doses varied from 0.8 to 8.8 g/d added in esterified form; the duration of the studies varied from 4 to 52 weeks). Serum non-cholesterol sterols were assayed with gas–liquid chromatography, cholesterol synthesis with the sterol balance technique, and fractional cholesterol absorption with the dual continuous isotope feeding method.
Results
The results demonstrated that during the control and the STAEST periods, the serum plant sterol/cholesterol- and the cholestanol/cholesterol-ratios reflected fractional cholesterol absorption, and the precursor sterol/cholesterol-ratios reflected cholesterol synthesis. Plant sterol levels were dose-dependently reduced by STAEST so that 2 g of plant stanols reduced serum campesterol/cholesterol-ratio on average by 32%. Serum cholestanol/cholesterol-ratio was reduced less frequently than those of the plant sterols by STAEST, and the cholesterol precursor sterol ratios did not change consistently in the individual studies emphasizing the importance of monitoring more than one surrogate serum marker.
Conclusions
Serum non-cholesterol sterols are valid markers of cholesterol absorption and synthesis even during cholesterol absorption inhibition with STAEST. Serum plant sterol concentrations decrease dose-dependently in response to plant stanols suggesting that the higher the plant stanol dose, the more cholesterol absorption is inhibited and the greater the reduction in LDL cholesterol level is that can be achieved.
Trial registration
Clinical Trials Register # NCT00698256 [Eur J Nutr 2010, 49:111-117]
Similar content being viewed by others
Background
The hypocholesterolemic effect of dietary plant sterol supplementation was demonstrated for the first time in humans in the 1950′s [1] and that of plant stanols in the 1980′s [2]. Today, several food products with added plant sterols and plant stanols are used worldwide as a dietary means to lower serum total and LDL cholesterol concentrations by interfering with cholesterol absorption [3, 4]. Thus, in addition to the reduction in the serum cholesterol concentration, these agents makes it possible to evaluate cholesterol metabolism in response to inhibition of cholesterol absorption.
The assessment of cholesterol absorption and synthesis is laborious in clinical studies. For this reason, serum non-cholesterol sterols have been examined as relative markers of whole-body cholesterol metabolism under steady state conditions with subjects consuming a normal habitual diet. The levels of serum cholesterol precursors (squalene, cholestenol, desmosterol, and lathosterol) reflect the activity of cholesterol synthesis, and serum plant sterols (campesterol and sitosterol), and cholestanol, reflect the absorption efficiency of cholesterol. Their validity has been assessed by comparing the synthesis marker values with those obtained with the sterol balance technique [5–11] or with the evaluation of hepatic 3-hydroxy-3-methyl-glutaryl-CoA reductase activity [12], and the absorption marker values have been validated with those obtained with continuous peroral or peroral-intravenous isotopes and tracers [6–9, 13, 14]. For particular, the cholesterol-standardized ratios of the relevant serum markers were best associated with cholesterol synthesis and absorption efficiency [6–9], and the absorption marker/synthesis marker ratios with whole-body cholesterol metabolism [6, 7]. However, especially during interventions and when only one serum marker has been used, there have been inconsistencies in the results between the serum markers and absolute methods [8, 11]. In a recent cross-sectional study, e.g., serum plant sterol/cholesterol-ratios did not correlate with fractional cholesterol absorption [15]. In this study, the study population of 175 hypercholesterolemic subjects was divided into those with the lowest and highest campesterol/cholesterol ratio, and cholesterol absorption efficiency was measured with a single oral-intravenous dose. Cholesterol absorption efficiency did not differ between the groups. Of special interest was the very low values of cholesterol absorption efficiency with a mean of 24%, and only a few subjects reached the value of 50%, which is considered the average mean value among different populations. The results were discussed by Grundy [16] that there may be methodological reasons related to the tracer or the single dose-method per se causing these particularly low cholesterol absorption values, which could explain the lack of association. To this end, the aim of this study was to assess the validity of the cholesterol absorption and synthesis markers during consumption of plant stanol-supplemented food products. We also examined the changes in cholesterol metabolism occurring in response to plant stanol interventions. Since in general the number of subjects in single plant stanol interventions has been somewhat limited, we gathered together from PubMed all randomized controlled studies in adults, in which at least two serum synthesis markers, two serum plant sterols, and serum cholestanol levels were analysed during plant stanol intervention.
