
Abstract
Background
Sonoran ethnic groups (Yaquis, Mayos, Seris, Guarijíos, Pimas, Kikapúes and Pápagos) use mainly herbal based preparations as their first line of medicinal treatment. Among the plants used are those with anti-tuberculosis properties; however, no formal research is available.
Methods
Organic extracts were obtained from nine medicinal plants traditionally used by Sonoran ethnic groups to treat different kinds of diseases; three of them are mainly used to treat tuberculosis. All of the extracts were tested against Mycobacterium tuberculosis H37Rv using the Alamar Blue redox bioassay.
Results
Methanolic extracts from Ambrosia confertiflora, Ambrosia ambrosioides and Guaiacum coulteri showed minimal inhibitory concentration (MIC) values of 200, 790 and 1000 μg/mL, respectively, whereas no effect was observed with the rest of the methanolic extracts at the concentrations tested. Chloroform, dichloromethane, and ethyl acetate extracts from Ambrosia confertiflora showed a MIC of 90, 120 and 160 μg/mL, respectively.
Conclusions
A. confertiflora and A. ambrosioides showed the best anti-mycobacterial activity in vitro. The activity of Guaiacum coulteri is consistent with the traditional use by Sonoran ethnic groups as anti-tuberculosis agent.
For these reasons, it is important to investigate a broader spectrum of medicinal plants in order to find compounds active against Mycobacterium tuberculosis.
Similar content being viewed by others


Background
Tuberculosis (TB) is a chronic infectious disease caused mainly by Mycobacterium tuberculosis[1, 2]. The World Health Organization (WHO) estimated that almost 9 million new cases and 1.4 million TB deaths (990 000 among HIV-negative people and 430 000 HIV-associated TB deaths), occurred in 2011 [3]. Ninety-five percent of TB cases are produced in underdeveloped countries, 80% of them corresponding to the 15 to 29-year-old group, generating strong socioeconomic problems [4]. Furthermore, the lack of treatment adherence has given rise to antibiotic-resistant M. tuberculosis strains. The resistance is classified into two groups: the multidrug-resistant TB (MDR-TB), which does not respond to the first-line standard treatment, and the extensively drug-resistant TB (XDR-TB), which occurs when resistance to second-line drugs develops [5]. According to the new 2012 WHO report on surveillance and response to MDR-TB and XDR-TB, an estimate of 310 000 (range, 232 000–400 000) MDR-TB cases occurred among recorded pulmonary TB patients in 2011, with 84 countries reporting at least one case of XDR-TB [3]. This emphasizes the need to search for new drugs against tuberculosis [6, 7].
According to the National Epidemiological Surveillance (SINAVE), Mexico has shown a reduction in TB incidence and has been considered as a medium security risk region by WHO. Nevertheless, 17 000 new cases and approximately 2000 deaths each year are reported in Mexico [8, 9].
Mexico possesses a great geographic diversity, and also has one of the richest flora on the planet, compared with that in Malaysia and some regions in central and South America [10]. Sonora is located on the northwestern region of Mexico and is the second largest state of the country, characterized by more than 3000 plant species widely known and used by the local ethnic groups: Yaquis, Mayos, Seris, Guarijíos, Pimas, Kikapúes, and Pápagos [11]. These groups use herbal remedies in their traditional medicine for cultural reasons, as well as due to the inaccessibility to medical services and/or their expectative of resolving pathologies considered incurable or inoperable by modern medicine [10, 11]. Since no report exists yet on studies showing the anti-tuberculosis activity of Sonoran plants, the objective of the present research was to evaluate the potential anti-mycobacterial activity of medicinal plants used by the Sonoran ethnic groups for the treatment of tuberculosis and other diseases.
