
Abstract
Background
Pregnant women remain are at an increased risk of malaria with primigravidae being at the highest risk. Genetic polymorphism of the Fc receptor IIa for immunologlobulin (Ig) G (FcγRIIa) determines IgG subclass binding. Protection against pregnancy-associated malaria (PAM) is associated with the production of IgG specific for apical membrane antigen-1 (AMA-1). The present study was undertaken to examine the relationship between specific IgG/IgG subclasses and malaria infection. The second aim of the study is to examine the association between FcγRIIa R/H131 polymorphism in correlation with specific anti-malarial IgG antibodies of AMA-1 distribution and asymptomatic malaria infection among Saudi women living in the southern part of Saudi Arabia.
Methods
One hundred and twenty pregnant women living in an area of meso-endemic Plasmodium falciparum malaria infection were consecutively enrolled onto the study. These pregnant women were asymptomatic and attending routine antenatal clinics. The levels of plasma antibodies (IgG and subclasses AMA-1) were measured using indirect enzyme-linked immunosorbent assays (ELISA). Genotyping of FcγRIIa-R/H131 dimorphism was performed using gene-specific polymerase chain reaction (PCR) amplification with allele-specific restriction enzyme digestion (Bst U1) of the PCR product.
Results
A total of sixty-two (52%) pregnant women was diagnosed with asymptomatic malarial infection (ASM) compared with 58 (48%) malaria free controls (MFC). In the ASM group, there were high levels of anti-malarial IgG1 and IgG3, when compared to MFC (P value <0.001, respectively). The FcγRIIa-R/R131 genotype and R131 were found to be statistically significantly more prevalent in the ASM group when compared to the MFC group [55% for ASM versus 12% for MFC, odds ratio (OR) 5.62, 95% confidence interval (CI)= (2.03- 15.58), P value= 0.001]. However, the H/H131 genotype showed statistically significant association with MFC [14% for ASM versus 50% for MFC, OR(0.36), 95% CI= (0.14- 0.95), P value= 0.03].
Conclusions
The study revealed that the ASM patients had higher anti-malarial IgG and IgG subclasses antibody levels when compared to the MFC. The FcγRIIa-R/R131 genotype and R131 allele were found to be statistically prevalent in the ASM when compared to the MFC group. The individuals carrying H/H131 were consistently associated with higher levels of anti-malarial IgG subclasses.
Similar content being viewed by others

Background
Malaria remains a devastating global health problem. The Arabian Peninsula lies at the fringes of malaria endemicity. Control efforts have successfully brought local transmission to a halt in many parts, with the exception of southern Saudi Arabia. In areas of intense parasite transmission, Plasmodium falciparum malaria is largely a childhood disease due to the gradual achievement of protective immunity. Each year, more than 125 million pregnant women are at risk of malaria infection with devastating consequences for the newborn and first and second time mothers [1]. In highly endemic settings, up to 50% of low birth weight (LBW) deliveries can be attributed to malaria in pregnancy. Pregnancy-associated malaria (PAM), which is characterized by accumulation of infected red blood cells (iRBCs) in the placental intervillous space [2–4], is a major cause of LBW and maternal anaemia in areas of endemic malaria transmission [5–7]. The pathogenesis of PAM and its association with adverse pregnancy outcome [8, 9], such as intrauterine growth restriction and LBW is not well understood. One hypothesis for the adverse pregnancy outcome is the impairment in nutrient transport to the foetus [10], with possible effects on growth regulating hormones [11], and trophoblast invasion [12]. Previous in vivo studies showed the absence of adhesiveness to other receptor molecules mediating adhesion to receptors located only in placental tissue [2]. This may explain the susceptibility to malaria in otherwise clinically immune women at the time of their first pregnancy [4].
Antibody-dependent cellular mechanisms are thought to be central in the elimination of the parasite [13–16], and severe malaria is associated with increased pro-inflammatory immune response [17]. Immunoglobulin G1 (IgG1) and IgG3 are considered cytophilic and protective against P. falciparum. While low levels of IgG4 was thought to be relatively associated with protective mechanisms [15]. FcγRIIa exhibits a genetic polymorphism, FcγRIIa-R/H131 which codes for different capacities of IgG binding and phagocytosis [18–22]. Furthermore, IgG2, which binds the H131 allelic form of FcγRIIa, may be involved in human resistance to malarial infection [15, 18, 20]. A defence mechanism requiring the association of antigen bound IgG antibodies with FcγRs on monocytes is thought to play an important role in protecting immune African adults from malaria [18–20, 23, 24]. Only a few studies on FcγRIIa- R/H 131 polymorphisms in relation to malaria have been performed. A study in Western Kenya showed that the FcγRIIa 131H/H genotype was associated with enhanced susceptibility to placental malaria in HIV-positive, but not in HIV-negative women [25].
Hypothetically, immune responses against malaria can be distinguished into long- and short-term responses. Long-term response being broad and represented by pre-existing immunity, which may or may not be protective [26, 27]. In contrast, the short-term immunity follows acute infection. Antibodies measured during acute infection or convalescence represent both boosted pre-existing and short-term immunity. However, it remains an open question as to whether a low level of malaria transmission is maintained throughout the dry season when clinical disease is absent. Furthermore, little is known about the relationship to the seasonal patterns of malaria transmission.
