
Abstract
Primary care is recognized as the most important form of healthcare for maintaining population health because it is relatively inexpensive, can be more easily delivered than specialty and inpatient care, and if properly distributed it is most effective in preventing disease progression on a large scale. Recent advances in the field of health geography have greatly improved our understanding of the role played by geographic distribution of health services in population health maintenance. However, most of this knowledge has accrued for hospital and specialty services and services in rural areas. Much less is known about the effect of distance to and supply of primary care on primary care utilization, particularly in the U.S.
For several reasons the shortage of information is particularly acute for urban areas, where the majority of people live. First, explicit definitions and conceptualizations of healthcare access have not been widely used to guide research. An additional barrier to progress has been an overwhelming concern about affordability of care, which has garnered the majority of attention and research resources. Also, the most popular measures of spatial accessibility to care – travel impedance to nearest provider and supply level within bordered areas – lose validity in congested urban areas. Better measures are needed. Fortunately, some advances are occurring on the methodological front. These can improve our knowledge of all types of healthcare geography in all settings, including primary care in urban areas.
This paper explains basic concepts and measurements of access, provides some historical background, outlines the major questions concerning geographic accessibility of primary care, describes recent developments in GIS and spatial analysis, and presents examples of promising work.
Similar content being viewed by others


Review
Access to primary healthcare is recognized as an important facilitator of overall population health. In the United States the majority of research and policy efforts to improve access and eliminate disparities in healthcare have focused on costs. Consequently we know quite a bit about the relationship between healthcare affordability and utilization rates. However, we know surprising little about how other barriers to healthcare effect utilization rates and population health. Chief among these less well understood barriers is geographic availability and accessibility of primary care providers. This knowledge deficit can now be more aggressively addressed, thanks to recent advances in the field of geospatial analysis, coupled with the decreasing cost and improving usability of geographic information systems (GIS).
This paper explains basic concepts and measurements of access, provides primary care researchers with some historical background, outlines the major questions concerning geographic accessibility of primary care, describes recent developments in GIS and spatial analysis, and presents examples of promising work. Emphasis will be given to the problems of urban areas, where the majority of needy populations are located and where spatial analysis methods have rarely been applied in a useful manner.
Defining access
Access to healthcare has multiple definitions, and its meaning in a given context is too often assumed [1]. The most basic problem is that it is both a noun referring to potential for healthcare use, and a verb referring to the act of using or receiving healthcare. This leads to confusion between ability to get care, the act of seeking care, the actual delivery of care, and indicators thereof. Concepts and communication become clearer if we think of access in terms of stages and dimensions. The two broad stages are "potential" for care delivery, followed by "realized" delivery of care. Potential exists when a needy population coexists in space and time with a willing and able healthcare delivery system. Realized care, sometimes referred to as actualized care, follows when all barriers to provision are overcome.
A number of barriers can impede progression from potential to realized access. Penchansky and Thomas [2] have usefully grouped barriers into five dimensions: availability, accessibility, affordability, acceptability and accommodation. The last three have received the most attention in the U.S. They are essentially aspatial, and reflect healthcare financing arrangements and cultural factors. However, the first two dimensions are spatial in nature. Availability refers to the number of local service points from which a client can choose. Accessibility is travel impedance (distance or time) between patient location and service points. While the distinction between availability and accessibility can be useful, in the context of urban areas, where multiple service locations are common, the two dimensions should be considered simultaneously. We refer to this fusion as "spatial accessibility" (SA), a term that is common in the geography and social sciences literature and is gaining some favor in the healthcare geography literature [1, 3–5].
In Table 1 we bring together the concepts of access stages and dimensions to create a taxonomy for healthcare access studies. This arrangement permits us to understand the strengths and limitations of the geospatial data available for a given study, and to make the proper interpretations of analyses based on those data. For example, a study of neighborhood racial composition and SA of primary care providers would fall into the upper left-hand cell of Table 1, as it is a study of spatial potential. It could not demonstrate or disprove any relationship of spatial accessibility and utilization or population health. There is a very large literature on realized care (utilization) and the aspatial dimensions of access to care. This paper focuses on that aspect of access that is less well understood – spatial accessibility, a measure of potential for health care delivery.
Spatial accessibility in the U.S
Distance to healthcare provider was recognized as a significant barrier to healthcare access in the U.S. in the 19th century [6, 7]. By the middle 1970s many attempts were made to measure spatial accessibility of health service locations, identify areas of provider shortage, and reveal social disparities in SA in both urban and rural areas [8–12]. The issue has been on the national policy agenda since the 1967 Report of the National Advisory Commission on Health Manpower attributed maldistribution of healthcare professionals to their preference for affluent neighborhoods [13]. Since then work has continued for rural and mixed urban-rural areas, despite a lack of consensus on how to best measure spatial accessibility [5, 14–19]. This primarily rural focus was fueled by the recognition that distance is an obvious impediment in sparsely populated areas, and by the alarming decline of healthcare workforce supply in rural America [20].
Concern about SA to healthcare providers in urban areas remains high [21–23]. However, with few exceptions [24, 25], U.S. cities have not been studied since the middle 1970s. One reason is that intuitive spatial indicators, which are arguably appropriate for large rural geographies (described below), are much less relevant in congested urban areas. Ironically, the waning of research on urban spatial accessibility of healthcare providers corresponded with the increasing availability of powerful software and hardware necessary for more valid and sophisticated urban studies.
