
Abstract
Backround
Vaginitis is among the most common conditions women are seeking medical care for. Although these infections can easily be treated, the relapse rate is high. This may be due to inadequate use of the diagnostic potential.
Methods
We evaluated the misjudgement rate of the aetiology of vaginal complaints. A total of 220 vaginal samples from women with a vaginal complaint were obtained and analysed for numbers of total lactobacilli, H2O2-producing lactobacilli, total aerobic cell counts and total anaerobic cell counts including bifidobacteria, Bacteroides spp., Prevotella spp. Additionally, the presence of Atopobium vaginae, Gardnerella vaginalis, Candida spp. and Trichomonas vaginalis was evaluated by DNA-hybridisation using the PCR and Affirm VPIII Microbial Identification Test, respectively.
Results
The participating physicians diagnosed Bacterial vaginosis (BV) as origin of discomfort in 80 cases, candidiasis in 109 cases and mixed infections in 8 cases. However, a present BV, defined as lack of H2O2-lactobacilli, presence of marker organisms, such as G. vaginalis, Bacteroides spp. or Atopobium vaginae, and an elevated pH were identified in only 45 cases of the women examined. Candida spp. were detected in 46 cases. Interestingly, an elevated pH corresponded solely to the presence of Atopobium vaginae, which was detected in 11 cases.
Conclusion
Errors in the diagnosis of BV and candida vulvovaginitis (CV) were high. Interestingly, the cases of misjudgement of CV (77%) were more numerous than that of BV (61%). The use of Amsel criteria or microscopy did not reduce the number of misinterpretations. The study reveals that the misdiagnosis of vaginal complaints is rather high.
Similar content being viewed by others


Backround
The microbiology of the vagina is complex, containing 109 bacterial colony forming units per gram of secretions and potentially dozens of species. It is mainly dominated by members of the genus Lactobacillus, which are capable of H2O2-production and lactic acid, thereby maintaining the generally acidic vaginal pH. Age, phase of the menstrual cycle, sexual activity, contraceptive choice, pregnancy, presence of necrotic tissue or foreign bodies, and use of hygienic products or antibiotics can disrupt this ecosystem. A disturbed vaginal microbiota is characterised as vaginitis. Vaginitis, whether infectious or not, poses one of the most common problems in gynaecology, and it is one of the main reasons leading women to seek advice from a physician [1]. However, diagnosis and treatment can be elusive, if based on clinical symptoms and the characterisation of vaginal discharge alone [2, 3]. This may lead to a lack of relief from symptoms and, because of inadequate treatment, to increased costs for the patient and social securities.
Bacterial vaginosis (BV) and candida vulvovaginitis are responsible for 90% of cases of vaginitis [4]. BV is characterised by the substitution of the regular, lactobacilli dominated microbiota by a complex and abundant flora of strictly or facultatively anaerobic bacteria (Gardnerella vaginalis, Bacteroides spp., Prevotella spp., Peptostreptococcus spp., and Mycoplasma hominis) [5–8]. Recent studies suggested a correlation between the metronidazole-resistant anaerobe Atopobium vaginae and BV [9–12].
Many cases of BV are asymptomatic or present with only malodorous vaginal discharge and no inflammatory complaints. In contrast, CV often correlates with scant discharge and marked inflammatory symptoms (pruritus and soreness) [13] and is characterised by an excessive proliferation of Candida spp. in the vaginal flora [14].
Due to the fact that clinical symptoms associated with vaginitis are various, the clinical diagnosis is often deceptive. As defined by Amsel and colleagues [15] a correct diagnosis of BV should comprise at least three of the following criteria: a thin homogeneous white discharge, the presence of "clue cells" on microscopic exam, a pH > 4.5 of vaginal fluid and fishy odour before or after adding 10% KOH (whiff test). Gram-staining of vaginal secretion is also an accepted additional diagnostic test of BV [16–19]. A current CV should be diagnosed by performing saline microscopy in order to look for candidal buds or hyphae. Additionally, the diagnostic panel can comprise culturing, PCR or antibody detection [20–22].
