
Abstract
Background
KRAS mutations represent key alterations in colorectal cancer development and lead to constitutive EGFR signaling. Since EGFR inhibition represents a therapeutic strategy in advanced colorectal cancer, KRAS mutation analysis has quickly been introduced as a treatment-predictive test.
Methods
We used a real-time PCR based method to determine KRAS mutations in 136 colorectal cancers with mutations identified in 53 (39%) tumors.
Results
KRAS mutations were significantly more often found in rectal cancer (21/38, 55%) than in colon cancer (32/98, 33%) (P = 0.02). This finding was explained by marked differences mutation rates in female patients who showed mutations in 33% of the colon cancers and in 67% of the rectal cancers (P = 0.01). Concurrent KRAS mutations were identified in three tumors; two colorectal cancers harbored Gly12Asp/Gly13Asp and Gly12Cys/Gly13Asp and a third tumor carried Gly12Cys/Gly12Asp in an adenomatous component and additionally acquired Gly12Val in the invasive component.
Conclusion
The demonstration of a particularly high KRAS mutation frequency among female rectal cancer patients suggests that this subset is the least likely to respond to anti-EGFR therapies, whereas the observation of concurrent KRAS mutations imply that repeated KRAS targeting may occur during tumor progression in a subset of colorectal cancers.
Similar content being viewed by others

Background
Inhibition of the epidermal growth factor receptor (EGFR) signaling pathway represents a therapeutic option in advanced colorectal cancer. Improved response rates and prolonged time to metastasis/survival has been demonstrated with the currently registered EGFR blocking antibodies cetuximab and panitumumab, and additional EGFR inhibitors are in various stages of clinical trials. Mutations in the KRAS oncogene typically occur already in the late adenoma stage and have since long been recognized as a key event in colorectal cancer development [1]. Overall, KRAS mutations are found in about 40% of the tumors and are predominantly located in codons 12 (82% of the mutations reported) and 13 (17%) http://www.sanger.ac.uk/genetics/CGP/cosmic. Activating mutations lead to permanently GTP bound KRAS and constitutive downstream pathway signaling, also in the absence of upstream EGFR stimulation. Presence of KRAS mutations therefore represents a negative predictor of response to EGFR therapy and KRAS mutation testing has rapidly moved into the molecular diagnostic work-up of colorectal cancers considered for EGFR treatment [2, 3]. Quality assurance programs for KRAS mutation testing and practice guidelines related to e.g. optimal testing material, methodological considerations and recommendations for the reporting of the results are currently being developed [4]. PCR-based assays constitute the cornerstone for clinical KRAS testing since these analyses allow high-throughput testing and have a favorable sensitivity, also in samples with low tumor cell content. We report the experiences from our first 136 treatment-predictive KRAS tests and herein report significant differences in mutation frequencies in colon cancer and rectal cancer and coexisting KRAS mutations in a subset of the tumors.
Methods
KRAS mutation testing was performed in 136 adenocarcinomas of the colon (n = 98) and the rectum (n = 38). The mean age was 56 (21-81) years and the series included 64 (47%) females. Representative tumor blocks were selected and were in the majority of the cases derived from the primary tumor, in 13 cases from metastatic tissue and in four cases from a local recurrence. Presence of at least 20% tumor cells in the tissue was verified by a pathologist. DNA was extracted from serial sections of formalin-fixed, paraffin-embedded tumor tissue using the Qiamp DNA FFPE tissue Kit (Qiagen, Hilsen, Germany) according to the manufacturer's recommendations. Standard clinical analysis applied the DxS real-time PCR based kit (Roche Diagnostics, Basel, Switzerland), which identifies 7 different KRAS mutations in exons 12 and 13 with high sensitivity. In order to confirm presence of double or triple coexisting mutations, samples with such unusual patterns were also subjected to pyrosequencing (PyroMark™ Q96 KRAS v2.0, Qiagen, Hilsen, Germany) according to the manufacturer's recommendations on PSQ™HS96A [5]. Mutations were quantified using the machine's software. Statistical analysis used a Chi2 test and the level of significance was set at 5%. KRAS mutation testing was carried out as part of standard care, all patients provided informed consent for testing, and the study was conducted according to the Helsinki declaration.
