
Abstract
Background
High consumption of fish carries a lower risk of cardiovascular disease as a consequence of dietary omega-3 long chain polyunsaturated fatty acid (n-3 PUFA; especially EPA and DHA) content. A controversy exists about the component/s responsible of these beneficial effects and, in consequence, which is the best proportion between both fatty acids. We sought to determine, in healthy Wistar rats, the proportions of EPA and DHA that would induce beneficial effects on biomarkers of oxidative stress, and cardiovascular disease risk.
Methods
Female Wistar rats were fed for 13 weeks with 5 different dietary supplements of oils; 3 derived from fish (EPA/DHA ratios of 1:1, 2:1, 1:2) plus soybean and linseed as controls. The activities of major antioxidant enzymes (SOD, CAT, GPX, and GR) were determined in erythrocytes and liver, and the ORAC test was used to determine the antioxidant capacity in plasma. Also measured were: C reactive protein (CRP), endothelial dysfunction (sVCAM and sICAM), prothrombotic activity (PAI-1), lipid profile (triglycerides, cholesterol, HDLc, LDLc, Apo-A1, and Apo-B100), glycated haemoglobin and lipid peroxidation (LDL-ox and MDA values).
Results
After three months of nutritional intervention, we observed statistically significant differences in the ApoB100/ApoA1 ratio, glycated haemoglobin, VCAM-1, SOD and GPx in erythrocytes, ORAC values and LDL-ox. Supplementation with fish oil derived omega-3 PUFA increased VCAM-1, LDL-ox and plasma antioxidant capacity (ORAC). Conversely, the ApoB100/ApoA1 ratio and percentage glycated haemoglobin decreased.
Conclusions
Our results showed that a diet of a 1:1 ratio of EPA/DHA improved many of the oxidative stress parameters (SOD and GPx in erythrocytes), plasma antioxidant capacity (ORAC) and cardiovascular risk factors (glycated haemoglobin) relative to the other diets.
Similar content being viewed by others

Background
Diets with high fish content have been associated with a low cardiovascular disease (CVD) risk. Of particular note are the n-3 polyunsaturated fatty acids (n-3 PUFA): eicosapentaenoic acid (EPA, 20:5 n-3) and docosahexaenoic acid (DHA, 22:6 n-3).
Fish are the major food sources of DHA and EPA and are carried in the circulation as triglycerides, especially phospholipids [1]. There are several experimental studies that show that the n-3 PUFA perform several functions in relation to the structure and function of the membrane, tissue metabolism, and gene regulation [2]. These fatty acids play important roles in reducing hypertriglyceridaemia [3, 4], low density lipoprotein cholesterol (LDLc), very low density lipoprotein cholesterol (VLDLc), and increasing high density lipoprotein cholesterol (HDLc) concentrations [5] as well as various components of these molecules e.g. ApoA1 and ApoB100 of HDL and LDL/VLDL respectively. EPA and DHA improve hypertension [6], insulin sensitivity and glycaemia [7]. Oxidative stress and vascular endothelial dysfunction also play a critical role in the pathogenesis of CVD. Increased oxidative stress underlies the pathophysiology of hypertension and atherosclerosis by directly affecting the cells of the vascular wall [8]. Higher levels of soluble intercellular adhesion molecule-1 (sICAM-1) and soluble vascular cell adhesion molecule-1 (sVCAM-1) have been associated with an increased risk of ischaemic disease and peripheral artery disease mediated, in part, by C reactive protein (CRP) [9]. Type 1 plasminogen activator inhibitor (PAI-1) is also related to metabolic syndrome, obesity, and CVD [5].
The amount of n-3 PUFA necessary to provide health benefits is unknown [10] as are the proportions of EPA and DHA that provide the greatest benefit. The majority of the clinical studies carried-out to date use fish-oil derived dietary supplements, but with a higher EPA/DHA ratio than that commonly found in the fish themselves [11, 12], and it would not trigger the effects in vivo compared to the ratio contained in fish. EPA and DHA derived from fish oils have demonstrable cardiovascular disease benefits in observational studies and experimental trials which, mainly, have investigated their effects in combination. As such, little is known of the potentially different effects of EPA and DHA, especially regarding which has the better protective effect on CVD [2].
