
Abstract
Background
Maps of malaria distribution are vital for optimal allocation of resources for anti-malarial activities. There is a lack of reliable contemporary malaria maps in endemic countries in sub-Saharan Africa. This problem is particularly acute in low malaria transmission countries such as those located in the horn of Africa.
Methods
Data from a national malaria cluster sample survey in 2005 and routine cluster surveys in 2007 were assembled for Somalia. Rapid diagnostic tests were used to examine the presence of Plasmodium falciparum parasites in finger-prick blood samples obtained from individuals across all age-groups. Bayesian geostatistical models, with environmental and survey covariates, were used to predict continuous maps of malaria prevalence across Somalia and to define the uncertainty associated with the predictions.
Results
For analyses the country was divided into north and south. In the north, the month of survey, distance to water, precipitation and temperature had no significant association with P. falciparum prevalence when spatial correlation was taken into account. In contrast, all the covariates, except distance to water, were significantly associated with parasite prevalence in the south. The inclusion of covariates improved model fit for the south but not for the north. Model precision was highest in the south. The majority of the country had a predicted prevalence of < 5%; areas with ≥ 5% prevalence were predominantly in the south.
Conclusion
The maps showed that malaria transmission in Somalia varied from hypo- to meso-endemic. However, even after including the selected covariates in the model, there still remained a considerable amount of unexplained spatial variation in parasite prevalence, indicating effects of other factors not captured in the study. Nonetheless the maps presented here provide the best contemporary information on malaria prevalence in Somalia.
Similar content being viewed by others


Background
Maps of disease distribution are an essential tool for optimizing the allocation of resources for malaria interventions [1, 2]. There have been a number of attempts to develop malaria transmission maps at different geographic scales based on expert opinion [3, 4]; deterministic biological models driven by the conceptual relationship between transmission and environmental covariates [5]; and empirical transmission models based on entomological inoculation rates [6, 7] or human infection prevalence data [8–17]. These methods suffer several limitations: expert opinion maps are subjective; deterministic models ignore the secular effects of expanded coverage of interventions that supersede the influence of climate on the epidemiology of malaria and do not quantify uncertainty around model results. Where studies have used observational data to predict malaria distributions, most have used historical data collected opportunistically from secondary sources [10, 15, 16] that did not involve random sampling and/or a sampling framework optimized for spatial analysis.
Arguably the greatest need for malaria maps is at the periphery of stable, endemic areas where decisions about the delivery of standard suites of interventions, such as those promoted by the Roll Back Malaria (RBM) initiative to support malaria control in high transmission areas, may become less appropriate or cost-efficient. In areas of perceived low malaria risk there is little empirical information on the risks and intensity of transmission. As such the semi-arid regions of the horn of Africa remain less well described epidemiologically compared to the rest of malaria endemic sub-Saharan Africa (SSA) and there are no contemporary national maps of the extents of malaria risk. The Malaria Atlas Project (MAP) while maintaining a global remit in its efforts to improve the cartography of malaria [2] is equally committed to developing national mapping initiatives with country partners, where the data available can support rigorous cartography. Somalia represents the first such example.
A Plasmodium falciparum malaria prevalence map for Somalia is presented here using Bayesian geostatistical analysis of community-based parasite prevalence survey data. The data used in this analysis have several unique features that minimize some of the problems of using retrospectively assembled data: first the community data were derived from random sample surveys undertaken as part of national malaria or nutritional surveys; second all the data were collected using similar methodologies; and finally all the data represent contemporary infection prevalence between 2005 and 2007.
Methods
Country context
Somalia is located in the horn of Africa with a predominantly semi-arid climate and is transected by two major seasonal rivers, the Shabelle and the Juba (Figure 1). Somalia is divided into three zones: South-Central; North-West (Somaliland); and North-East (Puntland) (Figure 1). The country has been without a functioning national government for almost two decades. Several international relief agencies and non-governmental organizations, however, support the provision of public services including health services [18]. While not internationally recognized, the three zones are all self-declared states, each with independent "ministries of health". In collaboration with these ministries of health, the United Nations Children Fund (UNICEF), as the principal recipient of money from the Global Fund to Fight Aids TB and Malaria (GFATM), together with World Health Organization (WHO), are responsible for supporting malaria control activities. These activities include: training health workers and equipping health facilities; supply of anti-malarials; distribution of insecticide-treated nets; and funding of entomological and parasitological surveillance [19].

Map of Somalia showing the self-declared states of Puntland, Somaliland and South Central; their capital cities; and the two main rivers of Juba and Shabelle.
The earliest malariometric surveys undertaken in Somalia were in the North-West in 1946 which reported a highly varying prevalence distribution of P. falciparum ranging from 0 to 17% across three clusters of villages [20]. Between the 1940s and 2005 there were only three malaria infection surveys across five villages in the Lower Shabelle area of the south-central zone [21–23]. Based on limited entomological data, malaria transmission is thought to be supported almost entirely by Anopheles arabiensis [24–26].
Assembling the survey data on parasite prevalence
Following the dearth of P. falciparum parasite rate (Pf PR) surveys over the last 50 years, community-based surveys of Pf PR have become a routine undertaking across the country since 2005. These surveys have been embedded in two major activities. First, a national malaria indicator survey was conducted by the WHO between January and February 2005 in the south-central and north-west zones [27] and in July 2005 in the north-east [28]. A stratified multi-stage random sampling strategy was adopted. Within each zone all regions were sampled and out of 120 districts in these regions, 88 were selected at random. Randomly selected villages within each district were surveyed successively until the required number of respondents of all ages (at least 845 per region) was achieved. Second, the United Nations Food Agricultural Organization-Food Security Analysis Unit (FAO/FSAU) completed 18 independent cluster sample surveys between March and November 2007. Malaria parasitology in all age-groups was included in these routine nutritional surveys at the request of UNICEF. In each survey a stratified multi-stage cluster sampling design was adopted where the sampling frame of a selected district was based on three livelihood definitions (pastoral, agro-pastoral, and riverine) [29, 30] within which 30 rural communities and 30 households within each community were selected at random.
