
Abstract
This article reviews the comprehensive data on the safety and tolerability from over 6,300 patients who have taken artemether/lumefantrine (Coartem®) as part of Novartis-sponsored or independently-sponsored clinical trials. The majority of the reported adverse events seen in these studies are mild or moderate in severity and tend to affect the gastrointestinal or nervous systems. These adverse events, which are common in both adults and children, are also typical of symptoms of malaria or concomitant infections present in these patients. The wealth of safety data on artemether/lumefantrine has not identified any neurological, cardiac or haematological safety concerns. In addition, repeated administration is not associated with an increased risk of adverse drug reactions including neurological adverse events. This finding is especially relevant for children from regions with high malaria transmission rates who often receive many courses of anti-malarial medications during their lifetime. Data are also available to show that there were no clinically relevant differences in pregnancy outcomes in women exposed to artemether/lumefantrine compared with sulphadoxine-pyrimethamine during pregnancy. The six-dose regimen of artemether/lumefantrine is therefore well tolerated in a wide range of patient populations. In addition, post-marketing experience, based on the delivery of 250 million treatments as of July 2009, has not identified any new safety concerns for artemether/lumefantrine apart from hypersensitivity and allergies, known class effects of artemisinin derivatives.
Similar content being viewed by others

Background
Malaria is one of the most significant causes of morbidity and mortality worldwide, causing approximately 881,000 deaths every year [1]. The current WHO guidelines for the treatment of malaria recommend the use of artemisinin-based combination therapy (ACT) owing to the rising threat of Plasmodium falciparum resistance to monotherapy [2]. Artemether/lumefantrine (AL) was the first fixed-dose combination of ACT to be approved by the European regulatory authorities according to the requirements of the International Committee on Harmonization (ICH). AL is also pre-qualified by WHO for efficacy, safety and quality and is marketed as Coartem® for use as a six-dose regimen in infants, children and adults with acute, uncomplicated infection due to P. falciparum or mixed infections including P. falciparum [3, 4].
The efficacy of AL has been confirmed in many different patient populations around the world and is discussed elsewhere in this supplement [5]. This article reviews the comprehensive safety data on AL that has been reported in the scientific literature from Novartis-sponsored and independent clinical trials.
Novartis-sponsored studies
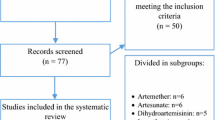
Six Novartis-sponsored clinical studies [6–11] have been conducted to assess efficacy and safety of the six-dose regimen of AL, with safety data from these summarized in Table 1. These studies were conducted in different regions of the world and so included patients who lived in areas with varying levels of drug resistant P. falciparum and malaria endemicity. Some of the studies included other anti-malarial drugs as active comparators [7, 8], one allowed the inclusion of patients with mixed infections that included P. falciparum [10], and one utilized a dispersible paediatric formulation [11].
In all of these studies AL was well tolerated and most reported adverse events were of mild or moderate severity. Reported adverse events occurred mainly in the nervous system or gastrointestinal system and were considered typical of the symptomatology of malaria or concomitant infections. No cardiac, neurological or audiological safety issues were identified in the studies that assessed these safety parameters [6–11].
Comparative results from independent studies
Many independent trials on AL have also been published in the scientific literature. Results from the studies conducted in Africa [12–32] are summarized in Table 2 and the results from studies conducted in Asia [33–39] in Table 3. The safety findings from these trials confirm the results of the Novartis-sponsored studies, namely that the majority of adverse events were mild or moderate in severity, tended to affect the gastrointestinal or nervous system, and were consistent with the symptoms of malaria. Serious adverse events were infrequent and were unrelated or unlikely to be related to study medication.
Data have also been pooled to provide a more complete assessment of the safety and tolerability of AL in a large number (>1,900) of adult and paediatric patients. The results of two of these meta-analyses, Mueller et al and Makanga et al are shown in Table 4[40, 41]. These pooled results confirm earlier data and show that AL is generally well tolerated with the majority of reported adverse events again affecting either the gastrointestinal or nervous systems and of mild or moderate severity [40, 41]. Few adverse events were considered by the investigators to be drug-related - most were regarded as being related to the symptomatology of malaria. Serious adverse events occurred infrequently [40, 41]. There were, however, some differences in the adverse event profile in children when different body weights were compared, but this is unlikely to be of clinical relevance. Instead, it is more likely to be related to the subjective nature of these adverse events and the differences in the ability of young infants and children to verbalize these complaints [41].