The present study was undertaken to examine the relationship between specific IgG/IgG subclasses and malaria infection. The second aim of the study is to examine the association between FcγRIIa R/H131 polymorphism in correlation with specific anti-malarial IgG antibodies of AMA-1 distribution and asymptomatic malaria infection among Saudi women living in the southern of Saudi Arabia.
Methods
Study area
This study was conducted in Jazan city in the southern Kingdom of Saudi Arabia (KSA), during the dry season, March to August 2012 (estimated population, 157,536 according to the 2010 census). The annual rainfall (between June and September) fluctuates from one year to another, and for that reason the incidence of malaria is markedly unstable. The uniqueness of this epidemiological setting is due to marked seasonality of low to moderate transmission of malaria. Whereas more than 90% of annual malaria incidence occurs between October and January; it is rare for a patient to develop more than one to two episodes of malaria during the season. Thus, it is easier to trace the immunological consequences of a single infection without interference of a superimposed infection. However, few sporadic cases of malaria may occur throughout the year.
Study design and patient enrolment
A prospective cohort (cross-sectional) study was conducted in pregnant women attending routine antenatal clinics in King Fahad Specialist Hospital in Jazan (KFSHJ), without a clinical diagnosis of malaria. Patients with asymptomatic malaria are those without any of the classical symptoms of malaria infection as described by the WHO [28]. Patients were recruited after written informed consent was gained from them. Blood samples were taken for confirmation of malaria. Once patients were found to be positive for malaria, treatment was offered. Patients with asymptomatic malaria in their first trimester of pregnancy received quinine (20 mg/kg loading dose) plus clindamycine for seven days. Patients in their second and third trimesters received standard anti-malarial combination therapy (ACT). Standard ACT constitutes artesunate (4 mg/kg/day) given on days 0–2 and a single dose of sulphadoxine-pyrimethamine (25 mg/kg) given on day 0 [29–31]. All patients were reviewed by the study gynaecologist to confirm that there were no other co-infections apart from malaria. No one from the study groups was found to be HIV positive. All patients with other infectious diseases were excluded from the study. To control for the ethnicity factor, all the patients were from a Saudi background. The Saudi populations are originally Arab tribes living in the Arabian Peninsula for more than 1,434 years.
The study was reviewed and approved by the Ethics Review Committee in the College of Medicine at Taif University.
Sample collection
Before pharmacological treatment was started, 50 μL of blood were collected on filter paper (Schleicher & Schuell; n° 903TM) for DNA amplification, parasite detection and measurement of immunoglobulin. One ml of venous blood sample was collected into EDTA Vacutainer® tubes (Becton Dickinson, Meylan, France) for parasite measurements. This was put into thick and thin blood smears obtained at the time of collection, which were then stained with Giemsa.
Serum and DNA extraction
Serum extraction was eluted from a 50 μl blood drop onto filter-paper samples, as described previously [32, 33]. DNA was extracted from a 50 μl blood drop onto filter paper with QIAamp® DNA Mini Kit (Qiagen, Hamburg, Germany), and re-suspended in 150 μl of TEB buffer [20].
Parasite genotype
Five μl of DNA samples were used to detect the P. falciparum malaria parasite using a polymerase chain reaction (PCR), targeting for ama-1_3D7 gene as described previously [34, 35]. For the negative controls, we used blood samples collected from Swedish individuals who were never exposed to P. falciparum malaria parasites. For the positive controls, we used blood samples collected from Sudanese individuals who have been exposed to P. falciparum malaria parasites in the past.
Enzyme-linked immunosorbent assays (ELISA)
IgG antibody was measured against the recombinant protein apical membrane antigen-1 (AMA-1), which has an N-terminal hexa-His tag, that is expressed in Escherichia coli and refolded in vitro. The expression and purification of these proteins was described earlier in [36, 37]. The levels of serum antibodies (IgG total and subclasses) to malaria antigen (AMA-1) was measured using enzyme-linked immunosorbent assays (ELISA) as previously described [19, 38]. EIA/RIA plates (Costar, MA, USA) were coated with AMA-1 at 1 μg/mL. The plates were incubated overnight at 4°C and then blocked for two hours with 0.5% bovine serum albumin (BSA) diluted in carbonate-bicarbonate buffer (pH 9.6). Plasma samples were diluted in incubation buffers (PBS + 0.5% BSA), 1:1000 for IgG and 1:400 for IgG subclasses (IgG1-4). Each sample was added in duplicates in the ELISA plate and incubated for one hour at 37°C. The plates were washed four times, and bound IgG antibodies were detected with goat anti-human IgG-ALP (1:2,000) (Mabtech, Nacka, Sweden). IgG subclasses were analysed with their respective biotin conjugated mouse anti-human subclass specific monoclonal antibodies: mouse anti-human IgG1 1:1,000 (M15015, Clone NL16, SkyBio, Bedfordshire, UK), mouse anti-human IgG2 1:3,000 (555874, Pharmingen, Erembodegem, Belgium), mouse anti-human IgG3 1:1,000 (MH 1532, Caltag Laboratories, Paisley, UK) and mouse anti-human IgG4 1:2,000 (B3648, Sigma, St. Louis, USA). Alkaline phosphatase (ALP) conjugated streptavidin (Mabtech) diluted 1:2,000 was added to detect bound antibodies of IgG2-4, while ALP-conjugated to goat anti-mouse Ig (Dakopatts, Glostrup, Denmark; 1:1,000) was used for IgG1 antibodies, and colour was developed with nitrophenyl phosphate (Sigma-Aldrich Chemie GmbH, Steinheim, Germany). The absorbance was read at 405 nm using a VmaxTM Kinetic microplate reader (Molecular Devices, Menlo Park, USA).