In all surveys, evidence of parasitaemia was determined using P. falciparum specific Rapid Diagnostic Tests (RDTs). WHO used ParaHIT – f™ Device (Span Diagnostics Limited, Surat, India) while FSAU used Paracheck Pf™ (Orchid Biomedical Systems, Goa, India). The purpose of the survey was explained to each household head or adult representative from whom informed consent was then sought prior to undertaking parasitological tests. All individuals who tested positive for infection were treated with nationally recommended first-line therapy [31]. An inclusion criterion of a minimum of 40 individuals per community was used to select villages to include in the analysis to minimize random variation inherent in small samples [32, 33].
Survey data from all three sources were combined into a single database. Where communities had been surveyed more than once, the survey with the largest sample size was selected. A detailed search was undertaken to establish a set of spatial coordinates for each community. For some of the later surveys undertaken by FSAU, global positioning systems (GPS) were used to provide a longitude and latitude. For the remaining settlements a combination of electronic gazetteers [34, 35] and other nationally derived UN sources of longitude and latitude [36] were used to locate the community. Finally, the location of each settlement was verified by using Google Earth (Google, Seattle, USA) to visually inspect whether the coordinates matched evidence of human settlement. Those settlements for which no reliable source of the coordinates could be obtained were excluded from the analysis.
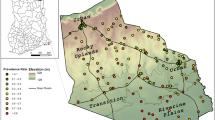
The assembled Pf PR data locations were not distributed evenly across Somalia with a higher concentration in the South-Central zone. Exploratory analysis showed different spatial autocorrelation structures for the two zones (Figure 2) and a single geostatistical model for the whole country was deemed inappropriate. To allow representative models to be developed in each region, the data were split and analysis was carried out separately for the north (north-west and north-east states combined) and the south (south-central state) (Figure 2).

Map and variograms of north and south of Somalia showing the distribution PR data locations (the X-axis shows distance as degrees latitude and longitude). The data were distributed as model (n = 113 north; n = 336 south) and outlier (n = 2 north; n = 1 south) locations. Variograms are of the data after outliers were removed.
Outlier detection
Geostatistical methods are particularly sensitive to outlying values that exert a significant effect on predictions. Extreme outliers were therefore identified and excluded using a spatial filter. The method assumes that the probability of an unusually large Pf PR value being a genuine 'outlier' is larger if (a) it is in a neighbourhood of generally much smaller values and/or (b) the neighbourhood is generally uniform. A spatial filtering algorithm was implemented that incorporated these heuristic considerations (Additional File 1).
Selection of covariates
Climatic and survey covariates were considered for inclusion in the spatial prediction model. The following four climatic variables were considered, each of which was resampled to 5 × 5 km resolution to be consistent with the prediction grid. 1) The enhanced vegetation index (EVI) derived from the global Moderate Resolution Imaging Spectroradiometer (MODIS) satellite imagery for the period 2001–2005 [37]. Temporal Fourier analysis was undertaken to derive a global EVI index [38]. These data were available for each month at 1 × 1 km spatial resolution and obtained from a global archive developed recently by the Spatial Ecology and Epidemiology Group of the Department of Zoology, University of Oxford [38]. Scaled EVI values ranged from 0–1, representing no, to complete vegetation cover. 2) Precipitation and temperature data described as the average monthly precipitation and temperature (minimum and maximum) at 1 × 1 km spatial resolution were downloaded from the WorldClim website [39]. These climate surfaces were developed through interpolation of global meteorological data collected from 1950–2000 [40]. 3) Distance to permanent water bodies was derived for each survey location using information provided by Africover [41] and those of marshes, flood plains and intermittent wetland from the Global Lakes and Wetlands databases [42]. 4) The effect of month of survey was assessed because of the observed temporal heterogeneity of Pf PR data. February was selected as the "reference month" for both zones as this was the earliest calendar month in which surveys were undertaken.
The annual mean of each environmental covariate (derived from the monthly data) was extracted at each survey location using ArcGIS 9.1 (ESRI Inc., USA). To assess the effects of the covariates on observed PfPR, non-spatial binomial logistic regression models were implemented in Stata/SE Version 10 (Stata Corporation, College Station, TX, USA). With PfPR as the dependent variable, bivariate binomial logistic regression models were fitted and covariates with Wald's P > 0.2 were excluded from subsequent analyses. Collinearity among all remaining covariates was assessed and if a pair had a correlation coefficient > 0.9, the variable with the highest value of Akaike Information Criterion (AIC) was discarded. To select which of the two temperature variables (maximum and minimum) to include into the multivariate model, the one with lowest value of AIC was chosen [9]. A non-spatial binomial multivariate logistic regression was then fitted, starting with a saturated model, and then seeking a parsimonious model using backwards variable elimination with an exit criterion of Wald's P > 0.2. Variables that exhibited non-linear relationships with PfPR were dichotomized at the median.
