
Abstract
Background
The Yusho poisoning incident, which was caused by rice bran oil contaminated with polychlorinated biphenyls (PCBs), polychlorinated quarterphenyls (PCQs) and polychlorinated dibenzofurans (PCDFs) generated by heat denaturation of PCB, occurred in 1968 in western Japan. Annual physical, dermatological, dental, ophthalmological and laboratory examinations were conducted for Yusho patients after the incident. From 2001, blood levels of individual PCDF congeners were also measured. The blood levels of 2,3,4,7,8-pentachlorodibenzofuran (2,3,4,7,8-PeCDF), PCBs and PCQs in Yusho patients were found to be significantly higher than those of the general population. We investigated the relationships between blood concentrations of 2,3,4,7,8-PeCDF, PCBs and PCQs in Yusho patients and the items measured in the annual medical examination.
Methods
Medical and laboratory examination data from 501 Yusho patients enrolled in the study from 2001 to 2004 were analyzed. The relationships between blood 2,3,4,7,8-PeCDF, PCB and PCQ concentrations and medical/laboratory examination data were investigated using principal components and logistic regression analyses.
Results
Serum Concentrations of 2,3,4,7,8-PeCDF, PCBs and PCQs in blood tended to correlate with either acneform eruptions, black comedones, cutaneous and mucosal pigmentation, and hypersecretion of meibomian glands as well as general fatigue, headaches, cough/sputum, abdominal pain, arthralgia, increased blood sugar, increased serum γ-GTP and decreased total bilirubin. The majority of these signs and symptoms are included in the diagnostic criteria for Yusho.
Conclusion
After Yusho patients had suffered chronic exposure to these chlorinated compounds for more than 35 years, the serum concentration of 2,3,4,7,8-PeCDF in blood was significantly related to arthralgia and decreased albumin/globulin (A/G) ratio; the serum concentration of PCBs was significantly related to ophthalmologic symptoms; and the serum concentration of PCQ to increased total cholesterol. These findings suggest that the co-contaminants may affect other functions than those originally associated with Yusho.
Similar content being viewed by others


Background
Yusho was a food poisoning incident that occurred in western Japan in 1968 [1–8]. When first reported, the food poisoning incident known as Yusho was considered to be caused by polychlorinated biphenyls (PCBs). However, following a number of studies, it is now considered to be caused by complex poisoning with polychlorinated quarterphenyls (PCQs) and polychlorinated dibenzofurans (PCDFs) [3–6]. Thirty-seven years have passed since the Yusho incident occurred, and more than 1,800 patients are known to have been affected.
Yusho patients are known to present with various symptoms related to the skin, eyes and teeth, and have abnormal findings on physical examinations [8–14]. The severity of symptoms in Yusho patients has gradually improved over the past 37 years. However, a number of patients still suffer from specific Yusho symptoms [3, 4, 8]. The initial diagnostic criteria published in 1968 were mainly: 1) proven history of ingestion of contaminated rice bran oil; 2) prominent dermatological, ophthalmological and mucosal signs; and 3) several nonspecific general signs and symptoms. Hyperglyceridemia, pulmonary disorders, intractable headache, elevated blood PCB concentrations and specific PCB patterns on gas chromatography were added to the initial diagnostic criteria in 1972 and 1976. Blood PCQ concentrations were added to the criteria in 1981 [3].
With recent advances in techniques for measuring individual PCDF congeners, it has become possible to precisely measure 2,3,4,7,8-pentachlorodibenzofuran (2,3,4,7,8-PeCDF) blood concentrations using as little as 5 ml of blood [17, 18]. Thus, measurements of 2,3,4,7,8-PeCDF blood concentrations have been initiated since 2001 in the routine mass screening of Yusho patients. The mean blood concentrations of PeCDF in these patients have been shown to be more than 10 times higher than those in normal controls [3]. In 2004, the blood 2,3,4,7,8-PeCDF concentration was added to the present diagnostic criteria (Table 1).
In this study, we analyzed the results of medical examinations of Yusho patients whose blood 2,3,4,7,8-PeCDF concentrations were measured from 2001 to 2004 (33 to 37 years after the occurrence of the Yusho disaster), and investigated the relationships among the 2,3,4,7,8-PeCDF, PCB and PCQ blood concentrations and the clinical data from physical and laboratory examinations.