Methods
Study population
With these criteria, 13 studies could be identified. These included 868 subjects (414 men and 454 women) with an age range from 20 to 73 years (Table 1). In eleven of the studies, the subjects had mild to moderate hypercholesterolemia [17–27]. In one study, the subjects were type 1 diabetics [28], and another study focused on type 2 diabetics [29]. All subjects were without lipid-lowering medication. The plant stanol dose varied from 0.8 to 8.8 g/d, and in all of the studies, the plant stanols were consumed as their fatty acid esters. Two of the studies were dose–response studies [23, 27]. Six studies had a cross-over and seven employed a parallel design. The duration of plant stanol ester (STAEST) consumption varied from 4 to 52 weeks.
All subjects gave their written informed consent. All studies were performed according to the principles of the Declaration of Helsinki. The Ethics Committees of the University of Helsinki, Second Department of Medicine (studies in ref 19,20,21,26,27,29), University of Kuopio (studies in ref 17,22,23,24,28), the North Karelia Central Hospital (study in ref 18), and Joint Ethics Committee of the University of Turku and Turku University Central Hospital (study in ref 25) had approved the study protocols.
Measurements
Serum concentrations of non-cholesterol sterols were quantified from non-saponifiable serum-based materials by capillary gas–liquid chromatography (GLC) (Agilent 6890 N Network GC System, Agilent Technologies, Wilmington, DE) equipped with a 50 m long non-polar Ultra 2 capillary column (5% phenyl-methyl siloxane; Agilent Technologies, Wilmington, DE) with 5α-cholestane as internal standard [30]. Typical CVs at relevant concentrations were: cholesterol 3.2%, cholestanol 2.7%, desmosterol 6.0%, lathosterol 3.7%, campesterol 1.8%, and sitosterol 2.4%. Serum non-cholesterol sterols are given as concentrations (μg/dl) and in terms of ratios to cholesterol (102 × μmol/mmol of cholesterol), which was obtained from the same GLC run.
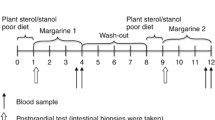
In the absolute metabolic studies, the participants took a capsule containing 200 mg of Cr2O3, 3H-sitostanol, and 14C-cholesterol three times a day with each major meal for a week. During the last three days, stools were collected and pooled for analysis of labels, neutral sterols, and bile acids. The sterols and bile acids were measured with GLC [31], using the recovery of Cr2O3 or labeled sitostanol for measurement of fecal flow. During the week, the participants kept a food diary so that energy, fat and cholesterol intakes could be quantified with the assistance of a computerized program [32].
Statistics
All statistical analyses were performed with the SPSS for Windows 19.0 statistics program (SPSS, Chicago, IL, USA).
Since the separate studies differed in their design (Table 1), the relative changes from the control values were recalculated from original data except in two studies [26, 27], in which the relative changes were calculated from the mean values given in the publications. The normal distribution of variables was confirmed before further statistical analyses. When detecting the relationships between the plant stanol dose and serum LDL cholesterol and non-cholesterol sterols, nine studies with hypercholesterolemic subjects [17–25] were included into the further statistical analyses. Curve equations were calculated by analysis of curve estimation and ANCOVA with the study as a covariate. Pearson correlation coefficients were also calculated. In addition, when detecting the validity, i.e. the associations between the simultaneous measurements of the serum non-cholesterol sterols and absolute cholesterol synthesis and absorption, the Pearson or Spearman correlation coefficients were calculated from the studies in which the data was available [20, 27, 29]. A P value of <0.05 was considered statistically significant.
Results
Serum non-cholesterol sterols as biomarkers of cholesterol metabolism
In three studies (n = 39) [20, 27, 29], cholesterol metabolism was evaluated with simultaneous measurements of fractional cholesterol absorption, cholesterol synthesis, and serum non-cholesterol sterols. During both the control and STAEST periods, serum cholestanol, campesterol and sitosterol concentrations (Table 2) and ratios to cholesterol, shown for cholestanol/cholesterol- and sitosterol/cholesterol-ratios in Figure 1 (Panels A and B), correlated with fractional cholesterol absorption. Similarly, during the control and STAEST periods, serum cholestenol, desmosterol, and lathosterol concentrations (Table 2) and ratios to cholesterol (shown for cholestenol/cholesterol-ratio in Figure 1 Panel C) correlated with cholesterol synthesis. Serum squalene concentration or squalene/cholesterol-ratio did not correlate with cholesterol synthesis. The sitosterol/lathosterol-ratio correlated with fractional cholesterol absorption during the control (r = 0.589, p < 0.001) and STAEST periods (r = 0.662, p < 0.001), and the corresponding values for cholesterol synthesis were r = −0.532, p < 0.001 and r = −0.512, p < 0.001.

