
Abstract
Background
Theories of behavior change indicate that an analysis of barriers to change is helpful when trying to influence professional practice. The aim of this study was to assess the perceived barriers to practice change by eliciting nurses' opinions with regard to barriers to, and facilitators of, implementation of a Fall Prevention clinical practice guideline in five acute care hospitals in Singapore.
Methods
Nurses were surveyed to identify their perceptions regarding barriers to implementation of clinical practice guidelines in their practice setting. The validated questionnaire, 'Barriers and facilitators assessment instrument', was administered to nurses (n = 1830) working in the medical, surgical, geriatric units, at five acute care hospitals in Singapore.
Results
An 80.2% response rate was achieved. The greatest barriers to implementation of clinical practice guidelines reported included: knowledge and motivation, availability of support staff, access to facilities, health status of patients, and, education of staff and patients.
Conclusion
Numerous barriers to the use of the Fall Prevention Clinical Practice Guideline have been identified. This study has laid the foundation for further research into implementation of clinical practice guidelines in Singapore by identifying barriers to change in acute care settings.
Similar content being viewed by others

Background
Patient care and outcomes could be significantly improved if knowledge gained from health research is better translated into practice [1]. The need to demonstrate clinically effective care is widely acknowledged yet research knowledge has been slow to influence practice. Barriers to implementing research in healthcare exist at many levels including the individual practitioner, the clinical team, the practice setting and the organizational context [2]. A plethora of literature has explored the research-practice gap phenomenon. The average practitioner, nurse or clinician does not have the time or the skills to locate and appraise the large volume of research publications. Furthermore, nurses may be uncertain about which treatment options to use when research results or advice from experts are conflicting [3]. These sentiments have been shared and confirmed by numerous studies which have consistently highlighted the barriers to research utilisation as time constraints, lack of awareness of available research literature, insufficient authority to change practice, inadequate skills in critical appraisal and lack of support for implementation of research findings [2, 4–7]. In response to these findings, synthesis of published research studies and the development of clinical practice guidelines have emerged as tools to facilitate the application of research evidence. Guidelines serve as an important vehicle for translating thcomplex research findings into recommendations; overcoming barriers to research use such as the requirement for skills in critical appraisal and synthesis; and removing the requirement for interpretation of large volumes of scientific studies [8].
The Institute of Medicine describes clinical practice guidelines (CPGs) as 'systematically developed statements to assist practitioner and patient decisions about health care for specific clinical circumstances' [9]. The successful implementation of CPGs reduces inappropriate variation in practice and provides a set of instructions for clinical decision-making to improve patient safety, improve patient outcomes, and promote cost effective and quality care [10–14]. Despite wide promulgation, guidelines have had limited effect on changing professional behavior and practice [15–18]. Most studies of CPG implementation strategies have focused on changing the performance of doctors, and a minority have targeted nurses or other health professionals [19, 20]. The findings of extensive research, from numerous studies, concur that passive dissemination of guidelines alone is usually insufficient to change clinical behavior and practice [11, 12, 21], while other interventions have small to moderate effects at best [22]. There is 'no magic bullet' [23] and little evidence exists to indicate which interventions to use for specific problems and settings [22, 24]. Grimshaw et al [19] in their latest systematic review argued that across all combinations of interventions, multifaceted interventions did not appear to be more effective than single interventions. Nonetheless, they concluded by highlighting that it is plausible that multifaceted interventions built upon a careful assessment of barriers to implementation of guidelines may be more effective than single interventions under different circumstances. However, there is still insufficient rigorous evaluative research on implementation strategies for clinical practice guidelines in hospitals.
Theories of behavior change suggest an analysis and understanding of factors that prevent or motivate change in behavior might be helpful in tailoring guideline implementation strategies [25–30]. There has been widespread acknowledgement that tailoring implementation strategies require creativity in addition to an understanding of the key barriers to change [25, 30]. However, there is a lack of empirical evidence to support any particular theory or framework for guiding development of strategies to influence change in nursing practice and there is no clear-cut basis for suggesting which specific interventions for which barriers to change are most effective. According to the NHS Centre for Reviews and Dissemination [31], implementation strategies need to be tailored to the local context; no single approach will have universal applicability. This message is reinforced by the development of the Promoting Action on Research Implementation in Health Services (PARIHS) framework [32–37], which proposed that the most successful implementation occurs when evidence is robust; the context is receptive to change with sympathetic cultures, strong leadership and appropriate monitoring and feedback systems; and when there is appropriate facilitation of change [32]. However, the effectiveness and utility of this framework in facilitating guideline implementation requires validation by further empirical research.