Hence, our present study seeks to determine the proportion of EPA/DHA that is best able to achieve a protective effect of the n-3 PUFA on CVD risk factors. Three dietary interventions with the optimal relation n-3/n-6 and different EPA/DHA ratios (1:1, 2:1, 1:2) were evaluated in a healthy animal model. Soybean and linseed oils were used as control diets. Soybean is a rich source of linoleic acid (LA, 18:2 n-6), while linseed oil has an elevated content of alpha-linolenic acid (ALA, 18:3 n-3) [13]. Parameters of oxidative stress, inflammation, endothelial dysfunction, prothrombotic state, protein glycation, lipid peroxidation, and lipid profile were determined as risk factors or biomarkers indicative of CVD risk.
Results
Anthropomorphic measures
None of the nutritional interventions, irrespective of the proportions of EPA/DHA (1:1, 2:1, 1:2) or soybean or linseed oil supplements, significantly increased the weight of the animals (260.3 ± 11; 259.3 ± 12; 255.5 ± 10; 259.1 ± 8; 266.3 ± 9, respectively). Abdominal fat tissue, as a percentage of overall body weight, was not significantly different in test diets compared to that of the animals on the control diets (3.89 ± 1.2; 3.62 ± 0.8; 4.12 ± 0.7; 4.3 ± 0.7; 4.2 ± 0.9, respectively).
Antioxidant status and oxidative stress
The biomarkers of antioxidant status and oxidative stress are summarised in Table 1.
The concentrations of antioxidant enzymes in erythrocytes indicated an activation of these enzymes in fish-oil diets.
SOD values were higher in 1:1 EPA/DHA diet followed by 2:1 EPA/DHA, compared to the other 3 diets. GPx values were also higher in 1:1 and 2:1 EPA/DHA. There was a trend, albeit not statistically significant, towards higher CAT and lower GR values in fish-oil diets compared to the control diets.
These results indicated that fish-oil diets, especially 1:1 and 2:1 EPA/DHA, had improved values of antioxidant enzymes than did soybean and linseed oils.
The two control diets (soybean and linseed) had no significant differences between them with respect to the values of erythrocyte antioxidant enzymes.
Finally, the plasma antioxidant capacity (ORAC) was significantly higher in the 1:1 diet than in the other diets. This result is in agreement with the high SOD and GPx values found in this supplemented group.
Lipid peroxidation
The mean LDL-ox values indicated higher oxidation in fish-oil diets than controls. LDL-ox of diets with 2:1 and 1:2 EPA/DHA ratios were significantly higher, compared to soybean and linseed diets. The EPA/DHA (1:1) group did not show significant differences with respect to control groups (Table 1).
Mean values of MDA in the liver were not significantly different between groups.
Lipid profile
TG, CHOL, LDLc, HDLc, LDLc/HDLc, Apo A1 and Apo B100 were not statistically significantly different between supplemented groups (Table 2).
TG, LDLc and HDLc values were within the reference ranges observed in other studies [14, 15], whereas CHOL concentrations were increased in all the groups compared to that observed by Levy et al. [14].
The linseed-oil diet group had significantly higher values of the ApoB100/ApoA1 ratio, compared to the 1:1, 2:1 and the soybean-oil diets.
Glycaemia control and insulin resistance
The post-intervention glucose concentrations were within the laboratory reference range in all the groups at <14 mM [16, 17], but the glucose decreases obtained at the end of the experiment were greater in 1:1 and 2:1 EPA/DHA with respect to the other diets (Table 2).
All EPA/DHA diets showed significantly lower values of glycated haemoglobin, relative to the linseed and soybean oil diets. Glycated haemoglobin concentrations were not significantly different among the 3 EPA/DHA diets (Table 2).