Special safety considerations
Neurological and audiological safety
There have been case reports of neurological problems (including ataxia, nystagmus, tremor and slurred speech) occurring after administration of herbal artemisinin [42] or artesunate monotherapy [43, 44]. However, it is questionable whether these neurological effects are related to artemisinin treatment [45–47]. Indeed, this is not supported by audiology case-control [48–50] or other audiology data [14, 51], although additional analyses are often called for to investigate this fully. There were, however, no neurological or audiological safety concerns identified for AL in the Novartis-sponsored studies [6–10, 52] as shown in Table 1. In addition, audiological data are currently being analysed from a Novartis-sponsored study in 265 patients treated with AL, malarone or mefloquine-artesunate. [Personal communication with Novartis, study A2417). A routine review of the data collected from the first 85 patients, however, did not raise any safety concerns. Neurological or audiological safety concerns have not been identified in the African studies by Bukirwa et al [12], Gürkov et al [14], and Adjei et al [20], as shown in Table 2, Asian studies by Krudsood et al [33], and Mayxay et al [35], as shown in Table 3, and in the pooled analyses reported by Mueller et al [40] or Makanga et al [41], which are summarized in Table 4.
Cardiac safety
Lumefantrine is chemically related to halofantrine, an anti-malarial known to be associated with significant prolongation of QTc interval. Indeed, QTc prolongation is a known class effect of many anti-malarial drugs. As such, cardiac safety has been thoroughly investigated during the preclinical and clinical development of AL.
The effects of lumefantrine and its major metabolite desbutyl-lumefantrine on wild-type hERG K+ channels have been investigated in stably transfected human embryonic kidney cells (HEK293) using a whole cell patch-clamp technique [52]. This in vitro hERG channel assay showed that lumefantrine and desbutyl-lumefantrine have higher IC50 values (approximately 200-fold) than halofantrine (see Table 5). In addition, the calculated cardiac safety indices, which are over 30 for lumefantrine, suggest that lumefantrine and its major metabolite pose an unlikely risk of cardiotoxocity compared with halofantrine [52]. A phase I, parallel group study with AL, moxifloxacin and placebo arms (n = 42 per group) was conducted in healthy volunteers to assess cardiac safety [52]. As shown in Figure 1, this study demonstrated that the six-dose regimen of AL was associated with a mean maximum increase in QTc (Fridericia's formula) of 7.45 msec compared with placebo (90% CI: 4.4 to 10.5 msec) in healthy volunteers. By comparison, the effect on QTc (Fridericia's formula) was much greater after dosing with moxifloxacin, the positive control. A formal analysis of the relationship between the plasma concentration of lumefantrine and the change from mean baseline in QTc (Fridericia's formula) was conducted (see Figure 2). This shows that the 95% confidence limit for the mean lumefantrine plasma concentration does not cross the upper confidence band for the threshold of relevance for change in QTc (Fridericia's formula).

Placebo-corrected mean change in QTc (Fridericia's formula) from time-averaged baseline in healthy volunteers. [Data on file (study A2101), Novartis]. AL = artemether/lumefantrine; CI = confidence interval.

Relationship between QTc (Fridericia's formula) and maximum plasma concentration (C max ) in healthy volunteers. [Data on file (study A2101), Novartis]. Note: the threshold of relevance for QTc change is 10 msec vs. placebo.
One possible explanation for the alterations in QTc seen with AL may be due to malaria itself and recovery from this disease, as well as to stress and anaemia. These conditions can affect cardiac electrophysiology and may lengthen the QT interval [53]. As QT correction formulae are based on a normal heart rate of 60 beats/minute, and patients with malaria tend to have elevated heart rates that decrease with successful treatment and defervescence, overcorrection of the QT interval can also occur. This is even more pronounced in small children, and heart rates higher than 60 beats/minute are routinely seen in healthy children. Despite the changes in QTc associated with malaria, no adverse events attributable to QTc prolongation (e.g. syncope or sudden death) have been reported in clinical trials with AL [6] as shown in Table 1[6–11], Table 3[39], and Table 4[40, 41].
Haematological safety
Preclinical data suggested that repeated exposure to AL may affect blood cell counts and as such, particular attention was paid to haemoglobin levels and haematological adverse events reported during clinical trials. A published pooled analysis of 15 trials conducted in China, India, Thailand, The Gambia, Tanzania, France, The Netherlands and the UK confirmed these results [54]. Indeed, in this analysis, anaemia and thrombocytopaenia were frequently present at baseline, but returned to normal or improved considerably with the resolution of disease [54]. No haematological safety concerns were identified during the safety assessment presented in this review.
Safety of repeated administration
Most safety data on antimalarials are collected as part of clinical trials and these tend to evaluate the treatment of a single episode of malaria. In practice, however, children in areas of high malaria endemicity are likely to suffer from repeated episodes of malaria and this raises concerns over potential toxicity due to repeated short-term exposure to the drugs.
