
Abstract
In the high malaria-transmission settings of sub-Saharan Africa, malaria in pregnancy is an important cause of maternal, perinatal and neonatal morbidity. Intermittent preventive treatment of malaria in pregnancy (IPTp) with sulphadoxine-pyrimethamine (SP) reduces the incidence of low birth-weight, pre-term delivery, intrauterine growth-retardation and maternal anaemia. However, the public health benefits of IPTp are declining due to SP resistance. The combination of azithromycin and chloroquine is a potential alternative to SP for IPTp. This review summarizes key in vitro and in vivo evidence of azithromycin and chloroquine activity against Plasmodium falciparum and Plasmodium vivax, as well as the anticipated secondary benefits that may result from their combined use in IPTp, including the cure and prevention of many sexually transmitted diseases. Drug costs and the necessity for external financing are discussed along with a range of issues related to drug resistance and surveillance. Several scientific and programmatic questions of interest to policymakers and programme managers are also presented that would need to be addressed before azithromycin-chloroquine could be adopted for use in IPTp.
Similar content being viewed by others


Background
Each year, 30 million pregnancies are at risk of malaria infection in sub-Saharan Africa, representing a major public health problem. Malaria in pregnancy (MIP) is associated with low birth-weight (LBW) [1–3], pre-term delivery [4] intrauterine growth-retardation [4, 5], and maternal anaemia [6]. LBW is a strong predictor of infant mortality in sub-Saharan Africa; death within the first year of life is three-times higher for LBW newborns compared to neonates of normal birth-weight [7]. Malaria is one of the few contributors to LBW that can be improved by specific interventions [8]. Thus, to reduce the effects of MIP in endemic areas, the World Health Organization (WHO) recommends use of Intermittent Preventive Treatment of Malaria in Pregnancy (IPTp) with sulphadoxine-pyrimethamine (SP).
IPTp has two primary objectives: (1) to clear asymptomatic peripheral and placental parasitaemia and (2) to provide intermittent chemoprophylaxis against malaria infection during pregnancy. The WHO recommends administration of two or three courses of SP, sulphadoxine (500 mg) and pyrimethamine (25 mg), after foetal quickening with each course given no less than one month apart, and all prior to the last month of pregnancy [9]. Anti-malarial chemoprophylaxis among paucigravidae increases birth-weight by an average of 127 g (95% CI 88.64 to 164.75 g) and reduces, by nearly half, the incidence of LBW (RR = 0.57, 95% CI 0.46 to 0.72) [10]. It has been estimated that universal coverage with IPTp would reduce all-cause neonatal mortality by 32% (95% CI -1 to 54%) [11].
Standard IPTp dosing does not provide the same degree of protective efficacy for pregnant women who are HIV-positive. This can be overcome, however, by administering more frequent courses of SP throughout pregnancy. A study in Malawi compared monthly SP treatment versus two courses during the antenatal period among HIV-positive and HIV-negative women. An estimated 7.8% of HIV-positive pregnant women had placental malaria after receiving monthly SP as compared to 21.5% of HIV-positive women who received two doses of SP (RR, 0.36 [95% CI, 0.17–0.79]). Among HIV-negative women, 2.3% who received monthly SP had placental parasitaemia in contrast to 6.3% of HIV-negative women who received two-dose SP (RR, 0.37 [95% CI, 0.11–1.19]) [8].
The benefits of IPTp are threatened by increasing resistance of Plasmodium falciparum to SP. In many countries, artemisinin combination therapy (ACT) has replaced SP for case management, according to WHO guidelines, because SP now demonstrates inadequate therapeutic efficacy in children [12]. Therapeutic efficacy of SP in children with clinical cases of P. falciparum malaria does not, however, predict efficacy of IPTp. Correlation analysis between paediatric treatment and IPTp suggests that SP may still offer some protection against MIP in geographic areas where day 14 post-treatment failure rates for SP in children are as high as 40% [13]. This protection, however, is not uniform across populations; primigravidae are particularly vulnerable to the effects of MIP and are protected the least by SP where sensitivity is on the decline. In Ghana, where parasite sensitivity to SP remains higher than in east and southern Africa, uncorrected parasitological failure rates by day 28 post-treatment were 36.4% (32 of 88) in children, 27.1% (29 of 107) in primigravidae, 6.1% (3 of 49) in secundigravidae, and 3.8% (2 of 52) in multigravidae [14]. Thus, SP is already compromised and an urgent need exists to identify alternative compounds for use in IPTp, even though SP still offers some protection up to an unknown threshold of parasite resistance.
An ideal anti-malarial drug or drug combination for IPTp should be safe, well tolerated, efficacious in the clearance of malaria parasites, provide a long period of chemoprotection and, preferably, not be deployed as the first-line treatment for clinical malaria. If a drug or drug combination used in IPTp is not simultaneously used for clinical malaria case management, then IPTp may actually lower the selection pressure on the first-line drug by decreasing symptomatic cases that require treatment. This is particularly important as countries increasingly treat pregnant women with uncomplicated clinical malaria in second- and third-trimesters with ACTs.
Several published reviews of drugs for IPTp have included azithromycin and chloroquine, although only as monotherapies [15–18]. This review summarizes in vitro and in vivo evidence for the therapeutic efficacy of azithromycin and chloroquine when used alone or together and discusses the additional benefits that the combination could have on many sexually transmitted diseases and, possibly, pneumococcal infection during pregnancy. Drug costs are presented along with issues related to drug resistance and surveillance. Several scientific and programmatic areas are outlined, as well, that would need to be addressed for policymakers and programme managers before azithromycin-chloroquine could be adopted for use in IPTp.
Azithromycin monotherapy for treatment and prevention of malaria
Pharmacokinetics
Azithromycin is a slow-acting anti-malarial macrolide [19], an analogue of erythromycin with a nitrogen atom inserted into the macrolide nucleus. As a result, there is enhanced penetration of drug into macrophages, fibroblasts and polymorphonuclear neutrophils, permitting greater accumulation within acidified vacuoles and extending the 1.5-hour half-life of erythromycin to 68 hours for azithromycin [20]. Stable at gastric pH, azithromycin has an absolute bioavailability of 37% following oral administration [21]. It accumulates in hepatic, renal, pulmonary and splenic tissue [22], and gradually leaches into the bloodstream over a period of one week [23]. Mild renal dysfunction and mild-to-moderate hepatic dysfunction do not affect excretion significantly.
Among pregnant women, serum concentrations peak within six hours of oral administration and are sustained for 24 hours. As the drug disperses, peak concentrations are maintained three-times longer in the placenta, myometrial and adipose tissues [24]; only 2.6% of a maternal dose, however, perfuses the placenta [25]. Azithromycin is excreted in human milk with no adverse events observed as a consequence [26].
Azithromycin targets the 70 S ribosomal subunit of the apical complex of susceptible micro-organisms including P. falciparum and P. vivax [23]. Once attached to the apicoplasts of the parasite, azithromycin hinders polypeptide development, triggering premature detachment and movement down the peptide exit tunnel. The potency of azithromycin, as a translation inhibitor, is greatest against the progeny of parasites that inherit a non-functioning apicoplast following drug exposure, thus creating a delayed-death effect [27–29]. Laboratory-generated P. falciparum that are resistant to azithromycin appear to accumulate mutations after in vitro passage in the structural proteins of the ribosome [23]. It is unknown whether mutations induced by azithromycin are capable of undermining the inhibitory action of other drugs that also target the apicoplast.
Safety and tolerability
Doses of azithromycin between 500 mg and 2,000 mg have been used in all trimesters of human pregnancy for the treatment of upper and lower respiratory tract infections, skin diseases, Chlamydia trachomatis, mycoplasma and group B streptococci infections among women allergic to other antibiotics.
Meta-analysis of eight randomized clinical trials among pregnant women with C. trachomatis infection found that azithromycin was associated with fewer gastrointestinal adverse events than erythromycin (OR = 0.11, 95% CI 0.07–0.18) and fewer total adverse events (OR = 0.11, 95% CI 0.07–0.18) [30]. A placebo-controlled trial, however, suggests that azithromycin may be poorly tolerated by HIV-positive patients. Gastrointestinal effects were reported by 78.9% of azithromycin recipients (67 of 85) and 27.5% of participants given placebo (24 of 89) [31]. Although an unusual side-effect, case reports indicate that HIV-positive patients may experience temporary ototoxicity with azithromycin use [32].
Adults treated with a 1,000 mg oral dose of azithromycin report moderate side-effects including diarrhoea or loose stools (7%), nausea (5%), vomiting (2%), and vaginitis (2%); up to 1% of adults experience dizziness, headache, vertigo, and somnolence [33]. There is no evidence of teratogenicity in animal models, even at four-times the human treatment dose [34–36].
Efficacy
The in vitro anti-malarial activity of azithromycin increases 200-fold against P. falciparum isolates when incubated between 24 and 48 hours, while its 50% inhibitory concentration values drop as low as 35 nanomolar [37]. At 48-hours, azithromycin is 10-fold more active than erythromycin against chloroquine-resistant P. falciparum; the two compounds are equipotent, however, when chloroquine-sensitive parasites are exposed to the same drug concentration [38, 39].
Daily regimens of 250 mg with a loading dose of 500 or 750 mg have shown an impressive chemoprophylactic effect against P. vivax. Azithromycin had a 99% protective effect (95% CI, 93% to 100%) among semi-immune subjects in Indonesia over a 20-week period [40]. A similar protective efficacy, 98% (95% CI, 88% to 100%), was seen in Thailand [41] in a semi-immune population. By comparison, the chemoprophylactic effect of azithromycin against P. falciparum has shown promise, but has been less impressive (Table 1).
The first published P. falciparum human challenge study with azithromycin involved four non-immune volunteers who received a loading dose of 500 mg and 250 mg daily for three days. Subjects were then inoculated with five Anopheles stephensi mosquitoes that had an average of 3.2 salivary-gland P. falciparum sporozoites each, after which they continued to receive 250 mg of azithromycin daily for four more days. With unquantifiable plasma concentrations of azithromycin, presumably due to poor absorption, one of four subjects developed parasitaemia in the 14-day post-challenge period [42].