Statistical analysis
Statistical analysis was performed by SPSS version 10.0 software for Windows (SPSS®, Inc, Chicago, IL, USA). In this study, the antibody (IgG and IgG subclass) levels were analysed using Kruskal-Wallis test (non parametric) and the P values were derived. With regards to the risk of malaria infection during the pregnancy period, P values were considered significant if < 0.05. Overall, the 95% confidence intervals (CI) for odds ratio (OR) that did not cross 1.00 were statistically significance. OR above 1 represents values associated with the asymptomatic malaria group while less than 1 represents the malaria-free control group. To assess the association between the FcγRIIa genotype and malaria infection (dependent variable), logistic regression analysis was preformed with age and pregnancy duration as confounding factors. The FcγRIIa- Arg/ His 131 group was used as a reference in the analyses, as this is the genotype most prevalent in the human population [39]. The comparison of allele frequency was performed using a 2 × 2 chi-square test. To assess the relationship between the IgG (AMA-1) isotype levels and prevalence of parasite density in asymptomatic malaria patients; we used logistic regression analysis test.
Results
Characteristics of the study participants
A total of 120 pregnant women, were consecutively enrolled in the study and were classified into three groups according to pregnancy duration. Group I: First trimester [n=47 (39.2%); median age of 21 with a range of (18–26) years] (Table 1). Group II: Second trimester [n=33 (27.5%); median age of 22 with a range of (18–26) years] (Table 1). Group III: Third trimester [n=40 (33.3%); median age of 23 with a range of (18–26) years] (Table 1). Overall, there was statistical difference in the median and range of mother's age in the pregnancy duration P value= 0.046 (Table 1). A total of 58 women (48%); median age of 22 with a range of 18–26 years, were malaria parasite negative and had no clinical symptoms of malaria infection [malaria-free controls (MFC)]. A total of 62 women (52%); median age of 22 with a range of 18–26 years were malaria parasite positive and had no clinical symptoms of malaria infection [asymptomatic malaria (ASM)]. In the ASM patients, the median parasite density was 1,200 with a range of 250–2,000 parasite/μL). This is relatively low parasite density according to the WHO criteria [28]. There were no differences in age between the two study populations (median age 22 years for ASM versus MFC; OR= 1.29, 95% CI= 0.63–2.68, P value 0.486). All women attending the outpatient clinic at the time of enrolment were assessed initially by microscopy of blood film, and subsequent confirmation by PCR as mentioned in the parasite genotype section.
Relative risk to malaria infection with parasite density, IgG and IgG subclasses in association with pregnancy duration
The characteristics of the pregnant women are shown in Table 1. The prevalence of malaria infection during the pregnancy duration was statistically significant, overall P value= <0.001 (Table 1). The pregnant women in the first and second trimesters showed higher incidence of malaria infection when compared with the pregnant women in their third trimester, P value <0.001. With regards to the prevalence of malaria infection in the first and second trimester, there was no statistical difference observed between the two groups P value= 0.253. There was statistically significant difference in the median parasite density of women in the third trimester compared to the first and second, P value= 0.007 (Table 1).
Overall, there were statistical differences with FcγRIIa genotype frequencies and pregnancy duration; P value <0.001 (Table 1). Furthermore; the frequency of R131 allele was higher within the first and second trimesters compared to women in the third trimester (Table 1). However, the H131 allele was of a significantly higher frequency in pregnant women during the third trimester compared to women in the first or second trimesters (Table 1). Overall, there was statistically significant difference between the allele frequency and pregnancy duration within the study groups; P value 0.004 (Table 1).
The median level of IgG and IgG2 were statistically different between groups within the pregnancy duration; P value= 0.003 and 0.040 respectively (Table 1). However, no statistical differences were observed between the median level of IgG1, IgG3 and IgG4 and the three trimesters (Table 1). In addition, the median levels of anti-malarial IgG and IgG subclasses were higher in the third trimester than the first trimester (Table 1).
Patterns of antibody isotype in relation to relative risk of malaria infection Plasmodium falciparum-specific IgG and IgG subclasses
For anti-malarial IgG1 and IgG3, the ASM group showed very high levels compared to the MFC (P value <0.001, respectively) (Table 2). For the anti-malarial IgG antibody and IgG subclasses, the ASM showed significantly higher levels of IgG, IgG2 and IgG4 (P value 0.001, respectively) (Table 2). The most dominant subclass amongst the anti-malarial antibodies was IgG3, followed by IgG1, IgG2 and IgG4 in both study groups.
