
Abstract
Background
Nitric oxide is a key molecule not only in the cardiovascular system, but also in the metabolic-endocrine system. The purpose of this study was to examine possible associations of the NOS3 T-786C polymorphism (rs2070744) with serum lipid levels on the basis of lifestyle factors for tailoring prevention of dyslipidemia.
Methods
For this cross-sectional study, a total of 2226 subjects aged 35 to 69 years (1084 men and 1142 women) were selected from Japanese participants in the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study. They were recruited in eight areas throughout Japan between February 2004 and November 2008.
Results
In a stratified analysis by leisure-time physical activity, the likelihood of hypertriglyceridemia (serum triglyceride levels ≥ 150 mg/dL) among subjects with the C allele was significantly lower than those without it in the active group (OR = 0.43, 95% CI = 0.22-0.84 in the fasting group), but not in the sedentary group. A gene-environment interaction between the T-786C polymorphism and leisure-time physical activity for hypertriglyceridemia was significant (P = 0.007 in the fasting group). Additionally, serum triglyceride levels (mean ± SD) across leisure-time physical activity classes decreased significantly only in the TC + CC genotype group (111 ± 60 mg/dL for sedentary, 95 ± 48 mg/dL for moderately active, 88 ± 44 mg/dL for very active, P for trend = 0.008 in the fasting group), but not in the TT genotype group. Total cholesterol, high-density lipoprotein (HDL) cholesterol, and non-HDL cholesterol levels had no significant association with the polymorphism.
Conclusions
This study suggests that the NOS3 T-786C polymorphism modifies the effect of leisure-time physical activity on serum triglyceride levels.
Similar content being viewed by others

Introduction
Nitric oxide (NO) is an endothelium-derived relaxing factor, and plays a crucial role in the cardiovascular system[1]. NO is synthesized from L-arginine by the nitric oxide synthase (NOS)[2]. NOS consists of three major isoforms: neuronal NOS, inducible NOS, and endothelial NOS (eNOS)[2]. eNOS is encoded by NOS3, a gene localized on chromosome 7q35-36[3], and is constitutively expressed in vascular endothelium, blood platelets, and cardiomyocytes[4]. eNOS-derived NO is involved in regulation of vascular tone and regional blood flow, suppression of vascular smooth muscle proliferation, and inhibition of monocyte adhesion and platelet aggregation[5].
Recently, attention has been focused on eNOS-derived NO as a key molecule, not only in the cardiovascular system, but also in the metabolic-endocrine system[5]. Homozygote eNOS-deficient mice have been shown to be hypertensive and have fasting hyperinsulinemia, hyperlipidemia, and a 40% lower insulin-stimulated glucose uptake than control mice[6]. Similarly, a number of epidemiological studies have shown associations between NOS3 polymorphisms and endocrine-metabolic disorders. Of these polymorphisms, the NOS3 T-786C polymorphism, a thymidine to cytosine transition mutation, substantially reduces the promoter activity of NOS3 in vitro, resulting in a decrease of endothelial NO production[7]. A case–control study reported that significantly more hypertensive patients with metabolic syndrome were homozygous for the C allele than those patients without it[8].
To date, several previous studies have recruited participants from the healthy population (n = 310, 233, 142, 118, and 101, respectively) to investigate the relationship between the T-786C polymorphism and serum lipid levels[9–13]. However, there has been no large-scale population-based study that has analyzed the association. Provided that gene-environment interactions between the T-786C polymorphism and lifestyle factors on serum lipid levels are well established, the polymorphism may be useful for tailoring prevention of dyslipidemia by lifestyle modification.
Therefore, the purpose of the present study was to examine possible associations of the T-786C polymorphism with serum lipid levels on the basis of lifestyle factors such as obesity, smoking, and leisure-time physical activity, using cross-sectional data from the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study. The study was launched in 2005 to examine gene-environment interactions in lifestyle-related diseases, especially cancers, by 10 research teams throughout Japan[14].