In the more recent literature there is clear evidence of social inequity in spatial distribution of healthcare providers, including primary care providers [3, 26]. However, few studies have tested for an effect of SA on actual healthcare delivery. In two studies Fortney and colleagues showed that travel distance affected the probability of utilization of mental health and alcoholic treatment services [27, 28]. Athas et al. [29] and Nattinger et al. [30] found increasing travel distance to be associated with decreased utilization of breast cancer treatment. Similarly, Meden et al. [31] showed that shorter travel distance to radiation oncology facilities was associated with lower rates of the equally efficacious but less desirable radical mastectomy treatment. Goodman and colleagues have reported that greater distance from hospital was associated with lower likelihood of admission for discretionary conditions [14, 32].
The aforementioned studies support the notion that SA impacts probability of contact with the healthcare system. Fewer studies address whether or how SA actually regulates population health. Three of these come from the literature on ambulatory care sensitive conditions (ACSCs) – conditions for which hospitalization may indicate a failure of the primary care system to treat a case that is manageable through ambulatory care [33]. ACSC rates are both a measure of utilization and an indicator of population health. Basu and Friedman [34] found that children living in areas with lower primary care availability were more likely to travel greater distances for ACSC inpatient services, the implication being that disease rates were higher in these areas. For adults, Basu et al. [35] and Parchman and Culler [36] found that lower primary care availability was associated with higher rates of ACSC admissions. In a British study Gulliford [37] found that lower general practitioner supply was associated with higher rates of avoidable hospitalizations. Finally, in a study of mortality rates in U.S. metropolitan areas, Shi and Starfield [38] found that physician supply levels were negatively associated with mortality rates. Notwithstanding these studies, much remains unknown.
Remaining questions
It is intuitive that communities located at insurmountable distances from any source of healthcare will be negatively impacted by the lack of resources. However, despite decades of attention we have surprisingly little quantitative information about the effect of spatial accessibility of care on population health, particularly regarding the effect of primary care. The most basic problem is that we do not know what is the most useful measure of SA. The best choice might vary with the circumstances, such as urbanicity, racial/ethnic composition, or economic status of the area under study. It is also reasonable to assume that population health should begin to be affected by SA at some point of increasing availability of primary care resources. However, we do not know what that point is. Furthermore, we do not know if there is a point of diminishing returns. The latter two issues are related to the question long asked by Dartmouth health services researchers – what is the right rate of healthcare [39, 40, 10, 41, 42]?
We also do not yet know how the effect of primary care SA varies across the spectrum of disease. For example, is the effect greater for asthma than cardiovascular health? The literature on ambulatory care sensitive conditions (ACSCs) is inconsistent on this point. Some studies suggest that ACSCs are sensitive to primary care availability, while other suggest that all disease categories are equally responsive to primary care availability [34, 35, 43–46].
Another problem concerns the importance of primary care SA relative to the SA of other types of healthcare. In other words, is the optimal SA of primary care providers more important than the optimal SA of specialists, such as allergists, neonatologists and rheumatologists? Also, is it more important than optimal SA of inpatient services? Most would agree that the answer is "yes" for both questions. However, if SA has not been satisfactorily quantified the relative value of SA of the various types of care cannot be quantified. Similarly, it is not known how important primary care SA is relative to the other dimensions of access, i.e. affordability, acceptability and accommodation. Furthermore, does its relative importance vary with social and economic circumstances? For example, among fully acculturated Americans SA of primary care might be more important than accommodation, while among immigrants satisfactory accommodation by providers might overshadow all other considerations. Again, proper quantification of SA is necessary to address the question.
Finally, when changes in SA of primary care occur, what is the latency of the effect on population health? How long would it be before improvements or deterioration in population health are noticeable? Until we know the answer to this question we should be careful about interpreting analyses of the relationship between SA and population health at a fixed point in time. It could be that the apparent effect or strength of association might be related as much to recent population movements as to availability of care in the setting studied.
Measuring spatial accessibility
Clearly, important questions remain and much work needs to be done. Here we will focus on basic questions of SA measurement, with emphasis on urban areas. Gesler [47] published a complex and comprehensive taxonomy of spatial analyses for the broader field of medical geography. However, most published measures of spatial accessibility to healthcare can be classified more simply into four categories: provider-to-population ratios, distance to nearest provider, average distance to a set of providers, and gravitational models of provider influence.
Provider-to-population ratios, also referred to as supply ratios, are computed within bordered areas. They are the most popular type of SA measure because they are highly intuitive, the data sources are readily available, and they do not necessarily require GIS tools and expertise. They are also the measurement type that has been used in the sentinel literature on ambulatory care sensitive conditions (ACSCs). Ratios are computed for bordered areas, such as states, counties, metropolitan statistical areas, or health service areas. These are the geographic units of analysis. The numerator is some indicator of health service capacity, such as number of physicians, clinics, or hospital beds. The denominator is the population size within the area. This is most often taken from census files, but may be taken from insurance plan enrollment files, e.g. Medicare, depending on the population of interest. Bordered areas are then analyzed for associations between provider-to-population ratio values and some indicator of healthcare utilization (e.g. rate of immunizations) or health status (e.g. disease prevalence rates).
As indicators of availability, supply ratios are good for gross comparisons of supply between large geopolitical units or service areas, and are used by policy analysts to set minimal standards of supply and to identify underserved areas [18, 22, 48]. Unfortunately, supply ratios have some serious limitations. First, they do not account for patient border crossing, which commonly occurs for small geographies such as urban census tracts and postal code areas [49]. Second, supply ratios are blind to variations in accessibility within bordered areas. Finally, they do not explicitly incorporate any measures of distance or travel impedance. Consequently the results and interpretations stemming from bordered area studies can vary greatly depending on the size, number and configuration of the areal units studied. This problem is well-known to geographers and spatial analysts as the modifiable areal unit problem (MAUP) [50].
Travel impedance to nearest provider is another very intuitive and commonly used measure of SA. It is typically measured from a patient's residence or from a population center, such as the geometric centroid of county of residence, depending on the resolution of the available data. Travel impedance, sometimes referred to as travel cost, is often measured in units of Euclidean (straight line) distance, travel distance along a road and/or rail system, or estimated travel time via a transportation network.