The purpose of this study was to evaluate, whether practitioners truly rely on the recommended criteria for diagnosis of BV [15, 18] and if so, whether the use of these criteria leads to a correct diagnosis according to our definition of BV. In addition, we evaluated the accuracy for the diagnosis of CV. In order to do so, we used a combination of culturing methods, DNA hybridisation and PCR for the differentiation of the various vaginal infectious types.
Methods
Participants and subjects
220 women diagnosed with relapsing vaginitis by the same physician within a period of three months were included in the study. "Relapsing" was defined as seeking medical help for identical symptoms. The age of the participants ranged from 17 to 65 years. Twelve participants were postmenopausal women. Vaginal samples were sent in by 53 general practitioners and 31 gynaecologists.
Collection of samples for analysis
All participating physicians used the same test system (VaginalStatus, IFM, Herborn, Germany), which contained two swabs. Using these swabs two vaginal samples were taken from each individual. One swab (pre-weighed) was placed into Portagerm-Amies-Agar transport tubes (bioMérieux) and was used for the culturing of aerobic and anaerobic bacteria. The second swab (Affirm hardwood swab; Becton Dickinson, Heidelberg, Germany) was used for DNA hybridisation and PCR analysis. It was placed into an inactivation medium provided by the supplier (Affirm VPIII; Becton Dickinson and Company, Spaks, USA, [23]). The VaginalStatus-test system was sent to the laboratory for further analysis. In addition, the vaginal pH was determined by litmus paper and documented by the physician.
Transport of samples
The performance of the Affirm VPIII following transport was evaluated elsewhere [24]. To ensure that the transport did not have any effect on the cultured species, a storage study was performed with vaginal samples from 10 healthy women and 10 women diagnosed with BV. Two vaginal samples were taken from each individual and both were placed in Portagerm-Amies-Agar transport tubes. The first swab was immediately removed from the transport medium and put in 1 ml of phosphate-buffered saline (PBS, pH 7.2)
The solution was vortexed for 5 s and serially diluted (neat to 10-5) in PBS, pH 7.2. One ml of each dilution was plated onto enrichment or selective agar media [Columbia blood agar for aerobic bacteria, Schaedler agar for anaerobic bacteria, DIC agar for Bifidobacterium spp., CPS agar for Enterobacteriaceae and Rogosa agar for Lactobacillus spp. (bioMérieux, Nuertingen, Germany)]. The second swab was stored in the transport medium for three days at 25°C, which represents the average temperature during shipment. Following the incubation period, the second swab was processed as described for the first and the results were compared. No significant differences in the cell counts of the investigated genera could be detected. Thus, it was concluded that a shipment of less than three days did not affect the composition of the studied microbiota. Therefore, only samples that took less than 3 days to arrive at the laboratory were included in the study.
Identification and enumeration of microorganisms
Vaginal samples were plated on selective agar (see above) and subsequently incubated under aerobic or anoxic conditions at 37°C for two days. The bacteria were submitted to Gram staining and the colony morphologies recorded. Additionally, identifications were performed by the API®- and VITEK®-systems (bioMérieux). All counts were listed as the numbers of log10 colony forming units (CFU) per ml of sample.
Detection of H2O2-production
Following identification, lactobacilli were tested for hydrogen peroxide production as described previously [25]. Colonies that produced H2O2 on the agar appeared dark blue. Colonies, which did not produce H2O2, were colourless.
DNA-hybridisation
Hybridisation was performed as described by the manufacturer (Affirm VPIII; Becton Dickinson and Company, Sparks, USA). The test system is based on two specific single-stranded nucleic acid probes for each organism as well as on capture probes and colour development probes that are complementary to unique genetic sequences of Gardnerella vaginalis, Candida spp. and Trichomonas vaginalis.