Materials and methods
Study subjects
From 4519 subjects recruited between February 2004 and November 2008 in this cross-sectional study[15], subjects who met any of the following criteria were excluded: (i) absence of data about serum lipid levels, physical examination, lifestyle, DNA genotyping, and blood sampling time from their last meal (n = 1416); (ii) medical history of diabetes mellitus, liver cirrhosis, thyroid disorder, nephrotic syndrome, and Cushing syndrome (n = 459); (iii) medication that affects lipid levels (statins, fibrates, β-blockers, steroids, estrogen preparations, and antiestrogens) (n = 227); (iv) blood samples taken within two hours from their last meal (n = 184); (v) living in enrollment areas where there were no subjects with hypertriglyceridemia in stratified analysis, making adjustment for enrollment area impossible (n = 7). The final study group was a total of 2226 subjects (1084 men and 1142 women) from eight areas (Shizuoka, Aichi, Shiga, Kyoto, Tokushima, Fukuoka, Saga, and Kagoshima) throughout Japan. Subjects who fasted for at least 12 hours after their last meal were defined as fasting. All subjects included in this study provided written informed consent, and the J-MICC study including the current study was approved by the ethics committee of Nagoya University School of Medicine (approval No. 253 and 939).
Clinical and laboratory data
At the time of enrollment, anthropometric and blood pressure measurements, blood samples, and questionnaires were collected from each subject. BMI was calculated on the basis of measured height and body weight at each enrollment area. Blood samples were obtained for analysis of total cholesterol, high-density lipoprotein (HDL) cholesterol and triglycerides by a standard laboratory protocol used in each research team. Non-HDL cholesterol levels were calculated as total cholesterol minus HDL cholesterol levels.
Lifestyle factors
The questionnaires investigated lifestyle factors such as eating habits, smoking status, and leisure-time physical activity. Eating habits were assessed using a validated food frequency questionnaire[16]. Fat energy ratio was calculated by using the following formula: 9 × fat intake (grams/day)/caloric intake (kcal/day) × 100.
Smoking habits were assessed by smoking status and cumulative exposure. Smoking status included; never, former, and current smoking. In former and current smokers, cumulative smoking exposure was quantified in terms of pack-years by multiplying the number of years smoked by the average number of packs per day. According to pack years, smokers were classified into three levels: light (< 20 pack-years), moderate (< 40 but ≥ 20 pack-years), and heavy (≥ 40 pack-years).
Leisure-time physical activity was evaluated using the International Physical Activity Questionnaire (IPAQ)[17]. IPAQ was developed and validated as an instrument for cross-national monitoring of physical activity and inactivity[17]. From the type, frequency of, and time spent on physical activity during leisure time, the degree of leisure-time physical activity was calculated as metabolic equivalent (MET)-minutes/week (MET levels × minutes of activity/day × days/week) according to IPAQ. The degree of leisure-time physical activity in subjects was classified into three groups: sedentary (< 600 MET-minutes/week), moderately active (< 1500 but ≥ 600 MET-minutes/week), and very active (≥ 1500 MET-minutes/week). In addition, subjects whose leisure-time physical activity was 600 MET-minutes/week or more were defined as active.
NOS3 genotyping
Each genomic DNA sample was prepared from peripheral blood by a BioRobot M48 Workstation (Qiagen Group, Tokyo, Japan) or an automatic nucleic acid isolation system (NA-3000, Kurabo, Co., Ltd, Osaka, Japan). The T-786C polymorphism was genotyped by a multiplex polymerase chain reaction (PCR)-based Invader assay (Third Wave Technologies, Madison, WI, USA) at the Laboratory for Genotyping Development, Center for Genomic Medicine, RIKEN, as described previously[18].
For multiplex PCR, a 180-bp fragment encompassing the T-786C polymorphism was amplified with the following primers: 5′-TGAAGTGCCTGGAGAGTGC-3′ and 5′-CCCACCCTGTCATTCAGTG-3′. The amplified fragment was diluted and used for the Invader assay. Signal intensities that discriminated genotypes were recorded after the reaction using the ABI7900HT sequence detection system (Applied Biosystems, Foster City, CA, USA).
Statistical analysis
Chi-squared tests were performed to analyze deviation of observed genotype frequencies from the Hardy-Weinberg equilibrium. Differences in the quantitative data among the genotypes were examined by one-way ANOVA. Normality was tested by the skewness and kurtosis test, and parameters without normal distribution were analyzed after log-transformation.
