
Abstract
Background
Although a few studies have been conducted, it is still unclear whether the apolipoprotein E (APOE) polymorphism is associated with maximal oxygen uptake (VO2max) after exercise training. The objective of this study was to examine if the APOE gene polymorphisms affect VO2max after exercise training in Chinese young adult.
Methods
A total of 360 Chinese young adult (180 male and 180 female) were recruited into this gender-specific cohorts. Anthropometrics, serum lipids, and VO2max were measured pre and post 6 months of supervised exercise training. Polymerase chain reaction restriction fragment length polymorphism (PCR-RFLP) assay was applied to assess the APOE gene polymorphisms.
Results
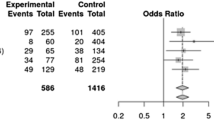
VO2max after exercise training increased significantly higher in carriers of E2/E3 in male [odds ratio (OR) =0.68, 95% confidence interval (CI) = 0.04, 1.32; P = 0.04] and female (OR =0.62, 95% CI = 0.05, 1.18; P = 0.03). VO2max after exercise training increased significantly higher in carriers of E3/E4 in male (OR =0.60, 95% CI = 0.09, 1.11; P = 0.02) and female (OR =0.62, 95% CI = 0.09, 1.15; P = 0.02). No significant differences were found in carriers of E2/E2, E2/E4, E3/E3, E4/E4 in either male nor female.
Conclusion
Our study found that APOE gene polymorphism was associated with VO2max levels after exercise training in Chinese young adult. In the future, further experiments will be necessary to confirm this finding and to find the possible mechanism.
Similar content being viewed by others


Introduction
Physical performance is a complex phenotype influenced by both environmental and genetic factors[1]. Great attention is paid to searching genes underlying athletic performance and variants predisposing to certain sport disciplines[1–4]. Changes in serum lipids with exercise training are often small and individually variable, limiting the role of exercise in treating lipid abnormalities[5]. Maximal oxygen uptake (VO2max) is traditionally recognized as the gold standard laboratory measure of cardio respiratory fitness, with increasing levels accompanying endurance training and high levels being a pre-requisite for success in endurance events[6].
Apolipoprotein E (apoE), a 299-amino acid, arginine-rich glycoprotein, is an integral surface component of chylomicrons, very-low-density lipoproteins (VLDL), and some subclasses of high-density lipoproteins (HDL). The APOE gene, encoded on chromosome 19, exists in three isoforms: E2, E3, and E4, giving six possible genotypes (E2/E2, E2/E3, E2/E4, E3/E3, E3/E4 and E4/E4)[7–9]. APOE gene polymorphisms seem to have some impact among patients with cardiovascular disease[10–12].
Although a few studies have been conducted, it is still unclear whether the APOE polymorphism is associated with VO2max after exercise training[13, 14]. The objective of this study was to examine if the APOE gene polymorphisms affect VO2max after exercise training in Chinese young adult.
Materials and methods
Study population
A total of 360 Chinese young adult (180 male and 180 female) were recruited into this gender-specific cohorts during the years 2012 to 2013 from Shanghai University of Sport, China. Anthropometrics, serum lipids, and VO2max were measured pre and post 6 months of supervised exercise training. Eligibility criteria included requirements for participants to be healthy, physically inactive, 18–40 years old, to pass a physician-administered physical examination, and to have no significant electrocardiographic abnormalities during a cycle ergometer maximal exercise test. Subjects were considered physically inactive if they participated in vigorous activity fewer than 4 times per month for the prior 6 months. Exclusion criteria included diabetes mellitus, hypertension, hyperlipidemia, or a body mass index (BMI) exceeding 30 kg/m2. Subjects underwent a progressive, supervised exercise training program. Subjects exercised between 60% and 85% of their VO2max based on their predetermined maximal heart rate. VO2max was defined as the average of the 2 highest consecutive 30-second values at peak exercise. Treadmill exercise was the primary mode of training. Subjects were requested to maintain their usual dietary composition throughout the study. The Ethical Committee of the Shanghai University of Sport approved the study protocols, and all participants gave written informed consent according to the Declaration of Helsinki. Each subject received an incremental honorarium for successful completion of the study.