Detection of Atopobium vaginae
For the detection of Atopobium vaginae the PCR-method described by Ferris et al. was used [26].
Evaluation criteria
Within the presented study the following criteria were analysed: Total aerobic and anaerobic cell counts, numbers of H2O2-producing lactobacilli, bifidobacteria, Bacteroides spp., Prevotella spp., Streptococcus agalactiae and Staphylococcus spp. In addition, Gardnerella vaginalis, Candida spp. or Trichomonas vaginalis were detected by DNA-hybridisation (Affirm VPIII) and Atopobium vaginae by PCR, respectively. Bacterial vaginosis (BV) was defined as manifested, if the following three criteria were fulfilled: elevated pH, decrease of H2O2-producing lactobacilli, presence of either G. vaginalis, A. vaginae or any other anaerobic organism. A positive DNA hybridisation was used as the gold standard for diagnosis of candida vulvovaginitis (CV). All participating physicians completed a questionnaire, whereby the presence of the following symptoms was recorded: itching, burning, odour, redness and discharge. Furthermore, the use of Amsel-criteria, Nugent-score [15, 18], microscopy for the identification of fungi and suspected causative of infection were inquired.
Statistical analysis
All data were compiled and analysed using SPSS (SPSS Inc., Chicago, IL.). P values for the difference in speeds of various methods were calculated using Wilcoxon's nonparametric test. The chi-square procedure was used to compare the isolation frequency of bacterial groups between categories of different vaginal pH. Diagnostic accuracy was measured by computing point estimates of the following test properties for each response, using standard methods: sensitivity, specificity, positive and negative predictive values, positive (LR+) and negative likelihood ratios (LR-). The precision of these estimates was evaluated using 95% confidence intervals. We used the kappa (κ) statistic to evaluate chance-corrected agreement between the diagnosis by physicians and our microbiologically based diagnosis. A kappa value of 0 indicates that the observed agreement is the same as that expected by chance. A kappa value of 1 indicates perfect agreement. The following guides were used for interpreting the kappa statistic: a kappa value of < 0.2 indicates poor agreement, 0.21–0.6 fair to moderate agreement, 0.61–0.8 good agreement and 0.81–1.0 very good agreement [27].
Results
Of the 220 vaginal samples obtained only 197 were included into the study, as 23 samples did not fulfil all evaluation criteria. No pH was recorded in 12 samples, no admission diagnosis was given in 10 samples, and one sample contained only the swab for DNA-hybridisation.
A comparison of frequencies of detection and mean counts of the major genera comprising the vaginal microbiota in relation to the recorded vaginal pH is shown in Table 1. No significant differences in the frequency of isolation of the various lactobacilli types (H2O2-producers and non-producers) could be observed between women with a normal pH and women with an elevated pH, respectively. However, cell counts were decreased by one order of magnitude between the two groups. A lower cell count was recorded for the group with an elevated pH. Interestingly, high rates of H2O2-producing lactobacilli (> 108CFU/ml) were significantly (P < 0.05) more often reduced in women who were recorded with an elevated vaginal pH. In several samples positive for H2O2-producing lactobacilli, colonies which appeared light blue were seen, but their amount was always less than the number of dark blue colonies.
In 45 cases an elevated pH was accompanied by a decrease in the frequency of H2O2-lactobacilli as well as by the presence of anaerobes, and was accordingly classified as bacterial vaginitis (BV). Candida spp. were detected in 46 cases and mixed infections in one case, whereas in 105 cases no sign of an infectious vaginitis could be identified. The mean counts of total aerobes, anaerobes, Staphylococcus agalactiae, Streptococcus spp., Bacteroides spp., and bifidobacteria were similar in women with a normal pH and women with an elevated pH. However, the amount of Bacteroides spp. was elevated by one order of magnitude in women with an elevated pH. No other anaerobic bacteria were identified. Furthermore, no significant differences in the presence of Gardnerella vaginalis, Candida spp. and Trichomonas vaginalis were detected. However, there was a significant correlation between Atopobium vaginae and an elevated pH. Interestingly, A. vaginae was always detected in combination with G. vaginalis. Within the study group no correlations between pre- and post-menopausal women, vaginal complaints and the microbiota could be drawn.