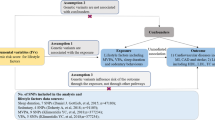
Odds ratios (ORs) and 95% confidence intervals (CIs) for the presence of the C allele for hypertriglyceridemia (serum triglyceride levels ≥ 150 mg/dL) and P values for the interaction between the polymorphism and lifestyle factors for hypertriglyceridemia were calculated by multiple logistic regression analysis, and adjusted in the following two ways: (model 1) for age (continuous), sex (male and female), and enrollment area (Shizuoka, Aichi, Shiga, Kyoto, Tokushima, Fukuoka, Saga, and Kagoshima); (model 2) for age, sex, enrollment area, BMI (continuous), fat energy ratio (continuous), smoking habits (never, light, moderate, and heavy), leisure-time physical activity (sedentary, moderately active, and very active), and blood sampling time from last meal (≥ 12 h, 8 h to < 12 h, 4 h to < 8 h, and 2 h to < 4 h). A multiplicative interaction term was included in the logistic model to test the interactions. The statistical power among total subjects to detect an OR of 0.50, 0.60, or 0.70 for carriers of the C allele was estimated to be 99%, 96%, or 73%, respectively (estimated minor allele carriers frequency in a Japanese population without hypertriglyceridemia = 0.20). Similarly, the powers among the subgroups examined were 98%, 83%, or 53% for BMI < 25, 74%, 50%, or 27% for BMI ≥ 25, 97%, 83%, or 53% for pack-years < 20, 73%, 49%, or 27% for pack-years ≥ 20, 96%, 80%, or 50% for sedentary, and 82%, 58%, or 32% for active, respectively. In the subgroups stratified by leisure-time physical activity, our sample size could detect an OR of 0.50 with more than 80% power.
In addition, serum triglyceride levels were compared between leisure-time physical activity classes, namely, sedentary, moderately active, and very active. Trends of serum triglyceride levels across the classes and differences in serum triglyceride levels between the classes were tested using multiple linear regression models by coding 1, 2, or 3 for sedentary, moderately active, and very active, respectively, as an independent variable with the same covariates as used in model 2 above. The dependent variable was the log-transformed value of serum triglyceride levels. A two-tailed P value of < 0.05 was considered to be statistically significant. All analyses were conducted using Stata version 11.0 (Stata Corp., College Station, TX, USA).
Results
Frequencies of the NOS3 T-786C polymorphism
A total of 19.2% of subjects were carriers of the C allele (TC + CC), with an allelic frequency of 10.2%. The T-786C genotype distribution of all subjects followed the Hardy-Weinberg equilibrium (χ2 = 0.47, P = 0.49, Table 1).
Clinical characteristics of subjects
The characteristics of study subjects by sex are shown in Table 1. Regarding leisure-time physical activity, males and females showed a similar distribution. Table 2 summarizes the BMI, blood pressure, and laboratory parameters of all subjects by the T-786C genotype. Serum triglyceride levels were significantly different among the three genotypes. Total cholesterol, HDL cholesterol, and non-HDL cholesterol had no significant association with the polymorphism.
Stratified analysis by lifestyle factors for hypertriglyceridemia
Multiple logistic regression analysis of an association between the T-786C polymorphism and hypertriglyceridemia (serum triglyceride levels ≥ 150 mg/dL) demonstrated that the ORs for the presence of the C allele for hypertriglyceridemia in both the total and fasting group were not significant (Table 3).
All subjects were stratified into two subgroups by BMI, pack-years of smoking, or leisure-time physical activity. There was no significant association between the polymorphism and hypertriglyceridemia in the subgroups stratified by BMI or pack-years of smoking. However, the likelihood of hypertriglyceridemia among subjects with the C allele was significantly lower than those without it in the active group. In addition, gene-environment interactions between the polymorphism (TC + CC vs. TT) and leisure-time physical activity (active vs. sedentary) for hypertriglyceridemia were also significant in both the total and fasting group. When stratified by sex, the interaction was significant only for females in the fasting group (P = 0.04), and not significant for both males and females in the total group.