Results
KRAS mutations were identified in 53/136 (39%) colorectal cancers. Overall, mutation status did not correlate with sex when analyzed in the whole cohort with mutations in 28/64 (44%) women and in 5/72 (35%) men (P = 0.28) or age (mean age 55 years in the mutant group and 57 years in the wild-type group). KRAS mutations, however, significantly correlated with tumor location with mutations found in 32/98 (33%) colon cancers and 21/38 (55%) rectal cancers (P = 0.02; Chi2-test). This difference was related to a high mutation rate in female rectal cancer patients (14/21, 67%) compared to females with colon cancer (14/43, 33%) (p = 0.01), whereas no significant difference related to tumor location was identified in men (41% in rectal cancer and 33% in colon cancer, P = 0.52). Though the materials in subsets are small, women with KRAS mutant rectal cancers were diagnosed mean 10 years earlier (mean age 48, range 25-71, years) than those with KRAS wild-type rectal cancers (mean age 58, range 52-70, years).
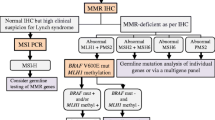
The mutation spectrum revealed the expected codon 12 and 13 mutations with the p.Gly12Asp, p.Gly13Asp, and p.Gly12Val being the most commonly found (table 1) [6]. Three tumors showed two-three different KRAS mutations (figure 1), which were identified using real-time PCR and verified in a separate tumor block and using pyrosequencing as a complementary method. The first case was a colon cancer from a 65-year old man with hereditary nonpolyposis colorectal cancer and a germline mutation in the MLH1 gene. The tumor was found to harbor two KRAS mutations, Gly12Asp (ΔCT value 6.9, cutoff 8) and Gly13Asp (ΔCT value 5.6, cutoff 9). The patient had 10 years earlier developed two synchronous colon cancers, both of which were retrospectively analyzed, but neither of these contained any KRAS mutation (data not shown). The second case was a 68-year old man with a rectal cancer metastatic to the liver. The primary tumor revealed coexisting coexistence of the KRAS mutations Gly12Cys (ΔCT value 5.4, cutoff 7.0) and Gly13Asp (ΔCT 4.8, cutoff 9.0). The third case was a 47-year old woman who presented with a rectal cancer and concurrent liver metastases. The initial biopsy from the rectal tumor revealed only adenomatous components, whereas a second biopsy contained infiltrative adenocarcinoma. Unfortunately, no histologic sample from the liver lesions was available. The tubulovillous adenoma harbored the mutations Gly12Asp (ΔCT value 6.2, cutoff 8.0) and Gly12Cys (ΔCT value 3.9, cutoff 7.0), whereas the sample with also an invasive component contained both these mutations and in addition (contained) a Gly12Val mutation (ΔCT value 4.1, cutoff 6.5). All mutations were identified by real-time PCR and verified using pyrosequencing.

Real-time PCR analysis identified coexisting KRAS mutations in three cases. Case 1) colon cancer with the Gly12Asp and Gly13Asp mutations, Case 2) colon cancer with coexisting Gly12Cys and Gly13Asp mutations, and Case 3) a rectal tumor that revealed Gly12Asp and Gly12Cys in adenomatous components and an additional Gly12Val mutation in the invasive tumor component. All mutations were verified using pyrosequencing. Case 1 contained 12% Gly12Asp and 24% Gly13Asp, and case 2 4% Gly12Cys and 34% Gly13Asp. Case 3 harboured 17% Gly12Asp and 22% Gly12Cys in the adenomatous component, and 10% Gly12Asp, 7% Gly12Cys, and 12% Gly12Val in the invasive component (data not shown).
Discussion
The overall KRAS mutation frequency of 39% is in line with the results from previous studies http://www.sanger.ac.uk/genetics/CGP/cosmic, though the different mutation rates - 33% in colon cancer and 55% in rectal cancer (p = 0.02) - has not been reported in conjunction with treatment-predictive testing. Distinct molecular pathways are preferentially involved in the adenoma-carcinoma sequence in the proximal and the distal colon with TP53 and KRAS mutations being favored in rectal cancer, whereas mismatch repair defects are more common in proximal colon tumors [7]. A higher mutation frequency in rectal cancers compared to colon cancer has previously been described, although the magnitude has been lower than identified herein [8]. The effect seems to be limited to females with rectal cancer, 67% of whom harbored KRAS mutations. This observation is in line with the findings in a large population-based series from the Netherlands in which Brink et al. reported a higher KRAS mutation rate in female rectal cancer patients [8]. Furthermore, in the subset of females with rectal cancer the KRAS mutant tumors were diagnosed mean 10 years earlier (mean age 48 years) behaviour than the wild-type tumors (mean age 58). Though this observation is new and needs confirmation, a recent study has demonstrated that early-onset colorectal cancers frequently show pathologic features associated with aggressive clinical features [9]. The tumors here investigated were selected based on potential EGFR treatment, which may bias the results toward tumors prone to metastatic development, though the overall KRAS mutation frequency of 39% and the relation between colon cancer and rectal cancer are as expected. The differences in KRAS mutation rates identified suggest that sex and tumor location influence the chance of clinical usefulness of EGFR inhibitors with a particularly low likelihood of benefit among female rectal cancer patients.