The results of the 197 questionnaires are summarised in Tables 2 and 3. Itching and burning were the most common symptoms reported, followed by discharge, redness, and odour (Table 2). None of the reported symptoms could be associated with the presence of a specific organism (P > 0.05; data not shown). The diagnosis of the participating physicians was BV in 80 cases, candida vulvovaginitis (CV) in 109 cases, and mixed infection in 8 cases (Table 3). Amsel-criteria were used in 54 out of 80 cases for the diagnosis of BV, microscopy in 60 out of 109 cases for the diagnosis of candida vulvovaginitis, and both were used in four out of eight cases for mixed infections (Table 3). Both, Amsel criteria and microscopy, were predominantly but not exclusively used by gynaecologists (data not shown). Not a single physician based his diagnosis on Nugent-score [18].
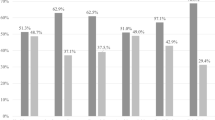
The diagnosis of BV by physicians agreed only fairly with our diagnosis (κ = 0.29; 95% CI 0.16, 0.42). There was an even poorer agreement for the diagnosis of candidiasis (κ = -0.01; 95% CI -0.12, 0.10). Regardless of the implementation of the various recommended criteria for evaluation of vaginitis [21, 28], the error of judgement for BV, CV or a mixed infection was high (Table 3). The level of misdiagnosis exceeded 70%. The misjudgement of a mixed infection was highest (87%), followed by CV (77%) and a manifested BV (>61%). The use of the Amsel criteria for the detection of BV or microscopy for the detection of Candida spp. did not enhance the diagnostic correctness (Table 3). Compared to the detection of a pathological vaginal colonisation as reference standard, which was based on our microbial verification of the pathologic agent or altered vaginal microbiota, the diagnostic classification by physicians was of relatively minor accuracy. Sensitivity and specificity (95% confidence interval), respectively, were 68.9% (55–82) and 67.8% (60–75) for the diagnosis BV, whereas only 54.3% (40–69) and 44.4% (36–52) for the diagnosis of a CV. Positive and negative predictive values as well as likelihood ratios (LR) of a positive and negative result were 38.8% (28–50), 88% (80–93), 2.1 (1.6–2.9) and 0.46 (0.29–0.71), respectively, for the diagnosis BV. The corresponding values for the diagnosis of a CV were 22.9% (15–31), 76.1 (65–84), 0.97 (0.72–1.31) and 1.03 (0.72–1.47), respectively. From these values the diagnostic odds ratios were calculated for the diagnosis of BV and Candidiasis with values of 4.66 (95% CI: 0.51, 2.16) and 0.95 (95% CI: 0.49, 1.84), respectively, indicating again that the diagnosis of a CV by physicians does not discriminate between diseased and not diseased.
Discussion
Studies showed that bacterial vaginosis (BV) resulted from an imbalance of the normal vaginal flora, with an overgrowth of gram-negative anaerobes and a reduction in lactobacilli, especially those that produced H2O2 [29–32]. Candida vulvovaginitis (CV) was primarily associated with Candida albicans, but other species are emerging [33, 34]. The standard diagnosis for BV should enclose the Amsel-criteria [28]. For the identification of fungal infections, culturing or microscopy was recommended [21].