Cholesterol absorption and synthesis and serum biomarkers. Three studies [20, 27, 29] combined, n=39. Panel A: Fractional cholesterol absorption (%) and serum cholestanol/cholesterol- ratio (102 × μmol/mmol of cholesterol) in 39 subjects during the control (closed circles) and plant stanol ester (STAEST) (open circles) intervention periods. The results from three studies [20, 27, 29] were combined. Panel B: Fractional cholesterol absorption (%) and serum sitosterol/cholesterol- ratio (102 × μmol/mmol of cholesterol) in 39 subjects during the control (closed circles) and plant stanol ester (STAEST) (open circles) intervention periods. The results from three studies [20, 27, 29] were combined. Panel C: Cholesterol synthesis (mg/kg/d) and serum cholestenol/cholesterol- ratio (102 × μmol/mmol of cholesterol) in 39 subjects during the control (open circles) and plant stanol ester (STAEST) (open circles) intervention periods.
Relative changes in LDL cholesterol and serum non-cholesterol sterol levels
In studies involving daily plant stanol intake ≥1.6 g, the LDL cholesterol concentration was significantly reduced (Table 1). Depending on the dose, the LDL cholesterol level was reduced by 6% (plant stanols 1.6 g/d) up to 17% (plant stanols 8.8 g/d). The extent of the reduction in LDL cholesterol correlated with the plant stanol dose (r = 0.686, p = 0.014) (Figure 2 Panel A).

Changes in LDL cholesterol concentration and serum campesterol/cholesterol-ratio and plant stanol dose. Panel A. Change (%) in LDL cholesterol concentration from controls during the different plant stanol doses in nine studies [17–25]. r = 0.686, p = 0.014. Panel B. Change (%) in serum campesterol/cholesterol-ratio from controls during the different plant stanol doses in nine studies [17–25]. r = −0.919, p < 0.001.
When compared to the controls, serum campesterol/cholesterol-ratio and sitosterol/cholesterol-ratio were reduced in every study (Table 1). The reductions of plant sterol/cholesterol-ratios were dose-dependent as shown for the serum campesterol/cholesterol-ratio in Figure 2 Panel B (r = −0.919, p < 0.001). On the contrary, serum cholestanol/cholesterol-ratio was reduced only in 5/17 trials (Table 1), and the reductions were not associated with the plant stanol dose.
Regarding the serum cholesterol precursors, STAEST consumption increased serum squalene/cholesterol-ratio in 1/17 trials, the cholestenol/cholesterol-ratio in 9/17 trials, the desmosterol/cholesterol-ratio in 8/17 trials, and the lathosterol/cholesterol-ratio in a clear majority in 13/17 of the trials (Table 1). The increase in the precursor sterol to cholesterol ratios varied from 7 to 34%, respectively, but there was extensive variation between different studies even with the same plant stanol dose. In two studies [17, 28], all of the precursors remained unchanged.
Discussion
The new results emerging from these analyses demonstrate that during plant stanol consumption, serum non-cholesterol sterol/cholesterol- ratios reflect the fractional absorption and whole-body synthesis of cholesterol. In addition, serum absorption/synthesis marker ratios were found to be valid markers of cholesterol metabolism during plant stanol intervention. Second, serum levels of plant sterols were dose-dependently reduced by plant stanols. The serum cholestanol level was reduced less frequently than the serum plant sterol levels during consumption of STAEST. The cholesterol precursor sterols, cholestenol, desmosterol and lathosterol, were not increased similarly or were not increased at all in some studies emphasizing the importance of adopting more than one surrogate serum marker. The serum squalene level was not related to cholesterol metabolism.
The study population contained all randomized controlled plant stanol interventions in adults gathered from PubMed, in which at least two serum synthesis markers, two serum plant sterols, and serum cholestanol were analysed. It turned out that the requirement for the non-cholesterol sterols excluded other than our own studies. In fact, 4 more studies could be retrieved from PubMed containing serum lathosterol and plant sterol quantifications, but not the other non-cholesterol sterols.