Grol [26] and Grol and Grimshaw [38] suggest that, in designing an effective implementation strategy, it is necessary to target local needs, barriers to and facilitators of, behavior change. These may include both structural and attitudinal factors and appropriate interventions might be targeted at both the structure and the process of care. Numerous studies identified that potential barriers to, and facilitators of, change can act at six different levels: 1) the innovation (feasibility, accessibility); 2) individual professional (knowledge, skills, attitudes, habits); 3) patient (knowledge, compliance); 4) social context (colleagues, authorities); 5) organizational context (available resources, organizational climate, structures); and 6) economic and political context (financial arrangements, regulation, policies) [2, 39, 40]. These factors underpin health professionals adoption of, and adherence to, the protocols developed from the clinical guidelines.
Recent work on efforts to implement fall prevention guidelines have incorporated locally targeted multi-intervention approaches in their fall prevention programme [41–43]. In response to the failure of two published, model-based, fall guidelines implementation projects, it was learnt that understanding local barriers and employing a locally tailored multifaceted implementation strategy are fundamental to successful implementation. However, research on issues about implementation of guidelines on fall prevention is non-existent in Singapore.
The Ministry of Health, Singapore (MOH), Nursing CPG on 'Prevention of Falls in Hospitals and Long Term Care Institutions' (Table 1) has been developed by the MOH taskforce. Since 2003, MOH has employed a working committee to develop CPGs, which are then disseminated to the acute care hospitals in Singapore. However, appropriate mechanisms to promote transfer and uptake of knowledge to change practice are unclear because the MOH does not give guidance on how to implement the guidelines and promote their use. It is anticipated that the identification of nurses' perceptions about barriers to implementation of the Fall Prevention CPG in acute care hospitals in Singapore, will assist in the process of selecting and more appropriately targeting implementation strategies locally to change nursing practice and reduce the burden of falls. The incidence of falls in the acute care hospitals in Singapore were low, between 0.68 and 1.44 per 1000 patient days [44], compared to international studies conducted in the United States, United Kingdom and Australia, which reported the incidence of falls ranging from 2 to 12 per 1000 patient days [45–47]. Despite the comparatively low fall rates in Singapore, the fall-associated injury rate was high, between 24.4 and 71.7% compared to international fall-associated injury rates which ranged between 5 to 10% [48, 49]. The current study results indicate a substantially lower rate of falls in hospitals in Singapore, with a conversely higher rate of injuries associated with falling. In a recent large-scale Taiwanese study, Chen et al. [50] pointed out that the rate of patient falls in the domestic setting averaged 0.03%, far lower than the average reported internationally (0.25%). However, the proportion of falls associated with injury is far higher in Asian countries than overseas [50]. The reason for this may lie in the culture of reporting in Asia. Anecdotally, many falls are unreported by patients and relatives when there is no associated injury because they deem the fall to have been uneventful.
The aim of the present study was to gain an understanding of perceived barriers to implementation of the Fall Prevention CPG in acute care hospitals in Singapore. This study was undertaken as part of a larger study, which aimed to develop a multifaceted implementation strategy targeting the perceived barriers, to effectively implement this guideline, to facilitate change in nursing practice, and to reduce the burden of falls in acute care hospitals in Singapore.
Methods
Design
A survey design was chosen to assess the perceived barriers to change by eliciting nurses' opinions with regards to barriers to implementation of clinical practice guidelines in their practice setting. This was undertaken with the administration of a questionnaire to nurses working in five acute care hospitals in Singapore.
Setting
All the acute care general hospitals (n = 5) in Singapore were involved in this study. The hospitals were acute care tertiary teaching facilities with an average bed capacity of 1000. These five hospitals had similar characteristics in terms of the range of clinical services provided, types of patients seen, and bed capacity to nursing staff strength.
Sample
All nursing staff (n = 1830) working in the medical, surgical and geriatric units (n = 66) in the study hospitals during the four-week survey distribution time frame were invited to complete the questionnaire. These areas were selected as they comprised the majority of clinical settings of the hospitals.
Data collection
The validated questionnaire titled, 'Barriers and facilitators assessment instrument', developed by Peters, Harmsen, Laurant, & Wensing [51], and designed to elicit perceptions of the barriers to implementation of CPGs in practice, was administered. Administration of the questionnaire took place over a period of three months from September to November 2005 for the five participating hospitals. A total of 1830 questionnaires (250 at Hospital A; 320 at Hospital B; 360 at Hospital C; 450 at Hospital D; and 450 at Hospital E) were distributed. Questionnaires were placed in personally addressed envelopes along with an explanatory letter of invitation. To facilitate distribution, the envelopes were hand delivered by one of the researchers or a hospital research collaborator to the nurse managers of the participating wards, who then accepted responsibility for distribution to all nurses in their respective areas. Each questionnaire took approximately 15 minutes to complete. Respondents were requested to return the completed questionnaire by placing the envelope into the 'return' box that was provided in each ward. A four-week time frame was allowed from distribution to return date. In the week before the due date an email was sent to the nurse managers to remind all nursing staff of the approaching due date for questionnaire return.
