
Abstract
Background
Diarrhoeal diseases constitute a major public health problem, particularly in the developing world, where the rate of mortality and morbidity is very high. The purpose of this study was to conduct a 2 years and 3 months study in order to determine the prevalence of five enteropathogen diarrheogenic agents in Mexico City.
Methods
Faecal samples were obtained from 300 Mexican children diagnosed as positive for diarrhoea, aged > 2 to < 12 years old, and from 80 children matched for age but with no symptoms of the disease (control group). Two multiplex PCR were used to detect Escherichia coli, Salmonella spp., and Shigella spp. In addition, the two protozoan parasites Entamoeba histolytica/Entamoeba dispar and Giardia intestinalis were detected by conventional methods.
Results
All diarrhoeal samples were positive for one or more enteropathogens. The most common enteropathogens in diarrhoeal samples were E. histolytica/E. dispar (70.3%), Salmonella (ohio 28.3%; typhimurium 16.3%; infantis 8%; anatum 0.6%; Newport 0.3%), G. intestinalis (33%), E. coli (ETEC 13.3%; EPEC 9.3%; VTEC 8.6%; EIEC 1%) and Shigella spp. (flexneri 1.6%, sonnei 1%). Infections by two (24%) three (16%) and four (12%) pathogens were observed.
Conclusion
This study revealed that 52% of the patients were infected by more than one enteropathogen, notably E. histolitica/E. dispar and Salmonella ohio. These results are useful for clinicians to improve the empiric treatment used in such cases.
Similar content being viewed by others

Background
Diarrhoeal diseases constitute a major public health problem, particularly in the developing world, where the rate of mortality and morbidity is very high [1]. The World Health Organization (WHO) has estimated that 1.5 billion episodes of diarrhoea occur every year in developing countries, resulting in 3 million deaths [2]. In Mexico, a governmental study conducted in the year 2003 reported 4556 cases caused by intestinal infectious [3]. The etiological agents of diarrhoea described in epidemiological studies are transmitted as waterborne and foodborne.
Some foodborne pathogens have been recently considered as emerging diseases [4], despite the fact they have been known since a long time ago. For example, outbreaks of salmonellosis have been described for many decades, and yet their incidence have increased over the last 25 years. Diarrhoeal infections can be caused by many etiological agents, but mainly by enterobacteria such as Escherichia coli, Salmonella spp., Shigella spp., Campylobacter jejuni and Vibrio cholerae; as well as parasites such as Entamoeba histolytica and Giardia intestinalis, and some rotaviruses are also important agents [5].
Escherichia coli is considered as the etiological agent for many diseases including some affecting the urinary tract and intestine. The classification of diarrhoegenic E. coli strains is based on their virulence properties, and comprises six groups: Enterotoxigenic E. coli (ETEC), Enteropathogenic E. coli (EPEC), Enteroinvasive E. coli (EIEC), Enterohaemorragic E. coli (EHEC), Enteroaggregative E. coli (EAggEC) and Diffuse Adhering E. coli (DAEC) [6]. Salmonella spp. is a facultative, gram negative, flagellated member of the Enterobacteriaceae family. The most extensive accepted classification of Salmonella strains is based on the diversity of two differentially expressed H flagellar antigens: flagellin phase I and phase II antigens (codified by fli C and flj B genes), and the O antigens of the bacterial lipopolysaccharide, both determined by serotyping [7]. Until now, 2501 serotypes have been described [8]; which turns Salmonella classification into a complex and laborious process in the clinical laboratory; therefore, several PCR based methods have recently been developed, and were reported to be a simple, highly sensitive, fast and reliable alternative when compared to traditional clinical laboratory methods [9, 10].
Shigella is a Gram negative, non-motile, rod-shaped bacteria, closely related to E. coli and Salmonella, and it is the etiological agent of human shigellosis and dysentery, which is characterized by severe diarrhoea with the presence of blood in the faeces. Classification of Shigella is based on serotyping, and comprise the following groups and serotypes: Serogroup A (S. dysenteriae) 12 serotypes, serogroup B (S. flexneri) 6 serotypes, serogroup C (S. boydii) 23 serotypes and serogroup D (S. sonnei) with only one serotype [11].