Correlation of IgG subclass levels in relative risk of Plasmodium falciparum parasite density
The sixty-two patients diagnosed with ASM were investigated to determine whether the anti-AMA-1 IgG levels were associated with P. falciparum parasite density. Interestingly, there was statistically significant association between higher levels of IgG, cytophilic IgG1 and IgG3 subclass antibodies and a reduction in parasite density (lower than1,000 parasites/μL). The OR for IgG = 0.13; 95% CI: (0.02- 0.71) and P value = 0.005. The OR for IgG1 = 0.13; 95% CI: (0.03- 0.59) and P value = 0.008]. The OR for IgG3 = 0.5; 95% CI: (0.14- 1.74) and P value = 0.034] (Table 3). No significant associations were observed for non-cytophilic IgG subclasses and the parasite density (IgG2 and IgG4) (Table 3).
FcγRIIa-R/H 131 genotype and allele frequency in relation to asymptomatic malaria
All subjects within the two study groups were genotyped for the G494A single nucleotide polymorphism (R131H) in the FcγRIIa gene (rs1801274). Both allele and genotype frequencies were found to be in Hardy-Weinberg equilibrium (P value= 0.813) (Table 4). R/R131 genotype was dominant amongst ASM patients compared to MFC (55% for R/R versus 31% for R/H genotypes; unadjusted OR= 5.62; 95% CI (2.03-15.58), P value= 0.001 and adjusted OR= 5.11; 95% CI (1.74- 15.00), P value= 0.003) (Tables 4 and 5). The homozygote H/H131 genotypes was found to be statistically significant at higher frequency in MFC individuals compared to ASM patients [50% for H/H versus 40% for R/H genotypes; unadjusted OR= 0.36; 95% CI (0.14- 0.95), P value = 0.03] (Tables 4 and 5). Following the adjustment of the OR for pregnancy duration and age of pregnant women, there appears to be no statistical significance [adjusted OR= 0.75; 95% CI (0.26- 2.62), P value= 0.75] (Tables 4 and 5). With regard to FcγRIIa allele frequencies, there were significant differences between the ASM and MFC individuals, the R131 allele being more frequent than the H131 allele amongst ASM patients (0.70 versus 0.30), OR 3.31, 95% CI (1.59–6.56), P <0.001 (Table 4).
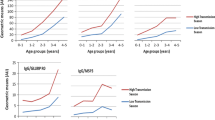
Analysis of anti-malarial antibodies in relation to FcγRIIa genotype
The distribution of FcγRIIa genotype and IgG subclass profile in the subject groups were analysed. Kruskal-Wallis (nonparametric) test showed that IgG3 antibodies specific to AMA-1 malarial antigen were associated with individuals carrying the R/R131 genotype than H/H131 genotype in the ASM group (P value <0.001) (Table 6). High levels of anti-malarial IgG1, IgG2 and IgG4 antibodies specific to AMA-1 malarial antigen, were associated with individuals carrying the R/R131 genotype than the H/H131 genotype in the ASM group (P value =0.021, 0.021 and 0.006 respectively) (Table 6).
Discussion
Despite the importance of malaria in pregnancy, this may be the first report on the immunology of P. falciparum in pregnant Saudi Women. This report investigated the relationship between specific IgG, IgG subclasses (AMA-1) antibodies, and FcγRIIa R/H131 polymorphism in association with asymptomatic malaria infection among Saudi women living in southern KSA. The risk of maternal infection was highest during the first and second trimester. One possible explanation may be that CD4+ and CD25+ regulatory T cells, which increase during the third trimester, modulate the immune response [40]. The levels of CD4+ and CD25+ regulatory T cells gradually returns to normal level after pregnancy, thus reflecting the pattern of increased incidence of malaria during the first and second trimesters [40]. Specific Th1–type immune responses are pivotal for successful immunity to malaria. These are altered during pregnancy, which might diminish the ability to control new infections and asymptomatic parasitaemia. As a consequence, pregnant women are put at an increased risk of the development of malaria [41].
When assessing the relationship between specific IgG, IgG subclasses (AMA-1) antibodies and pregnancy duration, it appears that there is a significant difference in IgG and IgG2 between the study groups and the duration of pregnancy. Furthermore, the levels of anti-malarial IgG and IgG subclasses were higher in the third trimester than the second and first trimesters. This finding may offer an explanation to the lower prevalence of malaria infection in the third trimester when compared to the first and second. In support of this finding, a previous study in Mali by Dicko et al. reported the first trimester as the main risk period for malaria infection [42]. Furthermore, a recent study in Sudan showed that pregnant women in their second trimester were more susceptible to malaria infection [43].
The current study showed accumulative association of high levels of IgG and IgG subclass antibodies with ASM patients. In support of this finding, a previous cohort study in Gabon showed that pregnant women who had malaria infection had higher levels of specific IgG of variant surface antigens (VSA) antibody compared to women who had no malaria infection [44].