A subsequent trial suggested that a regimen of longer duration might be required against P. falciparum. Ten non-immune subjects were given a loading dose of 500 mg followed by 250 mg daily for 2 weeks prior to parasite exposure. After inoculation, 250 mg was administered daily for one additional week, producing a protective effect of 40% (95% CI, 12% to 74%). A concurrent human challenge study with 10 non-immune subjects was conducted using the same regimen, except that 250 mg was given daily for two weeks post-exposure, rather than for just one, producing a 100% protective effect [43]. This high level of protection has not been replicated in the field, however, where multiple infections may be expected.
Among semi-immune populations, an equivalent or higher loading dose with the same daily regimen resulted in protective efficacies of 83% (95% CI, 69% to 91%) in Kenya [44], 71% (95% CI, -14% to 94%) in Thailand [41], and 72% (95% CI, 50% to 84%) in Indonesia [40]. There were two sub-populations in the Indonesian study which may have had slightly different degrees of acquired immunity: the chemoprophylactic effect among soldiers living for six months in the study area was 62.9% (95% CI, 29.5 to 80.4) while chemoprophylactic protection among civilians residing in the study area for less-than 18 months was 88.4 (95% CI, 56.6 to 97.4). The Kenyan trial also evaluated weekly dosing with 1,000 mg of azithromycin, in contrast to a daily regimen of 250 mg, producing just 64% protective efficacy (95% CI, 47% to 77%) [44]. Despite relatively poor in vivo protection against P. falciparum in field settings, the favourable safety profile of azithromycin in pregnant women and young children prompted further investigation into molecules that might be co-administered with azithromycin to improve its protective effect.
Chloroquine as monotherapy for the treatment and prevention of malaria
Pharmacokinetics
Chloroquine has been the first-line treatment of malaria in much of the world for most of the past 60 years. Absolute bioavailability is 70 to 75% while peak plasma concentrations are reached within two hours of oral administration. A single therapeutic dose against a chloroquine-resistant strain will persist six to 10 days in the blood, while its overall half-life is between one and two months [45, 46]. Chloroquine accumulates extensively in the liver, connective tissue and pigmented tissue such as skin and retina, enabling enormous total volume distribution. Greatest concentrations are found in erythrocytes, granulocytes and platelets, and 55% is protein-bound in plasma.
Chloroquine is active against erythrocytic life stages of Plasmodium species when haemoglobin is being actively digested. Haem is a toxic bi-product of haemoglobin ingestion and must be eliminated through dimerization. Under normal circumstances, parasites bio-crystallize haem to form haemozoin, the iron-containing pigment that accumulates as non-toxic cytoplasmic granules. Chloroquine prevents this process by concentrating at nanomolar levels outside parasites (10-9) and one million times higher (10-3) in parasite food vacuoles of infected erythrocytes [47]. Inside parasite vacuoles, chloroquine binds to haem, preventing its expulsion. Thus, the more haemoglobin ingested by parasites, the more toxic their food vacuoles become, rapidly causing cell death. Resistance to chloroquine is associated with polymorphisms in the P. falciparum food vacuole transporter protein (pfcrt) located on chromosome 7 [48]. All pfcrt alleles from chloroquine-resistant strains, regardless of geographic origin, encode a conserved K76T amino acid substitution. The effect of pfcrt on chloroquine pharmacokinetics remains disputed. Some researchers have theorized that pfcrt enables protonated chloroquine to escape the food vacuole while others argue pfcrt binds directly to chloroquine, thereby inhibiting its ability to alter food vacuole pH [49].
Safety and tolerability
Chloroquine is safe and generally well tolerated in treatment doses. Due to its rapid absorption, chloroquine has a narrow therapeutic index, increasing the potential for toxic overdose. Hypotension and cardiac failure can be prompted by a single oral dose of 3500 mg [50]. Despite toxicity at high doses, the most commonly reported side-effect in African populations is pruritus which peaks 24 hours after intake [51]. Chloroquine has been used safely in all trimesters of human pregnancy for decades as both a treatment and chemoprophylactic drug, crossing the placenta without teratogenic effect [52].
Prior to establishment of IPTp in sub-Saharan Africa, chloroquine was commonly given to pregnant women during antenatal visits in sachets containing four weekly doses of 300 mg for self-administration. Compliance with chloroquine remained low for many reasons including pruritus and its bitter taste which some women associate with medications that induce abortion [53, 54].
Efficacy
Although still a first-line treatment for P. vivax, chloroquine is no longer recommended for treatment of P. falciparum due to high levels of resistance. In combination with another anti-malarial drug, however, chloroquine might, once again, have a role in malaria control. Malawi changed its first-line drug to SP in 1993 when chloroquine in vivo failure rates were as high as 58% [55]. Five years later, chloroquine inhibited in vitro blood schizont development in 96.5% (28 of 29) of isolates from Malawi [56], indicating that pfcrt was no longer under selection pressure. In 2001, field sampling failed to find parasites carrying the pfcrt mutation associated with resistance [57] and a clinical trial using chloroquine monotherapy was 100% efficacious (63 of 63) among asymptomatic semi-immune adults who received 600 mg on day 0 and day 1, and 300 mg on day 2 [58]. Most recently, a study in 2005 showed chloroquine to clear parasite infection in 98.8% (79 of 80) of Malawi children with uncomplicated P. falciparum malaria [59].
The re-emergence of high in vitro sensitivity to chloroquine in Malawi – within just five years – suggests the pfcrt resistance mutation involves considerable fitness cost to P. falciparum [60–62]. This micro-evolutionary reversal is all the more remarkable because it occurred despite the continued availability of chloroquine in the formal and informal private sector. It is likely that P. falciparum sensitivity will return elsewhere in the region, if it has not already, with the declining chloroquine use.
Chloroquine monotherapy continues to demonstrate modest therapeutic utility in west Africa. A recent observational study in Benin examined the effect of self-administered chloroquine chemoprophylaxis among pregnant women (N = 1090), comparing self-reported dosing over pregnancy with birth weights. An estimated 49.9% of women reported taking weekly chloroquine in the first trimester, increasing to 92% of women in the second trimester and 97.5% in the final trimester. Random testing of urine samples at delivery established a point-prevalence for chloroquine use. In total, an estimated 99% of women had ingested chloroquine (N = 166); of these, 72% had levels consistent with consuming 300 mg in the previous seven days. Subjects with self-reported chemoprophylactic use for seven or more months were four times more likely to give birth to child of normal birth weight (> 2500 grams) than women who used chemoprophylaxis for less than four months (adjusted OR = 3.96; 95% CI = 1.9 to 8.28; p =< 0.001) [63].
Parasitological evidence of chloroquine efficacy was reported, as well, in a recent four-arm clinical trial conducted in Ghana among pregnant women with asexual P falciparum stage parasitaemia. Women randomized to a chloroquine treatment group (N = 225) received 600 mg for 2 days and 300 mg on the third day. The uncorrected day-28 treatment failure rate was 30% (62 of 208). Polymerase chain reaction (PCR) analysis confirmed that 14% (30 of 208) were treatment failures while 6% (11 of 208) were re-infections. PCR was unable to distinguish cases of recrudescence from new infection in the remaining 10% (21 of 208) [64].
Potential for azithromycin and chloroquine when used in combination for the prevention of malaria
Evidence for synergy of the combination in vitro
An additive effect between azithromycin and chloroquine has been shown in sensitivity testing conducted over a 48-hour period. When incubation is extended to 68 hours, drug synergy has been seen against chloroquine-resistant isolates; the combination remains additive, however, against chloroquine-sensitive parasites [65]. Sidhu et al in contrast, observed an additive effect at 96 hours of incubation against chloroquine-resistant isolates [23].
Azithromycin and chloroquine do not exhibit any clinically relevant pharmacokinetic interactions [66], although chloroquine resistance is reversible with calcium channel blockers, such as verapamil and desipramine, that inhibit p-glycoprotein-mediated efflux [67, 68]. Azithromycin is a p-glycoprotein substrate [69] which may suggest the presence of a metabolic mechanism for synergy. Whether additive or synergistic, complete parasitological clearance using the combination would not be expected in less than 48 hours, the equivalent of two schizogenesis cycles. Thus, a conservative approach to in vivo dosing may require a three-day regimen to realize the full benefits of the azithromycin-chloroquine combination against P. falciparum while minimizing the opportunity for survival of wild-type progeny.
Evidence for synergy of the combination in vivo
A two-stage trial in India demonstrated in vivo synergy between azithromycin and chloroquine against P. falciparum infection. The first stage, which was double-blinded, included 32 semi-immune subjects treated for uncomplicated P. falciparum malaria with either azithromycin (1,000 mg) plus chloroquine placebo on days 0, 1 and 2, or chloroquine (600 mg) on days 0, 1 and 300 mg on day 2 plus azithromycin placebo on days 0, 1 and 2. The second stage of the trial was open label and included 64 semi-immune subjects who received the azithromycin-chloroquine combination therapy in doses equal to stage one. Treatment response rates at day 28 showed in vivo synergy: 33% of those who received azithromycin monotherapy remained free of fever by day 28 compared to 27% in the chloroquine-treatment group. In contrast, 97% of patients who received drugs co-administered had resolved fever and parasitaemia by day 7 with no observed recrudescence by day 28. Parasitological responses by treatment group mirrored the synergy of clinical observations. Azithromycin monotherapy eradicated parasites in 19% of subjects (3 of 16) by day 3, increasing to 63% of subjects (10 of 16) by day 7, and dropping to 36% at day 28. As would be expected, chloroquine monotherapy was faster-acting than azithromycin alone, but it also demonstrated an increase in failures by day 28. Specifically, 56% of subjects (9 of 16) were free of parasites at day 3, followed by 88% (14 of 16) at day 7 and, finally, 27% (4 of 15) by day 28. For subjects receiving azithromycin-chloroquine combination treatment, however, 97% parasitological eradication was achieved by day 3 and sustained through day 7 and day 28 [70].