Diarrhoea can also be caused by protozoa such as Entamoeba histolytica and Giardia intestinalis, these zoonotic parasites are frequently transmitted by consumption of water contaminated with infective cysts [12].
The purpose of this study was to determine the prevalence of five enteropathogen diarrheogenic agents namely E. coli, Salmonella spp., Shigella spp., E. histolytica/E. dispar and Giardia intestinalis in Mexico City. Stool specimens obtained from children patients from several communities in Mexico City were examined; the association patterns between different pathogens and its correlation with occurrence of diarrhoea were also described.
Materials and methods
Stool samples
A total of 300 stool samples were obtained from children patients with diarrhoea from different hospitals in Mexico City (patient group); also, 80 samples were obtained from children attending schools in the surrounding area, who did not had diarrhoea in the previous 45 days (control group). All subjects aged > 2 to < 12 years, and samples were collected from September 2004 through December 2006.
The selection criteria for inclusion of children patients with diarrhoea was having at least 3 or more soft, semisolid or liquid bloody faeces within 24 hours. Also, selection was made on the basis of a questionnaire filled up by all subjects with assistance of a relative over 18 years old, providing information regarding other gastrointestinal disorders, non-related diseases, travelling, frequency of diarrhoeal episodes, previous and current antibiotic treatment; as well as general data such as age, gender and place of residence. The control and patient groups were matched for age and sex.
Bacteriology
Stool samples were streaked on the surface of MacConkey agar (DIBICO, Mexico) for obtaining E. coli isolates and on sodium deoxycholate agar for the selection of Shigell a and Salmonella, and were incubated overnight at 37°C. All samples were tested for Shigella by using colony morphology, biochemical properties, and agglutination with specific antisera (Serobac, BioRad).
Multiplex PCR assays for the detection of E. coli and Shigella spp. were performed following a previously reported method [13], which selectively amplifies specific regions of several virulence genes: ETEC (eltB 322 bp, and estA 147 bp) VTEC (eaeA 376 bp, vt1 130 bp, and vt2 298 bp), EPEC (eaeA 376 bp, and bfpA 367 bp) EIEC (ial 320 bp), E. coli O157:H7 (fliC H7 625 bp, and O157, 500 bp) present in diarrhoegenic E. coli; however, although this method is also capable of detecting Shigella spp., it can not distinguish it from EIEC, since the amplification target used by this method is a region of the invasion-associated locus (ial), common to both species. Therefore, the presence of Shigella spp. was also confirmed by using specific antisera.
In order to molecularly serotype Salmonella spp., we used two previously described methods [9, 10], which makes use of the ability of Salmonella spp. to differentially express fli C gene (phase I) and flj B (phase II) flagellar H antigens, allowing the identification of the corresponding DNA variable internal regions (H:i, H:r, H:I, v, H:e, h, H:z10, H:b, H:d, for phase I; and H:1,2, H:1,5, H:1,6, H:1,7, H:I, w, H:e, n, x and H:e, n, z15 for phase II).
Positive controls containing template DNA of the following reference strains were used in every amplification round: ETEC ATCC 35401; EPEC ATCC 43887, EHEC ATCC 43890, EHEC ATCC 43889, EIEC ATCC 43893, E. coli ATCC 11775 (negative control without virulence genes), Salmonella typhimurium, Salmonella paratyphi B and Salmonella infantis. All primers used were obtained from Sigma Genosys (Sigma). Gel electrophoresis was photodocumented using a Gel Logic 100 Imaging system (KODAK). Molecular sizing of the amplicons was performed using KODAK Molecular Imaging Software.
Parasitology
Determination of E. histolytica/E. dispar and G.intestinalis was done using Faust method. Protozoa were concentrated by centrifugal-floatation (500 × g 2 min) using zinc sulphate as the diluent (specific gravity 1.19) and observed with a light microscope at 40× [14].
Statistical methods
Differences between isolation rates among patient and control groups were evaluated by the χ2 test.