Serum triglyceride levels according to leisure-time physical activity
Figure 1 shows serum triglyceride levels according to leisure-time physical activity in the TT and TC + CC genotype groups. Serum triglyceride levels across leisure-time physical activity classes decreased significantly only in the TC + CC genotype group (111 ± 60 mg/dL for sedentary, 95 ± 48 mg/dL for moderately active, 88 ± 44 mg/dL for very active, P for trend = 0.008 in the fasting group), but not in the TT genotype group. Moreover, in the TC + CC genotype group, both the moderately and very active groups had significantly lower serum triglyceride levels than the sedentary group in the total group (P = 0.005 for moderately active and P = 0.02 for very active) and the fasting group (P = 0.04 for moderately active and P = 0.03 for very active). No significant difference was seen in the TT genotype group.

Serum triglyceride levels according to leisure-time physical activity by the NOS3 T-786C genotype. Serum triglyceride levels are presented as mean ± SD. Trends of serum triglyceride levels across leisure-time physical activity classes, namely, sedentary, moderately active, and very active, and differences in serum triglyceride levels between the classes were tested after adjustment for age (continuous), sex (male and female), enrollment area (Shizuoka, Aichi, Shiga, Kyoto, Tokushima, Fukuoka, Saga, and Kagoshima), BMI (continuous), fat energy ratio (continuous), smoking habits (never, light, moderate, and heavy), and blood sampling time from last meal (≥ 12 h, 8 h to < 12 h, 4 h to < 8 h, and 2 h to < 4 h) by multiple linear regression analysis. Values of serum triglyceride levels were log-transformed before analysis was carried out. * P < 0.05 compared to the sedentary group in each genotype group.
Discussion
The present study found that gene-environment interactions between the NOS3 T-786C polymorphism and leisure-time physical activity on serum triglyceride levels were significant, and that both the moderately and very active groups had significantly lower serum triglyceride levels than the sedentary group in the TC + CC genotype group, but not in the TT genotype group. This suggests that the presence of the C allele enhances the beneficial effect of leisure-time physical activity on serum triglyceride levels. An intervention study showed that the presence of the C allele did not affect the beneficial effect of exercise in reducing serum triglyceride levels among postmenopausal women (n = 49)[19], but the sex difference of this effect was unclear in the current study.
The genotype distribution of the current study subjects was very similar to that described previously in 233 Japanese (83.3%, 15.0%, and 1.7% for the TT, TC, and CC genotypes, respectively)[10]. Compared with Caucasians, C allele carriers were much less common in Japanese (32.0%, 52.0%, and 16.0% for the TT, TC, and CC genotypes in Caucasians, respectively)[20].
Recently, the role of triglycerides in atherosclerotic diseases was controversial because of the large variation in triglyceride measurements, and the strong inverse relationship between HDL cholesterol and triglycerides[21]. However, large meta-analyses of prospective studies have reported that triglycerides are an independent risk factor for coronary heart disease in the general Western populations, and Asian and Pacific populations[22, 23]. Triglycerides are not directly atherogenic, but represent an important biomarker of cardiovascular disease risk because of their association with atherogenic remnant particles and apolipoprotein C-III, a lipoprotein lipase (LPL) inhibitor[24]. Therapy with fibrates, most selective triglyceride-reducing drugs, was reported to produce a 10% risk reduction for major cardiovascular events and a 13% relative risk reduction for coronary heart disease[25].
Triglycerides are frequently associated with lifestyle factors, one of which is exercise. Aerobic exercise was reported to cause a 15% to 20% reduction in serum triglycerides when triglyceride levels were over 150 mg/dL[24]. In rats, exercise induces an increase in LPL mass and total and heparin-releasable LPL activity in white skeletal muscle[26]. Interestingly, these beneficial effects of exercise may involve NO[27]. In vitro, shear stress of bovine aortic endothelial cells increased the eNOS transcriptional rate and upregulated eNOS mRNA levels[28]. An experiment using Goto-Kakizaki rats (a model of type 2 diabetes) showed that exercise increased both the total eNOS expression and the dimer:monomer ratio in the left ventricle and induced significant increases in NO production and concomitant decreases in eNOS-dependent superoxide production[29].