Instrument
The questionnaire was developed by Peters et al [51] and applied in guideline implementation studies in the Netherlands to measure barriers to and facilitators for improvement of patient care, with a special focus on identifying physicians' and nurses' perceived barriers to change. Psychometric qualities, in particular item response and range, had been measured by the developers of the instrument. The first part of the instrument consisted of rating various possible barriers to, and facilitators of, the general implementation of a 'directive or innovation'. The second part of instrument consisted of identification of barriers to, and facilitators of, implementation of a specific 'directive or innovation' in practice. As recommended by the authors of the tool, six questions were reworded to address the specific guideline being employed in the study, specifically, the words 'directive or innovation' in the original questionnaire were replaced with the words 'Fall Prevention CPG'. Six questions which were not relevant in the context of the implementation of the CPG in Singapore were removed from the instrument. A total of 21 items remained. This questionnaire comprised two sections. The first section contained the 21 randomly ordered items from the 'Barriers and facilitators assessment instrument' [51]. Respondents were required to rate, on a 5-point Likert-type scale, ranging from 'Fully agree', which corresponded to a score of five to 'Fully disagree', which corresponded to a score of one. The scores related to the extent to which they believed each item was a barrier to the implementation of the CPG in practice. Items were grouped into four categories: 1) innovation characteristics, 2) care provider characteristics, 3) patient characteristics, and 4) characteristics of the organizational, social, political and societal context. Section Two of the questionnaire included a series of demographic questions.
Prior to distribution, the questionnaire was pre-tested for understandability of the questionnaire wording had relevance in the Singapore health care context, and to attain estimates of the amount of time required to complete the questionnaire. It was administered to five nurse managers and five nurse clinicians who did not work in the hospital in which the study was being conducted. Based on respondents' recommendations, some minor rewording of the barrier and demographic questions were undertaken.
Data analysis
Data were entered into, and analyzed, using SPSS version 11.0 (SPSS Inc, Chicago, Il, USA). Frequencies and descriptive statistics were employed to describe the demographic characteristics of respondents. Frequencies, described as percentages of responses, and descriptive data, reported as means, were used to analyze the questions from the 'Barriers and facilitators assessment instrument'.
Ethics
The study was approved by the Human Research Ethics Advisory Group of The University of Melbourne and the Institutional Review Boards of the five participating hospitals. Completion of the 'Barriers and facilitators assessment instrument' was voluntary. Consent to participate was implied with the return of completed questionnaires, and the questionnaires were completed anonymously. To avoid coercion, following distribution of the questionnaires the nurses were invited to voluntarily complete the survey and place the completed anonymous questionnaire in the 'return' box at any time within the study time frame. Regardless of their decision about participation, the nurses were also assured that their employment status within the organization would in no way be affected.
Results
Demographics
A total of 1467 nurses returned the questionnaires (80.2% response rate). Table 2 shows the demographic characteristics of the respondents for the five hospitals in Singapore. The mean age of respondents was 29.5 years (range: 18 – 62 years), while the mean number of years working as a nurse was 7.6 years (range: 0.08 – 40 years). About 34% (502) of respondents had research experience. The demographic characteristics of the nurse respondents were consistent throughout the five acute care hospitals in Singapore.
Barriers to implementation of guidelines
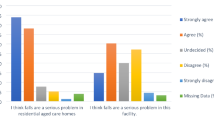
The item characteristics perceived by nurses as barriers to implementation of CPGs in practice are summarized in Table 3. The barriers to implementation of guidelines were identified from the combined percentage of 'disagree' and 'fully disagree' responses to the positive questions and the combined percentage of 'agree' and 'fully agree' responses to the negative questions. From the 21 questions, 16 item characteristics/barriers were identified. Overall, analysis showed that the greatest barriers to implementation of CPGs reported in five acute care hospitals in Singapore were: 1) knowledge and motivation (82.4%; range: 77.3% – 90.8%); 2) availability of support staff (77.8%; range: 69.7% – 83.9%); 3) access to facilities (73.3%; range: 68.6% – 79.6%); 4) health status of patients (55.7%; range: 53.0% – 61.4%); and 5) education of staff (49.4%; range: 26.8% – 55.7%).