However, error in diagnosis was rather high within the group of surveyed physicians, no matter whether they used the recommended techniques or not. The establishment of a wrong diagnosis was highest for mixed infections followed by CV and BV. This fact may be explained by an inadequate use of microscopy, as microscopy is the key technique in recognition of a vaginal infection. Microscopy without specific staining generally leaves room for interpretation. In example, none of the participating physicians detected A. vaginae under the microscope or interpreted the presence of small elliptical cocci as conspicuous. When asked in retrospect, none of the participating physicians was aware of the existence of this species. Taken into account that A. vaginae is resistant to metronidazol, a common antibiotic given for the treatment of BV, a proof of absence of this organism should be mandatory at least in women with recurring vaginal complaints.
According to its frequent citing in scientific publications the Nugent-score is well established for the diagnosis of BV [7, 17, 35, 36]. However, the herein presented results suggest that it is not commonly used on a day to day basis within the practicing community of physicians.
In recent years, the capability of lactobacilli to protect against vaginal infections by altering vaginal pH through the production of metabolic end-products including lactic acid, and by their ability to produce hydrogen peroxide (H2O2) has been widely recognised [31, 32, 40–42]. If those lactobacilli, which predominantly produce H2O2 are missing or underrepresented, serious problems including BV [42, 43], recurrent urinary tract infections [32] or even an increased risk of pre-term delivery are likely to occur [30, 44]. Interestingly, in over 50% of cases within our study, no association of complaints with BV or candida vulvovaginitis could be drawn. However, within this group of patients, low cell counts of H2O2-producing lactobacilli were observed. Lactobacilli, especially those capable of H2O2-production, are responsible for the maintenance of the normal vaginal ecosystem [29, 31, 45]. Therefore, in cases where lactobacilli cell counts are low it may be favourable to supplement the vaginal flora with lactobacilli to help restore the usual conditions.
Concerning the cases of misdiagnosed fungal infections, which occurred more frequently than cases of misdiagnosed BV, our results are in accordance with the literature [2, 22]. Because microscopic evaluation requires special diagnostic skills not available to all practitioners, misjudgement is common, therapy is frequently empirical and the relapse rate is high [20]. In our study, the recognition or the exclusion of the diagnosis candidiasis by surveyed physicians was nearly as likely in patients with the disease as in patients without the disease. Physicians diagnosed 54.3% of all candida infections correctly, but had a false positive CV diagnosis for 55.6% of all not infected cases. This is also demonstrated by the LR values close to 1, with which tests cannot help a clinician to rule in or rule out the target disease. Therefore, the diagnosis of a CV by physicians was not better than those expected by chance as judged by the positive and negative likelihood ratios. In one recent study, the sensitivity of microscopy for diagnosis of candida vulvovaginitis was only 22% [46]. Therefore, a more reliable test system, like the herein implemented hybridisation system (Affirm VPIII), which detects several Candida spp. (C. albicans, C. glabrata, C. kefyr, C. krusei, C. parapsilosis and C. tropicalis) is necessary.
Our results are in accordance with a recent study, which concluded that the clinical diagnosis of vaginal infections (history and physical examination, vaginal pH, wet mount microscopy, whiff test) is inadequate and should be confirmed by microbiological testing [47]. This was also reported by Anderson et al., who evaluated the role of clinical examinations in published articles from 1966 to 2003 [48]. The poor performance of individual symptoms and signs left one third of women with vaginal complaints without an adequate diagnosis. In general, laboratory tests should be more emphasized in the diagnosis of vaginal complaints.
Conclusion
It becomes evident from this study that the misjudgement of vaginal complaints is rather high and that the so called "gold-standards" for the diagnosis of vaginal infections are not widely and/or correctly used. Ultimately, a correct diagnosis is not yielded; it is rather throwing a dice for the diagnosis.
References
Kent HL: Epidemiology of vaginitis. Am J Obstet Gynecol. 1991, 165: 1168-1176.
Schaaf VM, Perez-Stable EJ, Borchardt K: The limited value of symptoms and signs in the diagnosis of vaginal infections. Arch Intern Med. 1990, 150: 1929-1933. 10.1001/archinte.150.9.1929
Bornstein J, Lakovsky Y, Lavi I, Bar-Am A, Abramovici H: The classic approach to diagnosis of vulvovaginitis: a critical analysis. Infect Dis Obstet Gynecol. 2001, 9: 105-111.