Bayesian geostatistical models
Bayesian geostatistical (kriging) techniques provide a framework for predicting (interpolating) values of a variable of interest at unobserved locations given a set of spatially distributed data, incorporating spatial autocorrelation and computing uncertainty measures around model predictions [43, 44]. Spatial autocorrelation in the Somalia Pf PR data was therefore first evaluated by computing empirical variograms, a graphical summary of spatial autocorrelation structure, separately for the south and the north. Different variogram structures were observed for the two zones indicating that a single stationary model for the whole country was inappropriate. Comparison of the variograms suggested greater heterogeneity of observed parasite prevalence data in the south than in the north consistent with expert opinion of the transmission dynamics across the country [26]. Consequently models were constructed separately for each zone. Bayesian binomial generalized linear geostatistical models [43] were implemented in each zone with the spatial component modelled as a stationary Gaussian process with mean of zero and covariance structure defined by a powered exponential function [45]. Because survey data were modelled as a conditionally binomial variable, given the underlying Gaussian process, the variance due to sample size was accounted for implicitly. The models were implemented in WinBUGS Version 1.4 (MRC Biostatistics Unit, Cambridge, UK). The models were constructed with and without the covariates in order to compare differences in model fit. Model fit was based on the deviance information criterion (DIC). Models with a smaller DIC value (with a difference >5) were considered to represent a better compromise between parsimony and fit [46]. The rate of decay of correlation between points (ϕ) with distance and the variance of the spatial process (σ2) were also recorded. The form of these models is shown in Additional File 2.
Predictions at non-sampled locations (defined over a regular 5 × 5 km grid overlaying the entire country) were made using the spatial.unipred function in WinBUGS which solves the model equation at each prediction location given the values of each covariate at the prediction location and the distance between prediction locations and observed data locations. Coefficients and model diagnostics were estimated using Markov Chain Monte Carlo (MCMC) simulations. The posterior probability distributions were used to classify prediction points to an endemicity class. Probability of class membership was computed as an additional measure to identify areas of high model uncertainties. For presentation purposes prediction maps from the best-fit model were combined for both zones. Continuous and categorical representations of predicted prevalence and probability maps were produced. The categorical classes of Pf PR selected were 0–<5% (low risk); 5–39% (medium risk); and ≥40% (high risk) and are based on a review of endemicity classification that would be most suitable as a guides for the likely impact of existing interventions [47].
Model validation
A spatially de-clustered random sampling strategy was implemented to generate validation sets that could be considered spatially representative of the prediction space. Thiessen polygons, which enclose the area closest to a given point, were defined around each survey location. A 10% sample or a minimum of 30 survey locations (whichever was larger) were then drawn randomly for the north and the south with each data point having a probability of selection proportional to the area of its Thiessen Polygon. This meant data located in densely surveyed regions had a lower probability of selection than those in sparsely surveyed regions [48]. The Bayesian geostatistical models were then repeated without the validation dataset. Predicted Pf PR values from the Bayesian geostatistical models were compared to actual Pf PR values observed at the validation locations using the mean error (ME), mean absolute error (MAE) and the area under the curve (AUC) of the receiver operating characteristic (ROC). ME is a measure of the bias of predictions (the overall tendency to over or under predict) whilst MAE is a measure of overall precision (the average magnitude of error in individual predictions) and AUC is a measure of discriminatory ability of predictions with respect to a true prevalence threshold (observed endemicity classes). AUC values greater than 0.9 indicate excellent discrimination; >0.7 moderate discrimination; >0.5 poor discrimination; and <0.5, the model does not discriminate any more successfully than random allocation of test status [49, 50].
Ethical approval
Ethical approval was provided through permission by the Ministry of Health Somalia, Transitional Federal Government of Somalia Republic, Ref: MOH/WC/XA/146./07, dated 02/02/07. Informed verbal consent was sought from all participating households and individuals.
Results
Sample description
A total of 500 independent community data locations with sample size ≥ 40 were assembled from the two survey sources (Table 1). Of these, 48 (9.6%) communities with sample size ≥ 40 could not be spatially positioned and were excluded from the analysis. Of the remaining 452 survey locations, 115 (25%) were located in the north and 337 (75%) in the south (Table 1 and Figure 1). Two locations in the north and one in the south were detected as outliers (Table 1 and Figure 2). The mean Pf PR of the data, excluding the outliers, was 2.8% (95% CI: 2.1–4.6, n = 10,468) for the north and 11.4% (95% CI: 10.4–14.2, n = 20,011) for the south.
Non-spatial bivariate and multivariate analysis of covariates
Both minimum and maximum temperatures exhibited non-linear relationships with Pf PR and were dichotomized at the median. No pairs of covariates demonstrated collinearity. During the non-spatial bivariate logistic regression analysis EVI, precipitation, maximum and minimum temperature, distance to water and survey month all displayed a highly significant association with Pf PR and met the initial entry criteria for the non-spatial multivariate logistic models for both the north and south (Table 2). Minimum rather than maximum temperature was selected for inclusion. When the selected variables were examined together in the multivariate model, EVI was not significantly associated with Pf PR in the north (p = 0.223) or the south (p = 0.395) (Table 2). Excluding EVI and maximum temperature, all remaining variables were entered into the multivariate Bayesian geostatistical model (Table 3).