DNA extraction and genotyping
Venous blood samples were collected in EDTA-containing tubes from each participant. DNA was extracted from peripheral blood leukocytes using the phenol-chloroform method. Polymerase chain reaction restriction fragment length polymorphism (PCR-RFLP) assay was applied to assess the APOE gene polymorphisms. Based on the GenBank reference sequence, the PCR primers were as follows: sense, ACAGAATTCGCCCCGGCCTGGTACAC; antisense, TAAGCTTGGCACGGCTGTCCAAGGA. The amplified PCR products were then digested with 2U of Hha I (New England BioLabs, Missisauga, ON, Canada) at 37°C for 3 hours. The resulting DNA fragments were electrophoresed on 3.5% agarose gel and visualized under UV light after ethidum staining.
Statistical analysis
All analyses were performed with Statistical Analyses System (SAS) package (version 8.01; SAS Institute, Cary, NC). Univariate analyses of variance were used to compare APOE groups for differences at baseline and differences in their responses to exercise training. The P value of statistical significance was adjusted by Fisher’s exact test where appropriate. A P-value was considered significant at a level of < 0.05. We calculated crude and adjusted odds ratios (OR) and 95% confidence intervals (CI) for the association between the APOE genotypes and VO2max after exercise training. A chi-square test was used to confirm that the APOE genotype frequencies were in Hardy-Weinberg equilibrium.
Results
The demographical and physiological characteristics of the participants were showed in Table 1. The mean age was 32.8 (±11.9) years for the male and 31.0 (±12.0) years for the female. The body weight was 75.1 (±15.8) kg for the male and 69.7 (±13.1) kg for the female. The BMI was 25.4 (±5.6) kg/m2 for the male and 26.0 (±6.2) kg/m2 for the female. The waist-to-hip ratio (WHR) was 0.81 (±0.08) for the male and 0.75 (±0.06) for the female. The VO2max was 2.62 (±0.51) L/min or 34.9 (±6.8) mL/kg/min for the male and 1.85 (±0.36) L/min or 26.5 (±5.2) mL/kg/min for the female. The total cholesterol (TC) was 171.4 (±6.4) mg/dL for the male and 163.5 (±5.7) mg/dL for the female. The low-density lipoprotein (LDL-C) was 116.1 (±4.8) mg/dL for the male and 112.2 (±4.1) mg/dL for the female. The HDL-C was 45.1 (±1.6) mg/dL for the male and 49.2 (±1.8) mg/dL for the female. The VLDL-C was 10.2 (±0.7) mg/dL for the male and 12.1 (±0.8) mg/dL for the female. The triglycerides (TG) was 106.5 (±13.2) mg/dL for the male and 89.7 (±10.2) mg/dL for the female (Table 1).
VO2max after exercise training increased significantly higher in carriers of E2/E3 in male (OR =0.68, 95% CI = 0.04, 1.32; P = 0.04) and female (OR =0.62, 95% CI = 0.05, 1.18; P = 0.03) (Tables 2 and3). VO2max after exercise training increased significantly higher in carriers of E3/E4 in male (OR =0.60, 95% CI = 0.09, 1.11; P = 0.02) and female (OR =0.62, 95% CI = 0.09, 1.15; P = 0.02) (Tables 2 and3). No significant differences were found in carriers of E2/E2, E2/E4, E3/E3, E4/E4 in either male nor female.
