
Abstract
Background
Monitoring local malaria transmission intensity is essential for planning evidence-based control strategies and evaluating their impact over time. Anti-malarial antibodies provide information on cumulative exposure and have proven useful, in areas where transmission has dropped to low sustained levels, for retrospectively reconstructing the timing and magnitude of transmission reduction. It is unclear whether serological markers are also informative in high transmission settings, where interventions may reduce transmission, but to a level where considerable exposure continues.
Methods
This study was conducted through ongoing KEMRI and CDC collaboration. Asembo, in Western Kenya, is an area where intense malaria transmission was drastically reduced during a 1997–1999 community-randomized, controlled insecticide-treated net (ITN) trial. Two approaches were taken to reconstruct malaria transmission history during the period from 1994 to 2009. First, point measurements were calculated for seroprevalence, mean antibody titre, and seroconversion rate (SCR) against three Plasmodium falciparum antigens (AMA-1, MSP-119, and CSP) at five time points for comparison against traditional malaria indices (parasite prevalence and entomological inoculation rate). Second, within individual post-ITN years, age-stratified seroprevalence data were analysed retrospectively for an abrupt drop in SCR by fitting alternative reversible catalytic conversion models that allowed for change in SCR.
Results
Generally, point measurements of seroprevalence, antibody titres and SCR produced consistent patterns indicating that a gradual but substantial drop in malaria transmission (46-70%) occurred from 1994 to 2007, followed by a marginal increase beginning in 2008 or 2009. In particular, proportionate changes in seroprevalence and SCR point estimates (relative to 1994 baseline values) for AMA-1 and CSP, but not MSP-119, correlated closely with trends in parasite prevalence throughout the entire 15-year study period. However, retrospective analyses using datasets from 2007, 2008 and 2009 failed to detect any abrupt drop in transmission coinciding with the timing of the 1997–1999 ITN trial.
Conclusions
In this highly endemic area, serological markers were useful for generating accurate point estimates of malaria transmission intensity, but not for retrospective analysis of historical changes. Further investigation, including exploration of different malaria antigens and/or alternative models of population seroconversion, may yield serological tools that are more informative in high transmission settings.
Similar content being viewed by others


Explore related subjects
Discover the latest articles, news and stories from top researchers in related subjects.Background
Measuring local malaria transmission intensity is critical for estimating the magnitude of malaria disease burden, planning evidence-based control strategies and evaluating the impact of interventions [1–3]. Moreover, malaria control programmes would benefit from monitoring long-term changes in transmission intensity in order to adapt control strategies to evolving local conditions [4]. No consensus exists, however, on which methods are most appropriate for programmatic monitoring of malaria endemicity over time, as all current tools have drawbacks [2, 4]. Hospital-based surveillance records may be readily available, but are considered unreliable as experts estimate that fewer than 20% of malaria cases and deaths are reported to the formal health system [4–6]. Inaccuracies are further compounded by presumptive diagnosis at health centres, leading to overestimation of malaria cases among those individuals seeking care [6, 7]. Entomological inoculation rate (EIR), which describes the average rate at which individuals are bitten by infective mosquitoes, is the most direct indicator of malaria transmission intensity [8, 9]. Unfortunately, measuring EIR is difficult and labour-intensive [10], and estimates can lack precision due to small-scale spatial and/or temporal heterogeneity in mosquito distributions [9, 11, 12]. In addition, EIR overestimates force of infection, the number of new infections per person per unit time, due to heterogeneous biting by mosquitoes [13, 14]. Parasite prevalence, the proportion of individuals with detectable Plasmodium parasites, is another common metric of malaria risk. Parasite prevalence is not a measure of incidence, however, and its relationship with force of infection is complicated by super-infection and acquired immunity [15]. Furthermore, estimates of parasite prevalence can vary widely in areas of seasonal transmission, and are influenced by the method of parasite detection, timing of measurement during the course of infection and access to anti-malarial drugs [13, 16, 17].
Anti-malarial antibodies are markers of past infection that can help to elucidate temporal trends in transmission [18, 19]. Because antibodies are longer lasting compared to patent parasitaemia and the lifespan of infective mosquitoes, serological tools are potentially more sensitive and robust than parasite prevalence or EIR. Large-scale serological surveys have proven useful in the past for examining impacts of interventions that reduce malaria parasite exposure. During the Garki Project in northern Nigeria, antibody prevalence and levels reflected recent changes in malaria exposure. Antibody responses fell abruptly during the intervention phase of the study, but rebounded soon after the intensive intervention was stopped [20]. More recently, by fitting a reversible catalytic conversion model to age-stratified seroprevalence data, investigators have estimated seroconversion rates (SCRs) that are analogous to force of infection [16, 18]. SCRs generated from several locations in Africa [16, 21, 22], Asia [23] and the Pacific [24] have shown close correlation with independent measures of transmission intensity such as malaria incidence among infants and young children, as well as averaged parasite prevalence and EIR values.
Because serological markers provide information on cumulative exposure over time [25], they are particularly well suited for evaluating long-term transmission trends [16, 18]. Data from a single cross-sectional serological survey can, in theory, be used to generate a point estimate of the current force of infection as well as analyse historic changes in exposure to infection [16, 18]. Sero-epidemiological studies from Tanzania [21], Vanuatu [24], Equatorial Guinea [22], and Swaziland [26] have confirmed that historic reductions in local malaria transmission (e.g., due to successful control strategies) can be demonstrated by a significantly lower SCR among younger cohorts born after the intervention(s). In these cases, age-seroprevalence curves exhibited a ‘break point’ signalling the timing of the change in SCR without the need for comparison against a baseline survey. To date, studies employing this method to reconstruct the timing and magnitude of transmission reduction have come from areas where transmission has dropped to low, sustained levels [21, 22, 24, 26]. It is unclear whether these serological tools are informative for reconstructing long-term malaria trends in regions of high transmission, where interventions may reduce transmission, but to a level where considerable exposure continues.
The purpose of this study was to investigate the utility of serological markers of Plasmodium falciparum exposure for estimating force of malaria infection and detecting temporal changes in malaria risk over an extended period in a highly endemic setting. Asembo, in Western Kenya, has historically experienced intense malaria transmission year round [27]. A community-randomized, controlled insecticide-treated net (ITN) trial conducted from 1997 to 1999 drastically reduced malaria transmission [28, 29]. Following the trial, continued high ITN coverage [30], coupled with expanded malaria interventions and health system and socio-economic improvements, led to further reductions in malaria morbidity and mortality from the late 1990s to late 2000s [31]. Despite these gains, however, malaria transmission in Asembo remains high [31].
For this study, three antigens spanning a range of immunogenicities were selected in order to identify at least one marker with sensitivity appropriate for the transmission intensities observed in Asembo. Immune responses against circumsporozoite protein (CSP) are considered short-lived, as sporozoites from each infective bite are present in the blood in small numbers and for only a short duration [32]. For this reason, anti-CSP antibodies are likely to underestimate malaria endemicity in low transmission areas [25], but be sensitive in hyper- and holo-endemic settings [33, 34]. The blood-stage antigen merozoite surface protein-119 (MSP-119) exhibits moderate immunogenicity and has been useful for estimating malaria endemicity across a range of low, moderate, and high transmission settings in Africa [18, 35]. Apical membrane antigen-1 (AMA-1), a blood-stage antigen known to be highly immunogenic, elicits a long-lived immune response that may cause population antibody responses to saturate at moderate transmission levels [18].