Bayesian geostatistical models
North
The Bayesian geostatistical model without covariates in the north had σ2 (variance of spatial process) with a posterior median of 4.35 (95% credible interval (CI): 2.71, 7.14); ϕ (rate of decay of spatial correlation) of 8.90 (95% CI: 3.11, 12.75); a DIC value (measure of model fit) of 326; a ME (measure of model bias) of 3.83% Pf PR; and a MAE (measure of model precision) of 4.12% Pf PR (Table 3). The results of the multivariate Bayesian geostatistical model showed that none of the selected covariates remained significant (odds 95% CI included 1) after accounting for spatial correlation (Table 3). The DIC of the multivariate model was 323 and only marginally lower than that of the model without covariates, implying that the inclusion of the covariates did not improve overall model fit in the north. However, the covariates did account for some of the spatial variation in the data with spatial variance (σ2) decreasing from 4.35 to 3.70 (Table 3). Although the model with covariates exhibited lower bias (ME = 2.56% Pf PR) it also had marginally lower precision (MAE = 4.75% Pf PR) compared to the model without covariates. AUC values were similar for both models and indicated acceptable overall fit for endemicity class <5% Pf PR (AUC values > 0.70) but less so for endemicty class 5–39% Pf PR (AUC values of < 0.70). There were insufficient data points in the validation set to compute AUC values for the endemicity class ≥ 40% Pf PR (Table 3).
South
In the south the posterior median variance of the spatial process for the model without covariates was 7.14 (95% Bayes CI: 5.00, 8.76) and that of the rate of spatial decay parameter was 4.79 (95% Bayes CI: 2.11, 6.79). For the model with covariates the month of survey, annual average maximum temperature and precipitation all remained significant explanatory factors for Pf PR (Table 3). Odds of P. falciparum infection were higher in March (OR: 4.06, 95% CI 2.20–7.63) relative to February; and with increasing precipitation (OR: 1.41, 1.07–1.94). Higher minimum temperatures (OR: 0.83, 0.67–0.96) and a survey month of November relative to February (OR 0.48, 0.23–0.96) both reduced the odds of P. falciparum infection (Table 3). The inclusion of the covariates improved model fit with DIC of 1,429 compared to 1,454 for the model without covariates. There were no clear differences, however, between the models with and without covariates in the other parameters of model assessment with values of ME (3.65% vs 4.14% Pf PR); MAE (5.00% vs 5.06% Pf PR) and AUC values (<5% Pf PR: 0.91 vs 0.87; 5–39% Pf PR: 0.81 vs 0.78; ≥ 40% Pf PR: 0.51 vs 0.56). Similar to the multivariate model in the south, most of the spatial residual variation remained unexplained by the covariates.
Overall, the models for the south (with or without covariates) had higher spatial variances and spatial autocorrelation occurred over larger distances compared to the north (Table 3). In addition, models in the south exhibited better model fit with AUC values higher across all endemicity classes probably due to greater availability and better distribution of data in this zone (Figure 2).
Predicted (posterior median) Pf PR maps
To maintain consistency for comparison, and because the inclusion of the covariates did account for some degree of spatial variation in the Pf PR data, the predictions based on the multivariate geostatistical models were retained for both zones (Figures 3a and 3b). Point estimates of Pf PR (based on the posterior median) for the prediction locations ranged from 0–9% (median = 0%) in the north. The majority of the area in this zone had predicted a Pf PR of <5% with a small number of locations in Puntland and on the south-western border between Somaliland and Ethiopia having Pf PR of >5–9% (Figure 3b). In the south, point estimates of Pf PR for prediction locations ranged from 0–52% (median 5%), with high Pf PR locations occurring in the densely populated farmlands between the Juba and Shabelle rivers (Figure 3b). The lower and upper 95% credible intervals posterior median Pf PR are shown in Additional File 3. Interestingly, predicted Pf PR was lower along the two rivers, particularly the Shabelle River, compared to the area in between. Overall, predictions of endemicity class membership in the north were associated with lower probabilities compared to those in the south indicating a higher degree of model uncertainty (Figure 3c).

Maps of north and south of Somalia showing: a) posterior median Pf PR; b) endemicity classes based on the posterior probability of Pf PR class membership Pf PR; c) probability that a prediction location is correctly classified to an endemicity class: <5%; 5–39%; and ≥40% Pf PR. Probabilities < 0.33 are considered no better than chance class assignment. In Somalia probabilities were all ≥ 0.45.
Discussion
There has been little historical description of the basic epidemiology of malaria transmission in Somalia. In 2002, an application was made to and successfully approved by the GFATM to support the funding of a suite of interventions and strategies managed by a consortium of non-government and governmental agencies across the three main zones of Somalia [51]. This application, similar to other successful applications and RBM policies in neighbouring, higher-intensity transmission countries of Kenya [52], Tanzania [53] and Uganda [54] involved a monitoring & evaluation component to investigate intervention coverage and P. falciparum infection rates. In Somalia rapid, sample malaria intervention and parasitological surveys of communities have now become part of a routine component of rolling nutritional surveillance surveys across the country [55]. Consequently, despite being a country without a functioning research capacity and a fragile health system, Somalia is now one of the 87 P. falciparum endemic countries worldwide with the largest series of infection prevalence data [56, 57].
Simple summaries of the data suggest that large parts of the country, particularly in the north, have very low human infection prevalence (Table 1). These summaries, however, mask spatial heterogeneities in risk that are important for better targeting of interventions and maintaining aggressive surveillance. A Bayesian geostatistical approach to predict Pf PR throughout Somalia is used here. In the north, the inclusion of the survey and environmental covariates appeared not to make a significant difference to model fit, while in the south they improved the model fit. Predictions of endemicity class membership made in the north were associated with lower prediction probabilities and generated generally lower AU-ROC values (Table 3 & Figure 3c). This greater prediction uncertainty in the north is due largely to the comparatively fewer empirical data points compared to the south (Figure 2). This disparity was essentially driven by the population distribution: approximately 65% of Somalia's population live in the South and communities in the North are more scattered in isolated settlements [58].