These top five barriers identified by respondents were consistent throughout the hospitals. 'Knowledge and motivation', 'supporting staff', and 'facilities' were in the top three barriers nominated by nurses at each of the five hospitals. 'Education' was in the top five barriers nominated by nurses at four hospitals. At two hospitals, 'ethnicity' was in the top five barriers identified. The following categorizations had been identified from the original questionnaire. Two of the top five barriers identified; 'knowledge and motivation' and 'education of staff', were considered 'care-provider' characteristics. 'Availability of supporting staff' such as a lack of a fall nurse specialist or change champion, and 'access to facilities' such as lack of resources or equipment, for example bed alarms, were categorized as 'context' barriers, while, the factor 'health status of patients' was related to the 'patient' characteristics. Leadership (4.4%; range 3% – 7.2%), didactic benefit (3.8%; range: 2.9% – 5.6%) and attractiveness of the guidelines (6.9%; range: 3.6% – 8.8%); both considered 'innovation' characteristics, were not perceived as major barriers.
Discussion
This study is the first to report an examination of the Singaporean context in which guideline implementation may be influenced by an understanding of the local barriers to change in acute care hospitals so as to assist in the process of selecting and more appropriately targeting implementation strategies locally. Advocates for an evidence-based approach to guideline implementation have advised that prior to choosing one or more interventions, decision-makers need an understanding of the target group and setting and potential facilitators of, and barriers to change [38]. The results of our study will inform the development of implementation strategies targeting the barriers to change, to facilitate the role of MOH in ensuring the effective implementation of CPGs and adoption of evidence-based practice.
The barriers most frequently mentioned by nurses in this study were related to care providers and the context in which practice occurred. Specifically, care provider characteristics, such as knowledge and motivation, were nominated as important barriers to implementation of guidelines by 82.4% of nurses, which is similar to the findings of other international studies [51, 52]. The expanding body of research and the increasing emphasis on evidence-based practice make it difficult for any practitioner to be aware of, familiar with, and able to critically apply, every applicable guideline to practice [53, 54]. This is especially so in the Singapore context where 19% of nurses hold a Bachelors or Masters university qualifications (Singapore Nursing Board, 2005). This concern is also highlighted in this study in which the majority of nurses (65%) are either certificate-trained in the technical institute or possess only a diploma in nursing from the polytechnic. These nurses were neither exposed to research nor evidence-based practice within their curriculum. Moreover, our results indicate that 66% of respondents had no research experience and even fewer (24%) had a degree qualification. These results are not surprising in the Singapore context, where nurses are starting to work towards attainment of degree qualifications.
A systematic review of the literature to identify barriers to guideline adherence yielded similar results to those found in the present study, identifying care provider characteristics, particularly knowledge, as a highly reported barrier in 38% of surveys [52]. Our findings are also similar to those of Peters et al. [51], in three different implementation studies in the Netherlands involving 190 general practitioners (GPs); 40 GPs; and 160 midwives respectively. Eighty percent reported knowledge and motivation as a perceived barrier to change.
Appropriate knowledge and attitudes are necessary, but not sufficient, for guideline adherence [55]. Practitioners may still encounter barriers to adoption of guideline recommendations due to the guideline itself, patient, or social/environmental factors [52]. Furthermore, adherence to guidelines may require changes that are beyond the control of the practitioner, such as acquisition of resources or facilities [56, 57]. This is clearly a challenging area that hospitals need to explore given their tight budgets and restrictions to additional resources. Context factors, such as lack of equipment or facilities; insufficient staff; and lack of opinion leaders, described by respondents as barriers in the study by Cabana et al [52], were congruent with those context characteristics identified in our study. This study found a high percentage of respondents (73.3%) perceived a lack of facilities and equipment such as bed alarms to be a barrier to the implementation of guidelines.
Currently, in the Singapore context, the MOH guidelines are simply disseminated to nurses through distribution the hospital wards in conjunction with a single 'road-show' to inform them of the publication. Seventy-seven per cent of respondents reported 'availability of supporting staff' as a barrier to implementation of guidelines. These findings were consistent with international studies where perceptions of general practitioners similarly identified lack of supporting staff as a barrier to change [51, 58] This finding clearly highlighted the critical need for appropriate facilitation which has been echoed by PARIHS [36]. The nurses also perceived that a change champion or a facilitator leading and supporting the change to implement the guidelines in their respective hospitals would result in change in their practice.
Leadership is vital in effective guideline implementation [28, 32, 35, 37]. It is encouraging that few nurses in the present study (4.4%) perceived leadership as a barrier to implementation. It could be argued that this illustrates that the nurses believe that their current leadership provides strong support and direction when guidelines are implemented.
The inability to reconcile patient characteristics (health status and ethnicity) with guideline recommendations was also identified as a barrier to change and these results are similar to those of other studies. This particularly could be explained by the multi-racial context in Singapore where nurses find such cultural differences difficult when implementing certain recommendations in the guideline, such as lack of interpreters to inform patients about risk of falling.