Travel impedance to nearest provider has been assumed to be a good measure of SA for rural areas, where provider choices are very limited and the nearest provider is also the most likely to be used. However, Fryer et al. [19] have provided evidence to the contrary. Regardless of suitability for rural areas, this measure is probably not suitable for urban settings because it is insensitive to the fact that in congested areas there is usually an array of provider options at similar distance from any reference point. In fairness, all reasonable options for the potential patient should be factored into SA measures. Therefore, travel impedance is a poor indicator of availability. Combined measures of travel impedance (accessibility) and supply (availability) are necessary to properly understand spatial accessibility [19].
Average travel impedance to provider is intriguing because it is a combined measure of accessibility and availability. It, too, is measured from any patient or population point of interest. From that point the travel impedance to all providers within a system is summed and averaged. The "system" might be a city or county. To the author's knowledge this measure has only been used once for a health services study [51]. It has two shortcomings. First, it over-weights the influence of providers located near the periphery of the study area. To illustrate for a large city, providers at the northern periphery may not be a practical option for residents near the southern periphery. Including these providers inflates the average distance, thereby decreasing apparent SA for those residents. An additional problem concerns border crossing. As with the provider-to-population ratios, patients routinely cross geopolitical boundaries to seek nearby healthcare services.
Gravity models are also a combined indicator of accessibility and availability. A modified version of Newton's Law of Gravitation, they were initially developed to predict retail travel [52] and help with land use planning [53]. They can provide the most valid measures of spatial accessibility, be the setting urban or rural. Gravity models attempt to represent the potential interaction between any population point and all service points within a reasonable distance, discounting the potential with increasing distance or travel impedance. Because gravity measures take into account all alternative service points, they are sometimes referred to as cumulative opportunity measures.
The simplest formula for gravity-based accessibility is:

A i is spatial accessibility from population point i, which may be a residence or the centroid of an area of interest such as a census tract. S j is service capacity at provider location j. It is typically measured as the count of professional FTEs at a clinic, but may be some other preferred measure of capacity. d is the travel impedance, e.g. distance or travel time, between points i and j. β is a gravity decay coefficient, sometimes referred to as the travel friction coefficient. β represents the change in difficulty of travel as travel time or distance change. SA improves as the summed provider capacity (numerator) increases, or the summed travel impedance (denominator) decreases.
Gravity values can be used in many ways. For example if A i is estimated for numerous points in a region of study a continuous three-dimensional surface of accessibility can be estimated from the point values. Areas with low values would correspond to areas of relatively poor access and the high point values would indicate areas of potential over-service. In another example, A i values might be estimated at multiple representative points within each of a sample of cities, and the cities can then be compared for variation in average Ai.
In spite of its elegance there are at least two problems with the simple gravity formulation. First, the A i value is not intuitive to healthcare workforce policy makers, who prefer to think of spatial accessibility in terms of provider-to-population ratios or simple distance, despite the aforementioned difficulty of applying ratios to urban communities. Second, it only models supply. There is no adjustment for demand. Therefore, A i at a given distance from two providers would appear to be the same, even if one provider were serving 1,000 people in her catchment area and the other were serving 5,000. Clearly the two providers are not equally accessible.
Joseph and Bantock [15] proposed a solution to the latter problem by adding a population demand adjustment factor, V j , to the denominator. The factor spatially distributes population demand in the same way that the previous formula distributes provider supply:

P k is population size at point k, the centroid of a census tract or block, for example. d is the distance between the population point and provider location j. The demand on provider location j is obtained by summing the gravity-discounted influence of all population points within a reasonable distance.
The improved gravity model is thus:

It is challenging for new students of spatial accessibility to grasp this model. Another problem is that the distance decay coefficient, β, is usually unknown and might take many mathematical forms, such as linear or exponential. Its form and magnitude can vary greatly with the service type and population under study [54]. Empirical investigation is required to estimate β, and there is little in the primary care service literature to suggest probable values in the meantime. Notwithstanding these caveats, the improved gravity model could prove to be very valuable for primary care accessibility studies.
Recent developments
Several new SA measurements and methods are in the works, with the potential for improving our understanding of SA of primary care.
Two-step floating catchment area
Provider source data are not always of the quality or spatial resolution needed for gravity-based estimations of SA. This most commonly occurs when working with the American Medical Association and American Osteopathic Association (AMA/AOA) membership list. Sometimes only the provider's ZIP code is available, and sometimes it is not clear if the address corresponds to clinic location. In these situations the provider location is usually "assigned" to a ZIP code centroid. This loss of resolution might account for the lack of gravity-based studies of primary care in the literature.
Luo and Wang [5] are attempting to address this problem with a derivation of the "floating catchment area" method first used by Peng [55] to study urban job accessibility. They are working with the 10-county Chicago consolidated metropolitan statistical area, which includes a great deal of rural area. They begin by declaring a reasonable drive time for primary care – 30 minutes as suggested by Lee [56].
In their two-step process a provider-to-population ratio is first estimated for each provider location (ZIP code centroid). The number of providers assigned to the ZIP centroid is divided by the population living within that centroid's 30-minute drive time catchment. The provider-to-population ratio so obtained is assigned to the entire catchment area, not just the centroid upon which it was based. This ZIP-centered catchment ratio computation is repeated for all ZIP centroids. (In essence, the focus of the calculation is "floated" over all ZIP centroids, hence the method's name.) The map resulting from this first step shows overlapping irregularly shaped ZIP-centered catchment areas. In sparsely populated areas with large ZIP codes there are also areas not covered by any catchment area, and hence having no apparent primary care service.