A stepwise accumulation of mutations in different pathways constitutes a hallmark of colorectal cancer development. The observation of coexisting KRAS mutations in a small number of colorectal cancers, however, suggests that some tumors benefit from repeated targeting of the same pathway. This observation is in line with the association between KRAS mutations and 12p gain in colorectal adenomas [10]. Recently, the "two-hit-hypothesis" was challenged in a study of inactivating APC gene mutations in colorectal cancer, in which three hits - including mutations, deletions, and copy number gain - were demonstrated in a subset of the tumors [11]. APC gene mutations, as well as KRAS mutations, are recognized as early events in colorectal cancer development. Based on our results and previous observations, concurrent KRAS mutations seem to occur in about 3% of colorectal cancers. The majority of these cases show coexisting mutations in codon 12, whereas a smaller number have mutations in different codons (12 and 13 or 12 and another codon) [8, 12–15]. Different KRAS mutations have shown variable efficacy in downstream signaling transduction and also seem to involve different effector molecules [16, 17]. The specific KRAS mutation may thereby influence different aspects of tumor progression, which could explain why repeated KRAS targeting is observed in a subset of colorectal cancer. Interestingly the p.Gly12Val mutation was found in 10 rectal cancers and 4 colon cancers, suggesting an overrepresentation in the former tumor type. This mutation has also been linked to a worse prognosis [16]. The addition of a p.Gly12Val mutation in the invasive component of a tumor already containing dual KRAS mutations (figure 1, case 3) suggests a role for repeated KRAS targeting during tumor progression and serves as a reminder to consider coexisting mutations when unexpected patterns occur in treatment predictive testing.
Conclusion
In conclusion, our experience from predictive testing for KRAS mutations reveal a high mutation frequency (67%) in rectal cancers from females and thus implicates that this subset is the least likely to respond to anti-EGFR therapies. Concurrent KRAS mutations were observed in 3/136 tumors and although it remains a rare finding suggests that repeated KRAS targeting may occur during colorectal cancer progression.
References
Cho KR, Vogelstein B: Genetic alterations in the adenoma-carcinoma sequence. Cancer. 1992, 70: 1727-31. 10.1002/1097-0142(19920915)70:4+<1727::AID-CNCR2820701613>3.0.CO;2-P.
Lindarou H, Dahabreh J, Kanaloupiti D, Siannis F, Bafaloukos D, Kosmidis P, Papadimitriou CA, Murray S: Assessment of somatic k-RAS mutations as a mechanism associated with resistance to EGFR-targeted agents: a systematic review and meta-analysis of studies in advanced non-small-cell lung cancer and metastatic colorectal cancer. Lancet Oncol. 2008, 9: 962-72. 10.1016/S1470-2045(08)70206-7.
Allegra CJ, Jessup JM, Somerfield MR, Hamilton SR, Hammond EH, Hayes DF, McAllister PK, Morton RF, Schilsky RL: American Society of Clinical Oncology provisional clinical opinion: testing for KRAS gene mutations in patients with metastatic colorectal carcinoma to predict response to anti-epidermal growth factor receptor monoclonal antibody therapy. J Clin Oncol. 2009, 27: 2091-6. 10.1200/JCO.2009.21.9170.
Van Krieken JHJM, Jung A, Kirchner T, et al: KRAS mutation testing for predicting response to anti-EGFR therapy for colorectal carcinoma: proposal for an European quality assurance programme. Virchow Arch. 2008, 453: 417-31. 10.1007/s00428-008-0665-y.