Two approaches were taken to reconstruct malaria transmission history in Asembo. First, point measurements of serological responses were calculated at five time points between 1994 and 2009, covering the period before the ITN trial to roughly a decade after the trial, for comparison against traditional malaria indices (parasite prevalence and EIR). Point measurements were also compared between villages that received ITNs in 1997 vs 1999 to understand if serological responses would reflect small differences in the length of population protection under ITNs. Second, within individual post-ITN years, age-seroprevalence curves were examined to look retrospectively for an abrupt drop in SCR corresponding to the timing of the ITN trial.
Methods
This research was conducted through ongoing collaboration between the Kenya Medical Research Institute (KEMRI) and the Centers for Disease Control and Prevention (CDC).
Study site
Asembo is located on the northern shores of Lake Victoria in Siaya County, Western Kenya. This lowland rural area (elevation 3,700 m) has served as the site of several malaria epidemiology studies and has been described in detail [27, 28, 30]. During the early 1990s, parasite prevalence in children aged < five years was 70-80% year round [36]. Plasmodium falciparum accounted for >95% of all clinical malaria infections [27, 36]. Predominant malaria vectors in the region included Anopheles gambiae s.s., Anopheles funestus and Anopheles arabiensis, with estimated EIRs ranging from 60 to 300 infective bites per person per year [37, 38].
During the community-randomized trial carried out in Asembo from 1997 to 1999 [28], 40 of 79 villages were randomized to receive ITNs and the rest served as controls until 1999, after which they also received ITNs [29]. The two-year trial resulted in a 74% reduction in malaria force of infection [39] and >90% reduction in EIR [40] in intervention villages compared to control villages. After the trial, ITN coverage was maintained at high levels [30]. ITNs were replaced periodically, and were retreated with a pyrethroid formulation at six- to nine-month intervals by KEMRI/CDC through 2007 (J Gimnig, unpublished data). In addition, the Kenya Ministry of Health promoted scale-up of ITNs throughout this region, first through subsidized ITN distribution at antenatal clinics beginning in 2004, and later through a mass campaign distributing free long-lasting ITNs to all children aged < five years in 2006 [31].
Entomological inoculation rates
Data on the number of blood-fed An. gambiae s.s., An. arabiensis and An. funestus captured, the number of houses sampled and the number of residents per house, were obtained from prior studies to estimate annual EIRs. Household mosquito collections have been conducted in Asembo since 1993, but sampling methods and trapping techniques have varied depending on the particular study in place. Bed net traps were used to collect anophelines from 1993 to 1996 [27, 32]. From 1997 to 2001, entomological collections were made by pyrethrum spray catch (PSC) [30, 40, 41]. Indoor CDC light traps were employed during the period from 2002 to 2007 [42, 43]. Since 2008, mosquito collections have again been conducted using PSCs (J Gimnig, unpublished data). For all entomological collections, anophelines were identified, sorted by sex and abdominal status and dried in individual tubes for laboratory analysis. Mosquitoes were tested for sporozoite infection by enzyme-linked immunosorbent assay (ELISA) [44] and a subset of all specimens classified as An. gambiae s.l. was identified to sibling species (An. gambiae s.s. or An. arabiensis) by polymerase chain reaction (PCR) [45].
Parasite prevalence
Annual parasite prevalence for children aged one to five years was calculated using blood film data from past surveys [27, 30, 31]. During all surveys, finger-prick blood samples were collected onto slides, stained with Giemsa and then examined under a microscope for asexual P. falciparum parasites. Parasites were enumerated against 300 white blood cells (prior to 1996) or 500 white blood cells (since 1996). Individuals included in parasite prevalence calculations were restricted to those for whom serological specimens (see below) were also available.
Serological specimens
Serological analyses were conducted using banked samples collected in 1994, 2000, 2007, 2008 and 2009. Samples from infants less than one year of age were excluded in all years to limit confounding of test results by maternal antibodies. Samples from 1994 were collected from a subset of 15 villages in Asembo [27], whereas samples from later years were collected across the entire Asembo area [30, 43]. In 1994 and 2000, capillary blood samples were collected into tubes and centrifuged to separate serum [27, 30], which was stored at −80°C until used for ELISAs. Immediately prior to serological testing, serum was diluted 1/200 in reconstitution buffer (phosphate buffered saline with 0.05% Tween 20 [PBS-T] containing 0.1% sodium azide).
Specimens from 2007, 2008 and 2009 were collected as dried blood spots on filter paper [46] during annual surveys conducted within the KEMRI/CDC Health and Demographic Surveillance System [31, 43, 47]. A 3-mm blood spot was punched from each filter paper and antibodies were eluted in reconstitution buffer as previously described [21]. The reconstituted blood spot solution, equivalent to a 1/200 dilution of serum, was stored at 4°C until used for ELISAs.
Enzyme-linked immunosorbent assays
All samples (sera and reconstituted blood spots) were tested by ELISA [16, 18] for total IgG antibodies against recombinant P. falciparum AMA-1 (3D7; Biomedical Primate Research Center, Rijswijk, The Netherlands), MSP-119 (Wellcome strain; CTK Biotech, San Diego, CA, USA) and CSP (Gennova Biopharmaceuticals, Pune, India). Briefly, recombinant AMA-1 (0.4ug/mL), MSP-119 (0.2ug/mL) and CSP (1.6ug/mL) were coated onto Immunolon-4 microtiter plates (Thermo Fisher Scientific, Waltham, MA, USA). The following day, plates were washed in PBS-T, blocked with 1% milk powder (Marvel, UK) in PBS-T (PBS-T/milk), and then incubated with samples. All samples were tested in duplicate, with final serum dilutions at 1/2,000 for AMA-1, 1/1,000 for MSP-119 and 1/200 for CSP. Each ELISA plate also included blank wells (PBS-T/milk only) and a positive control dilution series (pooled sera from six hyperimmune individuals from the Kisumu Blood Bank). On the third day, unbound antibodies were removed by washing in PBS-T, samples were incubated with peroxidase-conjugated rabbit anti-human IgG antibody (Dako, Carpinteria, CA, USA) (1/5,000 in PBS-T) and then plates were developed by adding o-phenylenediamine dihydrochloride (OPD) substrate (Sigma-Aldrich, St Louis, MO, USA). OPD reactions were held in the dark and stopped using 2 M H2SO4 after 11 min for AMA-1 and MSP-119, and 16 min for CSP. Optical density (OD) was read immediately at 492 nm using a plate reader (Molecular Devices SpectraMAX 340 and SoftMax Pro 5.4.1 software, Sunnyvale, CA, USA).
Data management and statistical analysis
Duplicate OD values for each sample were imported into Microsoft Excel (Microsoft, Redmond, WA, USA), averaged and normalized against values from blank wells to adjust for background reactivity. Samples were excluded from analysis if duplicate ODs differed by over 50%. Titration curves were fit to the positive control dilution series on each plate in order to adjust sample OD values for plate-to-plate variation and allow for calculation of titres. Antibody titre was estimated using the formula: titre = dilution/[maximum OD/(OD test serum – minimum OD)-1]. Using a mixture model, cut-off values for seropositivity were determined separately for each antigen (AMA-1, MSP-1 and CSP) during each year (1994, 2000, 2007, 2008 and 2009) to avoid direct quantitative comparison of ELISA results from samples collected by different methods (serum vs dried blood spot). Briefly, OD values were fit by maximum likelihood as two Gaussian distributions [46] and the cut-off value was assigned as three standard deviations above the mean of the lower distribution.