In the second step population points are the focus. Examples might include residences, tract centroids or ZIP centroids, depending on the resolution possible with the data. For each population point an SA value is obtained by summing the provider-to-population ratios of all the first step provider catchments that overlie the point. The summed supply ratios so obtained are assigned to the entire area represented by the population point. Thus all population areas, e.g. census tracts, have an assigned SA value (zero in some cases).
The SA values are in the familiar units of provider-to-population. Luo and Wang mathematically demonstrate that their method is a special case of the Joseph and Bantock [15] improved gravity model. They also show that the method takes care of the geopolitical border-crossing conundrum, and they make a strong case that this kind of work can improve or inform efforts to redefine Health Professional Shortage Areas and Medically Underserved Areas/Populations.
Luo and Wang recognize that the method has limitations. While geopolitical borders are well handled, the drive-time catchment borders are themselves artificially sharp. SA near the periphery of the catchment is as high as at the center, and drops to zero just over the line. They performed sensitivity analyses to determine how drive times thresholds ranging from 20 to 50 minutes affected variation in estimated SA. The change was gradual, with longer drive times producing less variation. However, this sensitivity test is less relevant than one that would reveal the association of SA with utilization rates, were such data available. Finally, Luo and Wang plan to improve the method by adding an adjustment for variation in transportation options between census areas.
Compound gravity model
This unpublished model is being developed for the study of SA of healthcare services in New Mexico by the University of New Mexico Division of Government Research (DRG), under contract for the New Mexico Health Policy Commission (Baca, [57] and Laurence Spear, personal communication.) It is similar to the improved gravity model of Joseph and Bantock [15], described above. However, reference points for provider influence and population influence (i.e. "need") are the same – ZIP code centroids. All persons and providers within the ZIP are assigned to the same point. For the compound gravity model SA is expressed as a population-to-provider ratio, and is estimated for each ZIP point. It is a trivial matter to reverse the numerator and denominator to achieve the familiar provider-to-population ratio.
The numerator is a simple gravity model of population influence at the ZIP point. The denominator is a simple gravity model of provider influence at the same point. In both terms distance decay, β, is a weighting scheme with three levels. The 35-mile radius around the reference point is assumed to be a friction-free zone. Hence all providers and residents in this zone are fully weighted, i.e. multiplier is 1.0. Providers and residents outside a 100-mile radius are considered inaccessible and receive a zero weight. Providers and persons in the intermediate zone are discounted by the inverse square of their distance from the reference point.
The New Mexico team is applying this SA model to the study of hospital beds, general dentists, and registered nurses, as well as primary care physicians. They recognize that resolution is lost by working at the ZIP code geography level. There are also concerns about assuming equal accessibility within the 35-mile range, particularly in urban areas, and applying the same distance decay scheme to a variety of health service types.
Kernel density method
The applications described above require specialized programming skills. Our GIS lab is developing an SA measure that can be computed using off-the-shelf components of ArcGIS, the most popular GIS software suite. Our work was suggested by Guptill's [58] marriage of the gravity and provider ratio methods in his study of Detroit physician locations. He created a continuous density layer from these points to represent physician accessibility across the entire city. (A density surface is a mathematical relative of classic gravity formulations.) Guptill overlaid his physician density layer with neighborhood borders. This permitted him to calculate the average physician density for each neighborhood. It was then a simple matter to estimate neighborhood physician-to-population ratios by dividing the community's average physician density by its population. Patient border crossing was accounted for because the density calculation, often referred to as a "smoothing" process [59, 60] allocated each physician's availability into all neighborhoods that could reasonably rely on that physician.
Our method [3] uses an approach that is free of the compromises Guptill found necessary, given the limitations of computing power and data in the early 1970s. We are able to include all medical specialties relevant to primary care, and we are not forced to group physicians into single point locations such as ZIP centroids. Rather, we can analyze them at street address resolution.
We begin by creating a continuous map layer representing the density of primary care providers. Density layers are made of small cells (one tenth square mile in our case) covering the entire study region. The provider density value associated with each cell is an estimate of spatial accessibility at the cell's center. We use the "Gaussian kernel" method to calculate the density value of each cell. This is a preprogrammed option in the ArcGIS Spatial Analyst module. The computational details are beyond the scope of this paper, but the quadratic approximation formula is well described at the web site of Quantitative Decisions, Inc. [61] (Also, see Longley et al. [62], McLafferty [59], and Silverman [63] for thorough discussions and examples of kernel density estimation.) With this method each provider is represented on a map surface by a cone (kernel), centered at the provider's office location. Cone volume reflects the provider's total capacity for service, conveniently assumed to be 1.0. The radius of the cone base reflects what is believed to be the extent of the provider's practical service area. A previous survey of city residents suggested that a 3-mile radius was a reasonable estimate for cone radius, i.e. the distance beyond which provider attractiveness was negligible.
The Gaussian kernel method allocates provider capacity to the cells underlying the cone in such a way that cells near the cone center receive higher values of service capacity (i.e. accessibility), and those near the periphery of the cone receive very little. In other words, a cell's accessibility value is inversely related to its distance from the cone's center. The density values of all cells covered by the cone sum to 1.0.
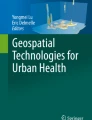
Provider cones frequently overlap, either partially or fully, as in the case of physicians belonging to the same practice. Cells in these overlapping areas receive an accessibility score (density value) that is the sum of contributions from all overlying cones. Therefore the summed cones above a large practice can be quite peaked. As a measurement refinement, a given provider's cone volume (service capacity) can be adjusted for any number of factors. For example, in our study of pediatric services we weighted full time clinical pediatricians with a factor of 1.0, and discounted family practitioners, general practitioners and residents following the American Academy of Pediatric guidelines [64]. The resulting density layer for our sample city, Washington, DC, is the top layer in Figure 1. The large mound in the center of the layer represents the summed influence of clinicians located at central-city hospitals.