Fleury FJ: Adult vaginitis. Clin Obstet Gynecol. 1981, 24: 407-438.
Larsson PG, Forsum U: Bacterial vaginosis--a disturbed bacterial flora and treatment enigma. APMIS. 2005, 113: 305-316. 10.1111/j.1600-0463.2005.apm_113501.x
Boggess KA, Trevett TN, Madianos PN, Rabe L, Hillier SL, Beck J, Offenbacher S: Use of DNA hybridization to detect vaginal pathogens associated with bacterial vaginosis among asymptomatic pregnant women. Am J Obstet Gynecol. 2005, 193: 752-756. 10.1016/j.ajog.2005.01.068
Sha BE, Chen HY, Wang QJ, Zariffard MR, Cohen MH, Spear GT: Utility of Amsel criteria, Nugent score, and quantitative PCR for Gardnerella vaginalis, Mycoplasma hominis, and Lactobacillus spp. for diagnosis of bacterial vaginosis in human immunodeficiency virus-infected women. J Clin Microbiol. 2005, 43: 4607-4612. 10.1128/JCM.43.9.4607-4612.2005
Fredricks DN, Fiedler TL, Marrazzo JM: Molecular identification of bacteria associated with bacterial vaginosis. N Engl J Med. 2005, 353: 1899-1911. 10.1056/NEJMoa043802
Ferris MJ, Masztal A, Aldridge KE, Fortenberry JD, Fidel PLJ, Martin DH: Association of Atopobium vaginae, a recently described metronidazole resistant anaerobe, with bacterial vaginosis. BMC Infect Dis. 2004, 4: 5- 10.1186/1471-2334-4-5
Verstraelen H, Verhelst R, Claeys G, Temmerman M, Vaneechoutte M: Culture-independent analysis of vaginal microflora: the unrecognized association of Atopobium vaginae with bacterial vaginosis. Am J Obstet Gynecol. 2004, 191: 1130-1132. 10.1016/j.ajog.2004.04.013
Verhelst R, Verstraelen H, Claeys G, Verschraegen G, Delanghe J, Van Simaey L, De Ganck C, Temmerman M, Vaneechoutte M: Cloning of 16S rRNA genes amplified from normal and disturbed vaginal microflora suggests a strong association between Atopobium vaginae, Gardnerella vaginalis and bacterial vaginosis. BMC Microbiol. 2004, 4: 16- 10.1186/1471-2180-4-16
Burton JP, Devillard E, Cadieux PA, Hammond JA, Reid G: Detection of Atopobium vaginae in postmenopausal women by cultivation-independent methods warrants further investigation. J Clin Microbiol. 2004, 42: 1829-1831. 10.1128/JCM.42.4.1829-1831.2004
Sobel JD: Treatment of vaginal Candida infections. Expert Opin Pharmacother. 2002, 3: 1059-1065. 10.1517/14656566.3.8.1059
Ferrer J: Vaginal candidosis: epidemiological and etiological factors. Int J Gynaecol Obstet. 2000, 71 Suppl 1: S21-S27. 10.1016/S0020-7292(00)00350-7
Amsel R, Totten PA, Spiegel CA, Chen KC, Eschenbach D, Holmes KK: Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. Am J Med. 1983, 74: 14-22. 10.1016/0002-9343(83)91112-9
Schwebke JR, Hillier SL, Sobel JD, McGregor JA, Sweet RL: Validity of the vaginal gram stain for the diagnosis of bacterial vaginosis. Obstet Gynecol. 1996, 88: 573-576. 10.1016/0029-7844(96)00233-5
Delaney ML, Onderdonk AB: Nugent score related to vaginal culture in pregnant women. Obstet Gynecol. 2001, 98: 79-84. 10.1016/S0029-7844(01)01402-8
Nugent RP, Krohn MA, Hillier SL: Reliability of diagnosing bacterial vaginosis is improved by a standardized method of gram stain interpretation. J Clin Microbiol. 1991, 29: 297-301.