If one adopts surrogate serum markers, there is always the caveat that their validity should not be considered as self-evident [8]. In situations when there is interference with the homeostasis of cholesterol or the metabolism of an individual marker, the serum value of the marker/s no longer reflects cholesterol metabolism. Accordingly, the metabolism of both cholesterol and the individual marker need to be taken into consideration when interpreting the data. A classic example of potential misinterpretation is the fact that plant sterols cannot be used as cholesterol absorption markers at the same time when the subjects are consuming plant sterol-added products. Similarly, when dietary intake of cholesterol was increased by adding daily egg consumption, there was an elevation in the serum lathosterol concentration, but this no longer reflected cholesterol synthesis but instead the increased intake of lathosterol present in the egg yolk [11]. Even under baseline situations, the relative serum markers may not reflect cholesterol metabolism. In vegetarians, cholesterol synthesis is known to be elevated as compared with control subjects, but there was no increase in the concentrations of the serum cholesterol precursors [33].
In the present study, all serum cholesterol precursors were unchanged in two studies. The subjects in one of these studies were type 1 diabetics, and the precursor ratios to cholesterol varied from −30% to +2%. Why in type 1 diabetes cholesterol synthesis seems not to be activated remains open and warrants further investigation. Regarding the second study, the cholesterol precursors were increased from 14% to 30%, but the increment did not reach significance.
Cholestanol is a saturated derivative of cholesterol produced by the liver. Its synthesis involves mainly a rate-limiting oxidation pathway, but a smaller fraction is also synthesized as a by-product of bile acid production [34]. The dietary intake of cholestanol is minimal, less than 2 mg/d [9], but if biliary secretion is impaired such as in cholestasis, then serum cholestanol values rapidly increase and no longer reflect the absorption efficiency of cholesterol [35]. Even though the serum cholestanol concentration and the cholestanol/cholesterol-ratio correlated with fractional cholesterol absorption during STAEST, in the individual studies the cholestanol/cholesterol-ratio was less frequently reduced than the serum plant sterol/cholesterol-ratios.
In the present analysis, the relative LDL cholesterol reduction varied from 6 to 17% depending on the plant stanol dose used in the different studies. Similarly, the relative reduction for campesterol/cholesterol-ratio varied from 35 to 62%. One can calculate that a 2 g plant stanol dose can achieve about a 10% reduction in the LDL cholesterol concentration and a 32% decrease in the serum campesterol/cholesterol-ratio (Figure 2). Accordingly, the change in serum campesterol/cholesterol-ratio can also be utilized as an indicator of the compliance of the STAEST intake. An earlier study demonstrated that when LDL cholesterol was lowered by 10% with plant stanols, fractional cholesterol absorption was reduced by 45% and the serum campesterol/cholesterol-ratio by 34% (p < 0.05 for all) [36], which is the same magnitude estimated in the present study. These values suggest that approximately a four-fold inhibition in cholesterol absorption efficiency is needed to achieve a unit decrease in the LDL cholesterol concentration.
Conclusions
In conclusion, serum non-cholesterol sterols are valid markers of cholesterol absorption and synthesis during cholesterol absorption inhibition with plant stanol ester. Serum levels of non-cholesterol sterols did not change consistently in the individual studies emphasizing the importance of utilizing more than one surrogate serum marker. Serum plant sterols decrease dose-dependently after consumption of plant stanols suggesting that the higher the plant stanol dose, the more cholesterol absorption will be inhibited and the more efficiently the LDL cholesterol levels will be reduced.
Abbreviations
- GLC:
-
Gas–liquid chromatography
- STAEST:
-
Plant stanol ester.
References
Pollak OJ: Reduction of blood cholesterol in man. Circulation. 1953, VII: 702-706.
Heinemann T, Leiss O, von Bergmann K: Effect of low-dose sitostanol on serum cholesterol in patients with hypercholesterolemia. Atherosclerosis. 1986, 61: 219-223. 10.1016/0021-9150(86)90141-3
Grundy SM, Ahrens EH, Davignon J: The interaction of cholesterol absorption and cholesterol synthesis in man. J Lipid Res. 1969, 10: 304-315.
Heinemann T, Kullak-Ublick G-A, Pietruck B, von Bergmann K: Mechanisms of action of plant sterols on inhibition of cholesterol absorption. Eur J Clin Pharmacol. 1991, 40 (Suppl. 1): S59-S63.