Discussion
A lot of studies have been conducted to examine the association of genetic polymorphism and athletic performance. A recent study found that genetic variants of uncoupling proteins-2 and -3 were associated with VO2max in different sports[1]. A study in 323 Russian athletes and 467 nonathletic controls found that monocarboxylate transporter 1 gene A1470T polymorphism was associated with VO2max[15]. A cohort of 67 Chinese men in Singapore suggested that the angiotensin-converting enzyme (ACE) DD genotype in young adult Chinese males was associated with higher levels of VO2max[16]. The ACE I/D polymorphism altered the response of muscle energy supply lines to exercise[17]. AKT1 G205T genotype influenced obesity-related metabolic phenotypes and their responses to aerobic exercise training in older Caucasians[18]. The Genathlete cohort found preliminary evidence that the hypoxia-inducible factor-1alpha Pro582Ser polymorphism may be associated with elite endurance athletes in Caucasian men[19]. A study in 1,423 Russian athletes and 1,132 controls suggested that the likelihood of becoming an elite endurance athlete depended on the carriage of a high number of endurance-related alleles[20]. The A2962G polymorphism of the peroxisome proliferator-activated receptor gamma coactivator 1 alpha (PPARGC1A) gene was associated with VO2max at baseline, as carriers of the G allele had higher levels of VO2max than the AA group endurance capacity in Chinese men[21]. The HERITAGE Family Study found that peroxisome proliferator-activated receptor-delta (PPARdelta) polymorphisms were associated with physical performance and plasma lipids[22].
The APOE gene polymorphisms were associated with diseases of the respiratory system and cardiovascular disease. Small lung volumes were prospectively associated with an increased risk for poor cognitive function and dementia in non-carriers of the APOE E4[23]. Studies in transgenic mice showed that alpha-tocopherol transport in the lung was affected by the APOE genotype[24]. APOE E4 and cardiorespitatory fitness could interact to influence child adiposity in 8-year-old children from the Tasmanian Infant Health Survey[25]. Although meta-analyses suggest that APOE E4 carriers may have a 40–50% increased coronary artery disease risk, the associations reported in individual studies are highly heterogeneous[26]. In the Tunisian population the APOE E4 appears to be only indirectly involved in the severity of cardiovascular disease[27]. Although the prevalence of the APOE E4 allele is generally low, there are areas with higher prevalence of the APOE E4 allele and a higher incidence of adult ischemic heart disease mortality in Spain[28]. An autopsy study suggested that the risk of developing and dying from cardiovascular disease, including coronary heart disease and cerebrovascular disease, was influenced by the APOE polymorphism[29]. The APOE E2 genotype might contribute to increased risk of cardiovascular complications in subjects with acromegaly[30]. The APOE genotype predicted cardiovascular endpoints in dialysis patients with type 2 diabetes mellitus[31]. A meta-analysis of 45 studies including 13,940 cases and 16,364 controls found that APOE gene polymorphisms were associated with essential hypertension[32].
How did the APOE gene polymorphisms affect VO2max after exercise training? The exact mechanism behind it is still unclear. There is animal evidence that Apo E can affect exercise performance[33]. Controversy exists as to relationship of APOE polymorphism to the blood lipid response to exercise[34, 35]. It was unlikely to explain the present results. Apo E mRNA is expressed in skeletal muscle and appears to be most abundant at neuromuscular junctions[36]. Therefore the effect of APOE genotype on exercise capacity may have been mediated by more direct effects on other tissues such as skeletal muscle[14].
There are some limitations to the present study that should be noted. First of all, the present study lacked a control group, since this is a self-control study. Second, the sample size of this study is relatively small, which may not have enough statistical power to explore the real association. Third, we cannot exclude the possibility that some other genetic factor associated with APOE variants is responsible for the differences in the VO2max response. Finally, these results should be interpreted with caution because the population was only from China, which reduces the possibility of confounding from ethnicity, so it does not permit extrapolation of the results to other ethnic groups.
Conclusion
In conclusion, our study found that APOE gene polymorphism was associated with VO2max levels after exercise training in Chinese young adult. In the future, further experiments will be necessary to confirm this finding and to find the possible mechanism.
Authors’ information
Bo Yu and Wenhua Chen are joint first authors.