Two longitudinal studies have therefore attempted to address this question by assessing the efficacy, safety and tolerability of amodiaquine-artesunate versus AL [55] and amodiaquine plus sulphadoxine-pyrimethamine versus artesunate-amodiaquine versus AL [56] after repeated use.
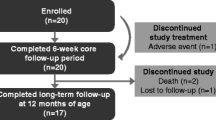
These studies in Ghanaian and Ugandan children indicated all treatments were efficacious, but the various treatments were associated with slightly different adverse event profiles. For example, treatment with amodiaquine plus sulphadoxine-pyrimethamine had a greater risk compared with AL of anorexia, weakness and subjective fever and a greater risk compared with artesunate-amodiaquine of weakness and subjective fever. Children treated with AL, however, had a higher risk of elevated temperature than those receiving artesunate-amodiaquine [56]. In both studies, repeated administration of AL did not seem to be associated with an increased risk of adverse drug reactions. The study in Ghanaian children also included neurological examinations for children treated with repeated artemisinin-based regimens. This did not identify any abnormal neurological signs that were considered related to artemisinin [55].
Comparison with other anti-malarial therapies
The safety of the six-dose regimen of AL has been compared with MAS in two Novartis-sponsored, open-label randomized trials [7, 8, 52], as summarized in Table 1. In these two studies, 314 patients received AL and 105 patients received MAS. Overall, AL was at least as well tolerated as MAS, and had a similar safety profile (Table 6) [52]. Only one patient, who developed urticarial rash, experienced a serious adverse event that was thought to be treatment-related [52]. Independent studies have also compared AL with other anti-malarial therapies as shown in Table 2, Table 3 and Table 4[12–40]. These studies showed that AL was at least as well tolerated as the various comparators (AQSP, ASAQ, ASCD, ASSP, AS plus sulphamethoxypyrazine plus pyrimethamine, atovaquone/proguanil, CQ, CQSP, DP, DNP, MAS, quinine, or SP) used in clinical trials.
Safety in pregnancy
Pregnant women with symptomatic malaria, and especially those in their second and third trimesters, are more likely to develop severe malaria than other women [2]. In addition, this is often complicated by pulmonary oedema and hypoglycaemia [2]. Prompt, safe, and effective treatment is, therefore, recommended in this high risk group to reduce maternal mortality, foetal death and premature labour [2]. ACT can be used in uncomplicated malaria in the second and third trimester. The use of ACT in the first trimester should, however, only be considered if they are the only effective treatment available and the benefits outweigh the risks of treatment [2, 4]. In severe malaria, ACT is preferred over quinine due to the hypoglycaemia associated with quinine. Until recently there has been limited evidence available to support the use of ACT in early pregnancy; however, McGready et al published data on the use of AL in pregnancy in 2009 [57]. These data were from a prospective eight-year study in Thailand on pregnant women exposed to artemisinin antimalarials. In this study, birth outcomes did not differ significantly from community rates of congenital malformations and stillbirth [57]. In addition, data from a prospective observational study to compare the safety of AL and SP in pregnant women treated for symptomatic falciparum malaria was presented at ASTMH Annual Meeting in December 2008 [58]. This study analysed data from 1,001 pregnant women (AL: n = 495; SP: n = 506) and their foetuses/newborns (AL: n = 470; SP: n = 477). There were no clinically relevant differences in perinatal mortality, neonatal mortality, still births, preterm deliveries, gestational age-adjusted low birth weight or birth defects between the two groups.
Post-marketing experience
As of July 2009, 250 million AL treatments (70% of which were for children) have been delivered to malaria-endemic countries. Post-marketing experience has not identified any new specific safety concerns apart from hypersensitivity and skin reactions (allergies), a recognized class effect for artemisinin derivatives [2].
Conclusion
This review summarizes some of the safety and tolerability data on AL (Coartem®) from published Novartis-sponsored and independently-sponsored clinical trials. Data are available to support the use of a six-dose regimen of AL as a safe and well-tolerated treatment for P. falciparum malaria or malaria due to mixed infection including P. falciparum in adults, adolescents, children and infants. Indeed, the safety profile of this drug is similar in both adults and children, and many of the reported adverse events are typical of symptoms of malaria or concomitant infections that are commonly seen in these patient populations. Reported adverse events are mainly of mild or moderate severity, with very few serious adverse events reported and even fewer serious adverse events considered related to treatment. In addition, no notable neurological adverse events or cardiac safety concerns were identified in the many studies that examined the safety of AL. As patients (and especially children) often take repeated courses of treatment for malaria, it is reassuring to note that data are available that show repeated administration of AL is not associated with an increased risk of adverse drug reactions, in particular with regard to neurological adverse events. In addition, a thorough review of the clinical data for AL does not identify any potential cardiac safety issues. Data are also available to show that there were no clinically relevant differences in perinatal mortality, neonatal mortality, still birth, pre-term delivery, low birth weight and spontaneous abortion in women exposed to AL compared with SP during pregnancy.
