
Abstract
Background
In resource poor settings where automated hematology analyzers are not available, the Cyanmethemoglobin method is often used. This method though cheaper, takes more time. In blood donations, the semi-quantitative gravimetric copper sulfate method which is very easy and inexpensive may be used but does not provide an acceptable degree of accuracy. The HemoCue® hemoglobin photometer has been used for these purposes. This study was conducted to generate data to support or refute its use as a point-of-care device for hemoglobin estimation in mobile blood donations and critical care areas in health facilities.
Method
EDTA blood was collected from study participants drawn from five groups: pre-school children, school children, pregnant women, non-pregnant women and men. Blood collected was immediately processed to estimate the hemoglobin concentration using three different methods (HemoCue®, Sysmex KX21N and Cyanmethemoglobin). Agreement between the test methods was assessed by the method of Bland and Altman. The Intraclass correlation coefficient (ICC) was used to determine the within subject variability of measured hemoglobin.
Results
Of 398 subjects, 42% were males with the overall mean age being 19.4 years. The overall mean hemoglobin as estimated by each method was 10.4 g/dl for HemoCue, 10.3 g/dl for Sysmex KX21N and 10.3 g/dl for Cyanmethemoglobin. Pairwise analysis revealed that the hemoglobin determined by the HemoCue method was higher than that measured by the KX21N and Cyanmethemoglobin. Comparing the hemoglobin determined by the HemoCue to Cyanmethemoglobin, the concordance correlation coefficient was 0.995 (95% CI: 0.994-0.996, p < 0.001). The Bland and Altman's limit of agreement was -0.389 - 0.644 g/dl with the mean difference being 0.127 (95% CI: 0.102-0.153) and a non-significant difference in variability between the two measurements (p = 0.843). After adjusting to assess the effect of other possible confounders such as sex, age and category of person, there was no significant difference in the hemoglobin determined by the HemoCue compared to Cyanmethemoglobin (coef = -0.127, 95% CI: -0.379 - 0.634).
Conclusion
Hemoglobin determined by the HemoCue method is comparable to that determined by the other methods. The HemoCue photometer is therefore recommended for use as on-the-spot device for determining hemoglobin in resource poor setting.
Similar content being viewed by others

Background
Hemoglobin (Hb) assessments are the most reliable indicator widely used to screen individuals for anaemia, to draw inferences about the iron status of populations and to evaluate responses to nutritional interventions [1]. The blood Hb concentration is an important variable directing transfusion therapy in patients suffering major blood loss due to accidents, surgery, labour and many other critical conditions [2]. Hb concentration is measured routinely using automated hematology analyzers, such as those produced by the Sysmex Corporation (Kobe, Japan). Although these counters are very accurate and reliable, they are expensive and transport of the samples to the laboratory delays the process which may delay treatment, resulting in preventable deaths [3]. In resource poor settings where automated hematology analyzers are not available, the Cyanmethemoglobin method is often used. Hb estimation by this method though cheaper than the automated method takes more time [4]. In blood donations, the semi-quantitative gravimetric copper sulfate method which is very easy and inexpensive may be used, but does not provide an acceptable degree of accuracy [5, 6]. The HemoCue® Hb photometer has been widely used for these purposes in recent years [7] because it is portable, requires only a small sample of capillary/venous blood, is relatively inexpensive and simple to use, does not require access to refrigeration or even electricity, and gives immediate, digitally displayed results [3]. However, data to support the use of this device for all categories of patients in resource limited areas of Ghana is not available. This study was therefore conducted to generate data to support or refute its use as a point-of-care device for Hb estimation, mobile blood donations and critical care areas in health facilities.
Methods
Study Subjects
A total of 398 consented study patients were involved in this study. They were placed in five groups: pre-school children (subjects within 1-4 years), school children (subjects within 5-14 years), pregnant women (No age limit), non-pregnant women (female subjects within 15-59 years) and men (male subjects within 15-59 years).
Study Design
This was a hospital-based study conducted at the Agogo Presbyterian Hospital in the Asante Akim North District (AAND), Ashanti Region, Ghana. Blood samples were collected from consented participants within the study group reporting to the hospital after study procedures had been explained to them. EDTA blood samples taken from patients for routine laboratory investigations were used for the study thus no extra blood was collected except for patients in which EDTA blood was not taken, in which case venous blood was taken from the arm. Venous blood collected from participants was processed to estimate their Hb content using three different methods (HemoCue®, Sysmex KX21N and Cyanmethemoglobin).