Results
Stool samples
Sex distribution was similar in both groups: 55% of population were females and 45% were males. Sex distribution did not show to play an important role regarding enteropathogen prevalence. Regarding the patient group, 58% presented abdominal pain, vomit and fever (> 39°C); and 20% required oral rehydration. Ten percent of the stool samples obtained from this group presented blood.
Identification of enteropathogens
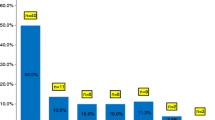
In the patient group, the predominant enteropathogen was E. histolytica/E. dispar (70.3%), followed by G. intestinalis (33%), S. ohio (28.3%), S. typhimurium (16.3%) and ETEC (13.3%); regarding the control group, E. histolytica/E. dispar (43.7%) was also the most commonly founded enteropathogen (Table 1), nevertheless, the prevalence of all detected enteropathogens was significantly different (P < 0.001).
The predominant pattern was comprised by a single enteropathogen infection (48%), followed by co infection involving two pathogens (24%), and being the less common co infection by four pathogens (12%) (Table 2).
In the control group, 27.5% stool samples were free of any of the bacterial enteropathogens analyzed, 62.5% were positive for one and 10% were positive for two enteropathogens (E. histolytica/E. dispar and G. intestinalis).
Multiplex PCR and detection of Enterobacteriaceae
Only 195 E. coli strains were detected in the stool samples (160/300 from patient group and 35/80 from control group); 46.6 % (140/300) of cases and 56.2% (45/80) of controls stools contain no E. coli. Analysis by multiplex PCR shows that only 101 out of 195 E. coli were positive (97/160, 60.6%) from patients and 4/35 (11.4%) from control group. Eight isolates from patients were further identified as Shigella (Table 1). The prevalence of diarrhoegenic E. coli in both groups was significantly different (P < 0.001). The frequencies of the diarrhoegenic E. coli positive for one of the targeted genes are shown in Table 3.
Regarding Salmonella spp., the most common species in the patient group was S. ohio (28.3%), followed by S. typhimurium (16.3%) and S. infantis (8.0%); compared with S. ohio (2.5%) and S. typhimurium (1.2%) in the control group (Table 1).
Discussion
The current study used a variety of diagnostic methods which helped estimate 100% prevalence of the enteropathogens in stool samples from children presenting diarrhoea symptoms. In addition, a high rate for multiple infections 156/300 (52%) was observed. However, not only the patient group had enteropathogens, also 50/80 (62.5%) members of the control group were positive for either one or two parasites (E. histolytica/E. dispar and Giardia intestinalis). Although only 4 (5%) of the control group were positive for diarrhoegenic E. coli (Table 3), they did not have any symptoms by the time this study was conducted. One of the strains detected in the controls was E. coli O157:H7, which has been recently described as an emerging pathogen worldwide [6, 15]. The high rate of enteropathogens detected in this study among both groups, reflects the importance of monitoring on a daily basis the most vulnerable population, such as low economic level children groups.
E. histolytica/E. dispar were the most frequently found enteropathogen in both, the patient (70.3%) and the control group (43.7%) (Table 1). Globally, amoebiasis is wide spread in approximately 20% of the world's population; 10% of those individuals get sick, and 0.1- 0.25% of them die. E. histolytica constitutes the third cause of death for parasitic diseases [16]. On the other hand, G. intestinalis a protozoa which causes symptomatic infections mainly in children under 12 years old was observed in 33% of the patient group, and 20% for the control group (Table 1). These results are in agreement with a previous study that reported G. intestinalis in 29.9% of a population group in Mexico City [17]. An interesting observation is that although 63.7% of the members of the control group were positive for E. histolytica/E. dispar and/or G. intestinalis (Table 1), none of them presented symptoms of disease.