Although the environmental covariates selected for inclusion in the Bayesian geostatistical model were significantly associated with Pf PR when examined in the non-spatial multivariate model (Tables 2 &3), none remained significant when spatial correlation was accounted for in the north and only precipitation and temperature remained significant in south. Overall the inclusion of these covariates accounted for a relatively small proportion of spatial variation suggesting that other unmeasured factors might be influencing the spatial distribution of malaria prevalence. These factors might include proximity to artificial breeding sites such as wells, dams, boreholes and seasonal streams and/or the use of interventions to prevent malaria at the household level. It has recently been demonstrated that in southern Somalia, the use of insecticide treated nets (ITN) reduced the prevalence of infection by as much as 54% [30]. Mapping the household or community levels of ITN use at high spatial resolutions is not currently feasible at a national scale. Similarly, the mapping of fluctuating, localized vector breeding sites would require very detailed spatial reconnaissance and infection mapping at finer scales than is currently possible using public domain covariate data at national scales. Furthermore, communities where sample sizes were less than 40, most of which could not be geo-located, were excluded from the analysis and these might have resulted in information loss for some areas of Somalia. Although the difference, in terms of mean parasite prevalence, was minimal between the excluded and included surveys, future analysis should include all data regardless of sample sizes given the Bayesian analytical approach implicitly adjusts for sample size.
Despite the constraints described above, the use of Bayesian geostatistics to model Pf PR does provide a valuable method to define sub-national spatial variation in prevalence, and a baseline against which future changes in prevalence can be quantified intervention coverage expands. Under such a scenario the value of the environmental covariates might be expected to wane further, particularly in areas of very low transmission intensity where the environment currently supports homogenously low transmission conditions. The similar levels of performance observed between the univariate and multivariate models for the north of Somalia may be evidence of this view. In addition, the relatively higher coverage of ITN among the communities closest to the two rivers in the south might explain the lower predicted prevalence in their immediate vicinity consistent with the observational data and reported effectiveness of ITN [30].
Population density or a derived categorisation of urbanisation, with known influences on malaria transmission [59, 60], would have been a worthy candidate covariate for testing in this study and in determining accurately the population at risk against varying malaria endemicity. However, the reliability of settlement and population data in Somalia is highly questionable. The last national census was undertaken in 1971 and the displacement and migration over the last 20 years of civil unrest has been substantial. Development agencies and non-governmental agencies working in Somalia continue to update a semi-quantitative database of settlement locations and population counts but its fidelity is unknown. The absence of an accurate national census also hampers the linkage of spatial malaria risk to populations-exposed to risk. Notwithstanding the precision and scale of calculating populations at risk, aggregated district-level estimates of population in 2004 across the 120 districts of Somalia have been used and assigned each district the dominant Pf PR risk class. From these numbers it can be estimated that approximately 75% of Somalia's estimated 7.4 million people live in areas that support unstable or very low Pf PR (0–5%) transmission and less than 0.1% live in areas classified as high, intense transmission (Pf PR > 40%). Areas of low Pf PR include many communities where infection prevalence was observed as zero (Table 1). In these locations it is assumed that these observations represent a statistical zero (i.e. resulting from a limited sample in areas of very low transmission) rather than implying a true absence of infection risk [56]. This is important to highlight because routine sample surveys in such areas demand considerably larger samples [45, 61] or the use of serological markers of parasite exposure [62] to truly exclude the possibility of transmission.
In communities exposed to low Pf PR, such as the majority of the population in Somalia, the risk of disease is low and spread across all age-groups. These are fundamentally different epidemiological conditions to areas of high transmission where functional immunity is developed early in life and a higher disease burden is experienced in young children and pregnant women [63–66]. Tailoring the existing intervention recommendations in the Somalia National Malaria Strategy [67] to the spatial transmission patterns shown in Figure 3 will be a challenge to the agencies providing malaria control services nationwide.
Conclusion
The use of routine, nationwide surveillance of infection prevalence is key to monitoring the changing epidemiology of malaria in all countries scaling up coverage of malaria preventative strategies. Including RDTs in on-going community-based health surveillance is a cost-effective means of assembling this information. The use of geostatistical methods can help focus surveillance efforts and define those areas where uncertainty exists, guiding future sampling [49, 68]. Coupled with better estimates of where people live, these should provide the basis for informed estimates of disease burden [63] and how these might change with changing infection-risk exposure. Somalia has a range of political and economic barriers that might limit the success of a strategic, epidemiologically driven malaria control programme. It has been possible to demonstrate, however, that the foci of greatest disease risk are predominantly concentrated in one area in the South and that infection risks are very low in the northern reaches of the country. Moreover, although the density of survey sites and hence the uncertainty of the modelled output varies spatially, also it has been demonstrated that, despite constant civil disturbance, routine survey data can be assembled to inform strategic decision making. Finally, areas where model uncertainties are greatest, predominantly in the north of the country, should be the focus of any future parasitological surveys to improve further the precision of the prevalence maps.
Abbreviations
- AIC:
-
Akaike Information Criterion
- AUC-ROC:
-
Area under the curve of the receiver operating characteristic
- DIC:
-
Deviance Information Criterion
- EVI:
-
Enhanced Vegetation Index
- FAO/FSAU:
-
Food Agricultural Organization-Food Security Analysis Unit (FSAU)
- GFATM:
-
Global Fund to Fight Aids TB and Malaria
- ITN:
-
Insecticide treated nets
- MAE:
-
Mean absolute error
- MAP:
-
The Malaria Atlas Project
- MCMC:
-
Markov Chain Monte Carlo
- ME:
-
Mean Error
- MODIS:
-
Moderate Resolution Imaging Spectroradiometer
- Pf PR:
-
Plasmodium falciparum parasite rate
- RDT:
-
Rapid Diagnostics Test
- SSA:
-
sub-Saharan Africa
- UNICEF:
-
United Nations Children Fund
- WHO:
-
World Health Organization.