The correlation of anti-malarial IgG, IgG subclass antibodies and malaria infection showed that the serum levels of IgG1 and IgG3 subclass antibodies were found to be higher than IgG2 and IgG4 antibodies, for P. falciparum blood-stage AMA-1 antigen. The cytophilic antibodies (IgG1 and IgG3) are currently thought to be instrumental in protective immunity, while non-cytophilic antibodies against the same epitopes may block the protective activity of cytophilic ones [16, 23, 45]. Several sero-epidemiological studies have supported these findings by indicating an association between protection from malarial infection with antibodies of IgG1 and IgG3 subclasses [20, 45, 46]. Furthermore, when comparing the antibody levels between the ASM and malaria free controls, the ASM showed significantly higher levels of IgG2 and IgG4 antibodies reactive to AMA-1. Previous studies from different endemic areas in Africa, showed a correlation between the severity of malarial infection and high circulating levels of IgG2 [15, 20, 47].
When assessing the relationship between anti-malarial IgG, IgG subclass antibodies and the risk of parasite density, there were higher levels of anti-malaria AMA-1 antibody IgG, IgG1 and IgG3. This may have played a crucial role in parasite reduction. The suggested mechanism by which these subclasses are protective involves their binding to the FcRs on monocytes, leading to antibody dependent cell mediated inhibition of parasite replication [23, 45]. This is supported by the results from this study, since the two most predominant IgG subclasses, are IgG1 followed by IgG3. All of the above mechanisms may have affected the parasite density and, therefore, leading to infected patients without clinical symptoms.
The importance of FcγRIIa with regards to malaria comes from its role as a link between the humoral and cellular branches of the immune system [48]. In the present study, the FcγRIIa genotype was related to PAM in Saudi women. FcγRIIa-R/R131 and R131 genotype were associated with ASM compared to MFC. However, FcγRIIa-H/H131 genotype and H131 allele had lower frequency in ASM compared to MFC. A previous study in western Kenya suggested that FcγRIIa- H/H131 genotype was associated with enhanced susceptibility to placental malaria in HIV positive women but not in HIV negative women [25]. Studies in different settings suggested that the FcγRIIa-R/R131 genotype protects against high levels of parasitaemia, whereas the FcγRIIa-H/H131 genotype was associated with susceptibility to severe malaria with high parasite burden [49–51]. An additional study in Sudan showed an association between FcγRIIa-R/R131 and severe malaria [20].
The present study was undertaken to examine the relationship between polymorphism in the gene for primary cellular IgG receptor, FcγRIIa and PAM. This study has provided evidence that the high levels of IgG subclasses are associated with FcγRIIa-R/R131 genotype among ASM women in southern Saudi. The results are in contrast with a study in western Kenya which described evidence that the IgG2-binding FcγRIIa-H/H131 genotype is associated with increased susceptibility to placental malaria in HIV-positive women [25].
Although, the FcγRIIa are important molecules in malaria outcome; several studies have attempted to associate mutations in these genes with increased susceptibility to developing different forms of malaria. However, the results are contradictory and no conclusion has yet been determined. This confliction may be due to differences in the degrees of malarial endemicity, and genetic background of the individual as well as the differences in the study designs.
Conclusions
Taken together, this study revealed that the ASM patients showed higher anti-malarial IgG and IgG subclass antibody levels when compared to the MFC. Furthermore, FcγRIIa-R/R131 genotype and R131 allele were associated with ASM patients. However, the FcγRIIa-H/H131 genotype is associated with higher levels of anti-malarial IgG subclass. Thus, the higher IgG subclass antibody levels seen in the ASM may be due to the relatively high prevalence of the individuals carrying the H/H131 genotype in this study group. Expectedly, the result of the present study suggests that the magnitude and the quality of anti-malarial humoral response is not the only key element for relative reduction in malaria infection in the ASM group. Further studies are needed to elucidate if the FcγRIIa-R/H131 polymorphism is a contributing factor to the differential susceptibility to malaria seen in different groups.
References
Dellicour S, Tatem AJ, Guerra CA, Snow RW, ter Kuile FO: Quantifying the number of pregnancies at risk of malaria in 2007: a demographic study. PLoS Med. 2007, 7: e1000221.
Achur RN, Valiyaveettil M, Alkhalil A, Ockenhouse CF, Gowda DC: Characterization of proteoglycans of human placenta and identification of unique chondroitin sulfate proteoglycans of the intervillous spaces that mediate the adherence of Plasmodium falciparum-infected erythrocytes to the placenta. J Biol Chem. 2000, 275: 40344-40356. 10.1074/jbc.M006398200.
Fried M, Duffy PE: Adherence of Plasmodium falciparum to chondroitin sulfate A in the human placenta. Science. 1996, 272: 1502-1504. 10.1126/science.272.5267.1502.
Yamada M, Steketee R, Abramowsky C, Kida M, Wirima J, Heymann D, Rabbege J, Breman J, Aikawa M: Plasmodium falciparum associated placental pathology: a light and electron microscopic and immunohistologic study. AmJTrop Med Hyg. 1989, 41: 161-168.
Brabin BJ: An analysis of malaria in pregnancy in Africa. Bull World Health Organ. 1983, 61: 1005-1016.
Guyatt HL, Snow RW: Malaria in pregnancy as an indirect cause of infant mortality in sub-Saharan Africa. Trans R Soc Trop Med Hyg. 2001, 95: 569-576. 10.1016/S0035-9203(01)90082-3.