In conclusion, AL is a safe and well-tolerated treatment for P. falciparum infections that should help fight malaria. Indeed, as of July 2009, 250 million AL (Coartem®) treatments have been delivered and post-marketing experience confirms the favourable safety and tolerability profile for this drug. In addition, this wealth of safety evidence has not identified any safety concerns for AL apart from rare type 1 hypersensitivity reactions, a recognized class effect of artemisinin derivatives [2].
Abbreviations
- ACT:
-
Artemisinin-based combination therapy
- AE:
-
Adverse event
- AL:
-
Artemether/lumefantrine
- AQ:
-
Amodiaquine
- AQSP:
-
Amodiaquine plus sulphadoxine-pyrimethamine
- AS:
-
Artesunate: ASAQ: Artesunate plus amodiaquine
- ASTMH:
-
American Society of Tropical Medicine and Hygiene
- CQ:
-
Chloroquine
- CQSP:
-
Chloroquine plus sulphadoxine-pyrimethamine
- DNP:
-
Dihydroartemisinin plus napthoquine plus trimethoprim
- DP:
-
Dihydroartemisinin-piperaquine
- ECG:
-
Electrocardiogram (also known as EKG)
- hERG:
-
Human ether-a-go-go related gene
- IC50:
-
Inhibitory concentration 50 (the concentration that gives 50% inhibition)
- ICH:
-
International Conference on Harmonization
- IKr:
-
Rectifying K+ current
- MAS:
-
Mefloquine plus artesunate
- MedDRA:
-
Medical Dictionary for Regulatory Activities
- SAE:
-
Serious adverse event
- SP:
-
Sulphadoxine-pyrimethamine
- vs.:
-
Versus
- WHO:
-
World Health Organization.
References
WHO World Malaria Report 2008: Chapter 1 - Introduction. [http://www.who.int/malaria/wmr2008/]
WHO Guidelines for the treatment of malaria 2006. [http://www.who.int/malaria/docs/TreatmentGuidelines2006.pdf]
WHO Prequalified Medicines List. [http://apps.who.int/prequal/default.htm]
Novartis Drug Regulatory Affairs: Coartem®/Riamet® Basic Prescribing Information. 2009
Makanga M, Krudsood S: The clinical efficacy of artemether/lumefantrine (Coartem®). Malar J. 2009, 8 (Suppl 1): S5-10.1186/1475-2875-8-S1-S5.
van Vugt M, Wilairatana P, Gemperli B, Gathmann I, Phaipun L, Brockman A, Luxemburger C, White NJ, Nosten F, Looareesuwan S: Efficacy of six doses of artemether/lumefantrine (benflumetol) in multidrug-resistant Plasmodium falciparum malaria. Am J Trop Med Hyg. 1999, 60: 936-942.
van Vugt M, Looareesuwan S, Wilairatana P, McGready R, Villegas L, Gathmann I, Mull R, Brockman A, White NJ, Nosten F: Artemether/lumefantrine for the treatment of multi-drug resistant falciparum malaria. Trans R Soc Trop Med Hyg. 2000, 94: 545-548. 10.1016/S0035-9203(00)90082-8.
Lefèvre G, Looareesuwan S, Treeprasertsuk S, Krudsood S, Silachamroon U, Gathmann I, Mull R, Bakshi R: A clinical and pharmacoki-netic trial of six doses of artemether/lumefantrine for multidrug-resistant Plasmodium falciparum malaria in Thailand. Am J Trop Med Hyg. 2001, 64: 247-256.
Falade C, Makanga M, Premji Z, Ortmann CE, Stockmeyer M, de Palacios PI: Efficacy and safety of artemether/lumefantrine (Coartem®) tablets (six-dose regimen) in African infants and children with acute, uncomplicated falciparum malaria. Trans R Soc Trop Med Hyg. 2005, 99: 459-467. 10.1016/j.trstmh.2004.09.013.
Hatz C, Soto J, Nothdurft HD, Zoller T, Weitzel T, Loutan L, Bricaire F, Gay F, Burchard GD, Andriano K, Lefèvre G, De Palacios PI, Genton B: Treatment of acute uncomplicated falciparum malaria with artemether/lumefantrine in non-immune populations: a safety, efficacy and pharmacokinetic study. Am J Trop Med Hyg. 2008, 78: 241-247.
Abdulla S, Sagara I, Borrmann S, D'Alessandro U, González R, Hamel M, Ogutu B, Mårtensson A, Lyimo J, Maiga H, Sasi P, Nahum A, Bassat Q, Juma E, Otieno L, Björkman A, Beck HP, Andriano K, Cousin M, Lefèvre G, Ubben D, Premji Z: Efficacy and safety of artemether/lumefantrine dispersible tablets compared with crushed commercial tablets in African infants and children with uncomplicated malaria: a randomised, single-blind, multi-centre trial. Lancet. 2008, 372: 1819-1827. 10.1016/S0140-6736(08)61492-0.