Study Site
The Agogo Presbyterian Hospital in Agogo was the study site. This is the major hospital serving the Asante-Akim North District and other parts of the Ashanti region. The main departments of the hospital are the Children's, Casualty, Surgical, Medical, Obstetrics and Gynecology, Eye and the laboratory Departments. The laboratory department of the hospital offers diagnostic as well as research services. The department is fully equipped and has functional Microbiology, Hematology, Parasitology and Clinical Chemistry departments. The laboratory participates in various External Quality Assessment programmes one of which is the United Kingdom National External Quality Assessment Service (UK NEQAS) in hematology. Among the most prevalent diseases in the district are malaria, buruli ulcer, typhoid fever and tuberculosis.
Ethical Approval
Ethical approval for this study was obtained from the Committee on Human Research, Publication and Ethics (CHRPE), of the School of Medical Sciences, KNUST-Kumasi. After information and appropriate explanations, adults or parents/legal guardians of children willing to participate in the study had to give their consent by appending their signature or thumbprint to the informed consent form before any study related procedures were done.
HemoCue® Portable Photometer
The HemoCue® B-Hemoglobin system (HemoCue AB, Ängelholm, Sweden) consists of disposable microcuvettes containing reagent in a dry form and a single purpose designed photometer. The microcuvettes were stored in a dry place at room temperature. Once opened, they were tightly closed and stored at the same conditions to maintain their integrity and shelf life. The reaction in the microcuvette is a modified azide-methemoglobin reaction. Sodium deoxycholate haemolyses erythrocytes and hemoglobin is released. Sodium nitrite converts hemoglobin to methemoglobin which, together with sodium azide, gives azidemethemoglobin. The absorbance is measured at two wavelengths (570 nm and 880 nm) in order to compensate for turbidity in the sample. The test was performed as stated by the manufacturer [8].
Sysmex KX21N Hematology Analyzer
The Sysmex KX21N (Sysmex Corporation, Kobe, Japan) is an automated blood cell counter intended for in vitro diagnostic use in clinical laboratories. It is a compact, fully automated hematology analyzer with simultaneous analysis of 18 parameters in whole blood mode and capillary blood mode. It measures the hemoglobin concentration using a non-cyanide hemoglobin method (STROMATOLYSER WH). The instrument has been proven to provide accurate and reliable results including hemoglobin concentrations [9, 10]. The test was performed as stated in the manufacturer's manual [11].
Cyanmethemoglobin Method
The principle of this method lies in conversion of hemoglobin to cyanmethemoglobin by the addition of Potassium cyanide and ferricyanide whose absorbance is measured at 540 nm in a photoelectric calorimeter against a standard solution. The test was performed as outlined by Bhaskaram et al [12].
Quality Control
The function of the HemoCue photometer was checked on a daily basis by measuring the control cuvette (Serial no: 0214-003 071) and a standard of known concentration. A three set EIGHTCHECK-3WP controls (Low, Normal and High) were run daily to ensure the function of the Sysmex KX21N. For the cyanmethemoglobin, a hemoglobin standard of known concentration was tested daily. Samples were only processed when the QC material had passed.
Statistical Analysis
Data was double-entered into a predesigned electronic database using Epi info version 6.04 (Center for Disease Control, Atlanta, GA, USA) and cleaned on a regular basis. It was then exported to Stata/ SE10.1 statistical software (Stata Corporation, Texas USA) for analysis. A pairwise t-test was used to compare the HemoCue and both the Sysmex and cyanmethemoglobin. Agreement between the test methods was assessed by the method of Bland and Altman [13], where the mean, standard deviation and limit of agreement of paired results were calculated. Figures plotting difference against the average were graphed as Bland and Altman recommended [13]. The Intraclass correlation coefficient (ICC) was used to determine the within subject variability of measured hemoglobin whiles the concordance correlation coefficient (CCC) was used to measure the agreement between the three methods.
Results
The study was carried out from August to December 2010. Three hundred and ninety eight consented study subjects were recruited for the study. Of these, school children constituted the highest population (22.4%) whilst adult males constituted the least (16.6%). Overall, there were fewer males (42%) than females. Whilst adult males had the highest mean age of 34.3 years (range: 16-59 years), pre-school children recorded the least with 2.3 years (range: 1-4 years), with the overall mean age being 19.4 years (range: 1-64 years) (Table 1).