NO can lower serum triglyceride levels by three mechanisms. Firstly, NO can promote triglyceride metabolism through an increase in blood flow and insulin to tissues[30]. Insulin and its counterregulation have been reported to play a central role in triglyceride metabolism by suppression of hepatic production and secretion of triglyceride-rich lipoproteins[31] and stimulation of LPL activity[32]. Secondly, NO can decrease free fatty acid concentration for the synthesis of triglycerides by promoting the formation of new metabolically active mitochondria[33] and activating carnitine palmitoyltransferase 1, an enzyme which transports activated fatty acids into mitochondria for oxidation[34]. Thirdly, NO can suppress the synthesis of triglycerides in liver by inhibiting the de novo fatty acid synthesis through an adenosine monophosphate-activated protein kinase-dependent inhibition of the activity of acetyl-CoA carboxylase, which catalyzes the carboxylation of acetyl-CoA to malonyl-CoA, a key substrate in chain elongation during fatty acid biosynthesis[34].
To date, there has been no experimental study that has shown the difference in responsiveness to exercise in NO production among the T-786C genotypes. It has been reported that a shear stress responsive element is located near the promoter region of NOS3 between nucleotides −1600 and −779[35], but the question of whether the polymorphism modifies the effect of physical activity on NO production is controversial. An intervention study showed that six months of aerobic exercise increased the bioavailability of NO only in subjects with the C allele[36]. In contrast, another study showed that the increase in NO production in response to six months exercise was greater in women without the C allele as compared with those with it[37].
In addition to exercise, the polymorphism has been reported to modulate the effect of statins, which are 3-hydroxy-3-methyl-glutaryl-CoA reductase inhibitors[38]. An in vitro experiment demonstrated that fluvastatin augmented eNOS transcriptional activity in human umbilical vein endothelial cells (HUVECs) containing the CC genotype more powerfully than those with the TT genotype. This effect was due to a decrease in gene expression of replication protein A1 (RPA1). RPA1 specifically binds to the C allele and significantly suppresses the transcriptional activity of NOS3[39]. This finding was supported by an epidemiological study that showed atorvastatin treatment increased whole blood nitrite concentrations and attenuated oxidative stress in the CC genotype group, but not in the TT genotype group[40]. Future studies investigating the effect of exercise on RPA1 expression by the T-786C genotype is eagerly anticipated.
The current study had several limitations. To begin with, the examination was limited to only one NOS3 polymorphism and did not consider combinations with other NOS3 polymorphisms, as well as polymorphisms of other genes that are associated with serum triglyceride levels. Next, there may have been differences among the institutions in measurement methods concerning clinical data. However, such differences may have had a limited impact on data analysis as enrollment area was added to the adjustment factors. Finally, physical activity of subjects was taken into account only during their leisure time, not all the time, and the effect of physical activity outside of leisure time may have been confounding.
In conclusion, the present study suggests that the NOS3 T-786C polymorphism modifies the effect of leisure-time physical activity on serum triglyceride levels. Tailoring prevention of hypertriglyceridemia on the basis of the T-786C genotypes could be achieved, provided that further studies, including cohort and intervention studies, validate the results of this cross-sectional study.
References
Yang Z, Ming XF: Recent advances in understanding endothelial dysfunction in atherosclerosis. Clin Med Res. 2006, 4: 53-65. 10.3121/cmr.4.1.53
Alderton WK, Cooper CE, Knowles RG: Nitric Oxide synthases: structure, function and inhibition. Biochem J. 2001, 357: 593-615. 10.1042/0264-6021:3570593
Marsden PA, Heng HH, Scherer SW, Stewart RJ, Hall AV, Shi XM, Tsui LC, Schappert KT: Structure and chromosomal localization of the human constitutive endothelial nitric oxide synthase gene. J Biol Chem. 1993, 268: 17478-17488.