The initial concentrations of insulin were within reference range values (3.5 – 4.4 ng/mL) described by other authors [17, 18] in all groups (results not shown). The insulin increases observed at the end of the experiment were not significantly different relative to the baseline values, and without differences between groups (Table 2).
Following nutritional intervention, the Wistar rats had HOMA values within laboratory reference ranges (<14) described by other authors [19]. The linseed group had significantly lower values compared to the EPA/DHA 1:1 and soybean supplemented groups (Table 2).
Cardiovascular disease risk biomarkers
Linseed diet decreased the sVCAM significantly with respect to the fish-oil diets while the 2:1 diet had significantly lower values than 1:2 diet (Table 3). The soybean group had lower values of PAI-1 than the 1:2 EPA/DHA group. No statistically significant differences were observed between the two control diets with respect to these biomarkers (Table 3).
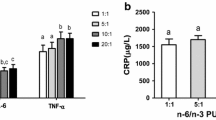
No significant differences were observed in CRP and in sICAM concentrations.
Discussion
Apart from the n-3 PUFA, fish oils contain aminoacids, vitamins, selenium and other minerals which contribute to the cardiovascular benefit. The majority of studies with purified EPA or DHA have demonstrated the bioactivity and effectiveness of these fatty acids; the implication being that the substantial CVD benefit of fish oil consumption is related to the n-3 PUFA content [2]. In our study, the supplemented dose of fish oils (extrapolated to animals) provides approximately double the amount of EPA and DHA of the European Union’s recommendation for the maintenance of normal blood concentration of triglycerides in adults [20].
Soybean and linseed oils were used as control diets. Soybean is a rich source of linoleic acid (LA, 18:2 n-6), while linseed oil has an elevated content of alpha-linolenic acid (ALA, 18:3 n-3) [13].
However, all diets had a similar fat and energy content and, hence, the observed differences can be attributed to the different ratios of EPA and DHA.
Moreover, the reasoning for using a weekly administration of the oils was because in a previous test; the daily feed became very stressing for animals. According to that, it was decided a weekly doses as has been already described in the article of Méndez et al. [13].
The influence of dietary interventions on the levels and composition of plasmatic FFA was also evaluated previously in a recently reported [13] in which we demonstrated that fish oil supplementation did not change the total amount of plasmatic FFA, but it altered the profile of the individual FFA. Animals fed fish oils exhibited significantly higher levels of EPA (20:5 n-3) and DHA (22:6 n-3) compared to those fed soybean oil. The supplementation with linseed oil provided similar levels of EPA compared to those observed in the FFA fraction from animals supplemented with fish oil; however, the amount of DHA in the FFA fraction was intermediate between those supplemented with fish and those with soybean oils. Animals fed linseed oil showed the highest amount of free LA (18:3 n-3), in agreement with the elevated content of LA in the linseed oil [13].
Oxidative stress
Fatty acids with a greater degree of unsaturation in their molecular structure are more easily oxidised. As a consequence, diets rich in fish-oils are predisposed to causing increased oxidative damage in humans and animals. However, other studies have shown that diets supplemented with fish oils do not increase cellular oxidative damage, but may even exert an antioxidant effect [21, 22].
Our results indicate that improvement in activity of SOD and GPX may explain the higher plasma antioxidant capacity (ORAC) in the EPA/DHA 1:1 supplemented group. In other study, n-3 PUFA diet corrected the decreased ORAC values in diabetic rats, and was probably due to the increased erythrocyte antioxidant enzymes SOD and GPX [11]. Our results corroborate this hypothesis.
Further, these results concur with those recently reported [13] in which we demonstrated that fish-oils, especially EPA:DHA 1:1, averted protein carbonylation in plasma and liver. All these findings favour diets rich in EPA and DHA with respect to antioxidant enzymes; the proportion of 1:1 having a higher relevance than others.