Bukirwa H, Yeka A, Kamya MR, Talisuna A, Banek K, Bakyaita N, Rwakimari JB, Rosenthal PJ, Wabwire-Mangen F, Dorsey G, Staedke SG: Artemisinin combination therapies for treatment of uncomplicated malaria in Uganda. PLoS Clin Trials. 2006, 1: e7-10.1371/journal.pctr.0010007.
Dorsey G, Staedke S, Clark TD, Njama-Meya D, Nzarubara B, Maiteki-Sebuguzi C, Dokomajilar C, Kamya MR, Rosenthal PJ: Combination therapy for uncomplicated falciparum malaria in Ugandan children. JAMA. 2007, 297: 2210-2219. 10.1001/jama.297.20.2210.
Gürkov R, Eshetu T, Miranda IB, Berens-Riha N, Mamo Y, Girma T, Krause E, Schmidt M, Hempel JM, Löscher T: Ototoxicity of artemether/lumefantrine in the treatment of falciparum malaria: a randomized trial. Malar J. 2008, 7: 179-10.1186/1475-2875-7-179.
Kamya MR, Yeka A, Bukirwa H, Lugemwa M, Rwakimari JB, Staedke SG, Talisuna AO, Greenhouse B, Nosten F, Rosenthal PJ, Wabwire-Mangen F, Dorsey G: Artemether/lumefantrine versus dihydroartemisinin-piperaquine for treatment of malaria: a randomized trial. PLoS Clin Trials. 2007, 2: e20-10.1371/journal.pctr.0020020.
Mårtensson A, Strömberg J, Sisowath C, Msellem MI, Gil JP, Montgomery SM, Olliaro P, Ali AS, Björkman A: Efficacy of artesunate plus amodiaquine versus that of artemether/lumefantrine for the treatment of uncomplicated childhood Plasmodium falciparum malaria in Zanzibar, Tanzania. Clin Infect Dis. 2005, 41: 1079-1087. 10.1086/444460.
Mohamed AO, Eltaib EH, Ahmed OA, Elamin SB, Malik EM: The efficacies of artesunate-sulfadoxine-pyrimethamine and artemether/lumefantrine in the treatment of uncomplicated, Plasmodium falciparum malaria, in an area of low transmission in central Sudan. Ann Trop Med Parasitol. 2006, 100: 5-10. 10.1179/136485906X86239.
Yeka A, Dorsey G, Kamya MR, Talisuna A, Lugemwa M, Rwakimari JB, Staedke SG, Rosenthal PJ, Wabwire-Mangen F, Bukirwa H: Artemether/lumefantrine versus dihydroartemisinin-piperaquine for treating uncomplicated malaria: a randomized trial to guide policy in Uganda. PLoS ONE. 2008, 3: e2390-10.1371/journal.pone.0002390.
Mulenga M, Van geertruyden J-P, Mwananyanda L, Chalwe V, Moerman F, Chilengi R, Van Overmeir C, Dujardin JC, D'Alessandro U: Safety and efficacy of lumefantrine-artemether (Coartem®) for the treatment of uncomplicated Plasmodium falciparum malaria in Zambian adults. Malar J. 2006, 5: 73-10.1186/1475-2875-5-73.
Adjei GO, Kurtzhals JA, Rodrigues OP, Alifrangis M, Hoegberg LC, Kitcher ED, Badoe EV, Lamptey R, Goka BQ: Amodiaquine-artesunate vs artemether/lumefantrine for uncomplicated malaria in Ghanaian children: a randomized efficacy and safety trial with one year follow-up. Malar J. 2008, 7: 127-10.1186/1475-2875-7-127.
Falade CO, Ogundele AO, Yusuf BO, Ademowo OG, Ladipo SM: High efficacy of two artemisinin-based combinations (artemether/lumefantrine and artesunate plus amodiaquine) for acute uncomplicated malaria in Ibadan, Nigeria. Trop Med Int Health. 2008, 13: 35-643.
Faye B, Ndiaye JL, Ndiaye D, Dieng Y, Faye O, Gaye O: Efficacy and tolerability of four antimalarial combinations in the treatment of uncomplicated Plasmodium falciparum malaria in Senegal. Malar J. 2007, 6: 80-10.1186/1475-2875-6-80.
Koram KA, Abuaku B, Duah N, Quashie N: Comparative efficacy of antimalarial drugs including ACTs in the treatment of uncomplicated malaria among children under 5 years in Ghana. Acta Trop. 2005, 95: 194-203. 10.1016/j.actatropica.2005.06.018.