Dudzinski DM, Igarashi J, Greif D, Michel T: The regulation and pharmacology of endothelial nitric oxide synthase. Annu Rev Pharmacol Toxicol. 2006, 46: 235-276. 10.1146/annurev.pharmtox.44.101802.121844
Huang PL: eNOS, metabolic syndrome and cardiovascular disease. Trends Endocrinol Metab. 2009, 20: 295-302. 10.1016/j.tem.2009.03.005
Duplain H, Burcelin R, Sartori C, Cook S, Egli M, Lepori M, Vollenweider P, Pedrazzini T, Nicod P, Thorens B, Scherrer U: Insulin resistance, hyperlipidemia, and hypertension in mice lacking endothelial nitric oxide synthase. Circulation. 2001, 104: 342-345. 10.1161/01.CIR.104.3.342
Nakayama M, Yasue H, Yoshimura M, Shimasaki Y, Kugiyama K, Ogawa H, Motoyama T, Saito Y, Ogawa Y, Miyamoto Y, Nakao K: T-786→C mutation in the 5′-flanking region of the endothelial nitric oxide synthase gene is associated with coronary spasm. Circulation. 1999, 99: 2864-2870. 10.1161/01.CIR.99.22.2864
Fernandez ML, Ruiz R, Gonzalez MA, Ramirez-Lorca R, Couto C, Ramos A, Gutierrez-Tous R, Rivera JM, Ruiz A, Real LM, Grilo A: Association of NOS3 gene with metabolic syndrome in hypertensive patients. Thromb Haemost. 2004, 92: 413-418.
Han Y, Xu W, Zhang W, Liu N, Ji Y: T-786C polymorphism in the endothelial nitric oxide synthase gene is associated with increased risk of coronary artery disease in a Chinese population. Pharmacology. 2010, 85: 211-216. 10.1159/000275135
Ohtoshi K, Yamasaki Y, Gorogawa S, Hayaishi-Okano R, Node K, Matsuhisa M, Kajimoto Y, Hori M: Association of -786T-C mutation of endothelial nitric oxide synthase gene with insulin resistance. Diabetologia. 2002, 45: 1594-1601. 10.1007/s00125-002-0922-6
Metzger IF, Sertorio JT, Tanus-Santos JE: Modulation of nitric oxide formation by endothelial nitric oxide synthase gene haplotypes. Free Radic Biol Med. 2007, 43: 987-992. 10.1016/j.freeradbiomed.2007.06.012
Paradossi U, Ciofini E, Clerico A, Botto N, Biagini A, Colombo MG: Endothelial function and carotid intima-media thickness in young healthy subjects among endothelial nitric oxide synthase Glu298→Asp and T-786→C polymorphisms. Stroke. 2004, 35: 1305-1309. 10.1161/01.STR.0000126482.86708.37
Imamura A, Takahashi R, Murakami R, Kataoka H, Cheng XW, Numaguchi Y, Murohara T, Okumura K: The effects of endothelial nitric oxide synthase gene polymorphisms on endothelial function and metabolic risk factors in healthy subjects: the significance of plasma adiponectin levels. Eur J Endocrinol. 2008, 158: 189-195. 10.1530/EJE-07-0632
Hamajima N: The Japan Multi-Institutional Collaborative Cohort Study (J-MICC Study) to detect gene-environment interactions for cancer. Asian Pac J Cancer Prev. 2007, 8: 317-323.
Wakai K, Hamajima N, Okada R, Naito M, Morita E, Hishida A, Kawai S, Nishio K, Yin G, Asai Y, Matsuo K, Hosono S, Ito H, Watanabe M, Kawase T, Suzuki T, Tajima K, Tanaka K, Higaki Y, Hara M, Imaizumi T, Taguchi N, Nakamura K, Nanri H, Sakamoto T, Horita M, Shinchi K, Kita Y, Turin TC, Rumana N, Matsui K, Miura K, Ueshima H, Takashima N, Nakamura Y, Suzuki S, Ando R, Hosono A, Imaeda N, Shibata K, Goto C, Hattori N, Fukatsu M, Yamada T, Tokudome S, Takezaki T, Niimura H, Hirasada K, Nakamura