Lipid peroxidation
To date, fish-oil supplements have not been unequivocally shown to prevent oxidation of LDL particles [23]. In our study, plasma oxidised LDL was higher in the groups supplemented with fish-oil n-3 PUFA. However, EPA/DHA 1:1 showed lower values than the other two diets with n-3 PUFA, and significant differences existed only among the groups supplemented with 2:1 and 1:2 diets, relative to soybean and linseed.
LDL-ox was lower in the linseed oil group i.e. the ALA is more effective, in this case, than the administration of EPA and DHA. This is contrary to that which occurs in antioxidant protection and protein oxidation, and may be due to a synergistic effect of ALA i.e. on the one hand having less unsaturated bonds than EPA and DHA and hence less susceptible to oxidative attack while, on the other hand, although the rate of conversion from ALA to EPA and DHA is low in the organism, small quantities of these PUFA can contribute to an increase in the levels of antioxidants that protect LDL.
There were no differences observed in liver MDA among the different groups, despite differences in the consumption of n-3 PUFA. As such, although the diets rich in fish oils do not exercise a clear protection to plasma LDL oxidation, liver lipoperoxidation were not affected in these groups, relative to the soybean and linseed oil groups.
Few studies have evaluated MDA levels in liver following fish-oil administration, and the results have been contradictory. While some studies concluded that the administration of fish-oil for 2 months decrease MDA in rats with partial hepatectomy [24], other studies demonstrated, following 2 months of nutritional intervention in rats with experimental non-alcoholic fatty liver disease, that fish-oil derived n-3 PUFA increased liver MDA concentrations and promoted severe fatty liver [25]. These differences can be due to the different fatty acid proportions contained in the oils compared to other molecules with antioxidant capacity such vitamins C and E that, as well, affect the redox status of the organism.
Lipid profile
None of the supplementations increased body-weight and the amount of abdominal fatty tissue of the animals. We need to bear in mind that the intake of total fat was the same in all groups of animals. There were trends, albeit not statistically significant, towards a decrease in triglycerides, total cholesterol, LDLc and ApoB100 in the group supplemented with EPA/DHA 1:1 diet, relative to the other groups. Decreases in these factors would support a CVD protective role for EPA/DHA 1:1 diet.
The Apo B100/Apo A1 ratio was significantly reduced by 1:1, 2:1 and soybean diets, compared to supplementation with linseed oil. Soybean and fish-oil PUFA reduce the risk of cardiovascular disease, essentially by improving the lipid profile, as has been shown by other studies [3, 5].
Glycaemia control and insulin resistance
Fish-oils are reported to be especially efficient in improving glycated haemoglobin concentrations in the circulation. Our study further highlighted that the 1:1 ratio of EPA/DHA induced the most beneficial improvement in this factor.
There is a dearth of physiological data regarding the effect of n-3 PUFA on glucose homeostasis and insulin resistance in healthy rats. Glycated haemoglobin decreased on average by 33% in the groups receiving fish-oil supplements compared to those receiving soybean and linseed diets at the end of the nutritional intervention. This result concurs with those observed by our group on the protective effect of supplementation with EPA/DHA on the carbonylation of proteins [13]. Diets enriched with fish oil decreased protein carbonylation, especially the diet with 1:1 ratio of EPA/DHA. The significant decreases in HbA1c and non-increase in circulating glucose values observed in the study, indicate a beneficial effect of marine-fish-derived long chain n-3 PUFA in healthy animals. These changes would contribute towards the prevention of some diseases such as metabolic syndrome and obesity [5, 7].
In our study, all the groups had values of insulin and HOMA index within the reference range [18, 19, 26]; the linseed diet group showing the lowest values in these parameters. As such, the n-3 PUFA did not provoke increases in plasma insulin in healthy rats.
Conclusions
Our results demonstrate a positive protective effect of fish-oil supplementation in vivo. Specifically, these beneficial protective effects depend on the different proportions of EPA and DHA; the 1:1 proportion of EPA:DHA being the most beneficial since it improved antioxidant status, oxidised LDL, Apo-B100/Apo-A1 ratio, and glycated haemoglobin.