To identify differences in seropositivity by sex, blood film result, or year in which the village received ITNs, logistic regression models were fit using PROC GENMOD in SAS 9.3 (SAS Institute, Cary, NC, USA). Age (continuous variable, cube root-transformed) and survey year were included to control for their effects, and models were adjusted for clustering of observations from the same household compound by incorporating an exchangeable correlation matrix.
Because data from 2000 were limited to children aged one to five years, a preliminary analysis was conducted to compare seroprevalence across the five time points specifically in this young age group. Year to year differences in the proportion of children seropositive were evaluated using Z-tests with Bonferroni correction for multiple comparisons. To calculate a measure analogous to SCR but using only data from this age group, linear regression models were fit, using median centile age as the predictor and centile seroprevalence as the outcome, to estimate the rate of increase in seroprevalence with age. This allowed for comparison of transmission intensity between years without making assumptions regarding missing older age groups. All regression lines were forced through the origin (intercept = 0) and regression coefficients were estimated in R version 3.2.0 (R Foundation for Statistical Computing, Vienna, Austria). Differences in geometric mean antibody titres (GMT) were also examined because antibody levels may respond more quickly to recent shifts in transmission than seroprevalence [22, 48]. To visualize distributions of antibody titres in more detail, reverse cumulative distribution plots were used, showing log10–transformed antibody titre on the X-axis and the percentage of individuals having the indicated antibody titre or higher on the Y-axis [49]. Differences in antibody titres between years were identified by Wilcoxon rank-sum test with Bonferroni correction.
To estimate population-wide SCRs in Asembo at each time point, data from all available age groups were used. Reversible catalytic conversion models were fit to age-stratified seroprevalence data using maximum likelihood in Stata 11 (StataCorp, College Station, TX, USA) [16, 18]. Seroreversion rates for each antigen were constrained for the Asembo population by first fitting a global model to aggregate data from all years. Individual models were then fit separately to datasets from each year to estimate year-specific SCRs. EIR equivalents (serology-based EIR estimates) were calculated from AMA-1 and MSP-119 results using previously developed log-log calibration curves that relate SCRs to EIR values [16, 18]. EIR equivalents could not be calculated from CSP SCRs because CSP calibration curves have not yet been developed.
Datasets from years after the ITN trial concluded were examined for temporal changes in force of infection by fitting alternative reversible catalytic conversion models in which the SCR was allowed to change at a single time point. The significance of each change was evaluated using a likelihood ratio test against the initial model with no change in SCR [16, 21].
Ethical review
Ethical approval for serological analyses was obtained from the KEMRI Ethical Review Committee and the CDC Institutional Review Board.
Results
Demographic data for persons sampled from Asembo are summarized in Table 1. Differences in study protocols led to variation in the number and age distribution of individuals sampled during each year. Individuals from 1994 included a higher proportion of females compared to other years (χ2 = 34.6, p < 0.001) because pregnant females were the only persons older than 15 years surveyed that year. When pregnant females were excluded in 1994, this difference was no longer observed. The proportion of individuals with positive blood films ranged from >80% in 1994 to 36% in 2007. No year to year differences were observed in the proportion of individuals residing in villages that received ITNs at the trial’s start in 1997 vs at the trial’s conclusion in 1999 (χ2 = 3.1, p = 0.533).
Across all years, the likelihood of individuals testing seropositive increased with age for all three antigens (AMA-1 OR = 6.0 [95% CI: 4.4-8.0], MSP-119 OR = 2.2 [95% CI: 1.9-2.5], CSP OR = 3.0 [95% CI: 2.5-3.5], p < 0.001 for all). Seropositivity was also associated with positive blood film for AMA-1 (OR = 3.7 [95% CI: 3.0-4.5], p < 0.001) and CSP (OR = 1.8 [95% CI: 1.4-2.3], p < 0.001), but not for MSP-119 (OR = 1.0 [95% CI: 0.8-1.2], p = 0.998). Females were more likely to be seropositive against MSP-119 (OR = 1.4 [95% CI: 1.1-1.7], p = 0.001), whereas sex had no effect for AMA-1 (OR = 1.1 [95% CI: 0.9-1.3], p = 0.540) or CSP (OR = 1.2 [95% CI: 1.0-1.4], p = 0.133). Whether an individual resided in a village that received ITNs in 1997 or 1999 had no impact on seropositivity against any of the three antigens (AMA-1 OR = 0.9 [95% CI: 0.7, 1.1], p = 0.352; MSP-119 OR = 1.0 [95% CI: 0.8-1.2], p = 0.834; CSP OR = 0.8 [95% CI: 0.7-1.1], p = 0.144).
Serological results for young children
Seroprevalence
Figure 1A shows seroprevalence among young children compared with parasite prevalence at each time point. AMA-1 exhibited the highest seroprevalence of the three antigens tested; within each year, AMA-1 seroprevalence was typically two- to four-fold greater than that for MSP-119 or CSP. AMA-1 seroprevalence fell between 1994 and 2000 (p < 0.001), and then again between 2000 and 2007 (p = 0.002). Seroprevalence against MSP-119 and CSP also decreased steadily from 1994 to 2007, but the year-to-year differences were not statistically significant (p > 0.013 for all [cut-off with Bonferroni correction]). This trend of falling seroprevalence began to reverse in 2008 for MSP-119 and in 2009 for AMA-1 and CSP, but none of these subsequent changes were statistically significant (p > 0.013 for all). Across the entire study period, AMA-1 seroprevalence values corresponded very closely to parasite prevalence values. Furthermore, proportionate changes in both AMA-1 and CSP seroprevalence (relative to baseline values from 1994) closely mirrored the pattern observed for parasite prevalence (Figure 1B). Proportionate changes in MSP-119 seroprevalence did not follow the pattern observed for parasite prevalence, particularly in 2008 and 2009.

Trends in seroprevalence compared with parasite prevalence. A) Seroprevalence (95% CI) and parasite prevalence (95% CI) were calculated for children aged one to five years in Asembo. B) Ratios of seroprevalence and parasite prevalence relative to baseline values from 1994.
To approximate seroconversion rates using only data from young children, linear regression coefficients (βs) were calculated to describe the increase in seroprevalence per year of age (Figure 2A). Overall, βs for each antigen exhibited similar patterns as seen for seroprevalence (Figure 1A). Proportionate changes in AMA-1 and CSP βs were similar to those observed for parasite prevalence, whereas proportionate changes in MSP-119 βs were not (Figure 2B). Within each year, no statistically significant difference in β was observed between individuals residing in villages that received ITNs in 1997 vs 1999 (Additional file 1).

Rate of increase in seroprevalence with age. A) Linear regression coefficients (95% CI) describing the increase in seroprevalence per year of age among children aged one to five years in Asembo. Regression coefficients were calculated to approximate seroconversion rates using only data from young children. B) Ratios of regression coefficients and parasite prevalence relative to baseline values from 1994.