Miettinen TA: Serum squalene and methyl sterols as indicators of cholesterol synthesis in vivo. Life Sci. 1969, 8: 713-721. 10.1016/0024-3205(69)90007-1
Miettinen TA, Tilvis RS, Kesäniemi YA: Serum plant sterols and cholesterol precursors reflect cholesterol absorption and synthesis in volunteers of a randomly selected male population. Am J Epidemiol. 1990, 131: 20-31.
Simonen P, Gylling H, Miettinen TA: The validity of serum squalene and non-cholesterol sterols as surrogate markers of cholesterol synthesis and absorption in type 2 diabetes. Atherosclerosis. 2008, 197: 883-888. 10.1016/j.atherosclerosis.2007.08.003
Miettinen TA, Gylling H, Nissinen MJ: The role of serum non-cholesterol sterols as surrogate markers of absolute cholesterol synthesis and absorption. Nutr Metab Cardiovasc Dis. 2011, 21: 765-769. 10.1016/j.numecd.2011.05.005
Miettinen TA, Tilvis RS, Kesäniemi YA: Serum cholestanol and plant sterol levels in relation to cholesterol metabolism in middle-aged men. Metabolism. 1989, 38: 136-140. 10.1016/0026-0495(89)90252-7
Kempen HJ, Glatz JF, Gevers Leuven JA, van der Voort HA, Katan MB: Serum lathosterol concentration is an indicator of whole-body cholesterol synthesis in humans. J Lipid Res. 1988, 29: 1149-1155.
Duane WC: Serum lathosterol levels in human subjects reflect changes in whole body cholesterol synthesis induced by lovastatin but not dietary cholesterol. J Lipid Res. 1995, 36: 343-348.
Björkhem I, Miettinen T, Reihnér E, Ewerth S, Angelin B, Einarsson K: Correlation between serum levels of some cholesterol precursors and activity of HMG-CoA reductase in human liver. J Lipid Res. 1987, 28: 1137-1143.
Crouse JR, Grundy SM: Evaluation of a continuous isotope feeding method for measurement of cholesterol absorption in man. J Lipid Res. 1978, 19: 967-971.
Racette SB, Lin X, Lefevre M, Anderson Spearie C, Most MM, Ma L, Ostlund RE: Dose effects of dietary phytosterols on cholesterol metabolism: a controlled feeding study. Am J Clin Nutr. 2010, 91: 32-38. 10.3945/ajcn.2009.28070
Jakulj L, Mohammed H, van Dijk TH, Boer T, Turner S, Groen AK, Vissers MN, Stroes ES: Plasma plant sterols serve as poor markers of cholesterol absorption in man. J Lipid Res. 2013, 54: 1144-1150. 10.1194/jlr.P031021
Grundy SM: Plasma noncholesterol sterols as indicators of cholesterol absorption. J Lipid Res. 2013, 54: 873-875. 10.1194/jlr.E036806
Gylling H, Hallikainen M, Nissinen MJ, Simonen P, Miettinen TA: Very high plant stanol intake and serum plant stanols and non-cholesterol sterols. Eur J Nutr. 2010, 49: 111-117. 10.1007/s00394-009-0055-5
Gylling H, Hallikainen M, Raitakari OT, Laakso M, Vartiainen E, Salo P, Korpelainen V, Sundvall J, Miettinen TA: Long-term consumption of plant stanol and sterol esters, vascular function and genetic regulation. Brit J Nutr. 2009, 101: 1688-1695. 10.1017/S0007114508116300
Gylling H, Miettinen T: Cholesterol reduction by different plant stanol mixtures and with variable fat intake. Metabolism. 1999, 48: 575-580. 10.1016/S0026-0495(99)90053-7
Gylling H, Radhakrishnan R, Miettinen TA: Reduction of serum cholesterol in postmenopausal women with previous myocardial infarction and cholesterol malabsorption induced by dietary sitostanol ester margarine. Women and dietary sitostanol. Circulation. 1997, 96: 4226-4231. 10.1161/01.CIR.96.12.4226
Gylling H, Puska P, Vartiainen E, Miettinen TA: Serum sterols during stanol ester feeding in a mildly hypercholesterolemic population. J Lipid Res. 1999, 40: 593-600.