Methods
Animals
This study was conducted in compliance with the norms of the Ethics Committee for Animal Research at the Centro Superior de Investigaciones Científicas, Spain.
Female Wistar rats (n = 35; 13 weeks of age) were purchased from Janvier (Le Genest St-Isle, France) and acclimatised for 8 days prior to the initiation of the study. The animal room was maintained at a temperature of 22 ± 2ºC and 50-60% relative humidity with a 12 h light/dark photoperiod. The animals were fed a standard pellet diet (Panlab A04, Barcelona, Spain) and had free access to bottled water and food, except for a fasting period before sacrifice.
Animals were randomly assigned to five groups (7 rats each).
Supplementation
Three groups had dietary supplements of fish oils containing different proportions of EPA/DHA (1:1, 2:1 and 1:2). The 4th group was fed soybean oil and the 5th with linseed oil. Oils differing in EPA:DHA ratio were obtained by mixing appropriate quantities of the commercial fish oils. Soybean oil, obtained from unrefined organic soy oil (first cold pressing), and linseed oil, obtained from unrefined organic flax oil (first cold pressing). All diets had a similar fat and energy content [13].
Feeding the selected oil involved weekly oral doses of 0.8 mL/Kg bodyweight for 13 weeks, and administered by gavage.
Because of the high predisposition of fish oils to peroxidation, we established quality control to ensure that the oils did not oxidise during the nutritional intervention [13].
At the end of the study, the animals were anaesthetised with ketamine/xylacine (80/10 mg/kg, respectively) by intra-peritoneal injection. The animals were sacrificed by cardiac puncture, and exsanguinated. Plasma, serum and erythrocytes were stored at -80ºC until required for batched analyses. Livers were removed, washed in phosphate buffered saline, weighed, and immediately frozen in liquid nitrogen and stored at -80ºC until required for processing.
Oxidative stress
Antioxidant enzymes in erythrocytes
Superoxide dismutase (SOD) [27], catalase (CAT) [28], glutathione peroxidase (GPx) [29] and glutathione reductase (GR) [30] activities were determined in erythrocytes using standard spectrophotometric methods. The units of measurement for SOD, GPx and GR are expressed as U/g Hb, and as mmol/min/g Hb for CAT.
Plasma antioxidant capacity
Plasma antioxidant capacity was measured as the oxygen radical absorbance capacity (ORAC method) [31]. The assay measures the oxidative degradation of fluorescein after being mixed with free radical generators such as azo-initiator compounds. The units of measurement are μmol trolox-equivalent/mL plasma (μmol TE/mL).
Lipid peroxidation
Liver malondialdehyde (MDA) levels
Liver samples were homogenised in a sodium phosphate buffer (200 mM, pH 6.25) and then ultra-centrifuged (129000 g, 1 h, 4ºC).
Lipid peroxidation was calculated by measuring MDA concentrations using high performance liquid chromatography with fluorescence detection (HPLC-FL). The results are expressed as micrograms of malondialdehyde per gram of liver [32].
Oxidised LDL
Plasma oxidised LDL (LDL-ox) was measured using ELISA kits (CUSABIO BIOTECH, China) according to the manufacturer’s instructions. The units of measurement are expressed as ng/mL.
Cardiovascular disease risk factors
Lipid profile
The lipid profiles consisting of total plasma triglycerides (TG), cholesterol (CHOL), HDL cholesterol (HDLc) and LDL cholesterol (LDLc) were measured by spectrophotometric methods (SPINREACT kits, Spain). ApoA1 and ApoB100 were measured using ELISA kits (CUSABIO BIOTECH, China). The units of measurement are expressed as mg/dL for TG, CHOL, HDLc, LDLc and as mg/mL for APO A1 and APO B100.