Owusu-Agyei S, Asante KP, Owusu R, Adjuik M, Amenga-Etego S, Dosoo DK, Gyapong J, Greenwood B, Chandramohan D: An open label, randomised trial of artesunate+amodiaquine, artesunate+chlorproguanil-dapsone and artemether/lumefantrine for the treatment of uncomplicated malaria. PLoS ONE. 2008, 3: e2530-10.1371/journal.pone.0002530.
Sagara I, Dicko A, Djimde A, Guindo O, Kone M, Tolo Y, Thera MA, Sogoba M, Fofana M, Ouattara A, Sissoko M, Jansen HF, Doumbo OK: A randomized trial of artesunate-sulfamethoxypyrazine-pyrimethamine versus artemether/lumefantrine for the treatment of uncomplicated Plasmodium falciparum malaria in Mali. Am J Trop Med Hyg. 2006, 75: 630-636.
Sowunmi A, Gbotosho GO, Happi CT, Adedeji AA, Fehintola FA, Folarin OA, Tambo E, Fateye BA: Therapeutic efficacy and effects of artemether/lumefantrine and amodiaquine-sulfalene-pyrimethamine on gametocyte carriage in children with uncomplicated Plasmodium falciparum malaria in southwestern Nigeria. Am J Trop Med Hyg. 2007, 77: 235-241.
Sutherland CJ, Ord R, Dunyo S, Jawara M, Drakeley CJ, Alexander N, Coleman R, Pinder M, Walraven G, Targett GA: Reduction of malaria transmission to Anopheles mosquitoes with a six-dose regimen of co-artemether. PLoS Med. 2005, 2: e92-10.1371/journal.pmed.0020092.
Zongo I, Dorsey G, Rouamba N, Tinto H, Dokomajilar C, Guiguemde RT, Rosenthal PJ, Ouedraogo JB: Artemether/lumefantrine versus amodiaquine plus sulfadoxine-pyrimethamine for uncomplicated falciparum malaria in Burkina Faso: a randomised non-inferiority trial. Lancet. 2007, 369: 91-498. 10.1016/S0140-6736(07)60236-0.
Zongo I, Dorsey G, Rouamba N, Dokomajilar C, Séré Y, Rosenthal PJ, Ouédraogo JB: Randomized comparison of amodiaquine plus sulfadoxine-pyrimethamine, artemether/lumefantrine, and dihydroartemisinin-piperaquine for the treatment of uncomplicated Plasmodium falciparum malaria in Burkina Faso. Clin Infect Dis. 2007, 45: 1453-1461. 10.1086/522985.
Fanello CI, Karema C, van Doren W, van Overmeir C, Ngamije D, D'Alessandro U: A randomised trial to assess the safety and efficacy of artemether/lumefantrine (Coartem®) for the treatment of uncomplicated Plasmodium falciparum malaria in Rwanda. Trans R Soc Trop Med Hyg. 2007, 101: 344-350. 10.1016/j.trstmh.2006.06.010.
Ndayiragije A, Niyungeko D, Karenzo J, Niyungeko E, Barutwanayo M, Ciza A, Bosman A, Moyou-Somo R, Nahimana A, Nyarushatsi JP, Barihuta T, Mizero L, Ndaruhutse J, Delacollette C, Ringwald P, Kamana J: [Efficacité de combinaisons thérapeutiques avec des dérivés de l'artémisinine dans le traitement de l'accès palustre non-compliqué au Burundi]. Trop Med Int Health. 2004, 9: 673-679. 10.1111/j.1365-3156.2004.01255.x.
Broek van den I, Kitz C, Al Attas S, Libama F, Balasegaram M, Guthmann JP: Efficacy of three artemisinin combination therapies for the treatment of uncomplicated Plasmodium falciparum malaria in the Republic of Congo. Malar J. 2006, 5: 113-10.1186/1475-2875-5-113.
Krudsood S, Chalermrut K, Pengruksa C, Srivilairit S, Silachamroon U, Treeprasertsuk S, Kano S, Brittenham GM, Looareesuwan S: Comparative clinical trial of two-fixed combinations dihydroartemisinin-napthoquine-trimethoprim (DNP®) and artemether/lumefantrine (Coartem®/Riamet®) in the treatment of acute uncomplicated falciparum malaria in Thailand. Southeast Asian J Trop Med Public Health. 2003, 34: 316-321.
Stohrer JM, Dittrich S, Thongpaseuth V, Vanisaveth V, Phetsouvanh R, Phompida S, Monti F, Christophel EM, Lindegardh N, Annerberg A, Jelinek T: Therapeutic efficacy of artemether/lumefantrine and artesunate-mefloquine for treatment of uncomplicated Plasmodium falciparum malaria in Luang Namtha Province, Lao People's Democratic Republic. Trop Med Int Health. 2004, 9: 1175-1183. 10.1111/j.1365-3156.2004.01320.x.