Ogino S, Kawasaki T, Brahmandam M, Ogino S, Kawasaki T, Brahmandam M, Yan L, Cantor M, Namgyal C, Mino-Kenudson M, Lauwers GY, Loda M, Fuchs CS: Sensitive sequencing method for KRAS mutation detection by Pyrosequencing. J Mol Diagn. 2005, 7: 413-21.
Andreyev HJN, Norman AR, Cunningham D, et al: Kirsten ras mutation sin patients with colorectal cancer: the "RASCAL II" study. Br J Cancer. 2001, 85: 692-6. 10.1054/bjoc.2001.1964.
Iacopetta B: Are there two sides to colorectal cancer?. Int J Cancer. 2002, 101: 403-8. 10.1002/ijc.10635.
Brink M, de Goeij FPM, Weijenberg MP, Brink M, Weijenberg MP, De Goeij AF, Schouten LJ, Koedijk FD, Roemen GM, Lentjes MH, De Bruïne AP, Goldbohm RA, Brandt Van Den PA: K-ras oncogene mutations in sporadic colorectal cancer in the Netherlands cohort study. Carcinogenesis. 2003, 24: 703-10. 10.1093/carcin/bgg009.
Yantiss R, Goodarzi M, Zhou X, Rennert H, Pirog EC, Banner BF, Chen YT: Clinical, pathologic, and molecular features of early-onset colorectal carcinoma. Am J Surg Pathol. 2009, 33: 572-82. 10.1097/PAS.0b013e31818afd6b.
Gattenlohner S, Germer C, Muller-Hermelink H-K: Letter to the editor. N Engl J Med. 2009, 380: 835.
Leslie A, Stewart A, Baty DU, et al: Chromosomal changes in colorectal adenomas: relationship to gene mutations and potential for clinical utility. Genes Chrom Cancer. 2006, 45: 126-35. 10.1002/gcc.20271.
Segditas S, Rowan AJ, Howarth K, et al: APC and the three-hit hypothesis. Oncogene. 2009, 28: 146-55. 10.1038/onc.2008.361.
Miyakura Y, Sugano K, Fukayama N, Konishi F, Nagai H: Concurrent mutations of K-ras oncogene at codons 12 and 22 in colon cancer. Jpn J Clin Oncol. 2002, 32: 219-21. 10.1093/jjco/hyf043.
Martinez-Garza SG, Nunez-Salazar AJ, Calderon-Garciduenas AL, Bosques-Padilla FJ, Niderhauser-García A, Barrera-Saldaña HA: Frequency and clinicopathology associations of K-ras mutations in colorectal cancer in a northeast Mexican population. Dig Dis. 1999, 17: 225-9. 10.1159/000016940.
Moerkerk P, Arends JW, van Driel M, de Bruine A, de Goeij A, ten Kate J: Type and number of Ki-ras point mutations relate to stage of human colorectal cancer. Cancer Res. 1994, 54: 3376-8.
Al-Mulla F, Milner-White EJ, Going J, Birnie G: Structural differences between Valine-12 and Aspartate-12 Ras proteins may modify carcinoma aggression. J Pathology. 1999, 187: 433-38. 10.1002/(SICI)1096-9896(199903)187:4<433::AID-PATH273>3.0.CO;2-E.
Monticone M, Biollo E, Maffei M, Donadini A, Romeo F, Storlazzi CT, Giaretti W, Castagnla P: Gene expression deregulation by KRAS G12D and G12V in a BRAF V600E context. Mol Cancer. 2008, 7: 92-10.1186/1476-4598-7-92.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6890/9/8/prepub
Acknowledgements
This study was supported by the Swedish Cancer Fund, the Medical Research Council and an unrestricted research grant from Merck A/S.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The investigators have received an unrestricted research grant and the principal investigator (M.N.) has in the past five years received lecture honorary from Merck A/S. No other competing interests apply.
Authors' contributions
MJ carried out mutation analysis and drafted the manuscript. AE performed mutation analysis. TE, JE and DB identified and clinically managed patients and herein contributed with clinical data, DG selected tumor tissues, MN planned the study and was responsible for the clinical testing. All authors have contributed to and approved of the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Jönsson, M., Ekstrand, A., Edekling, T. et al. Experiences from treatment-predictive KRAS testing; high mutation frequency in rectal cancers from females and concurrent mutations in the same tumor. BMC Clin Pathol 9, 8 (2009). https://doi.org/10.1186/1472-6890-9-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6890-9-8