Treatment trials with the azithromycin-chloroquine combination in Africa
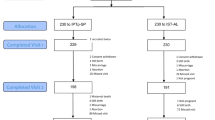
A double-blinded multi-centre trial was held in Burkina Faso, Ghana Mali, Kenya, Uganda, and Zambia to compare the therapeutic efficacy and tolerability of azithromycin-chloroquine with that of mefloquine [71]; a second, open-label, confirmatory trial was conducted in the same countries, with the addition of Senegal [72]. Together, these studies established an efficacious treatment course for azithromycin-chloroquine against uncomplicated P. falciparum infection: a fixed daily dose of 1,000 mg of azithromycin and 600 mg of chloroquine taken for three days. This treatment regimen represents a slightly higher dose of chloroquine than has been commonly administered. Most often, 25 mg of chloroquine is provided per kg of body weight over a three-day period: 10 mg per kg on days 1 and 2 with 5 mg per kg on day 3. The azithromycin-chloroquine fixed dose contains a total of 1,800 mg of chloroquine, an amount that would typically be given to a person weighing 72 kg. The average weight of pregnant women in the Ghana efficacy study [64] was 55.9 kilograms. Thus, 600 mg per day over three days is 22.4% more chloroquine than is in the typical treatment course.
Mefloquine was an appropriate comparator in these sub-Saharan studies because it has not been used regularly in the region and parasite sensitivity is likely quite high. Mefloquine is also a potential candidate to replace SP in IPTp. Preliminary results suggest that azithromycin-chloroquine is non-inferior to mefloquine with P. falciparum clearance rates comparable to those observed in India. The azithromycin-chloroquine combination warrants further investigation and may also offer particular advantages in settings where mixed infections of P. falciparum and P. vivax predominate.
The azithromycin-chloroquine combination for IPTp
Dosing
If azithromycin and chloroquine are used together in IPTp, then an initial priority should be to identify the most suitable dose of the combination. It seems likely that a three-day treatment regimen will be needed to ensure complete parasitological clearance while minimizing selection for resistant genotypes. Thus, as an initial investigation, it would be appropriate to give women two or three courses of IPTp during the antenatal period in a regimen of 1,000 mg of azithromycin plus 600 mg chloroquine base, once daily for three days. Because rates of drug absorption, distribution and excretion are commonly altered during pregnancy, pharmacokinetic investigations should be conducted as part of, or in parallel to, a clinical trial.
Acceptance and adherence
Acceptance of and adherence to a three-day regimen of azithromycin-chloroquine would be needed. In most operational settings, the first dose of azithromycin-chloroquine can be administered as directly observed therapy during antenatal visits, but doses on the following two days would require self-administration. Improvements in adherence to multi-day regimens have been shown for discrete treatment periods using pre-packaged sachets labeled with pictogram instructions that are explained during initial consultations [73–76]. Even so, achieving high rates of adherence to a three-day azithromycin-chloroquine regimen – administered two or three times during pregnancy – would likely be a challenge. Public education campaigns in recent years have discouraged chloroquine use. Thus, community acceptance, even in a new combination, would require innovative packaging and marketing. Adherence could be improved if a three-dose azithromycin-chloroquine fixed-dose formulation is designed specifically for IPTp. In countries currently implementing Home-based Management of Malaria and/or the community component of the Integrated Management of Childhood Illness, adherence to IPTp could be improved further with community health workers making house visits on days following antenatal consultations to verify self-treatment while taking the opportunity to develop or review an individualized perinatal plan in the home.
Azithromycin plus SP is another option for IPTp which would not present the disadvantage chloroquine-associated pruritus. However, SP may have surpassed a resistance threshold which would make it an ineffective partner drug. Alternatively, azithromycin could be combined with piperaquine to improve adherence; piperaquine is at least as effective as, and better tolerated than, chloroquine against P. falciparum and P. vivax [77]. Pyronaridine is another potential partner drug, shown to have additive properties with azithromycin [78]. Mefloquine, despite some important issues of tolerability, has the advantage that it can be administered as a single, observed dose.
Optimal timing
SP is contraindicated prior to quickening due to its teratogenic risk and, again, one month prior to delivery because of possible drug-induced kernicterus. Thus, providing IPTp with SP requires estimating gestational age and delivery date with some accuracy. In contrast, there are no known contraindications for azithromycin-chloroquine at any gestational age. This is important because current IPTp guidelines are currently based on operational convenience rather than the natural course of MIP [79]. Earlier IPTp administration may be important as maternal parasite densities peak between nine and 16 weeks [1, 3], tapering until term. IPTp administration in the last month of pregnancy may be of considerable value, too, increasing foetal weight gain during final stages of accelerated growth in utero [79].
Mefloquine may also be suitable for administration earlier and later in pregnancy than SP. Based, in part, on post-marketing surveys and retrospective studies which include 1271 first-trimester pregnancies, the US Centers for Disease Control and the UK Health Protection Agency recommend mefloquine chemoprophylaxis for pregnant women in any trimester when travelling to areas of high malaria transmission. Overall experience does not suggest that mefloquine is teratogenic [16, 80]. Administration in the first trimester, however, may warrant caution in light of two retrospective studies that found associations between mefloquine exposure and spontaneous abortion [81], and stillbirth [80].
ACTs are associated with embryotoxicity over a narrow dose range in animal models of early pregnancy with some additional evidence of lethality in second and third trimesters [82]. For this reason, the WHO recommends ACTs for curative purposes only during the second- and third-trimesters if other treatments have been considered unsuitable. First-trimester administration is contraindicated unless treatment is considered life-saving for the mother [83].
Potential additional benefits of azithromycin-chloroquine when used for IPTp
Use of the azithromycin-chloroquine combination in IPTp may offer several additional public health benefits over other possible replacements for SP.
Reduction of sexually transmitted infections
Sexually transmitted infections (STI) adversely affect pregnancy and contribute to pre-term delivery, LBW, intrauterine growth-retardation, spontaneous abortion, stillbirth, newborn morbidity and mortality [84]. Maternal health is also jeopardized by STIs with potential complications including pelvic inflammatory disease, ectopic pregnancy and infertility [85]. Prevalence estimates of symptomatic STIs at antenatal clinics in sub-Saharan Africa range between 2.5 and 17% for syphilis [86–91], 1.7 and 7% for Neisseria gonorrhoea [86–88, 91–96], 5.3 to 20.8% for C. trachomatis [86–88, 92–95, 97] and 7.3% to 62% for chancroid [98].
In resource-limited settings, testing women for STIs during antenatal consultations and providing appropriate care has been a public health challenge for decades. To assist countries, the WHO has developed syndromic-based algorithms for the detection of STIs. In high-transmission areas, the method is reliable for men, but much less so for women. Syndromic diagnosis of N. gonorrhoea and C. trachomatis among women has a sensitivity of 30 to 80% and a specificity of 40 to 80%; rarely does the sum of the two exceed 120% [99–102]. An additional shortcoming is that asymptomatic infection, a substantial portion of disease burden, remains undetected and, thus, untreated.
In South Africa's largest district, Hlabisa, 24.9% of females between 15 and 49 years of age are estimated to have at least one STI on any given day – Treponema pallidum, N. gonorrhoea, C. trachomatis, or Trichomonas vaginalis. While this prevalence may be higher than in some other parts of sub-Saharan Africa, of particular concern is that 48% of these infections are asymptomatic. In addition, just 2% of women with symptomatic STIs ever seek treatment in Hlabisa, and when they do, only 65% of them receive adequate care. Pregnant women are less likely to have asymptomatic STIs compared to non-pregnant women (17% vs. 59%), but the age-specific prevalence of infection is often twice as high for pregnant women [103]. This level of disease prevalence, symptomatic and asymptomatic, suggests a role for mass treatment during pregnancy.
The presumptive treatment of STIs in pregnancy improved maternal health and birth outcomes in a randomized clinical trial involving 4,033 pregnancies in Uganda [88]. Vaginal infections were significantly lower in women who received a one-time dose of azithromycin (1,000 mg), metronidazole (2,000 mg) and cefixime (400 mg) compared to women who received iron/folate and low-dose multivitamins. In the treatment group, the relative risk (RR) of T. vaginalis was 0.28 (95% CI, 0.18–0.49), the RR of bacterial vaginosis was 0.78 (95% CI, 0.69–0.87), and the RR of infant ophthalmia was 0.37 (95% CI, 0.20–0.70). The incidence of LBW was substantially reduced in the intervention group (RR, 0.68; 95% CI, 0.53–0.86) as was early neonatal mortality (25.4 per 1,000 live births), when compared to the control group (29.1 per 1,000 live births).
While difficult to attribute specific beneficial outcomes to each compound, azithromycin probably had a considerable effect. An oral dose of 1,000 mg of azithromycin clears more than 90% of cervical infections due to N. gonorrhoea and C. trachomatis [85]. The same dose will cure and provide chemoprophylaxis against chancroid and syphilis. Studies in Uganda [104] and Tanzania [105] have shown that azithromycin, 1,000 mg and 2,000 mg respectively, is equally effective as benzathine penicillin G in treating syphilis among non-pregnant adults. If untreated in pregnancy, one-third of women will develop congenital syphilis, carrying major risk for the foetus. One study in Tanzania found unscreened congenital syphilis associated with 51% of stillbirths, 24% of pre-term live births and 17% of adverse pregnancy events [90]. Another trial in Zambia implicated maternal syphilis in 42% of spontaneous abortions [106]. Despite the high cure rates observed in the clinical trials of Uganda and Tanzania, 1,000 mg and 2,000 mg of azithromycin given to five pregnant women with syphilis in China did not prevent trans-placental infection [107]. Thus, IPTp with azithromycin-chloroquine should not be viewed as a replacement for benzathine penicillin G in the prevention of congenital disease. However, azithromycin-chloroquine administered in IPTp may improve outcomes for the majority women whose syphilis infections, both symptomatic and asymptomatic, that are currently undiagnosed and untreated.