We used three multiplex PCR methods that accurately detected specific genetic virulence markers of Salmonella spp., Shigella spp., and E. coli groups ETEC (eltB and estA gene fragments), EPEC (eaeA and bfpA gene fragments), VTEC (eaeA and vt1 or vt2 genes), EIEC/Shigella (ial region), and E. coli O157:H7 (fliC H7 flagellar antigen and a characteristic O157:H7 DNA fragment previously described) [18]. EIEC and Shigella are closely related regarding some of their virulence factors and phenotypic properties [19, 20], the multiplex PCR method employed in this study can not be used alone for a definitive discrimination between these two enteropathogens since it recognizes the ial locus, which can be found in both, EIEC and Shigella spp. Therefore, ial positive amplification isolates were considered as positive for EIEC if they showed no agglutination when challenged against specific antiserum for Shigella spp. Also, because elt B and ial amplicons are very close regarding their molecular size (322 and 320 bp respectively) (Fig. 1), two separate PCR reactions were done, each containing specific primers against elt B or ial in order to avoid the overlapping of amplification products, that might lead to false positives.

2.5% Agarose gel electrophoresis of E. coli amplicons obtained from diarrhoeal samples (run conditions 120 V, 94 mA, 45 min.). Lane 1: VTEC ATCC43889 and ATCC43890 strains (positive control). Lane 2: Negative control without template DNA. Lane 3: EPEC ATCC43887 strain (positive control). Lane 4: ETEC ATCC 35401 (positive control); Lane 5: EIEC ATCC43893 (positive control). Lane 6: E. coli ATCC11775 (avirulent strain, negative control). Lane 7: MWM 50-bp ladder. Lane 8: EPEC (patient group sample). Lane 9: negative sample (control group). Lane 10; negative sample (control group). Lane 11; VTEC (patient group sample). Lane 12; negative sample (patient group). Lane 13; EIEC (patient group sample). Lane 14; ETEC (patient group sample).
Diarrhoegenic E. coli was present in 32% of the patient group and 5% of the control group (Table 3); these data are consistent with a previous study conducted in Hanoi, Vietnam, where diarrhoegenic E. coli was detected by multiplex PCR, in 22.5 % of the patient group and 12% for the control group [21]. The presence of diarrhoegenic E. coli groups has been reported world wide and recognized as one of the major causes of deceases involving enteropathogens in children [22–26]. In Mexico and other developing countries in the world, ETEC is the most prevalent diarrhoegenic E. coli group [27, 28]. It is considered as an important pathogen in children, especially during the first six months, where the isolation rate ranges from 10 to 30% [29]. In this study, the presence of ETEC in the patient group (13.3%) was the highest compared to the other E. coli groups detected (Table 1). However, this rate is lower than what has been reported in some parts of the world, which reaches up to 20.7% [30, 31]. It seems that, regardless of the location, the presence of eltB gene (encoding thermo labile toxin) is a definitive advantage for ETEC, since in our study, the virulence gene distribution rate for eltB was high (6.6%). The same observation was reported by another studies conducted in Sweden [13] and Vietnam [21], where eltB was the most commonly found ETEC virulence gene in the studied groups. The second most commonly found diarrhoegenic E. coli strain was EPEC (9.3%), which has been reported responsible for a high rate of mortality and morbidity among children, especially in developing countries where poor sanitary conditions prevail [6]. For example, in countries such as Mexico [32, 33] and Brazil [34] up to 40% of diarrhoeal episodes in children are due to EPEC. Interestingly, regarding virulence gene homogeneity distribution, it seems that the situation for EPEC is not the same as for ETEC. A higher percentage of eae A+/bfp A- isolates (atypical strains) was found compared to eaeA +bfpA+ (typical strains) (Table 3), which differs from others studies conducted in Vietnam, where most of the isolates were eaeA +bfpA+ [21].
VTEC E. coli, an enteropathogen distributed worldwide, that has been more extensively studied in USA [35] and Europe [36] was also detected in this study. One strain of VTEC was detected in the controls whereas in the patient group it had a prevalence rate of 8.6% (26/300) (Table 1), of which 17/26 (65.4 %) possessed vt1, vt2 and eaeA; 19.2% (5/26) possessed vt2 and eaeA and 15.3% (4/26) vt1 and eaeA; being vt1 the most abundant genotype within this group (Table 3). These results differ from those reported by Svenungsson et al., [13] where vt1 was in fact the less commonly found genotype in their samples.