References
Snow RW, Marsh K, Le Sueur D: The need for maps of transmission intensity to guide malaria control in Africa. Parasitol Today. 1996, 12: 455-457. 10.1016/S0169-4758(96)30032-X.
Hay SI, Snow RW: The Malaria Atlas Project: developing global maps of malaria risk. PLoS Med. 2006, 3 (12): e473-10.1371/journal.pmed.0030473.
Lysenko AY, Semashko IN: Geography of malaria: a medico-geographic profile of an ancient disease. Medicinskaja Geografija. Edited by: AW L. 1968, Moscow , Academy of Sciences, 146-
Omumbo JA, Hay SI, Goetz SJ, Snow RW, Rogers DH: Updating historical maps of malaria transmission intensity in East Africa using remote sensing. Photogramm Eng Rem Sens. 2002, 68 (2): 161-166.
Craig MH, Snow RW, le Sueur D: A climate-based distribution model of malaria transmission in Sub-Saharan Africa. Parasitol Today. 1999, 15: 105-111. 10.1016/S0169-4758(99)01396-4.
Kiszewski A, Mellinger A, Spielman A, Malaney P, Sachs SE, Sachs J: A Global index representing the stability of malaria transmission. Am J Trop Med Hyg. 2004, 70 (5): 486-498.
Rogers DJ, Randolph SE, Snow RW, Hay SI: Satellite imagery in the study and forecast of malaria. Nature. 2002, 415: 710-715. 10.1038/415710a.
Brooker S, Leslie T, Kolaczinski K, Mohsen E, Mehboob N, Saleheen S, Khudonazarov J, Freeman T, Clements A, Rowland M, Kolaczinski J: Spatial epidemiology of Plasmodium vivax, Afghanistan. Emerg Infect Dis. 2006, 12: 1600-1602.
Craig MH, Sharp BL, Mabaso ML, Kleinschmidt I: Developing a spatial-statistical model and map of historical malaria prevalence in Botswana using a staged variable selection procedure. Int J Health Geogr. 2007, 6: 44-10.1186/1476-072X-6-44.
Gemperli A, Kleinschmidt I, Bagayoko M, Lengeler C, Smith T: Spatial patterns of infant mortality in Mali: The effect of malaria endemicity. Am J Epidemiol. 2004, 159: 64-72. 10.1093/aje/kwh001.
Gemperli A, Sogoba N, Fondjo E, Mabaso M, Bagayoko M, Briet OJ, Anderegg D, Liebe J, Smith T, Vounatsou P: Mapping malaria transmission in West and Central Africa. Trop Med Int Health. 2006, 11 (7): 1032-1046. 10.1111/j.1365-3156.2006.01640.x.
Gemperli A, Vounatsou P, Sogoba N, Smith T: Malaria mapping using transmission models: application to survey data from Mali. Am J Epidemiol. 2006, 163 (3): 289-297. 10.1093/aje/kwj026.
Gosoniu L, Vounatsou P, Sogoba N, Smith T: Bayesian modelling of geostatistical malaria risk data . Geospat Health. 2006, 1 (1): 127-39.
Kazembe LN, Kleinschmidt I, Holtz TH, Sharp BL: Spatial analysis and mapping of malaria risk in Malawi using point-referenced prevalence of infection data. Int J Health Geogr. 2006, 5: 41-10.1186/1476-072X-5-41.
Kleinschmidt I, Omumbo J, Briet O, van de Giesen N, Sogoba N, Mensah NK, Windmeijer P, Moussa M, Teuscher T: An empirical malaria distribution map for west Africa. Trop Med Int Health. 2001, 6 (10): 779-786. 10.1046/j.1365-3156.2001.00790.x.
Omumbo JA, Hay SI, Snow RW, Tatem AJ, Rogers DJ: Modelling malaria risk in East Africa at high-spatial resolution. Trop Med Int Health. 2005, 10 (6): 557-566. 10.1111/j.1365-3156.2005.01424.x.
Snow RW, Gouws E, Omumbo J, Rapuoda B, Craig MH, Tanser FC, le Sueur D, Ouma JH: Models to predict the intensity of Plasmodium falciparum transmission: applications to the burden of disease in Kenya. Trans R Soc Trop Med Hyg. 1998, 92: 601-606. 10.1016/S0035-9203(98)90781-7.
SACB: Strategic framework in support of the health sector in Somalia. 2000, Developed at the SACB health strategy development workshop, Nakuru
GFATM: GFATM Round 6 Somalia project proposal 2006. [http://www.theglobalfund.org/search/docs/6SOMM_1418_0_full.pdf]
Wilson DB: Malaria in British Somaliland. East African Medical Journal. 1949, 26 (10): 1-9.
Ilardi L, Sebastiani A, Leone F, Madera A, Bile MK, Shiddo SC, Mohammed HH, Amiconi G: Epidemiological study of parasitic infections in Somali nomads. Trans Roy Soc Trop Med H. 1987, 81: 771-772. 10.1016/0035-9203(87)90027-7.
Warsame M, Lebbad M, Ali S, Wernsdorfer WH, Bjorkman A: Susceptibility of Plasmodium falciparum to chloroquine and mefloquine in Somalia. Trans R Soc Trop Med Hyg. 1988, 82: 202-204. 10.1016/0035-9203(88)90409-9.
Warsame M, Perlmann H, Ali S, Hagi H, Farah S, Lebbad M, Björkman A: The seroreactivity against Pf 155 (RESA) antigen in villagers from a mesoendemic area in Somalia. Trop Med Parasitol. 1989, 40: 412-414.