A, Tatebo M, Ogawa S, Tsunematsu N, Chiba S, Mikami H, Kono S, Ohnaka K, Takayanagi R, Watanabe Y, Ozaki E, Shigeta M, Kuriyama N, Yoshikawa A, Matsui D, Watanabe I, Inoue K, Ozasa K, Mitani S, Arisawa K, Uemura H, Hiyoshi M, Takami H, Yamaguchi M, Nakamoto M, Takeda H, Kubo M, Tanaka H: Profile of participants and genotype distributions of 108 polymorphisms in a cross-sectional study of associations of genotypes with lifestyle and clinical factors: a project in the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study. J Epidemiol. 2011, 21: 223-235. 10.2188/jea.JE20100139
Tokudome Y, Goto C, Imaeda N, Hasegawa T, Kato R, Hirose K, Tajima K, Tokudome S: Relative validity of a short food frequency questionnaire for assessing nutrient intake versus three-day weighed diet records in middle-aged Japanese. J Epidemiol. 2005, 15: 135-145. 10.2188/jea.15.135
Craig CL, Marshall AL, Sjöström M, Bauman AE, Booth ML, Ainsworth BE, Pratt M, Ekelund U, Yngve A, Sallis JF, Oja P: International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003, 35: 1381-1395. 10.1249/01.MSS.0000078924.61453.FB
Ohnishi Y, Tanaka T, Ozaki K, Yamada R, Suzuki H, Nakamura Y: A high-throughput SNP typing system for genome-wide association studies. J Hum Genet. 2001, 46: 471-477. 10.1007/s100380170047
Esposti RD, Sponton CH, Malagrino PA, Carvalho FC, Peres E, Puga GM, Novais IP, Albuquerque DM, Rodovalho C, Bacci M, Zanesco A: Influence of eNOS gene polymorphism on cardiometabolic parameters in response to physical training in postmenopausal women. Braz J Med Biol Res. 2011, 44: 855-863. 10.1590/S0100-879X2011007500106
Tanus-Santos JE, Desai M, Flockhart DA: Effects of ethnicity on the distribution of clinically relevant endothelial nitric oxide variants. Pharmacogenetics. 2001, 11: 719-725. 10.1097/00008571-200111000-00011
Austin MA: Plasma triglyceride as a risk factor for coronary heart disease. The epidemiologic evidence and beyond. Am J Epidemiol. 1989, 129: 249-259.
Sarwar N, Danesh J, Eiriksdottir G, Sigurdsson G, Wareham N, Bingham S, Boekholdt SM, Khaw KT, Gudnason V: Triglycerides and the risk of coronary heart disease: 10, 158 incident cases among 262, 525 participants in 29 Western prospective studies. Circulation. 2007, 115: 450-458. 10.1161/CIRCULATIONAHA.106.637793
Patel A, Barzi F, Jamrozik K, Lam TH, Ueshima H, Whitlock G, Woodward M: Serum triglycerides as a risk factor for cardiovascular diseases in the Asia-Pacific region. Circulation. 2004, 110: 2678-2686.
Talayero BG, Sacks FM: The role of triglycerides in atherosclerosis. Curr Cardiol Rep. 2011, 13: 544-552. 10.1007/s11886-011-0220-3
Jun M, Foote C, Lv J, Neal B, Patel A, Nicholls SJ, Grobbee DE, Cass A, Chalmers J, Perkovic V: Effects of fibrates on cardiovascular outcomes: a systematic review and meta-analysis. Lancet. 2010, 375: 1875-1884. 10.1016/S0140-6736(10)60656-3
Durstine JL, Grandjean PW, Cox CA, Thompson PD: Lipids, lipoproteins, and exercise. J Cardiopulm Rehabil. 2002, 22: 385-398. 10.1097/00008483-200211000-00002
Knott AB, Bossy-Wetzel E: Impact of nitric oxide on metabolism in health and age-related disease. Diabetes Obes Metab. 2010, 12: 126-133.