E. coli O157:H7 is an emergent pathogen causing the haemolytic – uremic syndrome, and is considered as an important foodborne source of intestinal infection causing more than 73,000 diarrhoeal episodes in the United States every year [15, 37]. We found one E. coli O157:H7 in the control group, however, no symptoms of diarrhoea were reported by the time this study was conducted. There is no explanation for this, but it might be possible that the infection was in an early stage when the stool sample was collected, or that the O157:H7 was a non-producing toxin strain. EIEC was the least detected in the patient group (1%) (Table 1), which is in agreement with a previous study conducted in a surrounding area of Mexico City where prevalence was 0.85% [28]. It has been estimated that EIEC in developing countries including Latin American is rare [5, 38]. The prevalence rate for Shigella sonnei (1.6%) and Shigella flexneri (1%) in the current study was very low (Table 1) when compared other studies [13, 21]. However, in other parts of the world, several Shigella outbreaks have been described, and the main feature is their ability to spread in the population, due to its very low infection doses (~10 bacterial cells per host) [19, 20]; therefore, a low prevalence of cases of Shigella should not be underestimated.
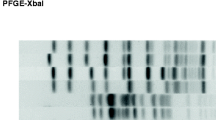
To detect Salmonella spp., two separate reactions containing primers complementary to all internal variable regions of the fliC and flj B genes, which codifies phase I and phase II flagellar antigens (Fig. 2), were used. Both multiplex PCR systems have been previously tested in hundreds of samples from different parts of the world, and were reported to be accurate, fast and reliable alternative to other traditional diagnostic methods used in the clinical laboratory [9, 10]. In our study, both stool sample groups showed S. ohio and S. typhimurium as the predominant serovars; nevertheless, many other serovars were present in both groups of samples in a considerable proportion (Table 1), which suggest that Salmonella diversity is more in comparison to E. coli, for which ETEC was considerably predominant (Table 1). Salmonellosis is one of the biggest challenges to public health all over the world. In the year 2000, a study conducted in Mexico showed S. typhimurium and S. ohio as the most and less commonly found serotypes of Salmonella respectively [39]. This may be related to the way the outbreak was studied, since we focused on most common serotypes in children (age < 12 years) and not in the whole population. This study is intended to investigate some interesting observations that deserve further studying. The results revealed that all stool samples from the patients and the majority of the control group were positive for at least one enteropathogen and that 52% of stool samples had multiple enteropathogens. All of the 300 stool samples tested except 2 had either E. histolytica/E. dispar or G. intestinalis and when an enterobacteria was present, it was most likely to be a Salmonella serotype. In addition, only 12 out of 300 stool samples tested E. coli presence was in association with a protozoa in the absence of any type of Salmonella spp. (Table 2).

(A) 2.5% Agarose gel electrophoresis of Salmonella phase I flagellar amplicons obtained from diarrhoeal samples. Lane 1: Negative control without template DNA. Lanes 2, 3, 4 10 and 12; S. ohio (150 bp) (patient group). Lanes 5, 6 and 11; negative samples (patient group). Lane 7 S. typhimurium (patient group). Lane 8; MWM 50 bp ladder. Lane 9; S. infantis (patient group); Lane 11; Negative sample (patient group); Lane 13; Salmonella anatum (patient group). (B) 2.5% agarose gel electrophoresis of Salmonella phase II flagellar amplicons obtained from diarrhoeal samples. Lanes 1, 8 and 10, negative samples (patient group); Lane 2, Negative control without template DNA; Lane 3, Salmonella anatum (patient group); Lane 4, S. typhimurium (patient group); Lane 5, MWM 50 bp ladder; Lane 6, S. infantis (patient group); Lanes 7 and 9, S. ohio (patient group). For both electrophoresis, run conditions were 120 V, 94 mA, 45 min.
It has been reported that S. typhimurium virulence is enhanced when exposed to the rumen protozoa [40]; this hypervirulent phenotype is linked to the presence of the Salmonella genomic island SGI1 integron [41]. Also, it has been shown that SGI1 is widely spread in other S. enterica serovars; and although rumen possesses different protozoa diversity than the parasites studied here, some Salmonella isolates from human infections have shown to posses such island [42]. It is tempting to speculate that a similar virulence enhancement process might occur in human digestive trait; possibly through E. histolytica/E. dispar or G. intestinalis. Whether those Salmonella strains studied in this work possesses or expresses such genomic island needs further study.