Choumara R: Notes sur le paludisme au Somaliland. Rivista di Malariologia. 1961, 40: 9-34.
Kamal M: Entomological surveillance in Somalia. Consultancy report for WHO Somalia. 2007
Mouchet J, Carnevale P, Coosemans M, Julvez J, Manguin S, Richard-Lenoble D, Sircoulon J: Biodiversité du Paludisme dans le Monde. 2004, UK , John Libbey, Eurotext, pp428:
WHO-Somalia: National malaria prevalence survey - Somalia 2005: summary of findings from the North East Zone. 2005
WHO-Merlin: National Malaria Prevalence Survey Somalia January-February 2005. 2005
FSAU: FSAU Project background. [http://www.fsausomali.org/index.php@id=3.html]
Noor AM, Moloney G, Borle M, Fegan GW, Shewchuk T, Snow RW: The use of mosquito nets and the prevalence of Plasmodium falciparum infection in rural South Central Somalia. PLoS One. 2008, 3 (5): e2081-10.1371/journal.pone.0002081.
WHO: Somalia Standard Treatment Guidelines and Training Manual on Rational Management and Use of Medicines at the Primary Health Care Level, Second Edition. 2008
Guerra CA, Hay SI, Lucioparedes LS, Gikandi PW, Tatem AJ, Noor AM, Snow RW: Assembling a global database of malaria parasite prevalence for the Malaria Atlas Project. Malaria J. 2007, 6: 17-10.1186/1475-2875-6-17.
Jovani R, Tella JL: Parasite prevalence and sample size: misconceptions and solutions. Trends Parasitol. 2006, 22: 214-218. 10.1016/j.pt.2006.02.011.
Microsoft: Microsoft Encarta version 16.0.0.0610. 2006, Microsoft Corporation
University of California : Alexandria Digital Library, University of California, USA. [http://www.alexandria.ucsb.edu]
FAO-SWALIM: FAO-SWALIM Databases. [http://www.faoswalim.org/resource_center/geonetwork/link.php?id=22]
Tatem AJ, Goetz SJ, Hay SI: Terra and Aqua: new data for epidemiology and public health. Int J Appl Earth Obs Geoinform. 2004, 6: 33-46. 10.1016/j.jag.2004.07.001.
Scharlemann JP, Benz D, Hay SI, Purse BV, Tatem AJ, Wint GR, Rogers DJ: Global data for ecology and epidemiology: a novel algorithm for temporal Fourier processing MODIS data. PLoS One. 2008, 9: e1408-10.1371/journal.pone.0001408.
WORLDCLIM: WORLDCLIM. [http://www.worldclim.org/download.htm]
Hijmans RJ, Cameron SE, Parra JL, Jones PG, Jarvis A: Very high resolution interpolated climate surfaces for global land areas. Intl J Climatology. 2005, 25: 1965-1978. 10.1002/joc.1276.
FAO-Africover: FAO-Africover. [http://www.africover.org]
Lehner B, Döll P: Development and validation of a global database of lakes, reservoirs and wetlands. J Hydrol. 2004, 296: 1-22. 10.1016/j.jhydrol.2004.03.028.
Diggle P, Moyeed R, Rowlingson B, Thompson M: Childhood malaria in the Gambia: a case-study in model-based geostatistics. Appl Stat. 2002, 51: 493-506.
Best N, Richardson S, Thomson A: A comparison of Bayesian spatial models for disease mapping. Stat Methods Med Res. 2005, 14 (35-59):
Thomas A, Best N, Lunn D, Arnold R, Spiegelhalter D: GeoBUGS User Manual version 1.2. 2004
Spiegelhalter D, Thomas A, Best N, Lunn D: WinBUGS user manual. 2003
Hay SI, Smith DL, Snow RW: Measuring malaria endemicity from intense to interrupted transmission. Lancet Infect Dis. 2008, 8: 369-378. 10.1016/S1473-3099(08)70069-0.
Isaacs EH, Srivastava RM: Applied geostatistics. 1989, Oxford University Press, 561-
Clements ACA, Lwambo NJS, Blair L, Nyandindi U, Kaatano G, Kinung'hi S, Webster JP, Fenwick A, Brooker S: Bayesian spatial analysis and disease mapping: tools to enhance planning and implementation of a schistosomiasis control programme in Tanzania. Trop Med Int Health. 2006, 11: 490-503. 10.1111/j.1365-3156.2006.01594.x.
Fawcett T: An introduction to ROC analysis. Pattern Recogn Lett. 2006, 27: 861-874. 10.1016/j.patrec.2005.10.010.
GFATM: 2002. [http://www.theglobalfund.org/search/docs/2SOMM_134_0_full.pdf]
Ministry_of_Health_Government_of_Kenya: National Malaria Strategy: 2001-2010. 2001, Division of Malaria Control, Ministry of Health, Government of Kenya
Ministry_of_Health_The_United_Republic-of_Tanzania: National Malaria Medium Term Strategic Plan, 2002-2007. The United Republic of Tanzania, Ministry of Health
Uganda_Ministry_of_Health: Uganda_Ministry_of_Health, National Health Policy. [http://www.health.go.ug/docs/NationalHealthPolicy.pdf]
FSAU: FSAU Nutrition. [http://www.fsausomali.org/index.php@id=41.html]
Guerra CA, Gikandi PW, Tatem AJ, Noor AM, Smith DL, Hay SI, Snow RW: The limits and intensity of Plasmodium falciparum transmission: Implications for malaria control and elimination worldwide. PLoS Med. 2008, 5 (2): e38-
MAP: Malaria Atlas Project. [http://www.map.ox.ac.uk]
FSAU-SOMALIA: FSAU-SOMALIA. [http://www.fsausomali.org/uploads/Other/188.pdf]
Hay SI, Guerra CA, Tatem AJ, Atkinson PM, Snow RW: Urbanization, malaria transmission and disease in Africa. Nature Rev. 2005, 3: 81-90. 10.1038/nrmicro1069.