Shulman CE, Marshall T, Dorman EK, Bulmer JN, Cutts F, Peshu N, Marsh K: Malaria in pregnancy: adverse effects on haemoglobin levels and birthweight in primigravidae and multigravidae. Trop Med Int Health. 2001, 6: 770-778. 10.1046/j.1365-3156.2001.00786.x.
McGregor IA, Wilson ME, Billewicz WZ: Malaria infection of the placenta in The Gambia, West Africa; its incidence and relationship to stillbirth, birthweight and placental weight. Trans R Soc Trop Med Hyg. 1983, 77: 232-244. 10.1016/0035-9203(83)90081-0.
Steketee RW, Wirima JJ, Slutsker L, Heymann DL, Breman JG: The problem of malaria and malaria control in pregnancy in sub-Saharan Africa. AmJTrop Med Hyg. 1996, 55: 2-7.
Guyatt HL, Snow RW: Impact of malaria during pregnancy on low birth weight in sub-Saharan Africa. Clin Microbiol Rev. 2004, 17: 760-769. 10.1128/CMR.17.4.760-769.2004.
Umbers AJ, Aitken EH, Rogerson SJ: Malaria in pregnancy: small babies, big problem. Trends Parasitol. 2011, 27: 168-175. 10.1016/j.pt.2011.01.007.
Muehlenbachs A, Mutabingwa TK, Edmonds S, Fried M, Duffy PE: Hypertension and maternal-fetal conflict during placental malaria. PLoS Med. 2006, 3: e446-10.1371/journal.pmed.0030446.
Aribot G, Rogier C, Sarthou JL, Trape JF, Balde AT, Druilhe P, Roussilhon C: Pattern of immunoglobulin isotype response to Plasmodium falciparum blood-stage antigens in individuals living in a holoendemic area of Senegal (Dielmo, west Africa). AmJTrop Med Hyg. 1996, 54: 449-457.
Aucan C, Traore Y, Fumoux F, Rihet P: Familial correlation of immunoglobulin G subclass responses to Plasmodium falciparum antigens in Burkina Faso. Infect Immun. 2001, 69: 996-1001. 10.1128/IAI.69.2.996-1001.2001.
Aucan C, Traore Y, Tall F, Nacro B, Traore-Leroux T, Fumoux F, Rihet P: High immunoglobulin G2 (IgG2) and low IgG4 levels are associated with human resistance to Plasmodium falciparum malaria. Infect Immun. 2000, 68: 1252-1258. 10.1128/IAI.68.3.1252-1258.2000.
Bouharoun-Tayoun H, Attanath P, Sabchareon A, Chongsuphajaisiddhi T, Druilhe P: Antibodies that protect humans against Plasmodium falciparum blood stages do not on their own inhibit parasite growth and invasion in vitro, but act in cooperation with monocytes. J Exp Med. 1990, 172: 1633-1641. 10.1084/jem.172.6.1633.
Grau GE, Piguet PF, Vassalli P, Lambert PH: Tumor-necrosis factor and other cytokines in cerebral malaria: experimental and clinical data. Immunol Rev. 1989, 112: 49-70. 10.1111/j.1600-065X.1989.tb00552.x.
Nasr A, Elghazali G, Giha H, Troye-Blomberg M, Berzins K: Interethnic differences in carriage of haemoglobin AS and Fcgamma receptor IIa (CD32) genotypes in children living in eastern Sudan. Acta Trop. 2008, 105: 191-195. 10.1016/j.actatropica.2007.10.003.
Nasr A, Iriemenam NC, Giha HA, Balogun HA, Anders RF, Troye-Blomberg M, ElGhazali G, Berzins K: FcgammaRIIa (CD32) polymorphism and anti-malarial IgG subclass pattern among Fulani and sympatric ethnic groups living in eastern Sudan. Malar J. 2009, 8: 43-10.1186/1475-2875-8-43.
Nasr A, Iriemenam NC, Troye-Blomberg M, Giha HA, Balogun HA, Osman OF, Montgomery SM, ElGhazali G, Berzins K: Fc gamma receptor IIa (CD32) polymorphism and antibody responses to asexual blood-stage antigens of Plasmodium falciparum malaria in Sudanese patients. Scand J Immunol. 2007, 66: 87-96. 10.1111/j.1365-3083.2007.01947.x.
Salmon JE, Millard S, Schachter LA, Arnett FC, Ginzler EM, Gourley MF, Ramsey-Goldman R, Peterson MG, Kimberly RP: Fc gamma RIIA alleles are heritable risk factors for lupus nephritis in African Americans. J Clin Invest. 1996, 97: 1348-1354. 10.1172/JCI118552.
Warmerdam PA, van de Winkel JG, Vlug A, Westerdaal NA, Capel PJ: A single amino acid in the second Ig-like domain of the human Fc gamma receptor II is critical for human IgG2 binding. J Immunol. 1991, 147: 1338-1343.
Groux H, Gysin J: Opsonization as an effector mechanism in human protection against asexual blood stages of Plasmodium falciparum: functional role of IgG subclasses. Res Immunol. 1990, 141: 529-542. 10.1016/0923-2494(90)90021-P.