Methods
Subjects and medical check items
Since immediately after the incident occurred, the Yusho Study Group has conducted annual health checks of Yusho patients. Between 2001 and 2004, a total of 501 individuals (81 individuals in 2001, 371 in 2002, 343 in 2003 and 292 in 2004, including multiple health checks) underwent the Yusho mass screening. In addition to blood PeCDFs, PCBs and PCQs serum concentrations, 241 check items (52 items in a questionnaire, 55 physical and laboratory examinations, 21 dermatological examinations, 108 dental examinations, and 5 ophthalmological examinations) were carried out (Table 2).
Statistical analysis
The relationships between blood 2,3,4,7,8-PeCDF concentrations(serum) and the physical/laboratory test items were analyzed using logistic regression analysis. Since the serum half-life of 2,3,4,7,8-PeCDF is long and the present blood concentrations are well correlated with the amount of exposure at the time of the incident, the correlations with these was examined [19]. Logistic regression analysis uses a formula to relate several explanatory variables to objective ones (2 values). We used the following equation which included results [y] and several factors [x 1, x 2, ..., x n] affecting these results with β i as coefficients
g(x) = β 0+β 1 x 1+β 2 x 2+ ...+β n x n
y = e g(x)/(e g(x)+1)
To conduct a logistic regression analysis, we conducted a principal component analysis as an auxiliary analysis to decide the explanatory variables. Specifically, of the 241 items examined in the Yusho medical checkup, the principal component analysis was conducted on 172 items, except for those related to frequency. As a result, examination items with 1 or higher eigenvalues and high factor scores in the principal component analysis were used as representative variables. In deciding the representative variables, items with high factor scores were not selected mechanically, but the following criteria were considered:
(1) Items included in the criteria.
(2) Items considered to be medically significant.
(3) A weak factor representing an item selected by multiple factors.
Furthermore, we confirmed that items whose associations with Yusho have been indicated were not overlooked, by reference to the criteria. We extracted 49 items, including 13 questionnaire-related items, 11 physical and laboratory examination items, 10 dermatological examination items, 12 dental examination items and 3 ophthalmological examination items, as representative variables. (Table 3)
Furthermore, the following patterns were set as objective variables for our logistic regression analyses:
2,3,4,7,8-PeCDF blood concentration(serum)
2 categories: [≥ 50 pg/g lipids] and [< 50 pg/g lipids] (as indicated by the diagnostic criteria [3])
PCB blood concentration(serum)
2 categories: [≥ 2.0 ppb] and [< 2.0 ppb] (Categorized by median value)
PCQ blood concentration(serum)
2 categories: [≥ 0.10 ppb] and [< 0.10 ppb] (as indicated by the diagnostic criteria [3])
Other examination items
The 49 factors extracted by the principal component analysis were classified into normal and abnormal categories considering the characteristics of the data for each test item, from the following viewpoints:
(1) Factors for which the presence or absence of symptoms was confirmed by two steps in the medical checkup by a doctor were classified into two steps of presence or absence.
(2) Factors whose measurement results had normal value standards, such as blood test results, were classified into normal or abnormal.
(3) Items relevant to subjective symptoms, like sputum, arthralgia and general fatigue, were classified into "normal" or "abnormal" for each patient.
(4) Items evaluated into five grades (-, ±, +, ++ and +++) of symptoms, such as severity of pigmentation, were classified into two groups, based on the criterion of "+" or above, to determine the presence of symptoms.
To conduct analyses on the above 3 patterns, 2,3,4,7,8-PeCDF, PCB and PCQ blood concentrations were added to the explanatory variables. SPSS11.5J for Windows was used for the analyses.
Results
2,3,4,7,8-PeCDF blood concentration as an objective variable, PCB and PCQ blood concentrations, blood glucose level, arthralgia, gender, total bilirubin, black comedones, acneform eruption, past history of skin pigmentation and acneform eruption, increased A/G ratio, abnormal respiratory sounds, blood potassium level, and total cholesterol showed less than a 0.05 level of significance. Most of these items are considered characteristic symptoms of Yusho. Even when PCB and PCQ blood concentrations are excluded from the explanatory variables, older age, A/G ratio, general fatigue, arthralgia, gender and oral pigmentation showed less than a 0.05 level of significance.