It is encouraging to note that most respondents in our study did not rate any 'innovation' characteristics as barriers to the implementation of guidelines which suggests that the nurses believe in the innovation and evidence, and find the recommendations of the guideline to be compatible with their daily practice. These results were similar to the reported perceptions of midwives in the study by Peters et al[51] It is possible the reason nurses believed the characteristics of the innovation did not present barriers to implementation is that the Fall Prevention CPG was locally adapted by the MOH workgroup, making it relevant to, and compatible with, the Singapore context [51, 52].
Change management theories are instructive when implementing strategies to facilitate change in practice. There is no single change theory that dominates behavioral change and many concepts in different theories overlap [38]. However, change theories are helpful in explaining behavior and nurses' propensity to change practice following the implementation of the CPG at acute care hospitals in Singapore.
The environmental context within which the nurses practice is a key determinant of guideline adoption to facilitate a change in practice. Behavioral theory based on conditioning and controlling behavior, emphasizes the importance of the environmental context of behavior, suggesting that environmental cues and reinforcements are central in encouraging and maintaining behaviour [59]. The main strategies used in the present study, consistent with the stimuli that Skinner described were: reviewing performance and providing feedback to care providers, giving reminders, providing incentives and instituting sanctions such as policies related to specific actions. Environmental and organizational supports, which enabled and reinforced the use of the CPG, operated at two levels in the acute care settings in Singapore. At the clinical level, strategies such as reminders, which integrated the CPG into the process of care, were found to provide important environmental support for change. Organizational supports for guideline implementation such as policy revision to comply with the Fall Prevention CPG and accreditation standards, were important stimuli for change in practice. It has been suggested that the provision of such environmental and organizational support can help to build positive attitudes among care providers, which strengthens the drive for change [60].
Social influence theory emphasizes the role of others in decision making about behavior, postulating that factors such as customs, habits, beliefs of peers and prevailing practices and social norms shape the change of practice [61]. Social influence theory can help to expand our understanding of the social processes which influence success of guideline implementation. Strategies to promote behavior change through social influence, including the use of change champions [62] and educational sessions [63] have been shown to be effective and were used in the present study. The opinions of peers and change champions play a major part in influencing the attitudes of care providers and, most importantly, their decisions to change practice [64–66]. The value of this approach lies in its emphasis on professional communication, whereby care providers constantly look to each other for support, approval, role models, information, and feedback. Collectively, these theories were useful in guiding development of the multifaceted intervention to target barriers to change, promote clinical behavior change, and ultimately improve patient care and outcomes.
Guided by theories of practice change [25–29], the implementation strategy (Table 4) targeted perceived barriers to implementation of guidelines identified in the present study. Interventions included conduct of educational sessions; facilitation and support by change champions including a fall nurse specialist; allocation of resources and equipment; revision of the hospital fall prevention policy; reminders and identification systems; and audit and feedback.
Study Limitations
Reporting bias associated with the self-report method raises questions about the extent to which the responses accurately represent nurses' actual experiences of barriers to change. That is, nurses may have reported 'socially acceptable' responses when completing the questionnaire. The written survey could have excluded other responses or items that were perceived by nurses as barriers to change. Additionally, there was limited psychometric testing of the revised tool, given that six questions were removed and six questions were reworded to address the practice guideline. The re-worded questions were pilot tested for understandability and relevance in the Singapore context, but have not undergone extensive psychometric testing.
Conclusion
In conclusion, a survey design was used to elicit nurses' perceptions regarding barriers to implementation of the Fall Prevention CPG in their practice setting. The greatest barriers to implementation of guidelines reported included: 1) lack of knowledge and education and motivation of staff; 2) lack of change champions availability of support staff; and 3) lack of access to resource facilities. The findings of this study informed the development of a multifaceted strategy, with tailored interventions designed to target the identified barriers to implementation of the Fall Prevention CPG, so as to promote guideline implementation and evidence-based nursing practice in Singapore.
References
Buchan H, Sewell JR, Sweet M: Translating evidence into practice. The Medical Journal of Australia. 2004, 180: S43.
Closs SJ, Cheater FM: Utilisation of Nursing Research: Culture, Interest and Support. Journal of Advanced Nursing. 1994, 19: 762-773. 10.1111/j.1365-2648.1994.tb01149.x.
Davies BL: Sources and models for moving research evidence into clinical practice. Journal of Obstetrics, Gynecologic, & Neonatal Nursing. 2002, 31: 558-562. 10.1111/j.1552-6909.2002.tb00081.x.
Hutchinson AM, Johnston L: Bridging the divide: a survey of nurses' opinions regarding barriers to, and facilitators of, research utilization in the practice setting. Journal of Clinical Nursing. 2004, 13: 304-315. 10.1046/j.1365-2702.2003.00865.x.
Funk SG, Champagne MT, Wiese RA, Tornquist EM: Barriers to Using Research Findings in Practice: The Clinician's Perspective. Applied Nursing Research. 1991, 4: 90-95.