The extent to which the control of STIs can prevent the spread of HIV remains unknown. Observational studies associate treatment of ulcerative STIs with reductions in HIV transmission, particularly among men [108], and yet a systematic review of eight clinical trials failed to find the same relationship in seven of them [109]. It is possible that two or three IPTp treatments with azithromycin-chloroquine could offer women some protection against HIV infection in pregnancy, but the observable difference may be undetectable due to sample size limitations in most clinical trials, especially in areas with low HIV prevalence rates.
Chloroquine may offer its own protection against HIV transmission. Cord blood containing high levels of chloroquine has been associated with a reduced risk of mother-to-child transmission (MTCT) of HIV [110]. In addition, viral shedding in breast milk has been lowered among HIV-positive women who received three days of 600 mg chloroquine as an anti-malarial chemoprophylactic [111]. It is unknown whether this reduction in viral load is sufficient to prevent HIV transmission among mothers who choose to breastfeed.
Prevention of pneumococcal infection in pregnancy
Pneumonia is not a common focus of maternal health packages in most resource-limited settings because the incidence in pregnancy is not appreciably higher than in non-pregnant women [112]. Disease progression, however, is substantially more virulent during gestation [113–115]. There are old data from Ibadan, Nigeria, that suggest the incidence of pneumococcal meningitis may increase during pregnancy and puerperal period [116]. Facility records between 1958 and 1962 revealed that 86% (26 of 31) of women with pneumococcal meningitis were pregnant (15) or had recently delivered (11). By comparison, disproportionately fewer pregnant or early postpartum women, 22% (7 of 32) in total, were diagnosed with other types of meningitis. It is uncertain whether this enhanced risk in pregnancy occurs in other parts of Africa. If so, then it is conceivable that IPTp with azithromycin might provide some protection against this uncommon but very serious infection.
Cost
The cost of 1,800 mg of chloroquine (600 mg per day for three days) ranges between US $0.10 and $0.20, while 3,000 mg of azithromycin (1,000 mg per day for three days) is approximately US $6.80 [117]. Thus, an azithromycin-chloroquine IPTp regimen administered two or three times would cost between US $14.00 and $21.00 per pregnancy. This is prohibitively expensive for national malaria control programmes in most endemic countries in Africa. Thus, external funding would be required for widespread implementation of the combination in IPTp. This could take many forms: a direct donation from the pharmaceutical industry, and/or a financing mechanism modelled after the Global ACT Subsidy or the International Financing Facility for Immunization.
Azithromycin and selection for resistance
There are concerns that use of azithromycin-chloroquine for IPT could encourage the emergence and spread of resistance to a variety of organisms. Pathogens that need to be considered include malaria parasites, organisms causing STIs, and the pneumococcus.
Malaria parasites
Apart from clinical trials, azithromycin has never been used operationally for treatment or prevention of malaria. The susceptibility of azithromycin-chloroquine for selecting parasites resistant to azithromycin is, therefore, unknown. The declining use of chloroquine throughout sub-Saharan Africa is likely to lead to reversal of resistance as witnessed in Malawi where parasite sensitivity returned five years after suspending its use. It is possible the re-introduction of chloroquine with azithromycin as a partner drug may prevent re-selection of parasites carrying the pfcrt resistance mutation. However, rigorous surveillance would be needed to verify this assumption.
Organisms causing STIs
Azithromycin sensitivity patterns in high-income countries do not suggest that its use in IPTp would rapidly induce resistance in N. gonorrhoea or C. trachomatis. Sensitivity of the gonococcus remains relatively high, even in the presence of growing penicillin resistance. In the United States, minimum inhibitory concentrations (MICs) of azithromycin exposed to gonococcal isolates have increased modestly since 1992 when tracking began. In 2006, 0.2% (14 of 6,089) of isolates provided through a national network were resistant to azithromycin with a MIC > 2.0 μg/ml, representing a slight decrease from 0.6% (35 of 6,199) of isolates in 2005 [118]. In the case of C. trachomatis, the most recent meta-analysis of 12 trials involving 1,543 patients estimates cure rates to be 97% with a single 1,000 mg dose of azithromycin [119].
There is greater concern regarding syphilis. Azithromycin has been used, for example, since 1999 in San Francisco (USA) for chemoprophylactic (1,000 mg) and curative (2,000 mg) purposes against syphilis. By 2004, a mutation associated with T. pallidum resistance to macrolides at the A2058 position in the 23S rRNA gene was found in 56% blood samples from the main metropolitan sexual health centre. All isolates were from men who have sex with men, 31% of which were from HIV-infected men [120]. The rapid decline in sensitivity is likely attributable, in large part, to underlying erythromycin resistance which has been in general use for over 50 years. Erythromycin-resistant T. pallidum isolates with mutation at the A2058 position confer resistance to macrolide antibiotics and are associated with treatment failures [121, 122]. Indeed, a risk factor for being infected with azithromycin-resistant syphilis is having used azithromycin or other macrolides in the recent past [123, 124].
The potential for rapid induction of T. pallidum resistance in Africa is difficult to estimate since molecular analyses of the A2058 region have not been included in most syphilis studies of the region. In Madagascar, the mutation was not found in analysis of 103 T. pallidum isolates and no azithromycin treatment failures have been reported in country [123, 125]. Because neither macrolide has been deployed on any scale in focus countries of IPTp, azithromycin may be less vulnerable to rapid loss of sensitivity as has been witnessed in high-income countries.
The pneumococcus
Pneumococcal resistance to macrolides occurs by two primary mechanisms, each with distinct genetic markers: ribosomal methylation (ermB or ermA genes) and efflux pump mutation (mefA or mefE genes). Based on experience in mass treatment of trachoma with azithromycin, there is concern that use of the azithromycin-chloroquine combination for IPTp might increase the prevalence of azithromycin- and erythromycin-resistant pneumococci. Trachoma eradication campaigns using azithromycin among vulnerable groups of children in Australia and Nepal found that one-time treatment may select macrolide-resistant pneumococcal strains in the nasopharynx [126, 127] and conjunctiva [128]. Selection, however, was transient. In Australia, 98.7% (78 of 79) of nasopharyngeal pneumococcal isolates collected at baseline were sensitive to azithromycin, decreasing to 84.2% (32 of 38) between two to three weeks, and then 73% (27 of 37) at two months. By six months, 94.9% of isolates were sensitive to azithromycin [126]. One-year after a trachoma campaign in Nepal, 86% (50 of 57) of randomly collected isolates were positive for S. pneumoniae, and 100% (50 of 50) were azithromycin sensitive [129]. Selection of azithromycin-resistant strains, however, has not always followed trachoma treatment campaigns. Very high macrolide sensitivity of nasopharyngeal pneumococci was observed in Tanzania when samples were obtained at three weeks, two months and six months post-treatment. Of 4,782 pneumococcal swabs tested, only one demonstrated pneumococcal resistance to azithromycin. Curiously, the resistant sample was collected at six months, not earlier, as might be expected with a treatment-induced mutation [130].
Ways to reduce opportunity for resistance
A number of steps could be taken to reduce the chances that azithromycin use in IPT might enhance macrolide resistance in bacteria responsible for several major infections. Considerations include the following:
Setting dose and duration above resistance breakpoint
A counter-selective dose – the minimum dosage necessary to prevent the emergence of drug resistance – can be used instead of the conventional minimum required dose to achieve adequate clinical and parasitological cure. Such a dose, set just above the resistance breakpoint of target micro-organisms, would suppress most pathogens during initial drug exposure and sustain concentrations sufficient to inhibit mutant progeny that might survive and select for resistance. Breakpoints and a counter-selective dose for azithromycin-chloroquine can be modelled using pharmacokinetic and pharmacodynamic parameters in IPTp target countries. While there will always be the potential for inducing resistance, a multi-national, multi-centre surveillance study over 10 years has shown that treatment of respiratory tract infections to the point of bacterial eradication minimizes potential for selecting and maintaining resistant strains [131].
Limiting availability
If azithromycin-chloroquine is limited to IPT, made available only through health facilities, and not simultaneously used for treatment purposes, then drug pressure can be kept to a minimum.
Monitoring sensitivity of pneumococci
Coordinated resistance surveillance of pneumococci should become a regional objective if countries choose to adopt azithromycin-chloroquine for IPT. Regional networks already exist for monitoring malaria and pneumococcal resistance, and could collaborate on this objective. Monitoring, however, can be a source of controversy as the relevance of in vitro macrolide sensitivity to clinical outcomes is not well established. There has not been a concomitant rise in S. pneumoniae case-mortality rates as increasing macrolide resistance has been observed in vitro [132]. A similar paradox has been seen with penicillin-resistant S. pneumoniae [133, 134]. Multiple reasons may contribute to these discordant trends. In the case of newer macrolides, including azithromycin, drug concentrations are able to reach higher levels in the intracellular tissue and in the epithelial lining fluid of the lung than concentrations measured in blood [135, 136]. Azithromycin, therefore, may have superior pharmacokinetics in vivo to inhibit S. pneumoniae infection, safeguarding favourable treatment outcomes in the face of increasing macrolide resistance as measured in vitro. However, macrolide efflux pump mutations have been identified in S. pneumoniae isolates with erythromycin MICs of at least 8 μg/mL – concentrations of azithromycin that have been associated with clinical failures [137]. The in vitro-in vivo paradox may be better understood with improved surveillance that involves analysis of in vitro MICs and in vivo treatment outcomes that include morbidity markers – not just morbidity rates – which may be more sensitive in detecting the effect of in vitro changes in macrolide resistance on clinical outcomes [134].
Key scientific and programmatic questions
Evidence to date suggests that azithromycin-chloroquine is a potential alternative for SP for IPTp and its evaluation in clinical trials is warranted. Several scientific and programmatic questions need to be addressed, however, so that policymakers and programme managers are able to consider the merits of azithromycin-chloroquine in IPTp. Key questions include:
-
1)
Is azithromycin-chloroquine superior to SP and other candidate replacements for IPTp in reducing LBW, maternal anaemia and parasite clearance?