Indik Z, Kelly C, Chien P, Levinson AI, Schreiber AD: Human Fc gamma RII, in the absence of other Fc gamma receptors, mediates a phagocytic signal. J Clin Invest. 1991, 88: 1766-1771. 10.1172/JCI115496.
Brouwer KC, Lal AA, Mirel LB, Otieno J, Ayisi J, Van Eijk AM, Lal RB, Steketee R, Nahlen BL, Shi YP: Polymorphism of Fc receptor IIa for immunoglobulin G is associated with placental malaria in HIV-1-positive women in western Kenya. J Infect Dis. 2004, 190: 1192-1198. 10.1086/422850.
Chang SP, Gibson HL, Lee-Ng CT, Barr PJ, Hui GS: A carboxyl-terminal fragment of Plasmodium falciparum gp195 expressed by a recombinant baculovirus induces antibodies that completely inhibit parasite growth. J Immunol. 1992, 149: 548-555.
Chappel JA, Holder AA: Monoclonal antibodies that inhibit Plasmodium falciparum invasion in vitro recognise the first growth factor-like domain of merozoite surface protein-1. Mol Biochem Parasitol. 1993, 60: 303-311. 10.1016/0166-6851(93)90141-J.
WHO:Severe falciparum malaria. World Health Organization, Communicable Diseases Cluster. Trans R Soc Trop Med Hyg. 2000, 94 (1): 1-90. 10.1016/S0035-9203(00)90413-9.
Parise ME, Ayisi JG, Nahlen BL, Schultz LJ, Roberts JM, Misore A, Muga R, Oloo AJ, Steketee RW: Efficacy of sulfadoxine-pyrimethamine for prevention of placental malaria in an area of Kenya with a high prevalence of malaria and human immunodeficiency virus infection. AmJTrop Med Hyg. 1998, 59: 813-822.
Shulman CE, Dorman EK, Cutts F, Kawuondo K, Bulmer JN, Peshu N, Marsh K: Intermittent sulphadoxine-pyrimethamine to prevent severe anaemia secondary to malaria in pregnancy: a randomised placebo-controlled trial. Lancet. 1999, 353: 632-636. 10.1016/S0140-6736(98)07318-8.
Verhoeff FH, Brabin BJ, Chimsuku L, Kazembe P, Russell WB, Broadhead RL: An evaluation of the effects of intermittent sulfadoxine-pyrimethamine treatment in pregnancy on parasite clearance and risk of low birthweight in rural Malawi. Ann Trop Med Parasitol. 1998, 92: 141-150. 10.1080/00034989859979.
Dua VK, Sarin R, Prakash A: Determination of quinine in serum, plasma, red blood cells and whole blood in healthy and Plasmodium falciparum malaria cases by high-performance liquid chromatography. J Chromatogr. 1993, 614: 87-93. 10.1016/0378-4347(93)80226-T.
Moll K, Ljungström I, Perlmann H, Scherf A, Wahlgren M: Methods in malaria research. MR4/. 2008, Virginia and BioMalPar Paris, France: ATCC Manassas
Marshall VM, Zhang L, Anders RF, Coppel RL: Diversity of the vaccine candidate AMA-1 of Plasmodium falciparum. Mol Biochem Parasitol. 1996, 77: 109-113. 10.1016/0166-6851(96)02583-2.
Soulama I, Bigoga JD, Ndiaye M, Bougouma EC, Quagraine J, Casimiro PN, Stedman TT, Sirima SB, Soulama I, Bigoga JD, Ndiaye M, Bougouma EC, Quagraine J, Casimiro PN, Stedman TT, Sirima SB: Genetic diversity of polymorphic vaccine candidate antigens (apical membrane antigen-1, merozoite surface protein-3, and erythrocyte binding antigen-175) in Plasmodium falciparum isolates from western and central Africa. AmJTrop Med Hyg. 2011, 84: 276-284. 10.4269/ajtmh.2011.10-0365.
Crewther PE, Matthew ML, Flegg RH, Anders RF: Protective immune responses to apical membrane antigen 1 of Plasmodium chabaudi involve recognition of strain-specific epitopes. Infect Immun. 1996, 64: 3310-3317.
Stanisic DI, Richards JS, McCallum FJ, Michon P, King CL, Schoepflin S, Gilson PR, Murphy VJ, Anders RF, Mueller I, Beeson JG: Immunoglobulin G subclass-specific responses against Plasmodium falciparum merozoite antigens are associated with control of parasitemia and protection from symptomatic illness. Infect Immun. 2009, 77: 1165-1174. 10.1128/IAI.01129-08.
Iriemenam NC, Khirelsied AH, Nasr A, ElGhazali G, Giha HA, Elhassan AETM, Agab-Aldour AA, Montgomery SM, Anders RF, Theisen M, Troye-Blomberg M, Elbashir MI, Berzins K: Antibody responses to a panel of Plasmodium falciparum malaria blood-stage antigens in relation to clinical disease outcome in Sudan. Vaccine. 2009, 27: 62-71. 10.1016/j.vaccine.2008.10.025.