References
Holdys J, Gronek P, Krysciak J, Stanislawski D: Genetic variants of uncoupling proteins-2 and -3 in relation to maximal oxygen uptake in different sports. Acta Biochim Pol. 2013, 60: 71-75.
Bray MS, Hagberg JM, Perusse L, Rankinen T, Roth SM, Wolfarth B, Bouchard C: The human gene map for performance and health-related fitness phenotypes: the 2006–2007 update. Med Sci Sports Exerc. 2009, 41: 35-73.
Peeters MW, Thomis MA, Beunen GP, Malina RM: Genetics and sports: an overview of the pre-molecular biology era. Med Sport Sci. 2009, 54: 28-42.
Lippi G, Longo UG, Maffulli N: Genetics and sports. Br Med Bull. 2010, 93: 27-47. 10.1093/bmb/ldp007
Tran ZV, Weltman A: Differential effects of exercise on serum lipid and lipoprotein levels seen with changes in body weight. A meta-analysis. JAMA. 1985, 254: 919-924. 10.1001/jama.1985.03360070057023
Bassett DR, Howley ET: Limiting factors for maximum oxygen uptake and determinants of endurance performance. Med Sci Sports Exerc. 2000, 32: 70-84.
Mahfouz RA, Sabbagh AS, Zahed LF, Mahfoud ZR, Kalmoni RF, Otrock ZK, Taher AT, Zaatari GS: Apolipoprotein E gene polymorphism and allele frequencies in the Lebanese population. Mol Biol Rep. 2006, 33: 145-149. 10.1007/s11033-006-6260-x
Laskowitz DT, Horsburgh K, Roses AD: Apolipoprotein E and the CNS response to injury. J Cereb Blood Flow Metab. 1998, 18: 465-471.
Boulenouar H, Mediene Benchekor S, Meroufel DN, Lardjam Hetraf SA, Ouhaibi Djellouli H, Hermant X, Grenier-Boley B, Hamani Medjaoui I, Saidi Mehtar N, Amouyel P, Houti L, Meirhaeghe A, Goumidi L: Impact of APOE gene polymorphisms on the lipid profile in an Algerian population. Lipids Health Dis. 2013, 12: 155- 10.1186/1476-511X-12-155
Eichner JE, Dunn ST, Perveen G, Thompson DM, Stewart KE, Stroehla BC: Apolipoprotein E polymorphism and cardiovascular disease: a HuGE review. Am J Epidemiol. 2002, 155: 487-495. 10.1093/aje/155.6.487
Loktionov A, Vorster H, O’Neill IK, Nell T, Bingham SA, Runswick SA, Cummings JH: Apolipoprotein E and methylenetetrahydrofolate reductase genetic polymorphisms in relation to other risk factors for cardiovascular disease in UK Caucasians and Black South Africans. Atherosclerosis. 1999, 145: 125-135. 10.1016/S0021-9150(99)00022-2
Smalinskiene A, Petkeviciene J, Luksiene D, Jureniene K, Klumbiene J, Lesauskaite V: Association between APOE, SCARB1, PPARalpha polymorphisms and serum lipids in a population of Lithuanian adults. Lipids Health Dis. 2013, 12: 120- 10.1186/1476-511X-12-120
Leon AS, Togashi K, Rankinen T, Despres JP, Rao DC, Skinner JS, Wilmore JH, Bouchard C: Association of apolipoprotein E polymorphism with blood lipids and maximal oxygen uptake in the sedentary state and after exercise training in the HERITAGE family study. Metabolism. 2004, 53: 108-116. 10.1016/j.metabol.2003.08.013
Thompson PD, Tsongalis GJ, Seip RL, Bilbie C, Miles M, Zoeller R, Visich P, Gordon P, Angelopoulos TJ, Pescatello L, Bausserman L, Moyna N: Apolipoprotein E genotype and changes in serum lipids and maximal oxygen uptake with exercise training. Metabolism. 2004, 53: 193-202. 10.1016/j.metabol.2003.09.010
Fedotovskaya ON, Mustafina LJ, Popov DV, Vinogradova OL, Ahmetov II: A common polymorphism of the MCT1 gene and athletic performance. Int J Sports Physiol Perform. 2014, 9: 173-180. 10.1123/IJSPP.2013-0026