Glycaemia control and insulin resistance
Glucose
Animals were fasted for 24 hours and a blood sample taken from the saphenous vein. The capillary blood was spotted on glucose strips and read in the Ascensia Elite XL glucometer (Bayer Consumer Care AG, Basel, Switzerland). The results are expressed in mmol/L.
Glycated haemoglobin
Glycated haemoglobin was measured using a spectrophotometric kit method (SPINREACT, Spain). The units of measurement are expressed as percentage of total haemoglobin.
Insulin
Insulin was measured using an ELISA kit (Millipore Corporation, Billerica, MA, USA). The results are expressed in ng/mL.
HOMA index
HOMA index (Homeostasis Assessment Model) is an estimate of insulin resistance and is calculated as:
Fasting insulin (μU/mL) * fasting glucose (mmol/L) / 22.5.
Biomarkers of cardiovascular disease risk
Plasma CRP, sICAM, sVCAM and PAI-1 were measured by ELISA kits (CUSABIO BIOTECH, China). The results are expressed as μg/mL for CRP, sVCAM and PAI-1 and in ng/mL for sICAM.
Statistical analysis
Results were expressed as means and standard deviations for each group of dietary supplementation. The data were analysed for differences between groups using one-way analysis of variance (ANOVA). The SPSS IBM 19 for Windows was used throughout. When significant differences were found, the means were compared using the Scheffé post-hoc test. Statistical significant was set at p < 0.05.
References
Ackman RG: Biogenic Lipids Fats and Oils. Boca Ratón. 1989, Florida: CRC Press.
Mozaffarian D, Wu JH: (n-3) fatty acids and cardiovascular health: are effects of EPA and DHA shared or complementary?. J Nutr. doi:10.3945/jn.111.149633.
Aguilera AA, Diaz GH, Barcelata ML, Guerrero OA, Ros RM: Effects of fish oil on hypertension, plasma lipids, and tumor necrosis factor-alpha in rats with sucrose induced metabolic syndrome. J Nutr Biochem. 2004, 15: 350-357. 10.1016/j.jnutbio.2003.12.008
Dyerberg J: Platelet - vessel wall interaction: Influence of diet. Philos Trans R Soc Lond B Biol Sci. 1981, 294: 373-381. 10.1098/rstb.1981.0113
Poudyal H, Panchal SK, Diwan V, Brown L: Omega-3 fatty acids and metabolic syndrome: Effects and emerging mechanisms of action. Prog Lipid Res. 2011, 50: 372-387. 10.1016/j.plipres.2011.06.003
Armitage JA, Pearce AD, Sinclair AJ, Vingrys AJ, Weisinger RS, Weisinger HS: Increased blood pressure later in life may be associated with perinatal n-3 fatty acid deficiency. Lipids. 2003, 38: 459-464. 10.1007/s11745-003-1084-y
Sener A, Zhang Y, Bulur N, Louchami K, Malaisse WJ, Carpentier YA: The metabolic syndrome of omega3-depleted rats. II. Body weight, adipose tissue mass and glycemic homeostasis. Int J Mol Med. 2009, 24: 125-129.
Nakazono K, Watanabe N, Matsuno K, Sasaki J, Sato T, Inoue M: Does superoxide underlie the pathogenesis of hypertension?. Proc Natl Acad Sci USA. 1991, 88: 10045-10048. 10.1073/pnas.88.22.10045
Urso C, Hopps E, Caimi G: Adhesion molecules and diabetes mellitus. Clin Ter. 2010, 161: e17-e24.
Dubnov G, Berry EM: Omega-6/omega-3 fatty acid ratio: the Israeli paradox. World Rev Nutr Diet. 2003, 92: 81-91.