Hallikainen M, Lyyra-Laitinen T, Laitinen T, Ågren JJ, Pihlajamäki J, Rauramaa R, Miettinen TA, Gylling H: Endothelial function in hypercholesterolemic subjects: Effects of plant stanol and sterol esters. Atherosclerosis. 2006, 188: 425-432. 10.1016/j.atherosclerosis.2005.11.012
Hallikainen MA, Sarkkinen ES, Uusitupa MIJ: Plant stanol esters affect serum cholesterol concentrations of hypercholesterolemic men and women in a dose-dependent manner. J Nutr. 2000, 130: 767-776.
Hallikainen MA, Sarkkinen ES, Gylling H, Erkkilä AT, Uusitupa MI: Comparison of the effects of plant sterol ester and plant stanol ester-enriched margarines in lowering serum cholesterol concentrations in hypercholesterolaemic subjects on a low-fat diet. Eur J Clin Nutr. 2000, 54: 715-725. 10.1038/sj.ejcn.1601083
Raitakari OT, Salo P, Gylling H, Miettinen TA: Plant stanol ester consumption and arterial elasticity and endothelial function. Brit J Nutr. 2008, 100: 603-608. 10.1017/S0007114508922546
Vanhanen HT, Blomqvist S, Ehnholm C, Hyvönen M, Jauhiainen M, Torstila I, Miettinen TA: Serum cholesterol, cholesterol precursors, and plant sterols in hypercholesterolemic subjects with different apoE phenotypes during dietary sitostanol ester treatment. J Lipid Res. 1993, 34: 1535-1544.
Vanhanen HT, Kajander J, Lehtovirta H, Miettinen TA: Serum levels, absorption efficiency, faecal elimination and synthesis of cholesterol during increasing doses of dietary sitostanol esters in hypercholesterolaemic subjects. Clin Sci. 1994, 87: 61-67.
Hallikainen M, Lyyra-Laitinen T, Laitinen T, Moilanen L, Miettinen TA, Gylling H: Effects of plant stanol esters on serum cholesterol concentrations, relative markers of cholesterol metabolism and endothelial function in type 1 diabetes. Atherosclerosis. 2008, 199: 432-439. 10.1016/j.atherosclerosis.2007.10.033
Gylling H, Miettinen TA: Serum cholesterol and cholesterol and lipoprotein metabolism in hypercholesterolaemic NIDDM patients before and during sitostanol ester-margarine treatment. Diabetologia. 1994, 37: 773-780. 10.1007/BF00404334
Miettinen TA: Cholesterol metabolism during ketoconazole treatment in man. J Lipid Res. 1988, 29: 43-51.
Miettinen TA: Gas–liquid chromatographic determination of fecal neutral sterols using a capillary column. Clin Chim Acta. 1982, 124: 245-248. 10.1016/0009-8981(82)90393-X
Knuts L-R, Rastas M, Haapala P: Micro-Nutrica. Version 1.0. 1991, Helsinki, Finland: Social Insurance Institution.
Vuoristo M, Miettinen TA: Absorption, metabolism, and serum concentrations of cholesterol in vegetarians: effects of cholesterol feeding. Am J Clin Nutr. 1994, 59: 1325-1331.
Björkhem I, Boberg KM, Leitersdorf E: Inborn errors in bile acid biosynthesis and storage of sterols other than cholesterol. The Metabolic and Molecular Bases of Inherited Disease. Edited by: Scriver CS, Beaudet AL, Sly WS, Valle D. 2001, 2961-2988. New York: McGraw-Hill.
Gylling H, Vuoristo M, Färkkila M, Miettinen TA: The metabolism of cholestanol in primary biliary cirrhosis. J Hepatol. 1996, 24: 444-451. 10.1016/S0168-8278(96)80165-6
Miettinen TA, Gylling H: Non-nutritive bioactive constituents of plants: phytosterols. Internat J Vit Nutr Res. 2003, 73: 127-134. 10.1024/0300-9831.73.2.127.
Acknowledgements
The study was supported by Raisio Nutrition Ltd (CL2009_019).
This study is dedicated to the memory of Professor Tatu A. Miettinen.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
HG has received research funding from Raisio Group, Finland. MH and PS declare no competing interests.
Authors’ contributions
MH collected the data, performed the statistical analysis and drafted the first version of the manuscript. MH, PS, and HG critically revised the manuscript and approved the final version.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Hallikainen, M., Simonen, P. & Gylling, H. Cholesterol metabolism and serum non-cholesterol sterols: summary of 13 plant stanol ester interventions. Lipids Health Dis 13, 72 (2014). https://doi.org/10.1186/1476-511X-13-72
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-511X-13-72