There was a significant but marginal increase in hemoglobin with age (0.03 g/dl/year, p < 0.001). Pre-school and school children recorded the lowest mean hemoglobin concentration of 9.2 g/dl (SD: 2.9) and 9.7 g/dl (SD: 3.1) respectively. This was followed by non-pregnant and pregnant women with mean hemoglobin of 10.7 g/dl (SD: 2.4) and 11.0 g/dl (SD: 1.7) respectively. Adult males had the highest mean hemoglobin of 11.3 g/dl (SD: 3.3). The mean hemoglobin concentration of males was 0.5 g/dl (95%CI: 0.1 to 0.8 g/dl, p = 0.01), higher than that of the females. This effect persisted even after correcting for the age, method used to estimate hemoglobin and study sub-population. Pairwise analysis revealed that the hemoglobin determined by the HemoCue method was higher than that measured by the KX21N and Cyanmethemoglobin with mean differences of 0.15 g/dl (95% CI: 0.12 to 0.17, p < 0.001) and 0.13 g/dl (95%CI: 0.10 to 0.15, p < 0.001) respectively. That measured by the KX21N and Cyanmethemoglobin methods were however not significantly different (0.02 g/dl, 95%CI: 0.00 to 0.04, p = 0.10).
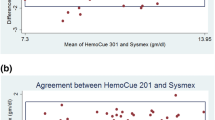
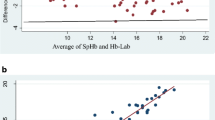
There was near perfect concordance correlation between the hemoglobin concentrations determined by the HemoCue and Cyanmethemoglobin methods (rho = 0.995) as well as HemoCue and KX21N (0.994). These were not significantly different for that between KX21N and the Cyanmethemoglobin method (0.997) (Table 2). Comparing the hemoglobin concentration determined by the HemoCue and Cyanmethemoglobin, the Bland and Altman's limit of agreement was from -0.39 to 0.64 g/dl with the mean difference being 0.13, and a non-significant difference in variability between the two measurements (p = 0.843). For HemoCue and KX21N, the Bland and Altman's limit of agreement was from -0.39 to 0.69 g/dl with a mean difference of 0.15 and a non-significant difference in variability between the two measurements (p = 0.391) (Figure 1, 2).

Bland and Altman plot for HemoCue and Cyanmethemoglobin. Mean of HemoCue and Cyanmethemoglobin (g/dl).

Bland and Altman plot for HemoCue and Sysmex KX21N. Mean of HemoCue and Sysmex (g/dl).
The within subject variability of measured hemoglobin was very minimal with high intraclass correlation coefficient for all the various subgroups (Table 3). The lowest intraclass coefficient was in pregnant women (0.986) and the highest was in school children (0.997). These coefficients were also associated with high estimated reliabilities ranging between 0.995 and 0.999.
After adjusting to assess the effect of other possible confounders such as sex, age and category of person, there was no significant difference in the hemoglobin determined by the HemoCue compared to Cyanmethemoglobin (coef = -0.127, 95%CI: -0.379 - 0.634) and that by HemoCue compared to Sysmex KX21N (coef = -0.147, 95%CI: -0.676 - 0.382).
Discussion
Accurate determination of hemoglobin concentration is a common element in assessing the extent of anemia and making a decision whether transfusion is necessary or not. This decision should be made based on reliable and rapidly assessed laboratory tests. In settings where a central laboratory is used for the purposes of testing and transfusion monitoring, the time loss for blood sample transportation create delays which may lead to the loss of lives[3, 12].
The HemoCue is a portable device for measuring hemoglobin concentration [14] and it requires very little staff training thus making it a very useful tool in resource limited areas, critical care areas such as the theatre, pediatric ward, maternity, intensive care units etc as well as at field conditions since it can easily be transported. In this study, we compared it with the Cyanmethemoglobin method and the Sysmex KX21N used in the laboratory. We found no significant differences in the hemoglobin concentrations determined by all the three methods, with no perceptible trend for disagreement with high or low values. The three devices had comparable concordance correlation coefficient, limits of agreement and intraclass correlation coefficients thus supporting the use of the HemoCue portable photometer among the various study groups in our study setting.
Our study is in agreement with other studies conducted in other settings to support the use of the device. These include the studies conducted by von Schenck et al [15], Van de Louw et al; among patients with gastrointestinal bleeding [16], Rippmann et al; among surgical patients [17], Bridges et al; on repeated measurement of one sample [7], Neville; within urban general practice [18], Rechner et al; among neonates [19], Lardi et al; among patients undergoing aortic surgery in the theatre [14], Sari et al; among Indonesian mothers [4] and Radtke et al; among blood donors [20].
Nevertheless, other studies such as that conducted by Zhou et al; among pregnant women in a higher altitude area of Tibet, China [21] and Bhaskaram et al; among apparently healthy children of 1-6 years [12] do not support the use of the HemoCue in their various study populations.