Mayxay M, Khanthavong M, Lindegårdh N, Keola S, Barends M, Pongvongsa T, Yapom R, Annerberg A, Phompida S, Phetsouvanh R, White NJ, Newton PN: Randomized comparison of chloroquine plus sulfadoxine-pyrimethamine versus artesunate plus mefloquine versus artemether/lumefantrine in the treatment of uncomplicated falciparum malaria in the Lao People's Democratic Republic. Clin Infect Dis. 2004, 39: 1139-1147. 10.1086/424512.
Ratcliff A, Siswantoro H, Kenangalem E, Maristela R, Wuwung RM, Laihad F, Ebsworth EP, Anstey NM, Tjitra E, Price RN: Two fixed-dose artemisinin combinations for drug-resistant falciparum and vivax malaria in Papua, Indonesia: an open-label randomised comparison. Lancet. 2007, 369: 757-765. 10.1016/S0140-6736(07)60160-3.
Hutagalung R, Paiphun L, Ashley EA, McGready R, Brockman A, Thwai KL, Singhasivanon P, Jelinek T, White NJ, Nosten FH: A randomized trial of artemether/lumefantrine versus mefloquine-artesunate for the treatment of uncomplicated multi-drug resistant Plasmodium falciparum on the western border of Thailand. Malar J. 2005, 4: 46-10.1186/1475-2875-4-46.
Broek van den IV, Maung UA, Peters A, Liem L, Kamal M, Rahman M, Rahman MR, Bangali AM, Das S, Barends M, Faiz AM: Efficacy of chloroquine + sulfadoxine-pyrimethamine, mefloquine + artesunate and artemether + lumefantrine combination therapies to treat Plasmodium falciparum malaria in the Chittagong Hill Tracts, Bangladesh. Trans R Soc Trop Med Hyg. 2005, 99: 727-735. 10.1016/j.trstmh.2005.02.007.
Thapa S, Hollander J, Linehan M, Cox-Singh J, Bista MB, Thakur GD, Davis WA, Davis TM: Comparison of artemether/lumefantrine with sulfadoxine-pyrimethamine for the treatment of uncomplicated falciparum malaria in Eastern Nepal. Am J Trop Med Hyg. 2007, 77: 423-430.
Mueller EA, van Vugt M, Kirch W, Andriano K, Hunt P, de Palacios PI: Efficacy and safety of the six-dose regimen of artemether-lumefantrine for treatment of uncomplicated Plasmodium falciparum malaria in adolescents and adults: a pooled analysis of individual patient data from randomized clinical trials. Acta Tropica. 2006, 100: 41-53. 10.1016/j.actatropica.2006.09.007.
Makanga M, Premji Z, Falade C, Karbwang J, Mueller EA, Andriano K, Hunt P, De Palacios PI: Efficacy and safety of the six-dose regimen of artemether-lumefantrine in pediatrics with uncomplicated Plasmodium falciparum malaria: a pooled analysis of individual patient data. Am J Trop Med Hyg. 2006, 74: 991-998.
Panossian LA, Garga NI, Pelletier D: Toxic Brainstem Encephalopathy after Artemisinin Treatment for Breast Cancer. Ann Neurol. 2005, 58: 812-813. 10.1002/ana.20620.
Miller LG, Panosian CB: Ataxia and slurred speech after artesunate treatment for falciparum malaria. N Eng J Med. 1997, 336: 1328-10.1056/NEJM199705013361818.
Franco-Paredes C, Dismukes R, Nicolls D, Kozarsky PE: Neurotoxicity due to antimalarials therapy associated with misdiagnosis of malaria. Clin Infect Dis. 2005, 40: 1710-1711. 10.1086/430180.
White NJ, Ashley EA, Nosten F: Toxic brainstem encephalopathy after artemisinin treatment for breast cancer. Ann Neurol. 2006, 59: 725-726. 10.1002/ana.20815.
Davis TME, Edwards GO, McCarthy JS: Artesunate and cerebellar dysfunction in falciparum malaria. N Engl J Med. 1997, 337: 792-793. 10.1056/NEJM199709113371116.
Newton PN, Day PJ, White NJ: Misattribution of Central Nervous System Dysfunction to Artesunate. Clin Infect Dis. 2005, 41: 1687-1688. 10.1086/498033.