Witt A, Petricevic L, Kaufmann U, Gregor H, Kiss H: DNA hybridization test: rapid diagnostic tool for excluding bacterial vaginosis in pregnant women with symptoms suggestive of infection. J Clin Microbiol. 2002, 40: 3057-3059. 10.1128/JCM.40.8.3057-3059.2002
Mardh PA, Novikova N, Witkin SS, Korneeva I, Rodriques AR: Detection of candida by polymerase chain reaction vs microscopy and culture in women diagnosed as recurrent vulvovaginal cases. Int J STD AIDS. 2003, 14: 753-756. 10.1258/09564620360719796
Evans EG: Diagnostic laboratory techniques in vaginal candidosis. Br J Clin Pract Suppl. 1990, 71: 70-72.
Weissenbacher S, Witkin SS, Tolbert V, Giraldo P, Linhares I, Haas A, Weissenbacher ER, Ledger WJ: Value of Candida polymerase chain reaction and vaginal cytokine analysis for the differential diagnosis of women with recurrent vulvovaginitis. Infect Dis Obstet Gynecol. 2000, 8: 244-247. 10.1002/1098-0997(2000)8:5<244::AID-IDOG1027>3.0.CO;2-Q
Brown HL, Fuller DD, Jasper LT, Davis TE, Wright JD: Clinical evaluation of affirm VPIII in the detection and identification of Trichomonas vaginalis, Gardnerella vaginalis, and Candida species in vaginitis/vaginosis. Infect Dis Obstet Gynecol. 2004, 12: 17-21. 10.1080/1064744042000210375
Brown HL, Fuller DA, Davis TE, Schwebke JR, Hillier SL: Evaluation of the Affirm Ambient Temperature Transport System for the detection and identification of Trichomonas vaginalis, Gardnerella vaginalis, and Candida species from vaginal fluid specimens. J Clin Microbiol. 2001, 39: 3197-3199. 10.1128/JCM.39.9.3197-3199.2001
Eschenbach DA, Davick PR, Williams BL, Klebanoff SJ, Young-Smith K, Critchlow CM, Holmes KK: Prevalence of hydrogen peroxide-producing Lactobacillus species in normal women and women with bacterial vaginosis. J Clin Microbiol. 1989, 27: 251-256.
Ferris MJ, Masztal A, Martin DH: Use of species-directed 16S rRNA gene PCR primers for detection of Atopobium vaginae in patients with bacterial vaginosis. J Clin Microbiol. 2004, 42: 5892-5894. 10.1128/JCM.42.12.5892-5894.2004
Altman DG: Practical statistics for medical research. 1991, London, Chapman & Hall, 1991.
Amsel R, Hawes SE, Hillier SL: Nonspecific vaginitis. Diagnostic criteria and microbial and epidemiologic associations. J Infect Dis. 1999, 180: 1950-1956. 10.1086/315109
Beigi RH, Wiesenfeld HC, Hillier SL, Straw T, Krohn MA: Factors associated with absence of H2O2-producing Lactobacillus among women with bacterial vaginosis. J Infect Dis. 2005, 191: 924-929. 10.1086/428288
Agrawal BM, Agrawal S, Rizvi G, Ansari KH: Role of non-H2O2 producing lactobacilli and anaerobes in normal and complicated pregnancy. J Indian Med Assoc. 2002, 100: 652-655.
Felten A, Barreau C, Bizet C, Lagrange PH, Philippon A: Lactobacillus species identification, H2O2 production, and antibiotic resistance and correlation with human clinical status. J Clin Microbiol. 1999, 37: 729-733.