-
2)
How much of the IPTp effect on birth weight, using azithromycin-chloroquine, may be due to a reduction in STIs, and what might be the savings, human and financial, due to reduced STIs in pregnancy that could result?
-
3)
Might administration of azithromycin-chloroquine prior to quickening and within the last month of gestation – periods contraindicated with SP – have additional effect on LBW, maternal anaemia and parasite clearance?
-
4)
Would the use of azithromycin-chloroquine for IPTp result in more than transient changes in the sensitivity of pneumococci to macrolides and penicillin?
-
5)
How might countries monitor the effect of azithromycin-chloroquine on the sensitivity of pneumococci to macrolides?
-
6)
What is the counter-selective dose for azithromycin-chloroquine against malaria parasites, organisms causing STIs, and pneumococci?
-
7)
How would pregnant women respond to receiving azithromycin-chloroquine and adhere to a regimen that requires partial self-administration, particularly as information campaigns have discouraged chloroquine use in recent years?
-
8)
Might IPTp with azithromycin-chloroquine reduce maternal acquisition of HIV during pregnancy, in utero MTCT or post-partum transmission among sero-positive women who choose to breastfeed?
Conclusion
Azithromycin-chloroquine is a potential alternative to SP for use in IPTp. The combination has demonstrated synergism in vivo against P. falciparum in India. Preliminary results of studies in non-pregnant adults in sub-Saharan Africa have shown that azithromycin-chloroquine is not inferior to mefloquine, a compound currently under consideration for IPTp. The azithromycin-chloroquine combination may be safely administered at any time in pregnancy. The secondary benefits of the combination, clearing of symptomatic and asymptomatic STIs, may be as important to maternal, foetal and neonatal health as the clearance and prevention of malaria. Innovative pricing mechanisms would be required to introduce azithromycin-chloroquine for IPTp since the drug cost per pregnancy would otherwise be US $14.00 to $21.00 for two or three courses. Close monitoring of antibiotic resistance markers would need to be an essential part of any IPTp programme using azithromycin-chloroquine.
References
Brabin B: An analysis of malaria in pregnancy in Africa. Bulletin of the World Health Organization. 1983, 61: 1005-1016.
McGregor IA: Epidemiology, malaria and pregnancy. Am J Trop Med Hyg. 1984, 33 (4): 517-525.
Brabin B: The Risks and Severity of Malaria in Pregnant Women. Applied Field Research in Malaria Reports. vol. TDR/FIELDMAL/1. 1991, Geneva: Special Programme for Research and Training in Tropical Diseases. World Health Organization
McGregor IA, Wilson ME, Billewicz WZ: Malaria infection of the placenta in The Gambia, West Africa; its incidence and relationship to stillbirth, birthweight and placental weight. Trans R Soc Trop Med Hyg. 1983, 77 (2): 232-244. 10.1016/0035-9203(83)90081-0.
Fried M, Muga RO, Misore AO, Duffy PE: Malaria elicits type 1 cytokines in the human placenta: IFN-gamma and TNF-alpha associated with pregnancy outcomes. J Immunol. 1998, 160 (5): 2523-2530.
Gilles HM, Lawson JB, Sibelas M, Voller A, Allan N: Malaria, anaemia and pregnancy. Ann Trop Med Parasitol. 1969, 63 (2): 245-263.
Guyatt HL, Snow RW: Malaria in pregnancy as an indirect cause of infant mortality in sub-Saharan Africa. Trans R Soc Trop Med Hyg. 2001, 95 (6): 569-576. 10.1016/S0035-9203(01)90082-3.
Filler SJ, Kazembe P, Thigpen M, Macheso A, Parise ME, Newman RD, Steketee RW, Hamel M: Randomized trial of 2-dose versus monthly sulfadoxine-pyrimethamine intermittent preventive treatment for malaria in HIV-positive and HIV-negative pregnant women in Malawi. J Infect Dis. 2006, 194 (3): 286-293. 10.1086/505080.
WHO: A Strategic Framework for Malaria Prevention and Control During Pregnancy in the Africa Region. vol. AFR/MAL/04/01. 2004, World Health Organization Regional Office for Africa
Garner P, Gulmezoglu AM: Drugs for preventing malaria in pregnant women. Cochrane Database Syst Rev. 2006, CD000169-4
Darnstadt GL, Bhutta ZA, Cousens S, Adam T, Walker N, de Bernis L: Evidence-based, cost-effective interventions: how many newborn babies can we save?. Lancet. 2005, 365: 977-988. 10.1016/S0140-6736(05)71088-6.
WHO: Assessment and Monitoring of antimalarial drug efficacy for the treatment of uncomplicated falciparum malaria. vol. WHO/HTM/RBM/2003.50. 2003, Geneva: World Health Organization
ter Kuile FO, van Eijk AM, Filler SJ: Effect of sulfadoxine-pyrimethamine resistance on the efficacy of intermittent preventive therapy for malaria control during pregnancy: a systematic review. JAMA. 2007, 297 (23): 2603-2616. 10.1001/jama.297.23.2603.
Tagbor H, Bruce J, Ord R, Randall A, Browne E, Greenwood B, Chandramohan D: Comparison of the therapeutic efficacy of chloroquine and sulphadoxine-pyremethamine in children and pregnant women. Trop Med Int Health. 2007, 12 (11): 1288-1297.
Vallely A, Vallely L, Changalucha J, Greenwood B, Chandramohan D: Intermittent preventive treatment for malaria in pregnancy in Africa: what's new, what's needed?. Malar J. 2007, 6: 16-10.1186/1475-2875-6-16.
Nosten F, McGready R, d'Alessandro U, Bonell A, Verhoeff F, Menendez C, Mutabingwa T, Brabin B: Antimalarial Drugs in Pregnancy: A Review. Current Drug Safety. 2006, 1: 1-15. 10.2174/157488606775252584.
Ward SA, Sevene EJ, Hastings IM, Nosten F, McGready R: Antimalarial drugs and pregnancy: safety, pharmacokinetics, and pharmacovigilance. Lancet Infect Dis. 2007, 7 (2): 136-144. 10.1016/S1473-3099(07)70025-7.
Newman RD, Parise ME, Slutsker L, Nahlen B, Steketee RW: Safety, efficacy and determinants of effectiveness of antimalarial drugs during pregnancy: implications for prevention programmes in Plasmodium falciparum-endemic sub-Saharan Africa. Trop Med Int Health. 2003, 8 (6): 488-506. 10.1046/j.1365-3156.2003.01066.x.
Girard AE, Girard D, English AR, Gootz TD, Cimochowski CR, Faiella JA, Haskell SL, Retsema JA: Pharmacokinetic and in vivo studies with azithromycin (CP-62,993), a new macrolide with an extended half-life and excellent tissue distribution. Antimicrob Agents Chemother. 1987, 31 (12): 1948-1954.
Dunn CJ, Barradell LB: Azithromycin. A review of its pharmacological properties and use as 3-day therapy in respiratory tract infections. Drugs. 1996, 51 (3): 483-505.
Ballow CH, Amsden GW: Azithromycin: the first azalide antibiotic. Ann Pharmacother. 1992, 26 (10): 1253-1261.
Peters DH, Friedel HA, McTavish D: Azithromycin. A review of its antimicrobial activity, pharmacokinetic properties and clinical efficacy. Drugs. 1992, 44 (5): 750-799. 10.2165/00003495-199244050-00007.
Sidhu AB, Sun Q, Nkrumah LJ, Dunne MW, Sacchettini JC, Fidock DA: In vitro efficacy, resistance selection, and structural modeling studies implicate the malarial parasite apicoplast as the target of azithromycin. J Biol Chem. 2007, 282 (4): 2494-2504. 10.1074/jbc.M608615200.
Ramsey PS, Vaules MB, Vasdev GM, Andrews WW, Ramin KD: Maternal and transplacental pharmacokinetics of azithromycin. Am J Obstet Gynecol. 2003, 188 (3): 714-718. 10.1067/mob.2003.141.
Heikkinen T, Laine K, Neuvonen PJ, Ekblad U: The transplacental transfer of the macrolide antibiotics erythromycin, roxithromycin and azithromycin. BJOG. 2000, 107 (6): 770-775. 10.1111/j.1471-0528.2000.tb13339.x.
Weiner C, Buhimschi C: Drugs for Pregnant and Lactating Women. 2004, New York: Churchill Livingston
Dahl EL, Rosenthal PJ: Apicoplast translation, transcription and genome replication: targets for antimalarial antibiotics. Trends Parasitol. 2008, 24 (6): 279-284. 10.1016/j.pt.2008.03.007.
Schlünzen F, Harms JM, Franceschi F, Hansen HA, Bartels H, Zarivach R, Yonath A: Structural basis for the antibiotic activity of ketolides and azalides. Structure. 2003, 11: 329-338. 10.1016/S0969-2126(03)00022-4.
Retsema J, Fu W: Macrolides: structures and microbial targets. International Journal of Antimicrobial Agents. 2001, 18 (Suppl 1): 3-10. 10.1016/S0924-8579(01)00401-0.
Pitsouni E, Iavazzo C, Athanasiou S, Falagas ME: Single-dose azithromycin versus erythromycin or amoxicillin for Chlamydia trachomatis infection during pregnancy: a meta-analysis of randomised controlled trials. Int J Antimicrob Agents. 2007, 30 (3): 213-221. 10.1016/j.ijantimicag.2007.04.015.
Oldfield EC, Fessel WJ, Dunne MW, Dickinson G, Wallace MR, Byrne W, Chung R, Wagner KF, Paparello SF, Craig DB, Melcher G, Zajdowicz M, Williams RF, Kelly JW, Zelasky M, Heifets LB, Berman JD: Once weekly azithromycin therapy for prevention of Mycobacterium avium complex infection in patients with AIDS: a randomized, double-blind, placebo-controlled multicenter trial. Clin Infect Dis. 1998, 26 (3): 611-619. 10.1086/514566.
Tseng AL, Dolovich L, Salit IE: Azithromycin-related ototoxicity in patients infected with human immunodeficiency virus. Clin Infect Dis. 1997, 24 (1): 76-77.