Omumbo JA, Guerra CA, Hay SI, Snow RW: The influence of urbanisation on measures of Plasmodium falciparum infection prevalence in East Africa. Acta Trop. 2005, 93: 11-21. 10.1016/j.actatropica.2004.08.010.
Pull JH: Malaria surveillance methods, their uses and limitations. Am J Trop Med Hyg. 1972, 21: 651-657.
Drakeley CJ, Corran PH, Coleman PG, Tongren JE, McDonald SLR, Carneiro I, Malima R, Lusingu J, Manjurano A, Nkya WMM, Lemnge MM, Reyburn H, Cox J, Riley EM: Estimating medium- and long-term trends in malaria transmission by using serological markers of malaria exposure. PNAS. 2005, 102: 5108-5113. 10.1073/pnas.0408725102.
Snow RW, Guerra CA, Noor A, Myint HY, Hay SI: The global distribution of clinical episodes of Plasmodium falciparum malaria. Nature. 2005, 434: 214-217. 10.1038/nature03342.
Snow RW, Marsh K: The consequences of reducing transmission of Plasmodium falciparum in Africa. Adv Parasitol. 2002, 52: 235-264.
Snow RW, Omumbo JA, Lowe B, Molyneux CS, Obiero JO, Palmer A, Weber MW, Pinder M, Nahlen BL, Obonyo CO, Newbold CI, Gupta S, Marsh K: Relation between severe malaria morbidity in children and level Plasmodium falciparum transmission in Africa. Lancet. 1997, 349: 1650-1654. 10.1016/S0140-6736(97)02038-2.
Trape JF, Rogier C: Combating malaria morbidity and mortality by reducing transmission. Parasitol Today. 1996, 12 (6): 236-240. 10.1016/0169-4758(96)10015-6.
Capobianco E: Somalia National Malaria Control Strategy 2005 - 2010. Edited by: UNICEF . 2005
Brooker S, Kabayereine NB, Tukahebwa EM, Kazibwe F: Spatial analysis of the distribution of intestinal nematode infections in Uganda. Epidemiol Infect. 2004, 132 (6): 1065-71.
Acknowledgements
The authors are grateful to the WHO-MERLIN and FAO/FSAU survey team for their invaluable supervision and support during the field surveys and subsequent data entry and cleaning and Bruno Moonen of MERLIN specifically for helping with training for the parasite survey. We thank Priscilla Gikandi and Victor Alegana for additional data cleaning and geo-referencing. We are also grateful to Anand Patil and Andy Tatem for statistical and GIS advise and to Simon Brooker, Carlos Guerra and Emelda Okiro for their comments on the manuscript.
Funding for the WHO-MERLIN 2005 surveys were provided by the UN Trust Fund for Human Security and the GFATM. FAO/FSAU funded training of assessment teams, data collection, paid enumerators and data entry clerks for the 2007 surveys. The FAO/FSAU nutrition surveillance project is funded primarily by OFDA-USAID and receives support from UNICEF, SIDA and EC for conducting nutrition assessments in Somalia. RDTs and anti-malarial treatment were provided by UNICEF through GFATM funding (SOM-202-G01-M-00). AMN is supported by the Wellcome Trust as a Research Training Fellow (#081829). SIH is supported by the Wellcome Trust as Senior Research Fellow (#079091). RWS is supported by the Wellcome Trust as Principal Research Fellow (#079081). AMN, SIH and RWS acknowledge the support of the Kenyan Medical Research Institute. The funders did not have a role in study design, data collection and analysis, decision to publish, or preparation of manuscript. This work forms part of the output of the Malaria Atlas Project (MAP: http://www.map.ox.ac.uk), principally funded by the Wellcome Trust, U.K.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors' contributions
AMN was responsible for data cleaning, analysis, interpretation and production of the final manuscript and revisions, ACC contributed to the data analysis, interpretation and production of final manuscript, PWG contributed to the data analysis, interpretation and production of final manuscript, GM was responsible for the study design, supervision of data collection, cleaning and contributed to the preparation of the final manuscript, MB provided the necessary interface with community leaders, and the Ministry of Health for approval and was responsible for the data collection, cleaning and contributed to the preparation of the final manuscript, TS assisted in the survey design, supported the field investigations, provided the interface with local ministry of health and helped in the preparation of the manuscript, SIH contributed to overall scientific direction interpretation and preparation of the final manuscript and revisions, RWS was responsible for overall scientific management, analysis, interpretation and preparation of the final manuscript and revisions.
Electronic supplementary material
12936_2008_634_MOESM1_ESM.doc
Additional File 1: A method for identifying outliers. Statistical outliers were identified using a spatial filtering algorithm that implemented the following procedure in turn for each datum p(x i ) at location x i . (DOC 290 KB)
12936_2008_634_MOESM2_ESM.doc
Additional File 2: The Bayesian model form developed in WinBUGS without covariates. The univariate Bayesian geostatistical models (DOC 145 KB)
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Noor, A.M., Clements, A.C., Gething, P.W. et al. Spatial prediction of Plasmodium falciparum prevalence in Somalia. Malar J 7, 159 (2008). https://doi.org/10.1186/1475-2875-7-159
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-7-159