The cyanrnethemoglobin method is a widely used method of estimating Hb. However, several reports indicate that results obtained using this method could be imprecise due to a number of factors: turbidity of the blood and the large dilution of the sample (20 μL of blood in 5 mL of Drabkin's solution) [22–24], it requires skillful technical operations in terms of accurate uptake of the blood volume into a calibrated hemoglobin pipette, careful mixing of the sample with the Drabkin's solution, measurement of absorbance in the photometer and calculation of actual value from a systematically constructed standard graph [12]. All these manual operations are time consuming and make the method unsuitable for large scale field/community studies. It is also well documented that conditions such as hyperlipemia [23] and Waldenstrom's macroglobulinemia [25] can cause falsely high results for hemoglobin in the filter photometer method such as the cyanmethemoglobin method.
The HemoCue is a portable machine which directly measures Hb from an undiluted blood sample [8] and background turbidity of the samples are corrected due to the measurement of two-wave lengths [15]. This method is quicker (60 seconds), simple to operate thus making it faster with a shorter turn-around time. In addition, it requires less blood (10 μL), is cost effective and a more accurate method [12, 16, 19] as well as having other properties as stated by Sari et al [4] and Sawant et al [26]. Issues of cost have also been being reported as a factor to take into account when considering Hb estimation with the HemoCue [4, 18, 26]. The mechanical filling of the cuvettes with 10 μl of the blood by capillary action avoids several manual errors which often occur in the collection, dilution and measurement of the sample in the cyanmethemoglobin method. Nevertheless, the presence of air bubbles, excess blood on the back of the cuvettes, over filling of the cuvettes and insufficient mixing of the samples may lead to erroneous results. These factors even though reduced to the barest minimum might have contributed to the higher Hb concentration observed in our study as also reported in other studies [14, 15, 17, 18]. However, by offering adequate training on the technique of proper filling the cuvettes to avoid air bubbles and over filling, mixing samples adequately but gently and wiping off excess blood from the cuvettes without reducing the blood quantity, these errors can be easily avoided.
Conclusion
Hemoglobin determined by the HemoCue method is comparable to that determined by both the Cyanmethemoglobin and Sysmex KX21N methods. The HemoCue photometer is therefore recommended for use as on-the-spot device for determining hemoglobin in resource limited areas as well as critical care areas of health facilities.
References
Morris SS, Ruel MT, Cohen RJ, Dewey KG, de la Briere B, Hassan MN: Precision, accuracy, and reliability of hemoglobin assessment with use of capillary blood. Am J Clin Nutr. 1999, 69 (6): 1243-1248.
Worldwide prevalence of anaemia 1993-2005: WHO global database on anaemia. [http://whqlibdoc.who.int/publications/2008/9789241596657_eng.pdf]
Jahr JS, Lurie F, Driessen B, Davis JA, Gosselin R, Gunther RA: The HemoCue®, a point of care B-hemoglobin photometer, measures hemoglobin concentrations accurately when mixedin vitro with canine plasma and three hemoglobin-based oxygen carriers (HBOC). Can J Anesth/j Can Anesth. 2002, 49 (3): 243-248.
Sari M, dePee S, Martini E, Herman S, Bloem MW, Yip R: Estimating the prevalence of anaemia: a comparison of three methods. Bull World Health Org. 2001, 79: 506-511.
Boulton F, Nightingale M, Reynolds W: Improved strategy for screening prospective blood donors for anaemia. Transfusion Med. 1994, 4: 221-225. 10.1111/j.1365-3148.1994.tb00275.x.
James V, Jones K, Turner E, Sokol R: Statistical analysis of inappropriate results from current Hb screening methods for blood donors. Transfusion. 2003, 43: 400-404. 10.1046/j.1537-2995.2003.00316.x.
Bridges N, Parvin RM, Van Assendelft OW: Evaluation of a new system for hemoglobin measurement. Am Clin Products Rev. 1987, 6 (4): 22-25.
HemoCue Blood Hemoglobin Photometer Operating Manual. [http://www.hemocue.com/files/900138_GB.pdf]
Gamperling N, Mast B, Hagbloom R, Houwen B: Performance Evaluation of the Sysmex KX-21 [TM] Automated Hematology Analyzer. Sysmex J Int. 1998, 8: 96-101.
United Kingdom National External Quality Assessment Scheme for Haematology (UK NEQAS (H)) WGHV, Watford, WD1 8FJ, UK: An evaluation of the Sysmex KX-21 automated haematology analyser. Sysmex J Int. 1998, 8: 102-109.