Kernel densities of pediatric services (top) and children (middle). Bottom layer is the two-dimensional representation of populated areas of Washington, DC.
Improving on Guptill's method, we also created a population density layer from census block group points (middle of Figure 1.) This layer has the same cell size and extent as the provider density layer above it. With ArcGIS "map algebra" it is a simple matter to create a mathematical combination of these layers. We divided each cell's provider density by its corresponding population density to obtain a layer of one-tenth square mile cells having provider-to-population ratio values. This layer of cell ratio values can clearly reveal variations in spatial accessibility of providers across the city in units that are easily understood. The result is shown in Figure 2 in two dimensions (Kafadar [60] performed a similar operation with a disease density layer and a population layer. Her layers were combined in a different way for a different purpose – to discover areas of disease clustering).

Layer of provider-to-population ratios overlaid by census tract borders, Washington, DC.
The final step was to overlay the ratio surface with census tract borders (the black lines in Figure 2), and compute the mean cell ratio within each tract. The mean cell ratio is our estimate of SA for the tract. We can then test for variation in spatial accessibility across socioeconomic gradients, such as tract median income and percent of minority residents. The maps are presented here only as a demonstration of the method. Readers are referred to Guagliardo, et al [3] for a careful interpretation of the maps and results of our pilot study.
Our method solves some but not all of the problems associated with other methods. The three-mile cone radius may not be any better than the time or distance cut-off values used in the other methods. Also, just as the nature of distance decay, β, may not be well understood for gravity models, neither can we be certain that a Gaussian (normal) curve is the best model for decay of provider influence with increasing distance. We have not adjusted our measure to account for transportation options, which may vary considerably between neighborhoods. Finally, our population and provider density cones, with their fixed radii, are similar to straight-line distance indicators of SA. It would be more desirable to compute provider and population density based on transportation routes rather than straight-line distance. To the author's knowledge such a method does not exist.
Further caveats
For researchers interested in the SA of primary care there are limitations beyond those previously mentioned. First, physicians do not provide all primary care. Mid-level providers (physicians assistants and nurse practitioners) provide considerable care in some areas [65, 66]. It would be useful to include them in SA estimates when geocodable data are available. Researchers should also be aware of that some physicians practice at multiple sites, but only one may be listed in membership databases [67].
Stimson [68] defines five categories of potential pitfalls for SA studies of healthcare delivery. First, he warns researchers to be aware of possible inaccuracies in their source data sets. A common example is misspellings and other errors in mailing addresses, or the misrepresentation of provider home addresses as clinic addresses in professional association membership lists. Incompleteness of data sources is another potential problem. For example, all U.S. physicians in clinical practice are not represented in the American Medical Association/American Osteopathic Association membership list. If representation is spatially biased this could result in a misrepresentation of the distribution and extent of service. A third problem is unwarranted causal inferences from ecological associations. To illustrate, it might be found that physicians are less common in minority than non-minority communities, implying a prejudice against minority patients. However, in many urban areas community racial/ethnic composition is correlated with income and crime rates. Therefore researchers should attempt to determine whether practice location is driven by monetary or safety concerns rather than an aversion to minority patients. Stimson further warns that data may not be sufficiently disaggregated to the smallest scale. For example, if a study is concerned with service distribution over the entire U.S. then provider statistics aggregated to the county level should provide satisfactory resolution. In contrast, if a study is focused on neighborhood level disparities in SA then aggregation of provider counts by postal code might not even be sufficient. Census tract or census block aggregations could be necessary, and perhaps even street address level data could be required. Stimson's final warning concerns data sets that do not correspond in scale or time. Providers and populations shift location over time, the well-known phenomena of urban decay and urban renewal being classic examples. It would be inappropriate to compare 1997 provider locations with 1990 U.S. decennial census data for a given city.
Researchers should also be aware that communities differ with regard to the transportation system efficiency and the number of transportation mode options [69, 70]. While some researchers have recognized the implications of this variation for SA studies, we should work to develop quantitative adjustments for its effect on measured SA.
Others have argued that daily activity spaces are more representative of an individual's "location" than residential address [24, 71]. Patients may find it convenient to obtain primary care near their work or shopping locations, a convenience that is overlooked by traditional studies based on residential address. Kwan [72–78] is working to address this problem for all forms of social science inquiry. She and colleagues ask subjects to keep daily activity diaries to record their movements and time of day. From these data Kwan builds 3-dimensional models – time being the third dimension – of subject movement. These "aquarium" visualizations of personal location and movement are remarkable and can reveal how very different, spatially and temporally, life can be for different gender and race/ethnicity groups. Figure 3, provided by Kwan, is a good illustration. It shows how existence in space-time differs for samples of African-American and Asian women in Portland, Oregon. It might be fruitful for health services researchers to attempt to match the space-time representation of the residents of various communities with the space-time availability of primary care providers in order to better identify gaps and disparities in space-time accessibility. Unfortunately the diary data are difficult to collect and the modeling methods are not yet generally available to researchers.

Space-time "aquarium" showing the paths of African American (purple) and Asian American (blue) women in Portland, Oregon, over the course of a typical day. The vertical dimension is time. (Reprinted with the permission of the creator, Mei-Po Kwan, Department of Geography, Ohio State University.)
That residential address may be an inadequate proxy for a person's location may be of less concern for pediatric primary care studies. A large proportion of children's lives are spent at home or in neighborhood schools. Most parents prefer to use pediatric services close to home, for convenience and sense of security. Still, the line of inquiry that Kwan is pursing holds much promise.