Pfizer: Trovano®/Zithromax® Compliance Pak. 1998, [http://www.fda.gov/CDER/foi/label/1998/50-762.pdf]
Duff P: Antibiotic selection in obstetric patients. Infect Dis Clin North Am. 1997, 11 (1): 1-12. 10.1016/S0891-5520(05)70338-X.
Ogasawara KK, Goodwin TM: Efficacy of azithromycin in reducing lower genital Ureaplasma urealyticum colonization in women at risk for preterm delivery. J Matern Fetal Med. 1999, 8 (1): 12-16. 10.1002/(SICI)1520-6661(199901/02)8:1<12::AID-MFM3>3.0.CO;2-8.
Donders GG: Treatment of sexually transmitted bacterial diseases in pregnant women. Drugs. 2000, 59 (3): 477-485. 10.2165/00003495-200059030-00005.
Sidhu ABS, Dunne MW, Lewis DE, Fidock DA: Identification of a novel mutation in the L4 plastid ribosomal protein in P. falciparum azithromycin-resistant lines. 54th Annual Meeting of the American Society of Topical Medicine and Hygiene. 2005, Washington DC: Albert Einstein College of Medicine and Pfizer Inc
Gingras B, Jensen J: Activity of azithromycin or erythromycin in combination with antimalarial drugs against multidrug-resistant Plasmodium falciparum in vitro. Am J Trop Med Hygiene. 1992, 47: 378-382.
Gingras B, Jensen J: Antimalarial activity of azithromycin and erythromycin against Plasmodium burghei. Am J Trop Med Hyg. 1993, 49 (1): 101-105.
Taylor WR, Richie TL, Fryauff DJ, Picarima H, Ohrt C, Tang D, Braitman D, Murphy GS, Widjaja H, Tjitra E, Ganjar A, Jones TR, Basri H, Berman J: Malaria prophylaxis using azithromycin: a double-blind, placebo-controlled trial in Irian Jaya, Indonesia. Clin Infect Dis. 1999, 28: 74-81. 10.1086/515071.
Heppner DG, Walsh DS, Uthaimongkol N, Tang DB, Tulyayon S, Permpanich B, Wimonwattrawatee T, Chuanak N, Laoboonchai A, Sookto P, Brewer TG, McDaniel P, Eamsila C, Yongvanitchit K, Uhl K, Kyle DE, Keep LW, Miller RE, Wongsrichanalai C: Randomized, controlled, double-blind trial of daily oral azithromycin in adults for the prophylaxis of Plasmodium vivax malaria in Western Thailand. Am J Trop Med Hyg. 2005, 73 (5): 842-849.
Kuschner R, Heppner D, Andersen S, Wellde B, Hall T, Schneider I, Ballou W, Foulds G, Sadoff J, Schuster B: Azithromycin prophylaxis against a chloroquine resistant strain of Plasmodium falciparum. Lancet. 1994, 343 (8910): 1396-1397. 10.1016/S0140-6736(94)92526-7.
Anderson S, Berman J, Kuschner R, Wesche D, Magill A, Wellde B, Schneider I, Dunne M, Schuster B: Prophylaxis of Plasmodium falciparum malaria with azithromycin administered to volunteers. Ann Intern Med. 1995, 123: 771-773.
Andersen SL, Oloo AJ, Gordon DM, Ragama OB, Aleman GM, Berman JD, Tang DB, Dunne MW, Shanks GD: Successful double-blinded, randomized, placebo-controlled field trial of azithromycin and doxycycline as prophylaxis for malaria in western Kenya. Clin Infect Dis. 1998, 26 (1): 146-150. 10.1086/516281.
Krishna S, White NJ: Pharmacokinetics of quinine, chloroquine and amodiaquine. Clinical implications. Clin Pharmacokinet. 1996, 30 (4): 263-299. 10.2165/00003088-199630040-00002.
Dollery D, (ed.): Therapeutic drugs. 1999, Edinburgh, UK: Churchill Livingstone
Krogstad DJ, Schlesinger PH: Acid-vesicle function, intracellular pathogens, and the action of chloroquine against Plasmodium falciparum. N Engl J Med. 1987, 317 (9): 542-549.
Sidhu AB, Verdier-Pinard D, Fidock DA: Chloroquine resistance in Plasmodium falciparum malaria parasites conferred by pfcrt mutations. Science. 2002, 298 (5591): 210-213. 10.1126/science.1074045.
Fidock DA, Nomura T, Talley AK, Cooper RA, Dzekunov SM, Ferdig MT, Ursos LM, Sidhu AB, Naude B, Deitsch KW, Su XZ, Wootton JC, Roepe PD, Wellems TE: Mutations in the P. falciparum digestive vacuole transmembrane protein PfCRT and evidence for their role in chloroquine resistance. Mol Cell. 2000, 6 (4): 861-871. 10.1016/S1097-2765(05)00077-8.
Jaeger A: Poisonous substances: Quinine and chloroquine. Medicine. 2007, 35: 652-653. 10.1016/j.mpmed.2007.09.023.
Sowunmi A, Walker O, Salako LA: Pruritus and antimalarial drugs in Africans. Lancet. 1989, 2 (8656): 213-10.1016/S0140-6736(89)90391-7.
Mutabingwa T, Villegas L, Nosten F: Chemoprophylaxis and other protective measures: Preventing pregnancy malaria. Malaria in Pregnancy: Deadly Parasite, Susceptible Host. Edited by: Duffy P, Fried M. 2001, London: Taylor and Francis, 189-222.
Helitzer-Allen DL, Macheso A, Wirima J, Kendall C: Testing strategies to increase use of chloroquine chemoprophylaxis during pregnancy in Malawi. Acta Trop. 1994, 58 (3–4): 255-266. 10.1016/0001-706X(94)90019-1.
Kaseje DC, Sempebwa EK, Spencer HC: Malaria chemoprophylaxis to pregnant women provided by community health workers in Saradidi, Kenya. I. Reasons for non-acceptance. Ann Trop Med Parasitol. 1987, 81 (Suppl 1): 77-82.
Mita T, Kaneko A, Lum JK, Bwijo B, Takechi M, Zungu IL, Tsukahara T, Tanabe K, Kobayakawa T, Bjorkman A: Recovery of chloroquine sensitivity and low prevalence of the Plasmodium falciparum chloroquine resistance transporter gene mutation K76T following the discontinuance of chloroquine use in Malawi. Am J Trop Med Hyg. 2003, 68 (4): 413-415.
Takechi M, Matsuo M, Ziba C, MacHeso A, Butao D, Zungu IL, Chakanika I, Bustos MD: Therapeutic efficacy of sulphadoxine/pyrimethamine and susceptibility in vitro of P. falciparum isolates to sulphadoxine-pyremethamine and other antimalarial drugs in Malawian children. Trop Med Int Health. 2001, 6 (6): 429-434. 10.1046/j.1365-3156.2001.00735.x.
Djimde A, Doumbo OK, Cortese JF, Kayentao K, Doumbo S, Diourte Y, Dicko A, Su XZ, Nomura T, Fidock DA, Wellems TE, Plowe CV, Coulibaly D: A molecular marker for chloroquine-resistant falciparum malaria. N Engl J Med. 2001, 344 (4): 257-263. 10.1056/NEJM200101253440403.
Kublin JG, Cortese JF, Njunju EM, Mukadam RA, Wirima JJ, Kazembe PN, Djimde AA, Kouriba B, Taylor TE, Plowe CV: Reemergence of chloroquine-sensitive Plasmodium falciparum malaria after cessation of chloroquine use in Malawi. J Infect Dis. 2003, 187 (12): 1870-1875. 10.1086/375419.
Laufer MK, Thesing PC, Eddington ND, Masonga R, Dzinjalamala FK, Takala SL, Taylor TE, Plowe CV: Return of chloroquine antimalarial efficacy in Malawi. N Engl J Med. 2006, 355 (19): 1959-1966. 10.1056/NEJMoa062032.
Hastings IM, Donnelly MJ: The impact of antimalarial drug resistance mutations on parasite fitness, and its implications for the evolution of resistance. Drug Resist Updat. 2005, 8 (1–2): 43-50. 10.1016/j.drup.2005.03.003.
Laufer MK, Plowe CV: Withdrawing antimalarial drugs: impact on parasite resistance and implications for malaria treatment policies. Drug Resist Updat. 2004, 7 (4–5): 279-288. 10.1016/j.drup.2004.08.003.
Walliker D, Hunt P, Babiker H: Fitness of drug-resistant malaria parasites. Acta Trop. 2005, 94 (3): 251-259.
Denoeud L, Fievet N, Aubouy A, Ayemonna P, Kiniffo R, Massougbodji A, Cot M: Is chloroquine chemoprophylaxis still effective to prevent low birth weight? Results of a study in Benin. Malar J. 2007, 6: 27-10.1186/1475-2875-6-27.
Tagbor H, Bruce J, Browne E, Randal A, Greenwood B, Chandramohan D: Efficacy, safety, and tolerability of amodiaquine plus sulphadoxine-pyrimethamine used alone or in combination for malaria treatment in pregnancy: a randomised trial. Lancet. 2006, 368 (9544): 1349-1356. 10.1016/S0140-6736(06)69559-7.
Ohrt C, Willingmyre GD, Lee P, Knirsch C, Milhous W: Assessment of azithromycin in combination with other antimalarial drugs against Plasmodium falciparum in vitro. Antimicrob Agents Chemother. 2002, 46 (8): 2518-2524. 10.1128/AAC.46.8.2518-2524.2002.
Cook JA, Randinitis EJ, Bramson CR, Wesche DL: Lack of a pharmacokinetic interaction between azithromycin and chloroquine. Am J Trop Med Hyg. 2006, 74 (3): 407-412.
Martin SK, Oduola AM, Milhous WK: Reversal of chloroquine resistance in Plasmodium falciparum by verapamil. Science. 1987, 235 (4791): 899-901. 10.1126/science.3544220.