Antibody levels
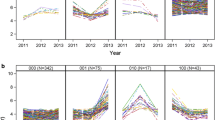
Geometric mean antibody titres for children one to five years of age are displayed in Figure 3A. Reverse cumulative distribution plots, showing the range of observed antibody titres on the X-axis and the proportion of individuals exhibiting each titre or higher on the Y-axis, are presented in Figures 3B-D. The magnitude of year-to-year change in antibody titres was greatest for AMA-1. In 2000, surprisingly, antibody titres against MSP-119 were higher in villages that received ITNs in 1997 (GMT = 25.4 [95% CI: 22.8-28.2]) compared with villages that received ITNs in 1999 (GMT = 19.3 [95% CI: 17.4-21.3]) (p >0.001). No differences were detected between villages receiving ITNs in 1997 vs 1999 for any other antigens. Antibody titres against all three antigens fell between 1994 and 2000 (p <0.001 for all antigens). For AMA-1, titres fell further in 2007 (p <0.001), exhibited no change in 2008 (p = 0.026 [cut-off with Bonferroni correction: p = 0.013]), and then subsequently increased in 2009 (p = 0.004). MSP-119 titres changed little between 2000 and 2007 (p = 0.148), but increased in 2008 (p <0.001) and then remained static in 2009 (p = 0.029). CSP titres did not change from 2000 to 2007 (p = 0.128), but increased in 2008 (p <0.001) and again in 2009 (p <0.001).

Trends in antibody titres. A) Geometric mean titres (95% CI) for children one to five years of age. Reverse cumulative distribution plots for: B) AMA-1, C) MSP-119 and D) CSP. Each plot shows antibody titres (log10-transformed) on the X-axis and the proportion of individuals exhibiting that titre or higher on the Y-axis.
Serological results for all age groups
Population SCRs
Results from reversible catalytic conversion models fit to data from all available age groups are presented in Figure 4. Seroreversion rates in the Asembo population were fixed at 0.050 yr−1 for AMA-1, 0.051 yr−1 for MSP-119 and 0.073 yr−1 for CSP, based on a preliminary model fit to data from all years. Consistent with the results from young children, population-wide immune responses were strongest against AMA-1. Year-specific SCRs were roughly an order of magnitude greater for AMA-1 than for MSP-119 and CSP across the entire study period. SCRs for all antigens were highest in 1994, before ITN introduction. Although concerns have been raised that anti-malarial antibody responses in pregnant women may differ systematically from those of the general population [50, 51], removing pregnant women from the 1994 analysis had no significant effect on SCRs (Additional file 2). All subsequent comparisons using the 1994 dataset include samples from pregnant women.

Trends in age-seroprevalence curves and seroconversion rates (SCRs). SCRs (95% CI) were estimated for the Asembo population by fitting reversible catalytic conversion models to data from all available age groups for: A) AMA-1, B) MSP-119 and C) CSP. D) Ratios of SCR and parasite prevalence relative to baseline values from 1994.
No statistical differences in SCRs were observed for individuals living in villages that received ITNs in 1997 vs 1999 (Additional file 3), so within each year, data from all villages were combined for analysis. For AMA-1, SCR fell dramatically between 1994 and 2000, and again between 2000 and 2007 (Figure 4A). AMA-1 SCR remained unchanged in 2008 and then increased significantly in 2009. For MSP-119, no change was observed between 1994 and 2000, but SCR fell significantly between 2000 and 2007 (Figure 4B). In 2008 and 2009, MSP-119 SCR rose slightly, but this trend was not statistically significant. SCRs for CSP decreased gradually between each time point from 1994 to 2008, before increasing again in 2009 (Figure 4C), but none of these changes were statistically significant. Proportionate changes in AMA-1 and CSP SCRs (relative to baseline values from 1994) correlated closely with the pattern observed for parasite prevalence (Figure 4D). Proportionate changes in MSP-119 SCR, on the other hand, were high compared to parasite prevalence in 2000, 2008, and 2009.
EIR equivalents
Figure 5A shows EIR equivalents estimated from AMA-1 and MSP-119 SCRs compared with EIR values previously measured in Asembo at the five time points [30] (J Gimnig, unpublished data). EIR equivalents based on AMA-1 showed greater variability over the study period compared to those based on MSP-119. Neither antigen, however, produced EIR equivalents that closely tracked observed EIRs, or proportionate changes in EIR values, over the study period (Figure 5B).

Entomological inoculation rates (EIRs) and EIR equivalents for Asembo. A) Observed EIRs are based on previously collected entomological data. EIR equivalents (95% CI) were estimated using AMA-1 and MSP-119 SCRs and previously developed log-log calibration curves. B) Ratios of EIRs and EIR equivalents relative to baseline values from 1994.
Changes in SCR
Because only young children, one to five years of age, were surveyed in 2000, this limited dataset could not be reliably assessed for temporal changes in SCR. For the remaining post-ITN trial datasets (2007, 2008 and 2009), none of the age-seroprevalence curves exhibited a break point suggestive of a past shift in SCR. For each antigen during each year, the initial model with only a single SCR provided a better fit than any alternative model allowing for a change in SCR.
Discussion
Serological markers of P. falciparum exposure were useful for monitoring long-term changes in malaria transmission intensity in this highly endemic region. Patterns in point measurements of seroprevalence, antibody titres and SCRs all indicate that a gradual but substantial drop in malaria transmission (46-70%) occurred in Asembo from 1994 to 2007, followed by a marginal increase beginning in 2008 or 2009. This is consistent with previous findings based on child mortality, parasite prevalence [31] and EIR (J Gimnig, unpublished data). In particular, proportionate changes in antibody responses, relative to 1994 baseline values, for AMA-1 and CSP (but not MSP-119) corresponded closely with trends in parasite prevalence throughout the 15-year study period.
AMA-1 is known to be highly immunogenic [18]; it was expected that AMA-1 immunological responses would saturate in the Asembo population, causing seroprevalence and SCR to remain static and therefore, uninformative. This was not the case, as AMA-1 seroprevalence and SCR varied three-fold between 1994 and 2008. Furthermore, proportionate changes for both AMA-1 seroprevalence and SCR exhibited a straightforward relationship with changes in parasite prevalence over the entire study period. As anticipated in this highly endemic region, CSP was also found to be a sensitive marker for detecting shifts in transmission; proportionate changes in CSP seroprevalence and SCR generally corresponded well with changing patterns in parasite prevalence. Despite having been informative across a range of malaria transmission settings throughout Africa [18, 35], MSP-119 performed poorly in Asembo; proportionate changes in MSP-119 seroprevalence and SCR overestimated changes in parasite prevalence during 2000, 2008 and 2009.