Conclusion
The study of enteropathogen associations may lead to a better understanding of the etiology of diarrhoea, and therefore in prescribing more suitable treatments in cases of outbreaks. This study revealed that 52% of the patients were infected by more than one enteropathogen, notably E. histolitica/E. dispar and Salmonella ohio. These results are useful for clinicians in improving the empiric treatment used in such cases.
References
Bern C, Martines J, de Zoysa I, Glass RI: The magnitude of the global problem of diarrhoeal disease: a ten-year update. Bull WHO. 1992, 70: 705-714.
Alper J: Date gaps need bridging to assess infectious gastrointestinal diseases. ASM News. 2003, 69: 65-68.
Secretaría de Salud , Mexico : Estadísticas de mortalidad en México: muertes registradas en el año 2003. Salud Pública Méx. 2005, 47: 171-187.
Foodborne diseases, emerging. http://www.who.int/mediacentre/factsheets/fs124/en/
Guerrant RL, Hughes JM, Lima NL, Crane J: Diarrhoea in developed and underdeveloping countries: magnitude, special settings, and etiologies. Rev Infect Dis. 1990, 12: s41-s50.
Nataro JP, Kaper JB: Diarrheagenic Escherichia coli. Clin Microbiol Rev. 1998, 11: 142-201.
Sonne-Hansen J, Jenabian SM: Molecular serotyping of Salmonella: Identification of the phase 1 H antigen based on partial sequencing of the fliC gene. APMIS. 2005, 113: 340-348. 10.1111/j.1600-0463.2005.apm_113505.x
Popoff MY, Le Minor L: Antigenic formulas of the Salmonella serovars. 2001, Institut Pasteur, Paris, France,
Echeita MA, Herrera S, Garaizar J, Usera MA: Multiplex PCR-based detection and identification of the most common Salmonella second-phase flagellar antigens. Res Microbiol. 2002, 153: 107-113. 10.1016/S0923-2508(01)01295-5
Herrera-León S, Mc Quiston JR, Usera MA, Fields PI, Garaizar J, Echeita MA: Multiplex PCR for distinguishing the most common phase-1 flagellar antigens of Salmonella spp. J Clin Microbiol. 2004, 42: 2581-2586. 10.1128/JCM.42.6.2581-2586.2004
Hale TL, Keusch GT: Shigella. Baron's Medical Microbiology. Edited by: Baron S. 1996, Texas: University of Texas Medical Branch, 4,
Haque R, Mondal D, Kirkpatrick BD, Akther S, Farr BM, Sack RB, Petri WA: Epidemiologic and clinical characteristics of acute diarrhea with emphasis on Entamoeba histolytica infections in preschool children in an urban slum of Dhaka, Bangladesh. Am J Trop Med Hyg. 2003, 69: 398-405.
Svenungsson B, Lagergren A, Ekwall E, Evengård B, Hedlund KO, Kärnell A, Löfdahl S, Svensson L, Weintraub A: Enteropathogens in adult patients with diarrhoea and healthy control subjects: a 1-year prospective study in a Swedish clinic for infectious diseases. Clin Infect Dis. 2000, 30: 770-778. 10.1086/313770
Faust EC, D'Antoni JS, Odom V, Miller MJ, Peres C, Sawitz W, Thomen LF, Tobie JE, Walker JH: A critical study of clinical laboratory techniques for the diagnosis of protozoan cysts and helminth eggs in feces. Am J Trop Med. 1938, 18: 169-183.
Rangel JM, Sparling PH, Crowe C, Griffin PM, Swerdlow DL: Epidemiology of Escherichia coli O157:H7 Outbreaks, United States, 1982–2002. Emerg Infect Dis. 2005, 11: 603-609.
Walsh JA: Problems in recognition and diagnosis of amebiasis: estimation of the global magnitude of morbidity and mortality. Rev Infect Dis. 1986, 8: 228-238.