Kissinger E, Hien TT, Hung NT, ND Nam ND, Tuyen NL, Dinh BV, Mann C, Phu NH, Loc PP, Simpson JA, White NJ, Farrar J: Clinical and neurophysiological study of the effects of multiple doses of artemisinin on brain-stem function in Vietnamese patients. Am J Trop Med Hyg. 2000, 63: 48-55.
van Vugt M, Angus BJ, Price RN, Mann C, Simpson JA, Poletto C, Htoo SE, Looareesuwan S, White NJ, Nosten F: A case-control auditory evaluation of patients treated with artemisinin derivatives for multidrug-resistant Plasmodium falciparum malaria. Am J Trop Med Hyg. 2000, 62: 65-69.
Hutagalung R, Paiphun L, Ashley EA, McGready R, Brockman A, Thwai KL, Singhasivanon P, Jelinek T, White NJ, Nosten FH: A randomized trial of artemether-lumefantrine versus mefloquine-artesunate for the treatment of uncomplicated multi-drug resistant Plasmodium falciparum on the western border of Thailand. Malar J. 2005, 4: 46-51. 10.1186/1475-2875-4-46.
McCall MBB, Beynon AJ, Mylanus EAM, Ven van der AJ, Sauerwein RW: No hearing loss associated with the use of artemether-lumefantrine to treat experimental human malaria. Trans R Soc Trop Med Hyg. 2006, 100: 1098-1104. 10.1016/j.trstmh.2006.02.017.
Cousin M, Kummerer S, Lefèvre G, Marrast AC, Stein D, Weaver M: Advisory Committee Briefing Book. Coartem® (artemether/lumefantrine) Tablets for the treatment of malaria in patients with acute, uncomplicated infections due to Plasmodium falciparum or mixed infections including P. falciparum. NDA 22-268. 2008, [http://www.fda.gov/ohrms/dockets/ac/08/briefing/2008-4388b1-02-Novartis.pdf]
White NJ: Cardiotoxicity of antimalarial drugs. Lancet Infect Dis. 2007, 7: 549-558. 10.1016/S1473-3099(07)70187-1.
Bakshi R, Hermeling-Fritz I, Gathmann I, Alteri E: An integrated assessment of the clinical safety of artemether-lumefantrine: a new oral fixed-dose combination antimalarial drug. Trans R Soc Trop Med Hyg. 2000, 94: 419-424. 10.1016/S0035-9203(00)90126-3.
Adjei GO, Kurtzhals JAL, Rodrigues OP, Alifrangis M, Hoegberg LCG, Kitcher ED, Badoe EV, Lamptey R, Goka BQ: Amodiaquine-artesunate vs artemether-lumefantrine for uncomplicated malaria in Ghanaian children: a randomized efficacy and safety trial with one year follow-up. Malar J. 2008, 7: 127-138. 10.1186/1475-2875-7-127.
Maiteki-Sebuguzi C, Jagannathan P, Yau VM, Clark TD, Njama-Meya D, Nzarubara B, Talisuna AO, Kamya MR, Rosenthal PJ, Dorsey G, Staedke SG: Safety and tolerability of combination antimalarial therapies for uncomplicated falciparum malaria in Ugandan children. Malar J. 2008, 7: 106-117. 10.1186/1475-2875-7-106.
McGready R, Cho T, Keo NK, Thwai KL, Villegas L, Looareesuwan S, White NJ, Nosten F: Artemisinin antimalarial in pregnancy: a prospective treatment study of 539 episodes of multidrug-resistant Plasmodium falciparum. Clin Infect Dis. 2001, 33: 2009-2016. 10.1086/324349.
Manyando C, Mkandawire R, Puma L, Sinkala M, Njunju E, Gomes M, Andriano K, Schlienger R, Virtanen M: Safety profile of artemether-lumefantrine (AL; Coartem®) compared with sulfadoxine-pyrimethamine (SP) in pregnant women with symptomatic malaria: preliminary results of an observational study. Abstract 570, 57th Meeting of the American Society of Tropical Medicine and Hygiene (ASTMH), New Orleans, Louisiana, USA. 2008
Acknowledgements
The authors would like to thank PreScript Communications, who provided editorial assistance with funding from Novartis Pharma AG.
This article is part of Malaria Journal Volume 8 Supplement 1: Coartem®: reviewing the impact on the malaria landscape. The full contents of the supplement are available online at http://www.malariajournal.com/supplements/8/S1. Publication of the supplement has been sponsored by Novartis Pharma AG.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors would like to acknowledge that Novartis Pharma AG sponsored this supplement. However, none of the authors works for, or represents in any way, Novartis Pharma AG.
Authors' contributions
All authors met International Committee of Medical Journal Editors criteria for authorship.
Catherine Falade and Christine Manyando contributed equally to this work.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Falade, C., Manyando, C. Safety profile of Coartem®: the evidence base. Malar J 8 (Suppl 1), S6 (2009). https://doi.org/10.1186/1475-2875-8-S1-S6
Published:
DOI: https://doi.org/10.1186/1475-2875-8-S1-S6