Conclusions
There is a long history in the U.S. of interest in local provider supply and travel distance. However, the role of these factors in maintaining population health would be better appreciated if researchers and policy makers gave consistent and due consideration to the various stages and dimensions of healthcare access. A simple taxonomy of access studies, such as the one presented in this paper, can bring these dimensions and stages into relief, and help researchers to refine questions and gather data in the most appropriate manner. The taxonomy helps to clarify where spatial accessibility studies fit in the broader scheme of access studies.
Most research has dealt with simple distance to nearest provider, or provider-to-population ratios, i.e. supply levels, within bordered areas. These have been useful for rural areas and for large-scale geographies, where they have linked distance or supply with rates or odds of healthcare utilization. However, these methods have significant limitations. Measures of supply level are only appropriate for suitably large geographies and cannot detect variations in supply within large bordered areas. Measures of distance or travel time to nearest provider ignore the potential service of providers that may be located only a short distance further. Neither of these measures is satisfactory for congested urban areas, where most of the population resides. The result is that we have a relatively small literature with respect to the geography of primary care, and many very basic questions remain.
To surmount these problems researchers are beginning to combine the concepts of distance and supply under the rubric "spatial accessibility" (SA). This is a timely development, as the geographic information systems necessary to exploit these newer methods are becoming more powerful, commonplace and easier to use. There are at least three new measures of SA under development. All have a mathematical relation to the classic gravity decay formulations that have been used in the social sciences for decades, but which are not easily applied to the data commonly available for primary care research. As a group they are improvements on previous methods. Yet none is without its own problems, and researchers would be hard-pressed to choose from among them. A grand study comparing their relative sensitivities to healthcare utilization rates is needed to sort things out.
Finally, it should be noted that nearly all primary care SA studies to date, whether based on simple or complex measures, have been limited to the exploration of social inequity in access, or the impact of SA on healthcare utilization. The body of work will be greatly advanced when we begin to precisely quantify how the SA of primary care actually impacts population health. This is a challenge made more difficult by recent regulations to protect patient privacy, including patient street address. Nonetheless, concerted efforts are needed to overcome these barriers in order to obtain health data at the very fine spatial resolutions needed. The payoff is potentially very great.
Abbreviations
- ACSC -:
-
ambulatory care sensitive conditions
- MAUP –:
-
modifiable area unit problem
- SA –:
-
spatial accessibility
References
Khan AA, Bhardwaj SM: Access to health care. A conceptual framework and its relevance to health care planning. Eval Health Prof. 1994, 17: 60-76.
Penchansky R, Thomas JW: The Concept of Access. Med Care. 1981, 19 (2): 127-140.
Guagliardo MF, Ronzio CR, Cheung I, Chacko E, Joseph JG: Physician accessibility: An urban case study of pediatric primary care. Health and Place. 2004
Luo W: Using a GIS-based floating catchment method to assess areas with shortage of physicians. Health and Place. 2004, 10 (1): 1-11. 10.1016/S1353-8292(02)00067-9.
Luo W, Wang F: Measures of spatial accessibility to healthcare in a GIS environment: Synthesis and a case study in Chicago region. Environment and Planning B. 2003, 30 (6): 865-884. 10.1068/b29120.
Hunter JM, Shannon GW, Sambrook SL: Rings of madness: service areas of 19th century asylums in North America. Soc Sci Med. 1986, 23 (10): 1033-1050. 10.1016/0277-9536(86)90262-5.
Jarvis E: On the supposed increase in insanity. Am J Insanity. 1852, 8: 333-364.
Shannon GW, Dever GEA: Health Care Delivery: Spatial Perspectives. 1974, New York, McGraw-Hill
Morrill RL, Earickson RJ, Rees P: Factors influencing distances traveled to hospitals. Economic Geography. 1970, 46 (2): 161-171.
Wennberg J, Gittelsohn A: Small area variations in health care delivery. Science. 1973, 182: 1102-8.
Elesh D, Schollaert PT: Race and urban medicine: factors affecting the distribution of physicians in Chicago. J Health Soc Behav. 1972, 13: 236-50.
U.S. Public Health Service, Ciocco A: Medical Service Areas and Distances Traveled for Physician Care in Western Pennsylvania. 1954, Washington, U. S. Govt. Print. Off
U.S. National Advisory Commission on Health Manpower: Report. 1967, Washington, U.S. Govt. Print. Off
Goodman DC, Fisher E, Stukel TA, Chang C: The distance to community medical care and the likelihood of hospitalization: Is closer always better?. Am J Public Health. 1997, 87: 1144-50.
Joseph AE, Bantock PR: Measuring potential physical accessibility to general practitioners in rural areas: a method and case study. Soc Sci Med. 1982, 16: 85-90. 10.1016/0277-9536(82)90428-2.
Shi L, Starfield B, Kennedy B, Kawachi I: Income inequality, primary care, and health indicators. J Fam Pract. 1999, 48: 275-84.
Fortney J, Rost K, Warren J: Comparing Alternative Methods of Measuring Geographic Access to Health Services. Health Services and Outcomes Research Methodology. 2000, 1 (2): 173-184. 10.1023/A:1012545106828.
Connor RA, Hillson SD, Krawelski JE: Competition, professional synergism, and the geographic distribution of rural physicians. Med Care. 1995, 33: 1067-78.
Fryer GE, Drisko J, Krugman RD, et al: Multi-method assessment of access to primary medical care in rural Colorado. J Rural Health. 1999, 15 (1): 113-121.
Salsberg ES, Forte GJ: Trends in the physician workforce, 1980–2000. Health Aff (Millwood). 2002, 21: 165-73. 10.1377/hlthaff.21.5.165.