In contrast, when 49 factors were extracted by the principal component analysis (PCB and PCQ as objective variables, 2,3,4,7,8-PeCDF blood concentration as an explanatory variable), PCQ and PCB blood concentrations, arthralgia, presence or absence of previous history since 1968, A/G ratio and blood glucose level indicated a significance probability of ≤ 0.05 for the 2,3,4,7,8-PeCDF blood concentration. (Table 4)
PCB blood level as an objective variable, 2,3,4,7,8-PeCDF blood concentration, sputum, age, female gender, past history of pigmentation and acneform eruption, toe nail pigmentation, hepatomegaly, headache, cheesy secretion from meibomian glands, total bilirubin, and general fatigue showed less than a 0.05 level of significance. When 2,3,4,7,8-PeCDF blood concentration was excluded from the explanatory variables, age, sputum, past history of pigmentation, total bilirubin, PCQ blood concentration, toe nail pigmentation, arthralgia, presence of a chief dental complaint, headache, and cheesy secretion from meibomian glands were significantly correlated with PCB blood concentrations.
In contrast, when 49 factors were extracted by the principal component analysis (2,3,4,7,8-PeCDF and PCQ as objective variables, PCB blood concentration as an explanatory variable), items which showed less than a 0.05 level of significance for PCB blood concentration (explanatory variable) included 2,3,4,7,8-PeCDF blood concentration and excessive eye discharge. (Table 5)
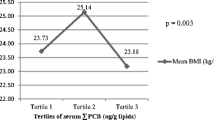
PCQ blood concentration as an objective variable, tooth pigmentation, arthralgia, γ-GTP, total bilirubin, cheesy secretion from meibomian glands, general fatigue, total cholesterol, toe nail pigmentation, female gender, and oral mucosa pigmentation all showed less than a 0.05 level of significance. When 2,3,4,7,8-PeCDF blood concentration was excluded from the explanatory variables, past history of pigmentation, tooth pigmentation, PCB blood concentrations, acneform eruption, abdominal pain, pigmentation, and total cholesterol were significantly correlated with PCQ blood concentrations. (Table 6)
Discussion
PCBs, PCQs and PCDFs are known as the causative agents of Yusho. The results from this study show that, the concentrations of 2,3,4,7,8-PeCDF, PCB and PCQ in blood were strongly related. The blood concentrations of 2,3,4,7,8-PeCDF, PCB and PCQ tended to correlate with older age, as adult victims were considered to have eaten greater amounts of the contaminated oil compared with child victims when the contaminated oil was available in shops in 1968. The blood concentrations of 2,3,4,7,8-PeCDF, PCB and PCQ also tended to correlate with female gender. This may be attributed to the fact that these chlorinated compounds are highly lipophilic and accumulate in adipose tissue [3]. Females who have more adipose tissue may have thus accumulated more 2,3,4,7,8-PeCDF, PCB and PCQ.
In our study, the blood concentrations of 2,3,4,7,8-PeCDF, PCB and PCQ also tended to correlate with acneform eruptions, black comedones, cutaneous and mucosal pigmentation, and hypersecretion of meibomian glands, in addition to general fatigue, headaches, cough, sputum, abdominal pain, increased serum γ-GTP, and decreased total bilirubin. These signs and symptoms are all included in the present diagnostic criteria of Yusho (Table 1). In addition to the symptoms listed in the diagnostic criteria, arthralgia was frequently correlated to 2,3,4,7,8-PeCDF, PCB and PCQ blood concentrations. Using the 2,3,4,7,8-PeCDF blood concentration as an objective variable, cases including or not including the PCB and PCQ concentrations as explanatory variables were compared. As a result, arthralgia and A/G ratio were related to the 2,3,4,7,8-PeCDF blood concentration.
Using the PCB blood concentration as an objective variable, cases including or not including the 2,3,4,7,8-PeCDF concentration as an explanatory variable were compared. As a result, PCB blood concentration was strongly related to ophthalmological symptoms.
The PCQ blood concentration was related to cutaneous, oral and ophthalmological manifestations, increased γ-GTP, and increased total cholesterol. When the 2,3,4,7,8-PeCDF blood concentration was excluded in the explanatory variables, oral pigmentation and increased total cholesterol were significantly related to PCQ blood concentration. The biochemical adverse effect of PCQ has been reported to include increased triacylglycerol concentration [20]. However, based on the results of this study, total cholesterol concentration, one of the markers of lipid metabolism such as triacylglycerol, was related to PCQ blood concentration.