Ginty AT, Conklin SM: Preliminary evidence that acute long-chain omega-3 supplementation reduces cardiovascular reactivity to mental stress: a randomized and placebo controlled trial. Biol Psychol. 2012, 89: 269-272. 10.1016/j.biopsycho.2011.09.012
Schuchardt JP, Neubronner J, Kressel G, Merkel M, von Schacky C, Hahn A: Moderate doses of EPA and DHA from re-esterified triacylglycerols but not from ethyl esters lower fasting serum triacylglycerols in statin-treated dyslipidemic subjects: results from a six month randomized controlled trial. Prostaglandins Leukot Essent Fatty Acids. 2011, 85: 381-386. 10.1016/j.plefa.2011.07.006
Méndez L, Pazos M, Gallardo JM, Torres JL, Pérez-Jimenez J, Nogués R, Romeu M, Medina I: Reduced protein oxidation in Wistar rats supplemented with marine ω-3 PUFAs. Free Radic Biol Med. 2013, 55: 8-20.
Levy E, Brunet S, Alvarez F, Seidman E, Bouchard G, Escobar E, Martin S: Abnormal hepatobiliary and circulating lipid metabolism in the Long-Evans Cinnamon rat model of Wilson’s disease. Life Sci. 2007, 80: 1472-1483. 10.1016/j.lfs.2007.01.017
Rusinol AE, Lysak PS, Sigurdson GT, Vance JE: Monomethylethanolamine reduces plasma triacylglycerols and apolipoprotein B and increases apolipoprotein A-I rats without induction of fatty liver. J Lipid Res. 1996, 37: 2296-2304.
Yessoufou A, Soulaimann N, Merzouk SA, Moutairou K, Ahissou H, Prost J, Simonin AM, Merzouk H, Hichami A, Khan NA: N-3 fatty acids modulate antioxidant status in diabetic rats and their macrosomic offspring. Int J Obes (Lond). 2006, 30: 739-750. 10.1038/sj.ijo.0803211. 10.1038/sj.ijo.0803211
El-Seweidy MM, Sadik NA, Shaker OG: Role of sulfurous mineral water and sodium hydrosulfide as potent inhibitors of fibrosis in the heart of diabetic rats. Arch Biochem Biophys. 2011, 506: 48-57. 10.1016/j.abb.2010.10.014
Hassanali Z, Ametaj BN, Field CJ, Proctor SD, Vine DF: Dietary supplementation of n-3 PUFA reduces weight gain and improves postprandial lipaemia and the associated inflammatory response in the obese JCR: LA-cp rat. Diabetes Obes Metab. 2010, 12: 139-147. 10.1111/j.1463-1326.2009.01130.x
Shah KB, Duda MK, O’Shea KM, Sparagna GC, Chess DJ, Khairallah RJ, Robillard-Frayne I, Xu W, Murphy RC, Des Rosiers C, Stanley WC: The cardioprotective effects of fish oil during pressure overload are blocked by high fat intake: Role of cardiac phospholipid remodeling. Hypertension. 2009, 54: 605-611. 10.1161/HYPERTENSIONAHA.109.135806
EFSA: Scientific Opinion on the substantiation of health claims related to eicosapentaenoic acid (EPA), docosahexaenoic acid (DHA), docosapentaenoic acid (DPA) and maintenance of normal cardiac function, maintenance of normal blood glucose concentrations, maintenance of normal blood pressure, maintenance of normal blood HDL-cholesterol concentrations, maintenance of normal (fasting) blood concentrations of triglycerides. EFSA J. 2010, 8: 1796
Romieu I, Garcia-Esteban R, Sunyer J, Rios C, Alcaraz-Zubeldia M, Velasco SR, Holguin F: The effect of supplementation with omega-3 polyunsaturated fatty acids on markers of oxidative stress in elderly exposed to PM (2.5). Environ Health Perspect. 2008, 116: 1237-1242. 10.1289/ehp.10578
Grim JM, Hyndman KA, Kriska T, Girotti AW, Crockett EL: Relationship between oxidizable fatty acid content and level of antioxidant glutathione peroxidases in marine fish. J Exp Biol. 2011, 214: 3751-3759. 10.1242/jeb.058214
Lapointe A, Couillard C, Lemieux S: Effects of dietary factors on oxidation of low density lipoprotein particles. J Nutr Biochem. 2006, 17: 645-658. 10.1016/j.jnutbio.2006.01.001
Kirimlioglu V, Kirimlioglu H, Yilmaz S, Ozgor D, Coban S, Karadag N, Yologlu S: Effect of fish oil, olive oil, and vitamin E on liver pathology, cell proliferation, and antioxidant defense system in rats subjected to partial hepatectomy. Transplant Proc. 2006, 38: 564-567. 10.1016/j.transproceed.2006.02.005
Hussein O, Grosovski M, Lasri E, Svalb S, Ravid U, Assy N: Monounsaturated fat decreases hepatic lipid content in non-alcoholic fatty liver disease in rats. World J Gastroenterol. 2007, 13: 361-368.