Sánchez-Vega JT, Zavala JT, Guerrero LR, Cabello RR, Sánchez DR, García CR: Frecuencia de parasitosis intestinales en asentamientos humanos irregulares. Rev Fac Med. 2000, 3: 80-83.
Gannon VP, D'Souza S, Graham T, King RK, Rahn K, Read S: Use of the flagellar H7 gene as a target in multiplex PCR assays and improved specificity in identification of enterohemorrhagic Escherichia coli strains. J Clin Microbiol. 1997, 35: 656-662.
Kopecko DJ, Baron LS, Buysse J: Genetic determinants of virulence in Shigella and dysenteric strains of Escherichia coli: their involvement in the pathogenesis of dysentery. Curr Top Microbiol Immunol. 1985, 118: 71-95.
Makino S, Sasakawa C, Yoshikawa M: Genetic relatedness of the basic replicon of the virulence plasmid in shigellae and enteroinvasive Escherichia coli. Microb Pathog. 1988, 5: 267-274. 10.1016/0882-4010(88)90099-X
Nguyen TV, Le Van P, Le Huy Ch, Gia KN, Weintraub W: Detection and characterization of diarrheagenic Escherichia coli from young children in Hanoi, Vietnam. J Clin Microbiol. 2005, 43: 755-760. 10.1128/JCM.43.2.755-760.2005
Albert MJ, Faruque SM, Faruque AS, Neogi PK, Ansaruzzaman M, Bhuiyan NA, Alam K, Akbar MS: Controlled study of Escherichia coli diarrheal infections in Bangladeshi children. J Clin Microbiol. 1995, 33: 973-977.
González R, Díaz C, Marino M, Cloralt R, Pequeneze M, Pérez-Schael I: Age-specific prevalence of Escherichia coli with localized and aggregative adherence in Venezuelan infants with acute diarrhea. J Clin Microbiol. 1997, 35: 1103-1107.
Okeke IN, Lamikanra A, Steinruk H, Kaper JB: Characterization of Escherichia coli strains from cases of childhood diarrhea in provincial southwestern Nigeria. J Clin Microbiol. 2000, 38: 7-12.
Orlandi PP, Silva T, Magalhaes GF, Alves F, De Almeida Cunha RP, Durlacher R, da Silva LH: Enteropathogens associated with diarrheal disease in infants of poor urban areas of Porto Velho, Rondonia: a preliminary study. Mem Inst Oswaldo Cruz. 2001, 96: 621-625. 10.1590/S0074-02762001000500005
Torres ME, Pirez MC, Schelotto F, Varela G, Parodi V, Allende F, Falconi E, Dell'Acqua L, Gaione P, Mendez MV, Ferrari AM, Montano A, Zanetta E, Acuna AM, Chiparelli H, Ingold E: Etiology of children's diarrhea in Montevideo, Uruguay: associated pathogens and unusual isolates. J Clin Microbiol. 2001, 39: 2134-2139. 10.1128/JCM.39.6.2134-2139.2001
Qadri F, Das SK, Faruque AS, Fuchs GJ, Albert MJ, Sack RB, Svennerholm AM: Prevalence of toxin types and colonization factors in enterotoxigenic Escherichia coli isolated during a 2-year period from diarrheal patients in Bangladesh. J Clin Microbiol. 2000, 38: 27-31.
Cortés-Ortíz IA, Rodríguez-Angeles G, Moreno-Escobar EA, Tenorio-Lara JM, Torres-Mazadiego BP, Montiel-Vázquez E: Brote causado por Escherichia coli en Chalco México. Salud Pública Méx. 2002, 44: 297-302. 10.1590/S0036-36342002000400002.
Rodríguez-Angeles G: Principales características y diagnóstico de los grupos patógenos de Escherichia coli. Salud Pública Méx. 2002, 44: 464-475.
Wolk M, Ohad E, Shafran R, Safir S, Cohen Y, Wiklund G, Svennerholm AM: Epidemiological aspects of enterotoxigenic Escherichia coli diarrhoea in infants in the Jerusalem area. Public Health Rev. 1995, 23: 25-33.