Zhao B, Moochhala SM, Tham S, Lu J, Chia M, Byrne C, Hu Q, Lee LK: Relationship between angiotensin-converting enzyme ID polymorphism and VO(2max) of Chinese males. Life Sci. 2003, 73: 2625-2630. 10.1016/S0024-3205(03)00608-8
Vaughan D, Huber-Abel FA, Graber F, Hoppeler H, Fluck M: The angiotensin converting enzyme insertion/deletion polymorphism alters the response of muscle energy supply lines to exercise. Eur J Appl Physiol. 2013, 113: 1719-1729. 10.1007/s00421-012-2583-6
McKenzie JA, Witkowski S, Ludlow AT, Roth SM, Hagberg JM: AKT1 G205T genotype influences obesity-related metabolic phenotypes and their responses to aerobic exercise training in older Caucasians. Exp Physiol. 2011, 96: 338-347. 10.1113/expphysiol.2010.055400
Doring F, Onur S, Fischer A, Boulay MR, Perusse L, Rankinen T, Rauramaa R, Wolfarth B, Bouchard C: A common haplotype and the Pro582Ser polymorphism of the hypoxia-inducible factor-1alpha (HIF1A) gene in elite endurance athletes. J Appl Physiol. 2010, 108: 1497-1500. 10.1152/japplphysiol.01165.2009
Ahmetov II, Williams AG, Popov DV, Lyubaeva EV, Hakimullina AM, Fedotovskaya ON, Mozhayskaya IA, Vinogradova OL, Astratenkova IV, Montgomery HE, Rogozkin VA: The combined impact of metabolic gene polymorphisms on elite endurance athlete status and related phenotypes. Hum Genet. 2009, 126: 751-761. 10.1007/s00439-009-0728-4
He Z, Hu Y, Feng L, Bao D, Wang L, Li Y, Wang J, Liu G, Xi Y, Wen L, Lucia A: Is there an association between PPARGC1A genotypes and endurance capacity in Chinese men?. Scand J Med Sci Sports. 2008, 18: 195-204.
Hautala AJ, Leon AS, Skinner JS, Rao DC, Bouchard C, Rankinen T: Peroxisome proliferator-activated receptor-delta polymorphisms are associated with physical performance and plasma lipids: the HERITAGE Family Study. Am J Physiol Heart Circ Physiol. 2007, 292: H2498-H2505. 10.1152/ajpheart.01092.2006
Giltay EJ, Nissinen A, Giampaoli S, Kromhout D: Apolipoprotein E genotype modifies the association between midlife lung function and cognitive function in old age. Dement Geriatr Cogn Disord. 2009, 28: 433-441. 10.1159/000255600
Huebbe P, Jofre-Monseny L, Rimbach G: Alpha-tocopherol transport in the lung is affected by the apoE genotype–studies in transgenic apoE3 and apoE4 mice. IUBMB Life. 2009, 61: 453-456. 10.1002/iub.177
Ellis JA, Ponsonby AL, Pezic A, Williamson E, Cochrane JA, Dickinson JL, Dwyer T: APOE genotype and cardio-respiratory fitness interact to determine adiposity in 8-year-old children from the Tasmanian Infant Health Survey. PLoS One. 2011, 6: e26679- 10.1371/journal.pone.0026679
Minihane AM, Jofre-Monseny L, Olano-Martin E, Rimbach G: ApoE genotype, cardiovascular risk and responsiveness to dietary fat manipulation. Proc Nutr Soc. 2007, 66: 183-197. 10.1017/S0029665107005435
Bahri R, Esteban E, Moral P, Hassine M, Ben Hamda K, Chaabani H: Apolipoprotein gene polymorphisms and plasma levels in healthy Tunisians and patients with coronary artery disease. Lipids Health Dis. 2008, 7: 46- 10.1186/1476-511X-7-46
Garces C, Cantos M, Benavente M, Granizo JJ, Cano B, Viturro E, De Oya M: Variations in APOE genotype distribution in children from areas with different adult cardiovascular disease mortality in Spain. Hum Biol. 2004, 76: 615-621. 10.1353/hub.2004.0055