Bray PG, Boulter MK, Ritchie GY, Howells RE, Ward SA: Relationship of global chloroquine transport and reversal of resistance in Plasmodium falciparum. Mol Biochem Parasitol. 1994, 63 (1): 87-94. 10.1016/0166-6851(94)90011-6.
Pachot JI, Botham RP, Haegele KD, Hwang K: Experimental estimation of the role of P-Glycoprotein in the pharmacokinetic behaviour of telithromycin, a novel ketolide, in comparison with roxithromycin and other macrolides using the Caco-2 cell model. J Pharm Pharm Sci. 2003, 6 (1): 1-12.
Dunne MW, Singh N, Shukla M, Valecha N, Bhattacharyya PC, Dev V, Patel K, Mohapatra MK, Lakhani J, Benner R, Lele C, Patki K: A multicenter study of azithromycin, alone and in combination with chloroquine, for the treatment of acute uncomplicated Plasmodium falciparum malaria in India. J Infect Dis. 2005, 191 (10): 1582-1588. 10.1086/429343.
Lewis D, Mulenga M, Oduro A, Mugyenyi P, Wasunna M, Kokwaro G, Aman R, Sagara I, Nambozi M, Ansah P, Kityo C, Dunne M: A Phase 2/3, Randomized, Double Blind, Comparative Trial of Azithromycin Plus Chloroquine Versus Mefloquine for the Treatment of Uncomplicated Plasmodium falciparum Malaria in Africa. 5th European Congress on Tropical Medicine and International Health. Amsterdam. 2007
Chandra R, Lewis D, Oduro A, Mulenga M, Sagara I, Sie A, Tiono A, Dieng Y, Ogutu B, Sarkar S, Djimde A, Ansha P, Nambozi M, Zoungrana A, Ouedraogo A, Fall M, Tina LO, Dunne M: A Phase 3, Randomized, Open-Label, Comparative Trial of Azithromycin plus Chloroquine versus Mefloquine for the Treatment of Uncomplicated Plasmodium falciparum Malaria in Africa. 56th Annual Meeting of the American Society of Topical Medicine and Hygiene. 2007, Philadelphia: Pfizer Inc
Kolaczinski JH, Ojok N, Opwonya J, Meek S, Collins A: Adherence of community caretakers of children to pre-packaged antimalarial medicines (HOMAPAK) among internally displaced people in Gulu district, Uganda. Malar J. 2006, 5: 40-10.1186/1475-2875-5-40.
Orton L, Barnish G: Unit-dose packaged drugs for treating malaria. Cochrane Database Syst Rev. 2005, CD004614-2
Connor J, Rafter N, Rodgers A: Do fixed-dose combination pills or unit-of-use packaging improve adherence? A systematic review. Bull World Health Organ. 2004, 82 (12): 935-939.
McDonald HP, Garg AX, Haynes RB: Interventions to enhance patient adherence to medication prescriptions: scientific review. JAMA. 2002, 288 (22): 2868-2879. 10.1001/jama.288.22.2868.
Davis TM, Hung TY, Sim IK, Karunajeewa HA, Ilett KF: Piperaquine: a resurgent antimalarial drug. Drugs. 2005, 65 (1): 75-87. 10.2165/00003495-200565010-00004.
Nakornchai S, Konthiang P: Activity of azithromycin or erythromycin in combination with antimalarial drugs against multidrug-resistant Plasmodium falciparum in vitro. Acta Trop. 2006, 100 (3): 185-191. 10.1016/j.actatropica.2006.10.008.
Rogerson SJ, Mwapasa V, Meshnick SR: Malaria in pregnancy: linking immunity and pathogenesis to prevention. Am J Trop Med Hyg. 2007, 77 (6 Suppl): 14-22.
Nosten F, Vincenti M, Simpson J, Yei P, Thwai KL, de Vries A, Chongsuphajaisiddhi T, White NJ: The effects of mefloquine treatment in pregnancy. Clin Infect Dis. 1999, 28 (4): 808-815. 10.1086/515183.
Smoak BL, Writer JV, Keep LW, Cowan J, Chantelois JL: The effects of inadvertent exposure of mefloquine chemoprophylaxis on pregnancy outcomes and infants of US Army servicewomen. J Infect Dis. 1997, 176 (3): 831-833.
Novartis: Coartem/Riamet. Product monograph: A novel antimalarial combination: one product, two concepts. 2005, Novartis Pharma AG
WHO: Assessment of the Safety of Artemisinin Compounds in Pregnancy. Report of two informal consultations convened by WHO in 2002 (Roll Back Malaria and the UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases). vol. WHO/CDS/MAL/2003.1094. WHO/RBM/TDR/Artemisinin/03.1. 2003, Geneva: World Health Organization, [http://www.who.int/malaria/cmc_upload/0/000/016/323/artemisinin_pregnancy.pdf]
Mullick S, Watson-Jones D, Beksinska M, Mabey D: Sexually transmitted infections in pregnancy: prevalence, impact on pregnancy outcomes, and approach to treatment in developing countries. Sex Transm Infect. 2005, 81 (4): 294-302. 10.1136/sti.2002.004077.
WHO: Sexually transmitted and other reproductive tract infections: Guide to essential practice. 2005, Geneva: Department of Reproductive Health and Research, World Health Organization
Latif AS, Mason PR, Marowa E, Gwanzura L, Chingono A, Mbengeranwa OL: Risk factors for gonococcal and chlamydial cervical infection in pregnant and non-pregnant women in Zimbabwe. Cent Afr J Med. 1999, 45 (10): 252-258.
Fonck K, Kidula N, Jaoko W, Estambale B, Claeys P, Ndinya-Achola J, Kirui P, Bwayo J, Temmerman M: Validity of the vaginal discharge algorithm among pregnant and non-pregnant women in Nairobi, Kenya. Sex Transm Infect. 2000, 76 (1): 33-38. 10.1136/sti.76.1.33.
Gray RH, Wabwire-Mangen F, Kigozi G, Sewankambo NK, Serwadda D, Moulton LH, Quinn TC, O'Brien KL, Meehan M, Abramowsky C, Robb M, Wawer MJ: Randomized trial of presumptive sexually transmitted disease therapy during pregnancy in Rakai, Uganda. Am J Obstet Gynecol. 2001, 185 (5): 1209-1217. 10.1067/mob.2001.118158.
Msuya SE, Mbizvo E, Stray-Pedersen B, Sundby J, Sam NE, Hussain A: Reproductive tract infections among women attending primary health care facilities in Moshi, Tanzania. East Afr Med J. 2002, 79 (1): 16-21.
Watson-Jones D, Changalucha J, Gumodoka B, Weiss H, Rusizoka M, Ndeki L, Whitehouse A, Balira R, Todd J, Ngeleja D, Ross D, Buve A, Hayes R, Mabey D: Syphilis in pregnancy in Tanzania. I. Impact of maternal syphilis on outcome of pregnancy. J Infect Dis. 2002, 186 (7): 940-947. 10.1086/342952.
Rastogi S, Das B, Salhan S, Mittal A: Effect of treatment for Chlamydia trachomatis during pregnancy. Int J Gynaecol Obstet. 2003, 80 (2): 129-137. 10.1016/S0020-7292(02)00371-5.
Sullivan EA, Abel M, Tabrizi S, Garland SM, Grice A, Poumerol G, Taleo H, Chen S, Kaun K, O'Leary M, Kaldor J: Prevalence of sexually transmitted infections among antenatal women in Vanuatu, 1999–2000. Sex Transm Dis. 2003, 30 (4): 362-366. 10.1097/00007435-200304000-00017.
Plummer FA, Laga M, Brunham RC, Piot P, Ronald AR, Bhullar V, Mati JY, Ndinya-Achola JO, Cheang M, Nsanze H: Postpartum upper genital tract infections in Nairobi, Kenya: epidemiology, etiology, and risk factors. J Infect Dis. 1987, 156 (1): 92-98.
Blankhart D, Muller O, Gresenguet G, Weis P: Sexually transmitted infections in young pregnant women in Bangui, Central African Republic. Int J STD AIDS. 1999, 10 (9): 609-614. 10.1258/0956462991914753.
Farley TA, Cohen DA, Elkins W: Asymptomatic sexually transmitted diseases: the case for screening. Prev Med. 2003, 36 (4): 502-509. 10.1016/S0091-7435(02)00058-0.
Marai W: Lower genital tract infections among pregnant women: a review. East Afr Med J. 2001, 78 (11): 581-585.
Schulz KF, Cates W, O'Mara PR: Pregnancy loss, infant death, and suffering: legacy of syphilis and gonorrhoea in Africa. Genitourin Med. 1987, 63 (5): 320-325.
Steen R: Eradicating chancroid. Bull World Health Organ. 2001, 79 (9): 818-826.
Mayaud P, ka-Gina G, Cornelissen J, Todd J, Kaatano G, West B, Uledi E, Rwakatare M, Kopwe L, Manoko D, Laga M, Grosskurth H, Hayes R, Mabey D: Validation of a WHO algorithm with risk assessment for the clinical management of vaginal discharge in Mwanza, Tanzania. Sex Transm Infect. 1998, 74 (Suppl 1): S77-84.
Alary M, Baganizi E, Guedeme A, Padonou F, Davo N, Adjovi C, van Dyck E, Germain M, Joly J, Mahony JB: Evaluation of clinical algorithms for the diagnosis of gonococcal and chlamydial infections among men with urethral discharge or dysuria and women with vaginal discharge in Benin. Sex Transm Infect. 1998, 74 (Suppl 1): S44-49.
Vuylsteke B, Laga M, Alary M, Gerniers MM, Lebughe JP, Nzila N, Behets F, Van Dyck E, Piot P: Clinical algorithms for the screening of women for gonococcal and chlamydial infection: evaluation of pregnant women and prostitutes in Zaire. Clin Infect Dis. 1993, 17 (1): 82-88.