Examination of antibody titres also revealed an unexpected outcome for MSP-119. In 2000 (immediately after the conclusion of the ITN trial), young children from villages that received ITNs in 1997 had significantly higher MSP-119 antibody levels compared with those from villages that received ITNs in 1999. Previous investigations on short-term immunologic responses in very young children in Asembo also reported counter-intuitive results for MSP-119. During a 1992–1994 cohort study following children from birth to 2.5 years, Singer et al.[32] found an inverse relationship between malaria exposure (based on EIR and incidence of parasitaemia) and MSP-119 antibody levels. In 1998, Kariuki et al.[52] reported that among children under three years of age, seroprevalence against MSP-119 was higher in intervention villages compared with control villages 14 months after the ITN trial’s start. At 22 months after the start of the trial, however, this pattern was no longer observed. Results from the current study, together with those of Singer et al.[32] and Kariuki et al.[52], indicate that MSP-119 is not a reliable short- or long-term marker of changing malaria exposure in Asembo. Singer et al.[32] and Kariuki et al.[52] hypothesized that in this area of intense year-round malaria transmission, immune systems of young children may be so overwhelmed by high-density parasitaemia that reducing parasite exposure leads to a higher immune response against blood-stage antigens. Findings for AMA-1 from the present study suggest that this is not true for all blood-stage antigens, but rather an irregularity of the MSP-119 response. This hypothesis of ineffective MSP-1 response may also explain why MSP-1 seroprevalence, unlike that of AMA-1 and CSP, was not correlated with positive blood film, an indicator of recent infection.
When comparing villages that received ITNs in 1997 vs 1999, it was anticipated that differences in serological responses would be apparent in 2000 and then gradually erode with time. Interestingly, aside from the unexpected finding of higher MSP-119 antibody titres among children from villages that received ITNs earlier, no serological differences were found between the two groups in 2000 or in any other year. This finding suggests that immune challenge by malaria parasites remains high enough in this region to maintain antibodies against the three antigens examined, making it difficult to detect subtle differences in the length of population protection under ITNs using these serological markers.
The different serological outcomes analysed (seroprevalence, increase in seroprevalence with age, antibody titre, and SCR) all produced similar trends for reconstructing transmission history in Asembo. Of note, linear regression proved to be a useful analysis tool. The relationship between seroprevalence and age tends to be linear in young age groups, and linear regression allowed for calculation of an SCR proxy using only data from children aged one to five years. The fact that these linear regression coefficients exhibited the same pattern over time as SCRs estimated using data from all age groups supports the idea that, in regions of high malaria transmission intensity, immunological changes are most evident in young children. For example, during the classic Garki study in northern Nigeria, Cornille-Brogger et al.[20] also found that changes in antibody levels were most pronounced in young children up to four years of age. In Asembo, periodic point estimates of seroprevalence against AMA-1 and/or CSP in young children appear to be adequate for reconstructing long-term changes in malaria exposure. A major disadvantage, however, of any analysis method relying on point estimates is that baseline values plus several subsequent time point measurements are required for comparison. A more powerful analysis method, particularly in settings where baseline measurements are unavailable, involves fitting the reversible catalytic conversion model to seroprevalence data from all age groups to retrospectively detect changes within a single cross-sectional survey.
The reversible catalytic conversion model generated accurate population-wide SCR estimates, but did not detect retrospective changes associated with the 1997–1999 ITN trial within individual post-trial surveys. Because EIR, parasite prevalence and child mortality statistics from Asembo all indicated that malaria transmission declined drastically as a result of the ITN trial [30, 39, 40, 53], children born after the trial were expected to exhibit a markedly reduced SCR compared with older age groups. However, no break points indicating change in SCR with age were found within the age-seroprevalence curves from 2007, 2008 or 2009. It is possible that changes in SCR would have been most pronounced immediately after the trial’s conclusion. Unfortunately, the serological samples from 2000 were restricted to young children aged one to five years, limiting the ability to assess for shifts in SCR across different age groups during that year.
Inability to detect break points in the 2007, 2008 or 2009 age-seroprevalence curves may be due to several non-mutually exclusive factors. First, the Kenya Ministry of Health has instituted a series of national interventions over the past decade, including introduction of long-lasting ITNs, revised recommendations for more effective first-line anti-malarials [31] and implementation of intermittent preventive treatment in pregnant women [47] as well as integrated management of childhood illness [54]. These health system changes, along with socio-economic improvements, have further reduced malaria morbidity and mortality in Asembo [31]. Thus, Asembo residents have experienced a gradual decline in malaria transmission over many years, making the reductions from the ITN trial more difficult to pinpoint. Second, despite the documented reductions in malaria morbidity and mortality over the last decade, transmission intensity in Asembo remains high compared to other malaria-endemic areas. When examining data from other locations where clear break points have been documented in the age-seroprevalence curves (e.g., Tanzania [21], Vanuatu [24], Equatorial Guinea [22]), post-intervention SCRs were generally two to ten times lower than the values observed for Asembo. It is possible that transmission intensity remains too high in Asembo for the reversible catalytic conversion model, combined with these antigens, to accurately predict shifts in SCR between age groups. Third, a great deal of short- and long-term migration occurs in and out of the Lake Victoria region [43, 55, 56]. Out of this highly mobile population, it is possible that many of the individuals surveyed in 2007, 2008 or 2009 did not reside in Asembo during the ITN trial, further diminishing the ability to detect a sharp drop in malaria exposure. Fourth, serological evidence of the historic decline in transmission may be obscured in part by the recent rise in malaria incidence in Asembo since 2008. While serological data from 2007 (and potentially 2008) would not have been influenced by this problem, samples from those two years were small in number and restricted to individuals aged ≤15 years, which could have hindered the ability to detect differences in SCR between age groups. Samples from 2009 were ample and included all ages, but the rebound in malaria transmission may have obscured any differences between age groups by disproportionately increasing seroprevalence in younger individuals.
In addition to limited sample sizes and age groups for certain years, reliance on past studies that employed different protocols presented multiple challenges. For example, serological specimens from 1994 and 2000 were collected as serum, whereas specimens from 2007 to 2009 were collected as dried blood spots. To be cautious, direct quantitative comparison of ELISA results between years was minimized by calculating different seropositivity cut-off values for each year. Unfortunately, direct comparisons could not be avoided when examining antibody titres. It should be noted, however, that Corran et al.[46] reported 93% correlation in antibody concentrations between paired serum and blood spot samples from the field, suggesting that both types of specimens serve as adequate and comparable sources of anti-malarial antibodies.
Different methods were also employed to measure EIRs in Asembo over time. Bed net traps, PSCs and CDC light traps differ in their sensitivity for capturing malaria vectors [11, 57, 58], making it difficult to compare EIRs from one year to the next. This problem extends far beyond the present study; EIR is the most commonly used metric of malaria transmission intensity, yet is notoriously difficult to standardize [3]. The lack of congruence between EIR equivalents estimated from serological data and measured EIR values could be due to poor fit of the calibration curves to Asembo serology data, failure to standardize EIR measurement techniques, or a combination of both. In addition, the heterogeneous distribution of mosquito bites across individuals within a population is known to introduce discrepancies between EIR and SCR [14]. Despite these problems, the overall trend of a dramatic decrease in EIRs and EIR equivalents from 1994 to the mid 2000s, followed by a small rise in recent years, is consistent with serological results [31].