Viboud GI, Jouve MJ, Binsztein N, Vergara M, Rivas M, Quiroga M, Svennerholm AM: Prospective cohort study of enterotoxigenic Escherichia coli infections in Argentinean children. J Clin Microbiol. 1999, 37: 2829-2833.
Cravioto A, Reyes RE, Ortega R, Fernández G, Hernández R, López D: Prospective study of diarrhoeal disease in a cohort of rural Mexican children: incidence and isolated pathogens during the first two years of life. Epidemiol Infect. 1988, 101: 123-134.
Cravioto A, Reyes RE, Trujillo F, Uribe F, Navarro A, de la Roca JM, Hernández JM, Pérez G, Vázquez V: Risk of diarrhea during the first year of life associated with initial and subsequent colonization by specific enteropathogens. Am J Epidemiol. 1990, 131: 886-904.
Gomes TA, Rassi V, MacDonald KL, Ramos SR, Trabulsi LR, Vieira MA, Guth BE, Candeias JA, Ivey C, Toledo MR, Blake PA: Enteropathogens associated with acute diarrheal disease in urban infants in Sao Paulo, Brazil. J Infect Dis. 1991, 164: 331-337.
Griffin PM, Tauxe RV: The epidemiology of infections caused by Escherichia coli 0157:H7, other enterohemorrhagic E. coli, and the associated haemolytic uremic syndrome. Epidemiol Rev. 1991, 13: 60-98.
Blanco M, Blanco JE, Blanco J, González EA, Alonso MP, Maas H, Jansen WH: Prevalence and characteristics of human and bovine verotoxigenic Escherichia coli strains isolated in Galicia (northwestern Spain). Eur J Epidemiol. 1996, 12: 13-19. 10.1007/BF00144422
Boyce TG, Swerdlow DL, Griffin PM: Escherichia coli O157:H7 and the hemolytic-uremic syndrome. N Eng J Med. 1995, 333: 364-368. 10.1056/NEJM199508103330608.
Valdespino JL, García ML, Del Río A: Epidemiología y etiología de las diarreas infecciosas. El caso de México. Rev Latinoam Microbiol. 1994, 36: 307-324.
Gutiérrez-Cogco L, Montiel-Vázquez E, Aguilera-Pérez P, González-Andrade MC: Serotipos de Salmonella identificados en los servicios de salud de México. Salud Pública Méx. 2000, 42: 490-495. 10.1590/S0036-36342000000600004.
Rasmussen MA, Carlson SA, Franklin SK, McCuddin ZP, Wu MT, Sharma VK: Exposure to rumen protozoa leads to enhancement of pathogenicity of and invasion by multiple-antibiotic-resistant Salmonella enterica bearing SGI1. Infect Immun. 2005, 73: 4668-4675. 10.1128/IAI.73.8.4668-4675.2005
Carlson SA, Sharma VK, McCuddin ZP, Rasmussen MA, Franklin SK: Involvement of a Salmonella genomic island 1 gene in the rumen protozoan-mediated enhancement of invasion for multiple-antibiotic-resistant Salmonella enterica serovar typhimurium. Infect Immun. 2007, 75: 792-800. 10.1128/IAI.00679-06
Levings RS, Lightfoot D, Partridge SR, Hall RM, Djordjevic SP: The genomic island SGI1, containing the multiple antibiotic resistance region of Salmonella enterica serovar typhimurium DT104 or variants of it, is widely distributed in other S. enterica serovars. J Bacteriol. 2005, 187: 4401-4409. 10.1128/JB.187.13.4401-4409.2005
Acknowledgements
This work was supported by DGAPA-UNAM grant PE200705. Authors acknowledge Ma. Esther Hernández Rojano for her assistance with the scholar children.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
GLP and EM carried out the molecular studies; OG, JA and EN characterized bacterial isolates, and identified the parasites; SV conceived of the study, and participated in its design and coordination, and drafted the manuscript. All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Paniagua, G.L., Monroy, E., García-González, O. et al. Two or more enteropathogens are associated with diarrhoea in Mexican children. Ann Clin Microbiol Antimicrob 6, 17 (2007). https://doi.org/10.1186/1476-0711-6-17
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-0711-6-17