Hunt J: Barriers to research utilization. Journal of Advanced Nursing. 1996, 23: 423-425. 10.1111/j.1365-2648.1996.tb00001.x.
Bryar RM, Closs SJ, Baum G, Cooke J, Griffiths J, Hostick T, Kelly S, Knight S, Marshall K, Thompson DR: The Yorkshire BARRIERS project: diagnostic analysis of barriers to research utilisation. International Journal of Nursing Studies. 2003, 40: 73-84. 10.1016/S0020-7489(02)00039-1.
Slutsky J: Using Evidence-Based Practice Guidelines: Tools for Improving Practice. Evidence-Based Practice in Nursing & Healthcare A guide to best practice. Edited by: Melnyk BM, Fineout-Overholt E. 2005, Philadelphia: Lippincott Williams & Wilkins
Institute of Medicine: Guidelines for clinical practice. From development to use. Edited by: Field MJ, Lohr KN. 1992, Washington: National Academy Press
Eccles M, Grimshaw J: Selecting, presenting and delivering clinical guidelines: Are there any "magic bullets"?. The Medical Journal of Australia. 2004, 180: S52-54.
Grimshaw J, Russell I: Effect of clinical guidelines on medical practice: a systematic review of rigorous evaluations. Lancet. 1993, 342: 1317-1322. 10.1016/0140-6736(93)92244-N.
Grimshaw J, Freemantle N, Wallace S, Russell I, Hurwitz B, Watt I, Long A, Sheldon T: Developing and implementing clinical practice guidelines. Quality in Health Care. 1995, 4: 55-64.
Grol R: Successes and Failures in the Implementation of Evidence-Based Guidelines for Clinical Practice. Medical Care. 2001, 39: II–46-II–54. 10.1097/00005650-200108002-00003.
Woolf SH, Grol R, Hutchinson A, Eccles M, Grimshaw J: Clinical guidelines: Potential benefits, limitations, and harms of clinical guidelines. British Medical Journal. 1999, 318: 527-530.
Lomas J, Anderson GM, Domnick-Pierre K, Vayda E, Enkin MW, Hannah WJ: Do practice guidelines guide practice? The effect of a consensus statement on the practice of physicians. New England Journal of Medicine. 1989, 321: 1306-1311.
Kanouse DE, Winkler JD, Kosecoff Jea: Changing medical practice through technology assessment: An evaluation of the NIH consensus development program. 1989, Santa Monica, Calif: RAND
Woolf SH: Practice guidelines: A new reality in medicine, III: impact on patient care. Archives of Internal Medicine. 1993, 153: 2646-2655. 10.1001/archinte.153.23.2646.
Hayward RSA: Clinical practice guidelines on trial. Canadian Medical Association Journal. 1997, 156: 1725-1727.
Grimshaw J, Thomas R, MacLennan G, Fraser C, Ramsay C, Vale L, Whitty P, Eccles M, Matowe L, Shirran L, et al: Effectiveness and efficiency of guideline dissemination and implementation strategies. Health Technology Assessment. 2004, 8: iii-iv. 1–72.
Thomas L, Cullum N, McColl E, Rousseau N, Soutter J, Steen N: Guidelines in professions allied to medicine. The Cochrane Library. 2004, Chichester, UK: John Wiley & Sons, Ltd, 3
Bero LA, Grilli R, Grimshaw JM, Harvey E, Oxman AD, Thomson MA: Getting research findings into practice: Closing the gap between research and practice: an overview of systematic reviews of interventions to promote the implementation of research findings. British Medical Journal. 1998, 317: 465-468.
Grimshaw J, Shirran L, Thomas R, Mowatt G, Fraser C, Bero L, Grilli R, Harvey E, Oxman A, O'Brien M: Changing Provider Behavior: An Overview of Systematic Reviews of Interventions. Med Care. 2001, 39 (8 suppl 2): II2-45. 10.1097/00005650-200108002-00002.
Oxman AD, Thomson MA, Davis DA, Haynes B: No magic bullets: A systematic review of 102 trials of interventions to improve professional practice. CMAJ. 1995, 153 (10): 423-431.
Foxcroft DR, Cole N: Organisational Infrastructures to Promote Evidence Based Nursing Practice (Cochrane Review). The Cochrane Library. The Cochrane Database of Systematic Reviews. 2005, Chichester, UK: John Wiley & Sons, Ltd, 2007: 4
Cheater FM, Closs SJ: The Effectiveness of Methods of Dissemination and Implementation of Clinical Guidelines for Nursing Practice: A Selective Review. Clinical Effectiveness in Nursing. 1997, 1: 4-15. 10.1016/S1361-9004(97)80022-2.