Daly CC, Wangel AM, Hoffman IF, Canner JK, Lule GS, Lema VM, Liomba NG, Dallabetta GA: Validation of the WHO diagnostic algorithm and development of an alternative scoring system for the management of women presenting with vaginal discharge in Malawi. Sex Transm Infect. 1998, 74: S50-58. 10.1136/sti.74.1.50.
Wilkinson D, Abdool Karim SS, Harrison A, Lurie M, Colvin M, Connolly C, Sturm AW: Unrecognized sexually transmitted infections in rural South African women: a hidden epidemic. Bull World Health Organ. 1999, 77 (1): 22-28.
Kiddugavu MG, Kiwanuka N, Wawer MJ, Serwadda D, Sewankambo NK, Wabwire-Mangen F, Makumbi F, Li X, Reynolds SJ, Quinn TC, Gray RH: Effectiveness of syphilis treatment using azithromycin and/or benzathine penicillin in Rakai, Uganda. Sex Transm Dis. 2005, 32 (1): 1-6. 10.1097/01.olq.0000148297.48590.d8.
Riedner G, Rusizoka M, Todd J, Maboko L, Hoelscher M, Mmbando D, Samky E, Lyamuya E, Mabey D, Grosskurth H, Hayes R: Single-dose azithromycin versus penicillin G benzathine for the treatment of early syphilis. N Engl J Med. 2005, 353 (12): 1236-1244. 10.1056/NEJMoa044284.
Ratnam AV, Din SN, Hira SK, Bhat GJ, Wacha DS, Rukmini A, Mulenga RC: Syphilis in pregnant women in Zambia. Br J Vener Dis. 1982, 58 (6): 355-358.
Zhou P, Qian Y, Xu J, Gu Z, Liao K: Occurrence of congenital syphilis after maternal treatment with azithromycin during pregnancy. Sex Transm Dis. 2007, 34 (7): 472-474. 10.1097/01.olq.0000246314.35047.91.
Rottingen JA, Cameron DW, Garnett GP: A systematic review of the epidemiologic interactions between classic sexually transmitted diseases and HIV: how much really is known?. Sex Transm Dis. 2001, 28 (10): 579-597. 10.1097/00007435-200110000-00005.
Gray RH, Wawer MJ: Reassessing the hypothesis on STI control for HIV prevention. Lancet. 2008, 371 (9630): 2064-2065. 10.1016/S0140-6736(08)60896-X.
Neely M, Kalyesubula I, Bagenda D, Myers C, Olness K: Effect of chloroquine on human immunodeficiency virus (HIV) vertical transmission. Afr Health Sci. 2003, 3 (2): 61-67.
Semrau K, Kuhn L, Kasonde P, Sinkala M, Kankasa C, Shutes E, Vwalika C, Ghosh M, Aldrovandi G, Thea DM: Impact of chloroquine on viral load in breast milk. Trop Med Int Health. 2006, 11 (6): 800-803. 10.1111/j.1365-3156.2006.01645.x.
Lim WS, Macfarlane JT, Colthorpe CL: Pneumonia and pregnancy. Thorax. 2001, 56 (5): 398-405. 10.1136/thorax.56.5.398.
Hopwood HG: Pneumonia in pregnancy. Obstet Gynecol. 1965, 25: 875-879.
Goodrum LA: Pneumonia in pregnancy. Semin Perinatol. 1997, 21 (4): 276-283. 10.1016/S0146-0005(97)80070-5.
Goodnight WH, Soper DE: Pneumonia in pregnancy. Crit Care Med. 2005, 33 (Suppl 10): S390-397. 10.1097/01.CCM.0000182483.24836.66.
Lucas AO: Pneumococcal meningitis in pregnancy and the puerperium. Br Med J. 1964, 1 (5375): 92-95.
Frye JE, (ed.): International Drug Price Indicator Guide. 2008, Cambridge, MA: Management Sciences for Health, [http://erc.msh.org/mainpage.cfm?file=1.0.htm&module=DMP&language=english]
CDC: Sexually Transmitted Disease Surveillance 2006 Supplement, Gonococcal Isolate Surveillance Project (GISP) Annual Report 2006. 2006, Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention
Lau CY, Qureshi AK: Azithromycin versus doxycycline for genital chlamydial infections: a meta-analysis of randomized clinical trials. Sex Transm Dis. 2002, 29 (9): 497-502. 10.1097/00007435-200209000-00001.
Mitchell SJ, Engelman J, Kent CK, Lukehart SA, Godornes C, Klausner JD: Azithromycin-resistant syphilis infection: San Francisco, California, 2000–2004. Clin Infect Dis. 2006, 42 (3): 337-345. 10.1086/498899.
Stamm LV, Bergen HL: A point mutation associated with bacterial macrolide resistance is present in both 23S rRNA genes of an erythromycin-resistant Treponema pallidum clinical isolate. Antimicrob Agents Chemother. 2000, 44 (3): 806-807. 10.1128/AAC.44.3.806-807.2000.
Lukehart SA, Godornes C, Molini BJ, Sonnett P, Hopkins S, Mulcahy F, Engelman J, Mitchell SJ, Rompalo AM, Marra CM, Klausner JD: Macrolide resistance in Treponema pallidum in the United States and Ireland. N Engl J Med. 2004, 351 (2): 154-158. 10.1056/NEJMoa040216.
Katz KA, Klausner JD: Azithromycin resistance in Treponema pallidum. Curr Opin Infect Dis. 2008, 21 (1): 83-91.
Marra CM, Colina AP, Godornes C, Tantalo LC, Puray M, Centurion-Lara A, Lukehart SA: Antibiotic selection may contribute to increases in macrolide-resistant Treponema pallidum. J Infect Dis. 2006, 194 (12): 1771-1773. 10.1086/509512.
Behets F, van Damme K, Ravelomanana N: Evaluation of azithromycin resistance in T. pallidum isolates from Madagascar [abstract 0-095]. 17th International Society for Sexually Transmitted Diseases Research and 10th International Union Against Sexually Transmitted Infections World Congress. 2007, Seattle, WA: International Society for Sexually Transmitted Diseases Research
Leach AJ, Shelby-James TM, Mayo M, Gratten M, Laming AC, Currie BJ, Mathews JD: A prospective study of the impact of community-based azithromycin treatment of trachoma on carriage and resistance of Streptococcus pneumoniae. Clin Infect Dis. 1997, 24 (3): 356-362.
Gaynor BD, Chidambaram JD, Cevallos V, Miao Y, Miller K, Jha HC, Bhatta RC, Chaudhary JS, Osaki Holm S, Whitcher JP, Holbrook KA, Fry AM, Lietman TM: Topical ocular antibiotics induce bacterial resistance at extraocular sites. Br J Ophthalmol. 2005, 89 (9): 1097-1099. 10.1136/bjo.2005.068981.
Chern KC, Shrestha SK, Cevallos V, Dhami HL, Tiwari P, Chern L, Whitcher JP, Lietman TM: Alterations in the conjunctival bacterial flora following a single dose of azithromycin in a trachoma endemic area. Br J Ophthalmol. 1999, 83 (12): 1332-1335. 10.1136/bjo.83.12.1332.
Gaynor BD, Holbrook KA, Whitcher JP, Holm SO, Jha HC, Chaudhary JS, Bhatta RC, Lietman T: Community treatment with azithromycin for trachoma is not associated with antibiotic resistance in Streptococcus pneumoniae at 1 year. Br J Ophthalmol. 2003, 87 (2): 147-148. 10.1136/bjo.87.2.147.
Batt SL, Charalambous BM, Solomon AW, Knirsch C, Massae PA, Safari S, Sam NE, Everett D, Mabey DC, Gillespie SH: Impact of azithromycin administration for trachoma control on the carriage of antibiotic-resistant Streptococcus pneumoniae. Antimicrob Agents Chemother. 2003, 47 (9): 2765-2769. 10.1128/AAC.47.9.2765-2769.2003.
Felmingham D, White AR, Jacobs MR, Appelbaum PC, Poupard J, Miller LA, Gruneberg RN: The Alexander Project: the benefits from a decade of surveillance. J Antimicrob Chemother. 2005, 56 (Suppl 2): ii3-ii21. 10.1093/jac/dki297.
Leclercq R: Mechanisms of resistance to macrolides and lincosamides: nature of the resistance elements and their clinical implications. Clin Infect Dis. 2002, 34 (4): 482-492. 10.1086/324626.
Feldman C: Clinical relevance of antimicrobial resistance in the management of pneumococcal community-acquired pneumonia. J Lab Clin Med. 2004, 143 (5): 269-283. 10.1016/j.lab.2004.02.002.
Bishai W: The in vivo-in vitro paradox in pneumococcal respiratory tract infections. J Antimicrob Chemother. 2002, 49 (3): 433-436. 10.1093/jac/49.3.433.
Gladue RP, Bright GM, Isaacson RE, Newborg MF: In vitro and in vivo uptake of azithromycin (CP-62,993) by phagocytic cells: possible mechanism of delivery and release at sites of infection. Antimicrob Agents Chemother. 1989, 33 (3): 277-282.
McCracken GH: Microbiologic activity of the newer macrolide antibiotics. Pediatr Infect Dis J. 1997, 16 (4): 432-437. 10.1097/00006454-199704000-00026.
Hyde TB, Gay K, Stephens DS, Vugia DJ, Pass M, Johnson S, Barrett NL, Schaffner W, Cieslak PR, Maupin PS, Zell ER, Jorgensen JH, Facklam RR, Whitney CG: Macrolide resistance among invasive Streptococcus pneumoniae isolates. JAMA. 2001, 286 (15): 1857-1862. 10.1001/jama.286.15.1857.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
MC structured the review and wrote the paper. RP reviewed the early manuscript and contributed to the writing of the paper. BG reviewed the early manuscript and contributed to the writing of the paper. DC refined the structure of the review and contributed to the writing of the paper. All authors read and approved the final version.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Chico, R.M., Pittrof, R., Greenwood, B. et al. Azithromycin-chloroquine and the intermittent preventive treatment of malaria in pregnancy. Malar J 7, 255 (2008). https://doi.org/10.1186/1475-2875-7-255
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-7-255