Ferreira L, Teixeira-de-Lemos E, Pinto F, Parada B, Mega C, Vala H, Pinto R, Garrido P, Sereno J, Fernandes R, Santos P, Velada I, Melo A, Nunes S, Teixeira F, Reis F: Effects of sitagliptin treatment on dysmetabolism, inflammation, and oxidative stress in an animal model of type 2 diabetes (ZDF rat). Mediators Inflamm. 10.1155/2010/592760.
Misra HP, Fridovich I: The role of superoxide anion in the autoxidation of epinephrine and a simple assay for superoxide dismutase. J Biol Chem. 1972, 247 (10): 3170-3175.
Cohen G, Dembiec D, Marcus J: Measurement of catalase activity in tissue extracts. Anal Biochem. 1970, 34: 30-38. 10.1016/0003-2697(70)90083-7
Wheeler CR, Salzman JA, Elsayed NM, Omaye ST, Korte DW: Automated assays for superoxide dismutase, catalase, glutathione peroxidase, and glutathione reductase activity. Anal Biochem. 1990, 184: 193-199. 10.1016/0003-2697(90)90668-Y
Goldberg DM, Spooner RJ: Glutathione reductase. Methods of enzymatic analysis. Edited by: Bergmeyer HU. 1983, 258-265. Weinheim, Germany: Verlag Chemie, 3.
Cao G, Booth SL, Sadowski JA, Prior RL: Increases in human plasma antioxidant capacity after consumption of controlled diets high in fruit and vegetables. Am J Clin Nutr. 1998, 68: 1081-1087.
Mateos R, Lecumberri E, Ramos S, Goya L, Bravo L: Determination of malondialdehyde (MDA) by high-performance liquid chromatography in serum and liver as a biomarker for oxidative stress. Application to a rat model for hypercholesterolemia and evaluation of the effect of diets rich in phenolic antioxidants from fruits. J Chromatogr B Analyt Technol Biomed Life Sci. 2005, 827: 76-82. 10.1016/j.jchromb.2005.06.035
Acknowledgements
This investigation was supported, in part, by the Spanish Ministry of Science and Innovation (Grants AGL2009-12374-C03-01, -02 and -03). We acknowledge the Spanish Ministry of Science and Innovation and Xunta de Galicia for the post-graduate fellowship to L. M. and the postdoctoral “Isidro Parga Pondal” contract to M. P.; the Panamanian Government (SENACYT / IFARHU) for the postgraduate fellowship to EMT and the Instituto de Salud Carlos III for a Sara Borrell postdoctoral contract to JP-J.
Editorial assistance was by Dr. Peter R. Turner of Tscimed.com.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All the authors have contributed substantially to the design and execution of the study as well as drafting and revising the manuscript. All have approved the final version submitted for publication.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Lluís, L., Taltavull, N., Muñoz-Cortés, M. et al. Protective effect of the omega-3 polyunsaturated fatty acids: Eicosapentaenoic acid/Docosahexaenoic acid 1:1 ratio on cardiovascular disease risk markers in rats. Lipids Health Dis 12, 140 (2013). https://doi.org/10.1186/1476-511X-12-140
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-511X-12-140