Malek AM, Jiang L, Lee I, Sessa WC, Izumo S, Alper SL: Induction of nitric oxide synthase mRNA by shear stress requires intracellular calcium and G-protein signals and is modulated by PI 3 kinase. Biochem Biophys Res Commun. 1999, 254: 231-242. 10.1006/bbrc.1998.9921
Grijalva J, Hicks S, Zhao X, Medikayala S, Kaminski PM, Wolin MS, Edwards JG: Exercise training enhanced myocardial endothelial nitric oxide synthase (eNOS) function in diabetic Goto-Kakizaki (GK) rats. Cardiovasc Diabetol. 2008, 7: 34- 10.1186/1475-2840-7-34
Higaki Y, Hirshman MF, Fujii N, Goodyear LJ: Nitric oxide increases glucose uptake through a mechanism that is distinct from the insulin and contraction pathways in rat skeletal muscle. Diabetes. 2001, 50: 241-247. 10.2337/diabetes.50.2.241
Sparks JD, Sparks CE: Insulin regulation of triacylglycerol-rich lipoprotein synthesis and secretion. Biochim Biophys Acta. 1994, 1215: 9-32. 10.1016/0005-2760(94)90088-4
Mead JR, Irvine SA, Ramji DP: Lipoprotein lipase: structure, function, regulation, and role in disease. J Mol Med. 2002, 80: 753-769. 10.1007/s00109-002-0384-9
Jobgen WS, Fried SK, Fu WJ, Meininger CJ, Wu G: Regulatory role for the arginine-nitric oxide pathway in metabolism of energy substrates. J Nutr Biochem. 2006, 17: 571-588. 10.1016/j.jnutbio.2005.12.001
Gao Y: The multiple actions of NO. Pflugers Arch. 2010, 459: 829-839. 10.1007/s00424-009-0773-9
Data SA, Roltsch MH, Hand B, Ferrell RE, Park JJ, Brown MD: eNOS T-786C genotype, physical activity, and peak forearm blood flow in females. Med Sci Sports Exerc. 2003, 35: 1991-1997. 10.1249/01.MSS.0000099105.99682.8B
Zago AS, Kokubun E, Fenty-Stewart N, Park JY, Attipoe S, Hagberg J, Brown M: Effect of physical activity and T-786C polymorphism in blood pressure and blood flow in the elderly. Arq Bras Cardiol. 2010, 95: 510-516. 10.1590/S0066-782X2010005000126
Sponton CH, Rezende TM, Mallagrino PA, Franco-Penteado CF, Bezerra MA, Zanesco A: Women with TT genotype for eNOS gene are more responsive in lowering blood pressure in response to exercise. Eur J Cardiovasc Prev Rehabil. 2010, 17: 676-681. 10.1097/HJR.0b013e32833a1301
Lacchini R, Silva PS, Tanus-Santos JE: A pharmacogenetics-based approach to reduce cardiovascular mortality with the prophylactic use of statins. Basic Clin Pharmacol Toxicol. 2010, 106: 357-361.
Abe K, Nakayama M, Yoshimura M, Nakamura S, Ito T, Yamamuro M, Sakamoto T, Miyamoto Y, Yoshimasa Y, Saito Y, Nakao K, Yasue H, Ogawa H: Increase in the transcriptional activity of the endothelial nitric oxide synthase gene with fluvastatin: a relation with the -786T>C polymorphism. Pharmacogenet Genomics. 2005, 15: 329-336. 10.1097/01213011-200505000-00008
Nagassaki S, Sertório JT, Metzger IF, Bem AF, Rocha JB, Tanus-Santos JE: eNOS gene T-786C polymorphism modulates atorvastatin-induced increase in blood nitrite. Free Radic Biol Med. 2006, 41: 1044-1049. 10.1016/j.freeradbiomed.2006.04.026
Acknowledgements
The authors would like to thank Mr. Kyota Ashikawa, Ms. Tomomi Aoi, and the other members of the Laboratory for Genotyping Development, Center for Genomic Medicine, RIKEN for support with genotyping, and Mses. Yoko Mitsuda, Keiko Shibata, and Etsuko Kimura at the Department of Preventive Medicine, Nagoya University Graduate School of Medicine for their co-operation, technical assistance, and valuable comments. Funding was provided by Grant-in-Aid for Scientific Research on Priority Areas of Cancer (No. 17015018) and Grant-in-Aid for Scientific Research on Innovative Areas (No. 221S0001) from the Japanese Ministry of Education, Culture, Sports, Science and Technology.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
TH was responsible for the complete analysis of the data and for preparing the tables and the manuscript. NH, HT, and KW participated in all aspects of the project, including study design, molecular genetic studies, statistical analysis, and manuscript preparation. MN, SK, and GY were responsible for data management, and carried out the molecular genetic studies. SS, YK, HN, TI, KO, KA, MS, HI, and HM acted as principal investigators for the J-MICC Study, and contributed to data acquisition. MK carried out the genotyping. All authors have read and approved the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Higashibata, T., Hamajima, N., Naito, M. et al. eNOS genotype modifies the effect of leisure-time physical activity on serum triglyceride levels in a Japanese population. Lipids Health Dis 11, 150 (2012). https://doi.org/10.1186/1476-511X-11-150
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-511X-11-150