Kumar NT, Liestol K, Loberg EM, Reims HM, Brorson SH, Maehlen J: The apolipoprotein E polymorphism and cardiovascular diseases–an autopsy study. Cardiovasc Pathol. 2012, 21: 461-469. 10.1016/j.carpath.2012.02.005
Bozok Cetintas V, Zengi A, Tetik A, Karadeniz M, Ergonen F, Kucukaslan AS, Tamsel S, Kosova B, Sahin SB, Saygili F, Eroglu Z: Does Apolipoprotein E genotype affect cardiovascular risk in subjects with acromegaly?. Endocrine. 2012, 41: 465-472. 10.1007/s12020-011-9585-8
Winkler K, Hoffmann MM, Krane V, Marz W, Drechsler C, Wanner C: Apolipoprotein E genotype predicts cardiovascular endpoints in dialysis patients with type 2 diabetes mellitus. Atherosclerosis. 2010, 208: 197-202. 10.1016/j.atherosclerosis.2009.06.036
Stoumpos S, Hamodrakas SJ, Anthopoulos PG, Bagos PG: The association between apolipoprotein E gene polymorphisms and essential hypertension: a meta-analysis of 45 studies including 13, 940 cases and 16, 364 controls. J Hum Hypertens. 2013, 27: 245-255. 10.1038/jhh.2012.37
Maxwell AJ, Schauble E, Bernstein D, Cooke JP: Limb blood flow during exercise is dependent on nitric oxide. Circulation. 1998, 98: 369-374. 10.1161/01.CIR.98.4.369
Taimela S, Lehtimaki T, Porkka KV, Rasanen L, Viikari JS: The effect of physical activity on serum total and low-density lipoprotein cholesterol concentrations varies with apolipoprotein E phenotype in male children and young adults: The Cardiovascular Risk in Young Finns Study. Metabolism. 1996, 45: 797-803. 10.1016/S0026-0495(96)90149-3
St-Amand J, Prud’homme D, Moorjani S, Nadeau A, Tremblay A, Bouchard C, Lupien PJ, Despres JP: Apolipoprotein E polymorphism and the relationships of physical fitness to plasma lipoprotein-lipid levels in men and women. Med Sci Sports Exerc. 1999, 31: 692-697. 10.1097/00005768-199905000-00011
Akaaboune M, Villanova M, Festoff BW, Verdiere-Sahuque M, Hantai D: Apolipoprotein E expression at neuromuscular junctions in mouse, rat and human skeletal muscle. FEBS Lett. 1994, 351: 246-248. 10.1016/0014-5793(94)00871-X
Acknowledgements
This study was supported by Key Laboratory of Exercise and Health Sciences (Shanghai University of Sport), Ministry of Education. Thanks are expressed to all coinvestigators, local project coordinators, research assistants, laboratory technicians, and secretaries/administrative assistants.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that they have no competing interests.
Authors’ contributions
BY and WC carried out the molecular genetic studies and drafted the manuscript. RW and QQ carried out the genotyping. KL and WZ participated in the design of the study and performed the statistical analysis. BY, WC and HW conceived of the study, and participated in its design and coordination and helped to draft the manuscript. All authors read and approved the final manuscript.
Bo Yu, Wenhua Chen contributed equally to this work.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Yu, B., Chen, W., Wang, R. et al. Association of apolipoprotein E polymorphism with maximal oxygen uptake after exercise training: a study of Chinese young adult. Lipids Health Dis 13, 40 (2014). https://doi.org/10.1186/1476-511X-13-40
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-511X-13-40