Sysmex KX-21N Operator's Manual. Sysmex Corporation. 2006
Bhaskaram P, Balakrishna N, Radhakrishna KV, Krishnaswamy K: Validation of hemoglobin estimation using Hemocue. Indian J Pediatr. 2003, 70 (1): 25-28. 10.1007/BF02722739.
Bland JM, Altman DG: Statistical methods for assessing agreement between two methods of clinical measurement. Lancet i. 1986, 1: 307-310.
Lardi AM, Hirst C, Mortimer AJ, McCollum CN: Evaluation of the HemoCue® for measuring intra operative haemoglobin concentrations: a comparison with the Coulter Max M® . Anaesthesia. 1998, 53 (4): 349-352. 10.1046/j.1365-2044.1998.00328.x.
Von Schenck H, Falkensson M, Lundberg B: Evaluation of" HemoCue," a new device for determining hemoglobin. Clin Chem. 1986, 32 (3): 526-529.
Van de Louw A, Lasserre N, Drouhin F, Thierry S, Lecuyer L, Caen D, Tenaillon A: Reliability of HemoCue in patients with gastrointestinal bleeding. Intens Care Med. 2007, 33 (2): 355-358. 10.1007/s00134-006-0461-6.
Rippmann CE, Nett PC, Popovic D, Seifert B, Pasch T, Spahn DR: HemoCue®, an Accurate Bedside Method of Hemoglobin Measurement?. J Clin Monit Comput. 1997, 13 (6): 373-377.
Neville RG: Evaluation of portable haemoglobinometer in general practice. BMJ (Clinical research ed). 1987, 294 (6582): 1263-1265. 10.1136/bmj.294.6582.1263.
Rechner IJ, Twigg A, Davies AF, Imong S: Evaluation of the HemoCue compared with the Coulter STKS for measurement of neonatal haemoglobin. Arch Dis Child Fetal Neonatal. 2002, 86 (3): F188-F189. 10.1136/fn.86.3.F188.
Radtke H, Polat G, Kalus U, Salama A, Kiesewetter H: Hemoglobin screening in prospective blood donors: comparison of different blood samples and different quantitative methods. Transfus Aph Sci. 2005, 33 (1): 31-35. 10.1016/j.transci.2004.11.004.
Zhou X, Yan H, Xing Y, Dang S, Zhuoma B, Wang D: Evaluation of a portable hemoglobin photometer in pregnant women in a high altitude area: a pilot study. BMC Public Health. 2009, 9 (1): 228-10.1186/1471-2458-9-228.
Van Kampen EJ, Assendelft DW: Quality Control in Clinical Chemistry. Quality control and hematology. Edited by: Anido G, Kampen Ev, Rosalki S, Rubin M. 1975, Berlin-New York: de Gruyter, 325-333.
Creer MH, Ladenson J: Analytical errors due to lipemia. Lab Med. 1983, 14: 351-355.
Sharma A, Artiss J, Strandbergh D, Zak B: The turbid specimen as an analytical medium: hemoglobin determination as a model. Clin Chim Acta. 1985, 147: 7-14. 10.1016/0009-8981(85)90004-X.
Waldenström JG, Raiend U: Plasmapheresis and cold sensitivity of immunoglobulin molecules. Acta Med Scand. 1984, 216: 449-466.
Sawant RB, Bharucha ZS, Rajadhyaksha SB: Evaluation of hemoglobin of blood donors deferred by the copper sulphate method for hemoglobin estimation. Transfus Apher Sci. 2007, 36 (2): 143-148. 10.1016/j.transci.2006.11.001.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6890/11/5/prepub
Acknowledgements
We sincerely thank all the study participants for taking part in the study. We are also thankful to the staff of the Agogo Presbyterian Hospital Laboratory for their support during the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Authors' contributions
BN planned, carried out the study and headed the drafting of the manuscript. SBN carried out the statistical interpretation and co-headed the drafting the manuscript. NS organized the day-to-day work as study coordinator. DD organized and contributed to the study. AI carried out the study and contributed in drafting of the manuscript. JM and YAS supervised the study and contributed to drafting the manuscript. All authors have read and approved the final manuscript. Financial support for this study was given by a Swiss Foundation.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Nkrumah, B., Nguah, S.B., Sarpong, N. et al. Hemoglobin estimation by the HemoCue® portable hemoglobin photometer in a resource poor setting. BMC Clin Pathol 11, 5 (2011). https://doi.org/10.1186/1472-6890-11-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6890-11-5