Smedley BD, Stith AY, Nelson AR, Institute of Medicine (U.S.), Committee on Understanding and Eliminating Racial and Ethnic Disparities in Health Care: Unequal Treatment Confronting Racial and Ethnic Disparities in Health Care. 2002, Washington, D.C, National Academy Press
Council on Graduate Medical Education: Tenth Report: Physician Distribution and Health Care Challenges in Rural and Inner-City Areas. 1998, Washington, DC, U.S. Department of Health and Human Services, Public Health Service, Health Resources and Services Administration
Heinrich , Janet : Health Workforce: Ensuring Adequate Supply and Distribution Remains Challenging. 2001, General Accounting Office
Gesler WM, Meade MS: Locational and population factors in health care-seeking behavior in Savannah, Georgia. Health Serv Res. 1988, 23 (3): 443-462.
McGuirk MA, Porell FW: Spatial patterns of hospital utilization: the impact of distance and time. Inquiry. 1984, 21: 84-95.
Barnett JR: Race and physician location: Trends in two New Zealand urban areas. New Zealand Geographer. 1978, 34 (1): 2-12.
Fortney J, Rost K, Zhang M, Warren J: The impact of geographic accessibility on the intensity and quality of depression treatment. Med Care. 1999, 37: 884-93. 10.1097/00005650-199909000-00005.
Fortney JC, Booth BM, Blow FC, Bunn JY: The effects of travel barriers and age on the utilization of alcoholism treatment aftercare. Am J Drug Alcohol Abuse. 1995, 21: 391-406.
Athas WF, Adams-Cameron M, Hunt WC, Amir-Fazli A, Key CR: Travel distance to radiation therapy and receipt of radiotherapy following breast-conserving surgery. J Natl Cancer Inst. 2000, 92: 269-71. 10.1093/jnci/92.3.269.
Nattinger AB, Kneusel RT, Hoffmann RG, Gilligan MA: Relationship of distance from a radiography facility and initial breast cancer treatment. J Natl Cancer Inst. 2001, 93 (17): 1344-1346. 10.1093/jnci/93.17.1344.
Meden T, St. John-Larkin C, Hermes D, Sommerschield S: MSJAMA. Relationship between travel distance and utilization of breast cancer treatment in rural northern Michigan. JAMA. 2002, 287 (1): 111-10.1001/jama.287.1.111.
Goodman DC, Fisher ES, Gittelsohn A, Chang CH, Fleming C: Why are children hospitalized? The role of non-clinical factors in pediatric hospitalizations. Pediatrics. 1994, 93: 896-902.
Billings J, Teicholz N: Uninsured patients in the District of Columbia Hospitals. Health Aff (Millwood). 1990, 9 (4): 158-165. 10.1377/hlthaff.9.4.158.
Basu J, Friedman B: Preventable illness and out-of-area travel of children in New York counties. Health Econ. 2001, 10: 67-78. 10.1002/1099-1050(200101)10:1<67::AID-HEC562>3.0.CO;2-K.
Basu J, Friedman B, Burstin H: Primary care, HMO enrollment, and hospitalization for ambulatory care sensitive conditions: a new approach. Med Care. 2002, 40: 1260-9. 10.1097/00005650-200212000-00013.
Parchman ML, Culler SD: Preventable hospitalizations in primary care shortage areas. An analysis of vulnerable Medicare beneficiaries. Arch Fam Med. 1999, 8: 487-91. 10.1001/archfami.8.6.487.
Gulliford MC: Availability of Primary Care Doctors and Population Health in England: Is There an Association?. J Public Health Med. 2002, 24 (4): 252-254. 10.1093/pubmed/24.4.252.
Shi L, Starfield B: The effect of primary care physician supply and income inequality on mortality among blacks and whites in US metropolitan areas. Am J Public Health. 2001, 91: 1246-50.
Goodman DC, Fisher ES, Little GA, Stukel TA, Chang CH: Are neonatal intensive care resources located according to need? Regional variation in neonatologists, beds, and low birth weight newborns. Pediatrics. 2001, 108: 426-31.
Goodman DC, Fisher ES, Bubolz TA, Mohr JE, Poage JF, Wennberg JE: Benchmarking the US physician workforce. An alternative to needs-based or demand-based planning. JAMA. 1996, 276: 1811-7. 10.1001/jama.276.22.1811.
Wennberg JE, Freeman JL, Culp WJ: Are hospital services rationed in New Haven or over-utilised in Boston?. Lancet. 1987, 1: 1185-9. 10.1016/S0140-6736(87)92152-0.
Weinstein JN, Goodman D, Wennberg JE: The orthopaedic workforce: which rate is right?. J Bone Joint Surg Am. 1998, 80: 327-30.
Parker JD, Schoendorf KC: Variation in hospital discharges for ambulatory care-sensitive conditions among children. Pediatrics. 2000, 106: 942-8.
Krakauer H, Jacoby I, Millman M, Lukomnik JE: Physician impact on hospital admission and on mortality rates in the Medicare population. Health Serv Res. 1996, 31: 191-211.
Reid FD, Cook DG, Majeed A: Explaining variation in hospital admission rates between general practices: cross sectional study. Br Med J. 1999, 319: 98-103.
Billings J, Zeitel L, Lukomnik J, Carey TS, Blank AE, Newman L: Impact of socioeconomic status on hospital use in New York City. Health Aff (Millwood). 1993, 12 (1): 162-73. 10.1377/hlthaff.12.1.162.
Gesler W: The uses of spatial analysis in medical geography: a review. Soc Sci Med. 1986, 23 (10): 963-73. 10.1016/0277-9536(86)90253-4.
Schonfeld HK, Heston JF, Falk IS: Numbers of physicians required for primary medical care. N Engl J Med. 1972, 286: 571-6.
Connor RA, Kralewski JE, Hillson SD: Measuring geographic access to health care in rural areas. Med Care Rev. 1994, 51: 337-77.