Conclusions
Sero-epidemiological tools have proven valuable for quantifying long-term changes in malaria transmission in numerous different locations. From the standpoint of programmatic monitoring, serology is relatively fast and efficient; finger-prick blood samples can be quickly collected in large numbers and ELISAs are high-throughput and easily standardized [16, 46]. In highly endemic areas, however, historic reductions in malaria transmission may be difficult to detect from a single post-intervention survey using current serological tools, potentially limiting the utility of these tools for retrospective analyses. Nevertheless, in high transmission settings, serological point measures could be effective as adjunct tools used in combination with parasite prevalence, as serology provides information on cumulative incidence and is less sensitive to seasonal fluctuations. Exploration of different malaria antigens or alternative models of population seroconversion (e.g., models that take into account age- or exposure-related changes in seroreversion rates [48, 59–61]) may yield tools that are more informative for retrospective analyses in high endemicity areas. As malaria control receives increasing attention and funding, there will be growing need for tools that can accurately measure the epidemiological impact of interventions over extended periods, particularly in high transmission settings where reductions are most difficult to achieve and sustain.
References
Smith DL, Dushoff J, Snow RW, Hay SI: The entomological inoculation rate and Plasmodium falciparum infection in African children. Nature. 2005, 438: 492-495. 10.1038/nature04024.
Hay SI, Smith DL, Snow RW: Measuring malaria endemicity from intense to interrupted transmission. Lancet Infect Dis. 2008, 8: 369-378. 10.1016/S1473-3099(08)70069-0.
Kelly-Hope LA, McKenzie FE: The multiplicity of malaria transmission: a review of entomological inoculation rate measurements and methods across sub-Saharan Africa. Malar J. 2009, 8: 19-10.1186/1475-2875-8-19.
Byass P: Making sense of long-term changes in malaria. Lancet. 2008, 372: 1523-1525. 10.1016/S0140-6736(08)61631-1.
Breman JG: The ears of the hippopotamus: manifestations, determinants, and estimates of the malaria burden. Am J Trop Med Hyg. 2001, 64: 1-11.
Rowe AK, Kachur SP, Yoon SS, Lynch M, Slutsker L, Steketee RW: Caution is required when using health facility-based data to evaluate the health impact of malaria control efforts in Africa. Malar J. 2009, 8: 3-10.1186/1475-2875-8-3.
Afrane YA, Githeko A, Yan GY: Misdiagnosis and overtreatment of clinical malaria cases and their implications in western Kenya highlands. Am J Trop Med Hyg. 2009, 81: 195-195.
Beier JC, Killeen GF, Githure JI: Short report: entomologic inoculation rates and Plasmodium falciparum malaria prevalence in Africa. Am J Trop Med Hyg. 1999, 61: 109-113.
Hay SI, Rogers DJ, Toomer JF, Snow RW: Annual Plasmodium falciparum entomological inoculation rates (EIR) across Africa: literature survey, internet access and review. Trans R Soc Trop Med Hyg. 2000, 94: 113-127. 10.1016/S0035-9203(00)90246-3.
Dye C: The analysis of parasite transmission by bloodsucking insects. Ann Rev Entomol. 1992, 37: 1-19. 10.1146/annurev.en.37.010192.000245.
Mbogo CN, Glass GE, Forster D, Kabiru EW, Githure JI, Ouma JH, Beier JC: Evaluation of light traps for sampling Anopheline mosquitoes in Kilifi, Kenya. J Am Mosquito Contr. 1993, 9: 260-263.
Magbity EB, Lines JD: Spatial and temporal distribution of Anopheles gambiae s.l. (Diptera: Culicidae) in two Tanzanian villages: implication for designing mosquito sampling routines. Bull Entomol Res. 2002, 92: 483-488.
Tusting LS, Bousema T, Smith DL, Drakeley C: Measuring changes in Plasmodium falciparum transmission: precision, accuracy and costs of metrics. Advances in Parasitology. Volume 84. Edited by: Rollinson D. 2014, San Diego: Elsevier Academic Press Inc, 151-208.
Smith DL, Drakeley CJ, Chiyaka C, Hay SI: A quantitative analysis of transmission efficiency versus intensity for malaria. Nat Comm. 2010, 1: 108-10.1038/ncomms1107. doi:10.1038/ncomms1107
Yukich J, Briët O, Bretscher MT, Bennett A, Lemma S, Berhane Y, Eisele TP, Keating J, Smith T: Estimating Plasmodium falciparum transmission rates in low-endemic settings using a combination of community prevalence and health facility data. PLoS One. 2012, 7: e42861-10.1371/journal.pone.0042861.
Corran P, Coleman P, Riley E, Drakeley C: Serology: a robust indicator of malaria transmission intensity?. Trends Parasitol. 2007, 23: 575-582. 10.1016/j.pt.2007.08.023.
O’Meara WP, Collins WE, McKenzie FE: Parasite prevalence: a static measure of dynamic infections. Am J Trop Med Hyg. 2007, 77: 246-249.
Drakeley CJ, Corran PH, Coleman PG, Tongren JE, McDonald SLR, Carneiro I, Malima R, Lusingu J, Manjurano A, Nkya WMM, Lemnge MM, Cox J, Reyburn H, Riley EM: Estimating medium- and long-term trends in malaria transmission by using serological markers of malaria exposure. Proc Natl Acad Sci U S A. 2005, 102: 5108-5113. 10.1073/pnas.0408725102.
Bousema T, Youssef RM, Cook J, Cox J, Alegana VA, Amran J, Noor AM, Snow RW, Drakeley C: Serologic markers for detecting malaria in areas of low endemicity, Somalia, 2008. Emerg Infect Dis. 2010, 16: 392-399. 10.3201/eid1603.090732.
Cornille-Brogger R, Mathews HM, Storey J, Ashkar TS, Brogger S, Molineaux L: Changing patterns in the humoral immune response to malaria before, during, and after the application of control measures: a longitudinal study in the West African savanna. Bull World Health Organ. 1978, 56: 579-600.
Stewart L, Gosling R, Griffin J, Gesase S, Campo J, Hashim R, Masika P, Mosha J, Bousema T, Shekalaghe S, Cook J, Corran P, Ghani A, Riley EM, Drakeley C: Rapid assessment of malaria transmission using age-specific sero-conversion rates. PLoS One. 2009, 4: e6083-10.1371/journal.pone.0006083.
Cook J, Kleinschmidt I, Schwabe C, Nseng G, Bousema T, Corran PH, Riley EM, Drakeley CJ: Serological markers suggest heterogeneity of effectiveness of malaria control interventions on Bioko Island. Equatorial Guinea PLoS One. 2011, 6: e25137-10.1371/journal.pone.0025137.
Lim CS, Yoon JK, Chang EA, Suh IB, An SSA, Lee KH, Chung JT, Tockgo YC: Seroprevalence to the circumsporozoite protein peptide antigen of Plasmodium vivax in Korean children. Microbiol Immunol. 2005, 49: 521-527. 10.1111/j.1348-0421.2005.tb03757.x.
Cook J, Reid H, Iavro J, Kuwahata M, Taleo G, Clements A, McCarthy J, Vallely A, Drakeley C: Using serological measures to monitor changes in malaria transmission in Vanuatu. Malar J. 2010, 9: 169-10.1186/1475-2875-9-169.
Druilhe P, Pradier O, Marc JP, Miltgen F, Mazier D, Parent G: Levels of antibodies to Plasmodium falciparum sporozoite surface antigens reflect malaria transmission rates and are persistent in the absence of reinfection. Infect Immun. 1986, 53: 393-397.