Gupta K, Stapleton AE, Hooton TM, Roberts PL, Fennell CL, Stamm WE: Inverse association of H2O2-producing lactobacilli and vaginal Escherichia coli colonization in women with recurrent urinary tract infections. J Infect Dis. 1998, 178: 446-450.
Loh KY, Sivalingam N: Recurrent vaginal candidiasis. Med J Malaysia. 2003, 58: 788-792.
Holland J, Young ML, Lee O, Chen A: Vulvovaginal carriage of yeasts other than Candida albicans. Sex Transm Infect. 2003, 79: 249-250. 10.1136/sti.79.3.249
Burton JP, Reid G: Evaluation of the bacterial vaginal flora of 20 postmenopausal women by direct (Nugent score) and molecular (polymerase chain reaction and denaturing gradient gel electrophoresis) techniques. J Infect Dis. 2002, 186: 1770-1780. 10.1086/345761
Culhane JF, Desanto D, Goldenberg RL, McCollum KF, King F, Guaschino S: Variation in Nugent score and leukocyte count in fluid collected from different vaginal sites. Obstet Gynecol. 2005, 105: 120-123.
Barbes C, Boris S: Potential role of lactobacilli as prophylactic agents against genital pathogens. AIDS Patient Care STDS. 1999, 13: 747-751.
Redondo-Lopez V, Cook RL, Sobel JD: Emerging role of lactobacilli in the control and maintenance of the vaginal bacterial microflora. Rev Infect Dis. 1990, 12: 856-872.
Hillier SL, Krohn MA, Rabe LK, Klebanoff SJ, Eschenbach DA: The normal vaginal flora, H2O2-producing lactobacilli, and bacterial vaginosis in pregnant women. Clin Infect Dis. 1993, 16 Suppl 4: S273-S281.
Hillier SL, Krohn MA, Klebanoff SJ, Eschenbach DA: The relationship of hydrogen peroxide-producing lactobacilli to bacterial vaginosis and genital microflora in pregnant women. Obstet Gynecol. 1992, 79: 369-373.
Onderdonk AB, Lee ML, Lieberman E, Delaney ML, Tuomala RE: Quantitative microbiologic models for preterm delivery. J Clin Microbiol. 2003, 41: 1073-1079. 10.1128/JCM.41.3.1073-1079.2003
Al Mushrif S, Jones BM: A study of the prevalence of hydrogen peroxide generating Lactobacilli in bacterial vaginosis: the determination of H2O2 concentrations generated, in vitro , by isolated strains and the levels found in vaginal secretions of women with and without infection. J Obstet Gynaecol. 1998, 18: 63-67.
Landers DV, Wiesenfeld HC, Heine RP, Krohn MA, Hillier SL: Predictive value of the clinical diagnosis of lower genital tract infection in women. Am J Obstet Gynecol. 2004, 190: 1004-1010. 10.1016/j.ajog.2004.02.015
Karaca M, Bayram A, Kocoglu ME, Gocmen A, Eksi F: Comparison of clinical diagnosis and microbiological test results in vaginal infections. Clin Exp Obstet Gynecol. 2005, 32: 172-174.
Anderson MR, Klink K, Cohrssen A: Evaluation of vaginal complaints. Jama. 2004, 291: 1368-1379. 10.1001/jama.291.11.1368
Acknowledgements
We thank Lilian Schoefer and Dorothee Moseley for assistance in preparing the manuscript.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
Herewith, the authors declare that they obtain, except for DT, funding by the Institute for Microecology.
Authors' contributions
AS, KR and VR planned and carried out the design of the study. AS and KR participated in laboratory studies and interpretation of the data. AS wrote the first draft of the manuscript. DT carried out the statistics. All authors had intellectual contribution, and all read and approved of the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Schwiertz, A., Taras, D., Rusch, K. et al. Throwing the dice for the diagnosis of vaginal complaints?. Ann Clin Microbiol Antimicrob 5, 4 (2006). https://doi.org/10.1186/1476-0711-5-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-0711-5-4