Openshaw S: The Modifiable Areal Unit Problem. 1984, Norwick Norfolk, Geo Books
Dutt AK, Dutta HM, Jaiswal J, Monroe C: Assessment of service adequacy of primary health care physicians in a two county region of Ohio, U.S.A. GeoJournal. 1986, 12: 443-455.
Reilly WJ: The Law of Retail Gravitation. 1931, New York, Knickerbocker Press
Hansen WG: How accessibility shapes land use. J Am Inst Plann. 1959, 25: 73-76.
Talen E, Anselin L: Assessing spatial equity: An evaluation of measures of accessibility to public playgrounds. Environment and Planning A. 1998, 30: 595-613.
Peng Z: The jobs-housing balance and urban commuting. Urban Studies. 1997, 34: 1215-1235. 10.1080/0042098975600.
Lee RC: Current approaches to shortage area designation. J Rural Health. 1991, 7: 437-50.
Health Care Facilities/Provider Gravity Model. [http://www.unm.edu/~drgint/hpc_grav.html]
Guptill SC: The Spatial Availability of Physicians. Proceedings of the Association of American Geographers. 1975, 7: 80-84.
McLafferty S, Williamson D, McGuire PG: Identifying Crime Hot Spots Using Kernel Smoothing. In Analyzing Crime Patterns: Frontiers of Practice. Edited by: Goldsmith V, McGuire PG, Mollenkopf JB, Ross TA. 1999, Thousand Oaks, CA: Sage Publications, 77-85.
Kafadar K: Smoothing geographical data, particularly rates of disease. Stat Med. 1996, 15: 2539-60. 10.1002/(SICI)1097-0258(19961215)15:23<2539::AID-SIM379>3.3.CO;2-2.
Density Calculations. [http://www.quantdec.com/SYSEN597/GTKAV/section9/density.htm]
Longley PA, Goodchild MF, Maguire DJ, Rhind DW: Geographic Information Systems and Science. 2001, Chichester, NY, Wiley
Silverman BW: Density Estimation for Statistics and Data Analysis. 1986, New York, Chapman and Hall
American Academy of Pediatrics: Physician Workforce: Ratios for Child Health, 1998. 2000, Elk Grove Village, Illinois, American Academy of Pediatrics
Cooper RA, Laud P, Dietrich CL: Current and projected workforce of nonphysician clinicians. JAMA. 1998, 280: 788-94. 10.1001/jama.280.9.788.
Hooker RS, McCaig LF: Use of physician assistants and nurse practitioners in primary care, 1995–1999. Health Aff (Millwood). 2001, 20 (4): 231-8. 10.1377/hlthaff.20.4.231.
Cromley EK, Albertsen PC: Multiple-site physician practices and their effect on service distribution. Health Serv Res. 1993, 28: 503-22.
Stimson RJ: Research design and methodological problems in the geography of health. In Geographical Aspects of Health. Edited by: McGlashan ND, Blunden JR. 1983, London: Academic Press, 322-334.
Bostock L: Pathways of disadvantage? Walking as a mode of transport among low-income mothers. Health and Social Care in the Community. 2001, 9 (1): 11-18. 10.1046/j.1365-2524.2001.00275.x.
Kimes D, Ullah A, Levine E, et al: Relationships between pediatric asthma and socioeconomic/urban variables in Baltimore, Maryland. Health and Place. 2004
Cromley EK, Shannon GW: Locating ambulatory medical care facilities for the elderly. Health Serv Res. 1986, 21: 499-514.
Kim H-M, Kwan M-P: Space-time accessibility measures: A geocomputational algorithm with a focus on the feasible opportunity set and possible activity duration. Journal of Geographical Systems. 2003, 5: 71-91. 10.1007/s101090300104.
Kwan M-P: Interactive geovisualization of activity-travel patterns using three-dimensional geographical information systems: A methodological exploration with a large data set. Transportation Research Part C. 2000, 8: 185-203. 10.1016/S0968-090X(00)00017-6.
Kwan M-P: Space-time and integral measures of individual accessibility: A comparative analysis using a point-based framework. Geographic Analysis. 1998, 30: 191-217.
Kwan M-P: Gender and individual access to urban opportunities: A study using space-time measures. Professional Geographer. 1999, 51: 210-227.
Kwan M-P, Janelle DG, Goodchild MF: Accessibility in space and time: A theme in spatially integrated social science. Journal of Geographical Systems. 2003, 5: 1-3. 10.1007/s101090300100.
Kwan M-P, Murray AT, O'Kelly ME, Tiefelsdorf M: Recent advances in accessibility research: Representation, methodology and applications. Journal of Geographical Systems. 2003, 5: 129-138. 10.1007/s101090300107.
Weber J, Kwan M-P: Bringing time back in: A study on the influence of travel time variations and facility opening hours on individual accessibility. The Professional Geographer. 2002, 54 (2): 226-240.
Acknowledgements
This review was supported by grant number 1P20MD000165-01 from the National Center on Minority Health and Health Disparities, NIH (Jill G. Joseph, MD, PhD, principal investigator). It is based on a presentation made at the 18th Annual Primary Care Research Methods and Statistics Conference, San Antonio, Texas, 2003. Cynthia R. Ronzio, PhD provided many ideas and useful comments. Mei-Po Kwan of the Department of Geography, Ohio State University was kind enough to allow the use of Figure 3, which she created. The author also wishes to thank the anonymous reviewers for helpful suggestions.
Author information
Authors and Affiliations
Corresponding author
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Guagliardo, M.F. Spatial accessibility of primary care: concepts, methods and challenges. Int J Health Geogr 3, 3 (2004). https://doi.org/10.1186/1476-072X-3-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-072X-3-3