Hsiang MS, Hwang J, Kunene S, Drakeley C, Kandula D, Novotny J, Parizo J, Jensen T, Tong M, Kemere J, Dlamini S, Moonen B, Angov E, Dutta S, Ockenhouse C, Dorsey D, Greenhouse B: Surveillance for malaria elimination in Swaziland: a national cross-sectional study using pooled PCR and serology. PLoS One. 2012, 7: e29550-10.1371/journal.pone.0029550.
Bloland PB, Ruebush TK, McCormick JB, Ayisi J, Boriga DA, Oloo AJ, Beach R, Hawley W, Lal A, Nahlen B, Udhayakumar V, Campbell CC: Longitudinal cohort study of the epidemiology of malaria infections in an area of intense malaria transmission I. Description of study site, general methodology, and study population. Am J Trop Med Hyg. 1999, 60: 635-640.
Phillips-Howard PA, Nahlen BL, Alaii JA, ter Kuile FO, Gimnig JE, Terlouw DJ, Kachur SP, Hightower AW, Lal AA, Schoute E, Oloo AJ, Hawley WA: The efficacy of permethrin-treated bed nets on child mortality and morbidity in western Kenya I. Development of infrastructure and description of study site. Am J Trop Med Hyg. 2003, 68: 3-9.
Phillips-Howard PA, ter Kuile FO, Nahlen BL, Alaii JA, Gimnig JE, Kolczak MS, Terlouw DJ, Kariuki SK, Shi YP, Kachur SP, Hightower AW, Vulule JM, Hawley WA: The efficacy of permethrin-treated bed nets on child mortality and morbidity in western Kenya II. Study design and methods. Am J Trop Med Hyg. 2003, 68: 10-15.
Lindblade KA, Eisele TP, Gimnig JE, Alaii JA, Odhiambo F, ter Kuile FO, Hawley WA, Wannemuehler KA, Phillips-Howard PA, Rosen DH, Nahlen BL, Terlouw DJ, Adazu K, Vulule JM, Slutsker L: Sustainability of reductions in malaria transmission and infant mortality in Western Kenya with use of insecticide-treated bednets: 4 to 6 years of follow-up. J Am Med Assoc. 2004, 291: 2571-2580. 10.1001/jama.291.21.2571.
Hamel MJ, Adazu K, Obor D, Sewe M, Vulule J, Williamson JM, Slutsker L, Feikin DR, Laserson KF: A reversal in reductions of child mortality in western Kenya, 2003–2009. Am J Trop Med Hyg. 2011, 85: 597-605. 10.4269/ajtmh.2011.10-0678.
Singer LM, Mirel LB, Kuile FO, Branch OH, Vulule JM, Kolczak MS, Hawley WA, Simon KK, Kaslow DC, Lanar DE, Lai AA: The effects of varying exposure to malaria transmission on development of antimalarial antibody responses in preschool children. XVI. Asembo Bay cohort project. J Infect Dis. 2003, 187: 1756-1764. 10.1086/375241.
Webster HK, Gingrich JB, Wongsrichanalai C, Tulyayon S, Suvarnamani A, Sookto P, Permpanich B: Circumsporozoite antibody as a serologic marker of Plasmodium falciparum transmission. Am J Trop Med Hyg. 1992, 47: 489-497.
Esposito F, Lombardi S, Modiano D, Zavala F, Reeme J, Lamizana L, Coluzzi M, Nussenzweig RS: Prevalence and levels of antibodies to the circumsporozoite protein of Plasmodium falciparum in an endemic area an their relationship to resistance against malaria infection. Trans R Soc Trop Med Hyg. 1988, 82: 827-832. 10.1016/0035-9203(88)90007-7.
Badu K, Afrane YA, Larbi J, Stewart VA, Waitumbi J, Angov E, Ong’echa JM, Perkins DJ, Zhou G, Githeko A, Yan G: Marked variation in MSP-1(19) antibody responses to malaria in western Kenyan highlands. BMC Infect Dis. 2012, 12: 50-10.1186/1471-2334-12-50.
Bloland PB, Boriga DA, Ruebush TK, McCormick JB, Roberts JM, Oloo AJ, Hawley W, Lal A, Nahlen B, Campbell CC: Longitudinal cohort study of the epidemiology of malaria infections in an area of intense malaria transmission II. Descriptive epidemiology of malaria infection and disease among children. Am J Trop Med Hyg. 1999, 60: 641-648.
Beier JC, Perkins PV, Onyango FK, Gargan TP, Oster CN, Whitmire RE, Koech DK, Roberts CR: Characterization of malaria transmission by Anopheles (Diptera, Culicidae) in western Kenya in preparation for malaria vaccine trials. J Med Entomol. 1990, 27: 570-577.
Beier JC, Oster CN, Onyango FK, Bales JD, Sherwood JA, Perkins PV, Chumo DK, Koech DV, Whitmire RE, Roberts CR, Diggs CL, Hoffman SL: Plasmodium falciparum incidence relative to entomological inoculation rates at a site proposed for testing malaria vaccines in western Kenya. Am J Trop Med Hyg. 1994, 50: 529-536.
ter Kuile FO, Terlouw DJ, Phillips-Howard PA, Hawley WA, Friedman JF, Kolczak MS, Kariuki SK, Shi YP, Kwena AM, Vulule JM, Nahlen BL: Impact of permethrin-treated bed nets on malaria and all-cause morbidity in young children in an area of intense perennial malaria transmission in western Kenya: cross-sectional survey. Am J Trop Med Hyg. 2003, 68: 100-107.
Gimnig JE, Vulule JM, Lo TQ, Kamau L, Kolczak MS, Phillips-Howard PA, Mathenge EM, ter Kuile FO, Nahlen BL, Hightower AW, Hawley WA: Impact of permethrin-treated bed nets on entomologic indices in an area of intense year-round malaria transmission. Am J Trop Med Hyg. 2003, 68: 16-22.
Lindblade KA, Gimnig JE, Kamau L, Hawley WA, Odhiambo F, Olang G, Ter Kuile FO, Vulule JM, Slutsker L: Impact of sustained use of insecticide-treated bednets on malaria vector species distribution and culicine mosquitoes. J Med Entomol. 2006, 43: 428-432. 10.1603/0022-2585(2006)043[0428:IOSUOI]2.0.CO;2.
Amek N, Bayoh N, Hamel M, Lindblade KA, Gimnig JE, Odhiambo F, Laserson KF, Slutsker L, Smith T, Vounatsou P: Spatial and temporal dynamics of malaria transmission in rural Western Kenya. Parasit Vectors. 2012, 5: 86-10.1186/1756-3305-5-86.
Adazu K, Lindblade KA, Rosen DH, Odhiambo F, Ofware P, Kwach J, van Eijk AM, Decock KM, Amornkul P, Karanja D, Vulule JM, Slutsker L: Health and demographic surveillance in rural western Kenya: a platform for evaluating interventions to reduce morbidity and mortality from infectious diseases. Am J Trop Med Hyg. 2005, 73: 1151-1158.
Wirtz RA, Zavala F, Charoenvit Y, Campbell GH, Burkot TR, Schneider I, Esser KM, Beaudoin RL, Andre RG: Comparative testing of monoclonal antibodies against Plasmodium falciparum sporozoites for ELISA development. Bull World Health Organ. 1987, 65: 39-45.