Grol R: Personal paper: Beliefs and evidence in changing clinical practice. British Medical Journal. 1997, 315: 418-421.
Wensing M, Laurant M, Hulscher M, Grol R: Methods for identifying barriers and facilitators for implementation. Changing Professional Practice Theory and Practice of Clinical Guidelines Implementation. Edited by: Thorsen T, Makela M. 1999, Copenhagen: DSI, 119-132.
McCormack B, Kitson A, Harvey G, Rycroft-Malone J, Titchen A, Seers K: Getting evidence into practice: the meaning of 'context'. Journal of Advanced Nursing. 2002, 38: 94-104. 10.1046/j.1365-2648.2002.02150.x.
Rycroft-Malone J, Seers K, Titchen A, Harvey G, Kitson A, McCormack B: What counts as evidence in evidence-based practice?. Journal of Advanced Nursing. 2004, 47: 81-90. 10.1111/j.1365-2648.2004.03068.x.
Oxman AD, Flottorp S: An overview of strategies to promote implementation of evidence based health care. Evidence-based practice in primary care. Edited by: Silagy C, Haines A. 2001, London: BMJ Books, 91-109.
NHS Centre for Reviews and Dissemination: Getting evidence into practice. Effective Health Care. 1999, 5: 1-15.
Rycroft-Malone J: The PARIHS Framework – A Framework for Guiding the Implementation of Evidence-based Practice. Journal of Nursing Care Quality. 2004, 19: 297-304.
Kitson A, Harvey G, McCormack B: Enabling the implementation of evidence-based practice: A conceptual framework. Quality in Health Care. 1998, 7: 149-158.
Rycroft-Malone J, Kitson A, Harvey G, McCormack B, Seers K, Titchen A, Estabrooks C: Ingredients for change: Revisiting a conceptual framework. Qual Saf Health Care. 2002, 11 (2): 174-180. 10.1136/qhc.11.2.174.
Rycroft-Malone J, Harvey G, Kitson A, McCormack B, Seers K, Titchen A: Getting evidence into practice: Ingredients for change. Nursing Standard. 2002, 16: 38-43.
Harvey G, Loftus-Hills A, Rycroft-Malone J, Titchen A, Kitson A, McCormack B, Seers K: Getting evidence into practice: the role and function of facilitation. Journal of Advanced Nursing. 2002, 37: 577-588. 10.1046/j.1365-2648.2002.02126.x.
Rycroft-Malone J, Harvey G, Seers K, Kitson A, McCormack B, Titchen A: An exploration of the factors that influence the implementation of evidence into practice. Journal of Clinical Nursing. 2004, 13: 913-924. 10.1111/j.1365-2702.2004.01007.x.
Grol R, Grimshaw J: Evidence-based implementation of evidence-based medicine. Joint Commission Journal on Quality Improvement. 1999, 25: 503-513.
Grol R, Wensing M: What drives change? Barriers to and incentives for achieving evidence-based practice. The Medical Journal of Australia. 2004, 180: S57-60.
Grol R, Grimshaw J: From best evidence to best practice: effective implementation of change in patients' care. Lancet. 2003, 362: 1225-1230. 10.1016/S0140-6736(03)14546-1.
Fonda D, Cook J, Sandler V, Bailey M: Sustained Reduction in Serious Fall-Related Injuries in Older People in Hospital. The Medical Journal of Australia. 2006, 184: 379-382.
Helm van der J, Goossens A, Bossuyt P: When Implementation Fails: The Case of a Nursing Guideline for Fall Prevention. Jt Comm J Qual Patient Saf. 2006, 32 (3): 152-160.
Semin-Goossens A, Helm Van der JMJ, Bossuyt PMM: A failed model-based attempt to implement an evidence-based nursing guideline for fall prevention. Journal of Nursing Care Quality. 2003, 18: 217-225.
Koh SSL, Manias E, Hutchinson A, Johnston L: Fall incidence and fall prevention practices at acute care hospitals in Singapore: a retrospective audit. Journal of Evaluation in Clinical Practice. 2007, 13: 722-727. 10.1111/j.1365-2753.2006.00743.x.
Lane AJ: Evaluation of the fall prevention program in an acute care setting. Orthopaedic Nursing. 1999, 18: 37-43. 10.1097/00006416-199911000-00008.
Poe S, Cvach M, Gartrell D, Radzik B, Joy T: An Evidence-based Approach to Fall Risk Assessment, Prevention, and Management: Lessons Learned. Journal of Nursing Care Quality. 2005, 20: 107-116.
Morse JM: Preventing patient falls. 1996, London: Sage publications
Gryfe C, Amies A, Ashley M: A longitudinal study on falls in an elderly population. Incidence and morbidity. Age and Ageing. 1977, 6: 201-210. 10.1093/ageing/6.4.201.