Rascu A, Repp R, Westerdaal NA, Kalden JR, van de Winkel JG: Clinical relevance of Fc gamma receptor polymorphisms. Ann N Y Acad Sci. 1997, 815: 282-295. 10.1111/j.1749-6632.1997.tb52070.x.
Somerset DA, Zheng Y, Kilby MD, Sansom DM, Drayson MT: Normal human pregnancy is associated with an elevation in the immune suppressive CD25+ CD4+ regulatory T-cell subset. Immunology. 2004, 112: 38-43. 10.1111/j.1365-2567.2004.01869.x.
Cruz Cubas AB, Gentilini M, Monjour L: Cytokines and T-cell response in malaria. Biomed Pharmacother. 1994, 48: 27-33. 10.1016/0753-3322(94)90187-2.
Dicko A, Mantel C, Thera MA, Doumbia S, Diallo M, Diakite M, Sagara I, Doumbo OK: Risk factors for malaria infection and anemia for pregnant women in the Sahel area of Bandiagara, Mali. Acta Trop. 2003, 89: 17-23. 10.1016/j.actatropica.2003.07.001.
Omer SO, Khalil EAG, Sharif AH, Hashim AA: Pregnancy-associated malaria in Sudan: prevalence and possible risk factors. Open Trop Med J. 2011, 4: 6-10. 10.2174/1874315301104010006.
Khattab A, Reinhardt C, Staalsoe T, Fievet N, Kremsner P, Deloron P, Hviid L, Klinkert M-Q: Analysis of IgG with specificity for variant surface antigens expressed by placental Plasmodium falciparum isolates. Malar J. 2004, 3: 21-10.1186/1475-2875-3-21.
Bouharoun-Tayoun H, Druilhe P: Antibodies in falciparum malaria: what matters most, quantity or quality?. Mem Inst Oswaldo Cruz. 1992, 87 (Suppl 3): 229-234.
Tebo AE, Kremsner PG, Luty AJ: Fc gamma receptor-mediated phagocytosis of Plasmodium falciparum-infected erythrocytes in vitro. Clin Exp Immunol. 2002, 130: 300-306. 10.1046/j.1365-2249.2002.01972.x.
Ntoumi F, Ekala MT, Makuwa M, Lekoulou F, Mercereau-Puijalon O, Deloron P: Sickle cell trait carriage: imbalanced distribution of IgG subclass antibodies reactive to Plasmodium falciparum family-specific MSP2 peptides in serum samples from Gabonese children. Immunol Lett. 2002, 84: 9-16. 10.1016/S0165-2478(02)00131-1.
van de Winkel JG, Capel PJ: Human IgG Fc receptor heterogeneity: molecular aspects and clinical implications. Immunol Today. 1993, 14: 215-221. 10.1016/0167-5699(93)90166-I.
Shi YP, Nahlen BL, Kariuki S, Urdahl KB, McElroy PD, Roberts JM, Lal AA: Fcg Receptor IIa (CD32) Polymorphism is associated with protection of infants against high-density Plasmodium falciparum infection. VII. Asembo Bay cohort project. J Infect Dis. 2001, 184: 107-111. 10.1086/320999.
Cooke GS, Aucan C, Walley AJ, Segal S, Greenwood BM, Kwiatkowski DP, Hill AV: Association of Fcgamma receptor IIa (CD32) polymorphism with severe malaria in West Africa. AmJTrop Med Hyg. 2003, 69: 565-568.
Ouma C, Keller CC, Opondo DA, Were T, Otieno RO, Otieno MF, Orago AS, Ong'Echa JM, Vulule JM, Ferrell RE, Perkins DJ: Association of FCgamma receptor IIA (CD32) polymorphism with malarial anemia and high-density parasitemia in infants and young children. AmJTrop Med Hyg. 2006, 74: 573-577.
Acknowledgments
We are grateful to the donors, their families and the staff at KFSHJ for their participation, sustained cooperation and generous hospitality during over a decade of fieldwork. We would like to thank the field assistants and Mrs Muna Eltoum at Jazan University, KSA for their support. we are grateful to Dr Saeed A for sending the standard plasma and DNA controls for ELISA and PCR. We are also grateful to the cooperation of the Al-Neelain Research Centre, Faculty of Medicine, Al-Neelain University, Sudan. We are grateful to Dr Yassin A, Dr Karrar I, and Dr Iriemenam NC for the contribution in improving the science and the language of the manuscript. This work was supported by grants from the Taif University, Ministry of Higher Education, KSA (Grant number: 1-433-1761).
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
OH and GA designed the study and carried out the sampling; AN and GA performed the ELISA; AN performed the genotyping of FcγRIIa polymorphism and participated in the statistical analysis. Both AN and GA drafted the manuscript. AN, AAG and GA set up the framework, financed and revised the manuscript. All authors participated in the manuscript preparation, read and approved the final version of the manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Nasr, A., Hamid, O., Al-Ghamdi, A. et al. Anti-malarial IgG subclasses pattern and FcγRIIa (CD32) polymorphism among pregnancy-associated malaria in semi-immune Saudi women. Malar J 12, 110 (2013). https://doi.org/10.1186/1475-2875-12-110
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1475-2875-12-110