Scott JA, Brogdon WG, Collins FH: Identification of single specimens of the Anopheles gambiae complex by the polymerase chain reaction. Am J Trop Med Hyg. 1993, 49: 520-529.
Corran PH, Cook J, Lynch C, Leendertse H, Manjurano A, Griffin J, Cox J, Abeku T, Bousema T, Ghani AC, Drakeley C, Riley EM: Dried blood spots as a source of anti-malarial antibodies for epidemiological studies. Malar J. 2008, 7: 195-10.1186/1475-2875-7-195.
Odhiambo FO, Laserson KF, Sewe M, Hamel MJ, Feikin DR, Adazu K, Ogwang S, Obor D, Amek N, Bayoh N, Ombok M, Lindblade K, Desai M, ter Kuile F, Phillips-Howard P, van Eijk AM, Rosen D, Hightower A, Ofware P, Muttai H, Nahlen B, DeCock K, Slutsker L, Beriman R, Vulule JM: Profile: the KEMRI/CDC Health and Demographic Surveillance System-Western Kenya. Int J Epidemiol. 2012, 41: 977-987. 10.1093/ije/dys108.
Ondigo BN, Hodges JS, Ireland KF, Magak NG, Lanar DE, Dutta S, Narum DL, Park GS, Ofulla AV, John CC: Estimation of recent and long-term malaria transmission in a population by antibody testing to multiple Plasmodium falciparum antigens. J Infect Dis. 2014, 210: 1123-1132. 10.1093/infdis/jiu225.
Reed GF, Meade BD, Steinhoff MC: The reverse cumulative distribution plot- a graphic method for exploratory analysis of antibody data. Pediatrics. 1995, 96: 600-603.
Deloron P, Steketee R, Campbell GH, Peyron F, Kaseje D, Brandling-Bennett AD: Serological reactivity to the ring-infected erythrocyte surface antigen and circumsporozoite protein in gravid and nulligravid women infected with Plasmodium falciparum. Trans R Soc Trop Med Hyg. 1989, 83: 58-62. 10.1016/0035-9203(89)90705-0.
Campbell CC, Martinez JM, Collins WE: Seroepidemiological studies of malaria in pregnant women and newborns from coastal El Salvador. Am J Trop Med Hyg. 1980, 29: 151-157.
Kariuki SK, Lal AA, Terlouw DJ, ter Kuile FO, Ong’echa JM, Phillips-Howard PA, Orago ASS, Kolczak MS, Hawley WA, Nahlen BL, Shi YP: Effects of permethrin-treated bed nets on immunity to malaria in western Kenya II. Antibody responses in young children in an area of intense malaria transmission. Am J Trop Med Hyg. 2003, 68: 108-114.
Phillips-Howard PA, Nahlen BL, Kolczak MS, Hightower AW, ter Kuile FO, Alaii JA, Gimnig JE, Arudo J, Vulule JM, Odhacha A, Kachur SP, Schoute E, Rosen DH, Sexton JD, Oloo AJ, Hawley WA: Efficacy of permethrin-treated bed nets in the prevention of mortality in young children in an area of high perennial malaria transmission in western Kenya. Am J Trop Med Hyg. 2003, 68: 23-29.
Perkins BA, Zucker JR, Otieno J, Jafari HS, Paxton L, Redd SC, Nahlen BL, Schwartz B, Oloo AJ, Olango C, Gove S, Campbell CC: Evaluation of an algorithm for integrated management of childhood illness in an area of Kenya with high malaria transmission. Bull World Health Organ. 1997, 75 (Suppl 1): 33-42.
Pindolia DK, Garcia AJ, Huang Z, Smith DL, Alegana VA, Noor AM, Snow RW, Tatem AJ: The demographics of human and malaria movement and migration patterns in East Africa. Malar J. 2013, 12: 12-10.1186/1475-2875-12-12.
Wesolowski A, Eagle N, Tatem AJ, Smith DL, Noor AM, Snow RW, Buckee CO: Quantifying the impact of human mobility on malaria. Science. 2012, 338: 267-270. 10.1126/science.1223467.
Davis JR, Hall T, Chee EM, Majala A, Minjas J, Shiff CJ: Comparison of sampling anopheline mosquitoes by light-trap and human-bait collections indoors at Bagamoyo, Tanzania. Med Vet Entomol. 1995, 9: 249-255. 10.1111/j.1365-2915.1995.tb00130.x.
Mathenge EM, Omweri GO, Irungu LW, Ndegwa PN, Walczak E, Smith TA, Killeen GF, Knols BGJ: Comparative field evaluation of the Mbita trap, the Centers for Disease Control light trap, and the human landing catch for sampling of malaria vectors in western Kenya. Am J Trop Med Hyg. 2004, 70: 33-37.
Bosomprah S: A mathematical model of seropositivity to malaria antigen, allowing seropositivity to be prolonged by exposure. Malar J. 2014, 13: 12-10.1186/1475-2875-13-12.
Drakeley C, Cook J: Potential contribution of sero-epidemiological analysis for monitoring malaria control and elimination: historical and current perspectives. In Adv Parasitol. 2009, 69: 299-352.
Akpogheneta OJ, Duah NO, Tetteh KKA, Dunyo S, Lanar DE, Pinder M, Conway DJ: Duration of naturally acquired antibody responses to blood-stage Plasmodium falciparum is age dependent and antigen specific. Infect Immun. 2008, 76: 1748-1755. 10.1128/IAI.01333-07.
Acknowledgements
We thank the residents of Asembo who participated in this study, as well as the KEMRI and CDC personnel who conducted surveys and collected serological specimens. Funding for surveys and sample collection came from CDC through a cooperative agreement with KEMRI. Funding for reagents and serological analysis was through the Malaria Transmission Consortium (grant no. 45114). JW was supported by a fellowship from the American Society for Microbiology. This paper was published with the permission of the KEMRI director.
Disclaimer
The opinions or assertions contained in this manuscript are the private ones of the authors and are not to be construed as official or reflecting the views of the US Public Health Service or Department of Health and Human Services. Use of trade names is for identification only and does not imply endorsement by US Public Health Service or Department of Health and Human Services.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contribution
JW participated in study design, carried out the ELISA assays, performed the statistical analysis, and wrote the manuscript; MJH conceived of the study, participated in its design, coordinated field surveys and sample collection, and helped to draft the manuscript; CJD participated in study design, supplied reagents and analysis tools, provided technical support for serological work and statistical analysis, and helped to draft the manuscript; SK and YPS participated in study design and provided technical and logistical support for serological work; AAL, BLN, PBB, LS, and KAL coordinated field surveys and sample collection and helped to revise the manuscript; VW managed data from field surveys; KO conducted laboratory processing of field-collected samples; PO and CO collected data and samples during field surveys; JMV participated in study design and provided logistical support; JEG conceived of the study, participated in its design, oversaw collection of entomological data, and helped to draft the manuscript. All authors have read and approved the final manuscript.
Electronic supplementary material
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article

Cite this article
Wong, J., Hamel, M.J., Drakeley, C.J. et al. Serological markers for monitoring historical changes in malaria transmission intensity in a highly endemic region of Western Kenya, 1994–2009. Malar J 13, 451 (2014). https://doi.org/10.1186/1475-2875-13-451
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-13-451