Robertson MC, Campbell AJ: Preventing falls and fall-related injuries in the elderly: A literature review. 1993, Dunedin, New Zealand: Fall Prevention Research Group
Chen YC, Lin LH, Jeng SF: The impacting factors of hospitalised patient injurious falls and the correlation with the consumption of medical resources. Tzu Chi Nursing Journal. 2002, 1: 66-76.
Peters MAJ, Harmsen M, Laurant MGH, Wensing M: Barriers to and facilitators for improvement of patient care. 2002, Nijmegen, the Netherlands: Centre for Quality of Care (WOK), Radboud University Nijmegen Medical Centre
Cabana MD, Rand CS, Powe NR, Wu AW, Wilson MH, Abboud P-AC, Rubin HR: Why Don't Physicians Follow Clinical Practice Guidelines?: A Framework for Improvement. Journal of the American Medical Association. 1999, 282: 1458-1465. 10.1001/jama.282.15.1458.
Lomas J: Retailing research: Increasing the role of evidence in clinical services for childbirth. The Milbank Quarterly. 1993, 71: 439-475. 10.2307/3350410.
Stross JK, Harlan WR: The dissemination of new medical information. Journal of the American Medical Association. 1979, 241: 2622-2624. 10.1001/jama.241.24.2622.
Solberg LI, Brekke ML, Kottke TE: How important are clinician and nurse attitudes to the delivery of clinical preventive services?. Journal of Family Practice. 1997, 44: 451-461.
Resnicow KA, Schorow M, Bloom HG, Massad R: Obstacles to family practitioners use of screening tests: Determinants of practice?. Preventive Medicine. 1989, 18: 101-112. 10.1016/0091-7435(89)90057-1.
Kosecoff J, Kanouse DE, Rogers WH, McCloskey L, Winslow CA, Brook RH: Effects of the National Institutes of Health Consensus Development Program on Physician Practice. Journal of the American Medical Association. 1987, 258: 2709-2713.
Dijkstra R, Braspenning J, Uilers E, van Ballegooie E, Grol R: Perceived barriers to the implementation of diabetes guidelines in hospitals in the Netherlands. The Netherlands Journal of Medicine. 2000, 56: 80-85. 10.1016/S0300-2977(99)00123-0.
Skinner B: The behaviour of organisms: an experimental analysis. 1938, New York: Appleton-Century
Petrie JC, Grimshaw JM, Bryson A: The Scottish intercollegiate guidelines network initiative: SIGN – getting validated guidelines into practice. Health Bulletin. 1995, 53: 345-348.
Mittman BS, Tonesk X, Jacobson PD: Implementing clinical practice guidelines: social influence strategies and practitioner behavior change. Quality Review Bulletin. 1992, 18: 413-422.
Lomas J, Enkin M, Anderson G, Vayda E, Hannah W, Singer J: Opinion leaders vs audit and feedback to implement practice guidelines. Delivery after previous cesarean section. Journal of the American Medical Association. 1991, 265: 2202-2207. 10.1001/jama.265.17.2202.
Soumerai SB, Avorn J: Principles of educational outreach ('academic detailing') to improve clinical decision making. Journal of the American Medical Association. 1990, 263: 549-556. 10.1001/jama.263.4.549.
Thomson MA, Oxman AD, Haynes RB: Outreach visits to improve health care professional practice and health care outcomes (Cochrane Review). The Cochrane Library. 1998, Oxford, UK.: Update Software, 2
Thomson MA, Oxman AD, Haynes RB: Local opinion leaders to improve health professional practice and health care outcomes (Cochrane Review). The Cochrane Library. 1999, Oxford, UK: Update Software, 2
Wensing M, Grol R: Single and Combined Strategies for Implementing Changes in Primary Care: A Literature Review. International Journal for Quality in Health Care. 1994, 6: 115-132.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6963/8/105/prepub
Acknowledgements
This research was supported by a grant from the MOH (Singapore) Nursing Research Committee. The assistance of Ms Jesbindar Kaur, Ms Rubavathy Muthu, Ms Siti Zubaidah, Mr Wong Yew Hong, and Ms Lee Jin Yih is gratefully acknowledged.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
SSLK, EM, AMH, LJ study design, SSLK, SD data analysis, SSLK, EM, AMH, LJ manuscript preparation, SSLK literature review.
Serena SL Koh, Elizabeth Manias, Alison M Hutchinson and Linda Johnston contributed equally to this work.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Koh, S.S., Manias, E., Hutchinson, A.M. et al. Nurses' perceived barriers to the implementation of a Fall Prevention Clinical Practice Guideline in Singapore hospitals. BMC Health Serv Res 8, 105 (2008). https://doi.org/10.1186/1472-6963-8-105
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6963-8-105