Like Kanemi Yusho, Taiwan Yucheng, a health hazard caused by PCB or PCDFs, has been reported to have a high incidence of symptoms of chloracne, goiter, arthritis, and anemia [21, 22]. Chloracne and arthritis are considered e symptoms common to Yusho and Taiwan Yucheng. Health hazards caused by 2,3,7,8-tetrachlorodibenzo-p-dioxin (TCDD) in the Seveso (Italy) event have also been studied. In a death survey, conducted 20–25 years after the Seveso (Italy) event, a high incidence of deaths due to cancer, circulatory disease, chronic obstructive pulmonary disease (COPD), and diabetes mellitus was reported [23, 24]. It thus seems necessary to examine the presence of a relationship between Yusho and COPD in the future, since cough, sputum, and bursitis, included in the Yusho criteria, are also symptoms seen in COPD.
Cutaneous, mucosal and ophthalmological manifestations, related to the blood concentrations of 2,3,4,7,8-PeCDF, PCB and PCQ in this study, were considered characteristic of Yusho and were included in the diagnostic criteria.
Conclusion
Although 35 years have passed since the occurrence of Yusho, the 2,3,4,7,8-PeCDF blood concentration appeared related to the PCQ and PCB blood concentrations, arthralgia and A/G ratio; The blood PCB concentration was strongly related to ophthalmological symptoms; while PCQ blood concentration was related to total cholesterol. These findings suggest that the co-contaminants may affect other functions than those originally associated with Yusho.
Abbreviations
- PCBs:
-
polychlorinated biphenyls
- PCQs:
-
polychlorinated quarterphenyls
- PCDFs:
-
polychlorinated dibenzofurans
- TCDD:
-
2,3,7,8-tetrachlorodibenzo-p-dioxin.
References
Masuda Y: Behavior and toxic effects of PCBs and PCDFs in Yusho patients for 35 years. J Dermatol Sci. 2005, S11-S20. Suppl 1
Furue M, Uenotsuchi T: Steps for establishment of the diagnostic standard in Yusho patients. Fukuoka Igaku Zasshi. 2005, 96: 124-134. (In Japanese)
Furue M, Uenotsuchi T, Urabe K, Ishikawa T, Kuwabara M: Overview of Yusho. J Dermatol Sci. 2005, S3-S10. Suppl 1
Kuratsune M, Yoshimura H, Hori Y, Okumura M, Matsuda Y: Yusho – A human disaster caused by PCB and related compounds. 1996, Kyushu University Press, Fukuoka
Yamaguchi N, Kaneko S: A study on evaluation of carcinogenesis in patients with Yusho and A study on health evaluation in Yusho. 2001, 2002. Health and Labour Sciences Research. (integrated study report, summarized and allotted study report). 2002
Imamura T, Kanagawa Y: A study on correlations between blood serum levels of PCDFs and clinical symptoms in patients with Yusho (78 patients for 2001, 279 patients for 2002). Health and Labour Sciences Research, Summarized and allotted study report. 2003, (In Japanese)
Kanagawa Y, Imamura T: Relationship between blood PCDFs level and symptoms in Yusho patients. Fukuoka Igaku Zasshi. 2005, 96: 169-179. (In Japanese)
Kanagawa Y, Imamura T: Relationship of clinical symptoms and laboratory findings with the blood serum levels of PCDFs in patients with Yusho. J Dermatol Sci. 2005, S85-S93. Suppl 1
Uenotsuchi T, Furue M, Nakayama J, Asahi M, Kanagawa Y, Imamura T: Evaluation of dermatological symptoms of Yusho patients in the annual examinations of 2003–2004. Fukuoka Igaku Zasshi. 2005, 96: 216-219. (In Japanese)
Uenotsuchi T, Inoo Y, Tadakuma S, Haratsuka R, Kanagawa Y, Imamura T, Furue M: Sex ratio of newborn infants from parents with Yusho. Fukuoka Igaku Zasshi. 2005, 96: 183-184. (In Japanese)
Uenotsuchi T, Lio Y, Tadakuma S, Haraduka R, Kanagawa Y, Imamura T, Furue M: Sex ratio in the children of Yusho patients. J Dermatol Sci. 2005, S81-S83. Suppl 1
Uenotsuchi T, Nakayama J, Asahi M, Kohro O, Akimoto T, Muto M, Shimizu K, Katayama I, Kanzaki Y, Kanagawa Y, Imamura T, Furue M: Dermatological manifestations in Yusho: correlation between skin symptoms and blood levels of dioxins, such as polychlorinated dibenzofurans (PCDFs) and polychlorinated biphenyls (PCBs). J Dermatol Sci. 2005, S73-S80. Suppl 1
Uenotsuchi T, Nakayama K, Asahi S, Takamichi O, Akimoto T, Muto M, Kiyomizu K, Katayama I, Kanzaki Y, Kanagawa Y, Imamura T, Furue M: Skin symptoms in Yusho patients related to blood dioxin level. Fukuoka Igaku Zasshi. 2005, 96: 164-168. (In Japanese)
Imamura T, Matsumoto S, Kanagawa Y, Tajima B, Matsuya S, Furue M, Oyama HA: Technique for identifying three diagnostic findings using association analysis. Med Biol Eng Comput. 2007, 45 (1): 51-59. 10.1007/s11517-006-0121-6.
Imamura T, Kanagawa Y, Matsumoto S, Tajima B, Uenotsuchi T, Shibata S, Furue M: Relationship between clinical features and blood levels of pentachlorodibenzofuran in patients with Yusho. Environmental Toxicology. 2007, 22 (2): 221-237. 10.1002/tox.20251.
Imamura T, Kanagawa Y, Matsumoto S, Tajima B, Uenotsuchi T, Shibata S, Furue M: Epidemiological Aspects of Yusho; Clinical features and blood levels of Pentachlorodibenzofuran in Yusho Patients. DIOXIN 2007 27th International Symposium. Organohalogen Compounds. 2007, 69: 87-90.
Iida T, Todaka T, Hirakawa H, Tobiishi K, Matsueda T, Hori T, Nakagawa R, Furue M: Follow-up survey of dioxins in the blood of Yusho (in 2001). Fukuoka Igaku Zasshi. 2003, 94: 126-135.
Todaka T, Hirakawa H, Tobiishi K, Iida T: New protocol of dioxins analysis in human blood. Fukuoka Igaku Zasshi. 2003, 94: 148-157.
Masuda Y, Yoshimura T, Kajiwara J: Changes in PCBs and PCDFs blood levels in patients for 38 years since the occurrence of Yusho. Fukuoka Igaku Zasshi. 2007, 98 (5): 182-195.
Kunita N, Kashimoto T: Biological effects of PCB-related substances. The Saishin-Igaku. 1982, 57: 378-383. (In Japanese)
Guo YL, Yu ML, Hsu CC, Rogan WJ: Chloracne, goiter, arthritis, and anemia after polychlorinated biphenyl poisoning: 14-year follow-Up of the Taiwan Yucheng cohort. Environ Health Perspect. 1999, 107 (9): 715-719. 10.2307/3434656.
Guo YL, Lambert GH, Hsu CC, Hsu MM: Yucheng health effects of prenatal exposure to polychlorinated biphenyls and dibenzofurans. Int Arch Occup Environ Health. 2004, 77 (3): 153-158. 10.1007/s00420-003-0487-9.
Bertazzi PA, Consonni D, Bachetti S, Rubagotti M, Baccarelli A, Zocchetti C, Pesatori AC: Health effects of dioxin exposure: a 20-year mortality study. Am J Epidemiol. 2001, 153 (11): 1031-1044. 10.1093/aje/153.11.1031.
Consonni D, Pesatori AC, Zocchetti C, Sindaco R, D'Oro LC, Rubagotti M, Bertazzi PA: Mortality in a population exposed to dioxin after the Seveso, Italy, accident in 1976: 25 years of follow-up. Am J Epidemiol. 2008, 167 (7): 847-858. 10.1093/aje/kwm371.
Acknowledgements
We acknowledge the support from a Grant-in-Aid for scientific research from the Ministry of Health, Labour and Welfare, Japan.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
YK designed the study and drafted the manuscript. SM designed the data analysis, analyzed data, and assisted manuscript drafting. SK assisted manuscript drafting. BT assisted designing of data analysis. NF, SS and HU collected data. MF designed the whole study and assisted manuscript drafting. All the authors, except TI, reviewed the final manuscript and all authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Kanagawa, Y., Matsumoto, S., Koike, S. et al. Association of clinical findings in Yusho patients with serum concentrations of polychlorinated biphenyls, polychlorinated quarterphenyls and 2,3,4,7,8-pentachlorodibenzofuran more than 30 years after the poisoning event. Environ Health 7, 47 (2008). https://doi.org/10.1186/1476-069X-7-47
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1476-069X-7-47