Methods
Plants and extracts preparations
Plants collection
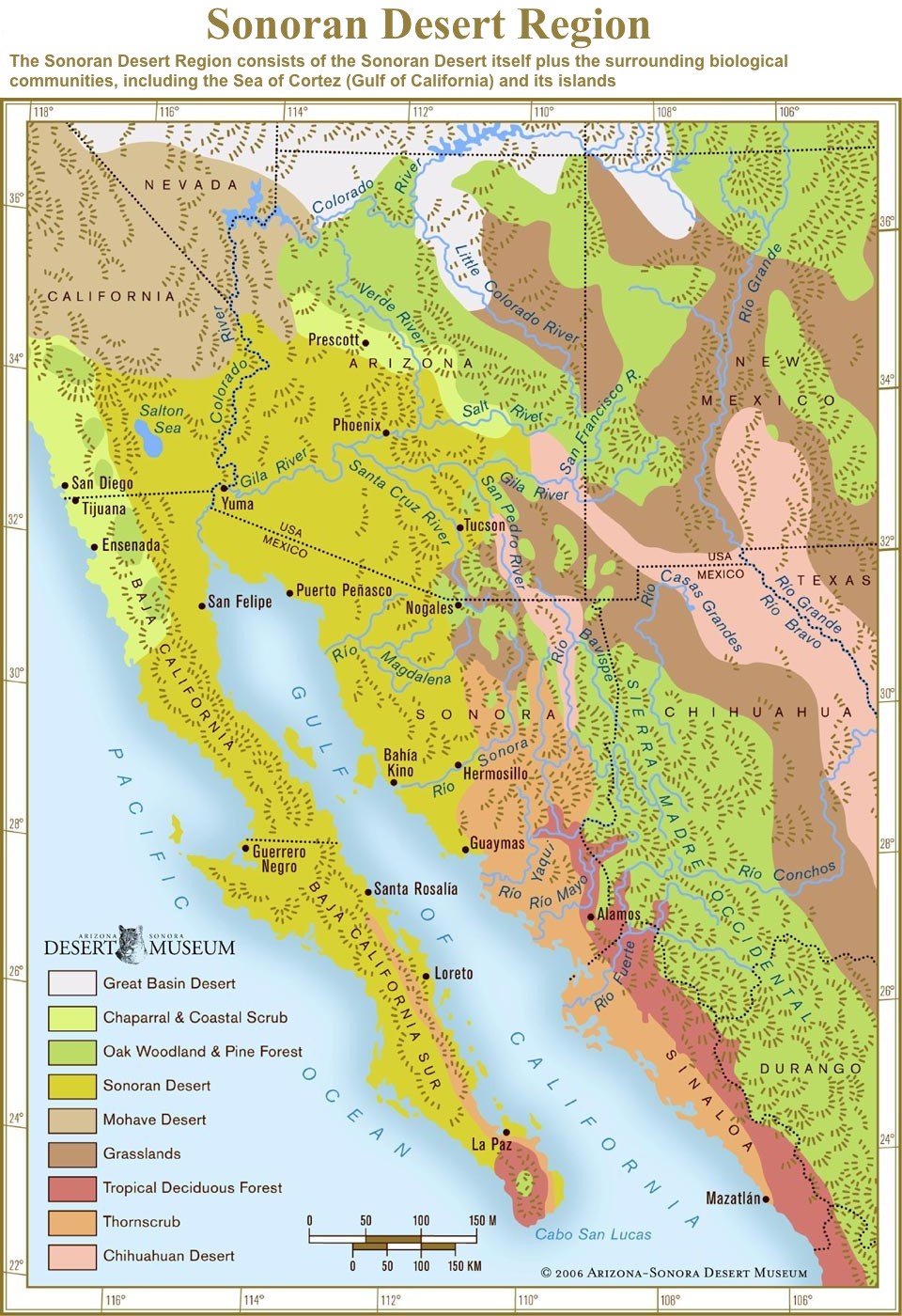
Nine plants were selected based on their traditional use by Sonoran ethnic groups for tuberculosis or symptom-related diseases, such as cough, fever, lack of appetite, and weakness or caquexia (Table 1). Plants were collected from wild environments located in the surrounding area of Hermosillo, Sonora, and Phoradendrom californicum was collected in a zone located 80 km South of Hermosillo; both collecting areas belong to the Sonoran desert ecosystem [12]. The aerial parts, fruits, and/or flowers were obtained and handled separately. The plants were authenticated at the Herbarium of the University of Sonora by Professor Jesús Sánchez-Escalante, where voucher specimens were deposited.
Preparation of methanolic extracts of collected plants
One-hundred grams of dry samples were macerated and kept in 1 L methanol at room temperature for one week, with occasional stirring. Solids were filtered out and the extracts concentrated by evaporation under reduced pressure at 40°C in a Yamato RE300 rotator evaporator [13]. For their use in the susceptibility testing, working solutions of the methanolic extracts were prepared in Middlebrook 7H9 broth containing 20% DMSO, at four times the maximum desired testing concentration. All solutions were sterilized by filtration through a 0.22-μm pore size nitrocellulose membrane (Millipore). Final concentration of DMSO in the assay was ≤5%, which does not produce mycobacterial toxicity (internal control).
Preparation of organic extracts of plants with anti-mycobacterial activity
The plant whose methanolic extract exhibited anti-mycobacterial activity at ≤ 200 μg/mL was further extracted with dichloromethane, chloroform, and ethyl acetate, with a similar protocol to that used for methanolic extract preparation. This extraction was done non-sequentially.
Mycobacterium tuberculosis
Mycobacterium tuberculosis strain H37Rv (sensitive to streptomycin, isoniazide, rifampicin, ethambutol, and pyrazinamide) was provided by the Institute of Epidemiological Diagnosis and Reference of the Mexican Ministry of Health, and was stored and handled at the State of Sonora’s Public Health Laboratory.
Preparation of Mycobacterium tuberculosis inoculum
An initial inoculum was prepared from a solid M. tuberculosis culture, until it reached the log growth phase (approximately 12 days). The bacterium was then transferred to a sterile vial containing five glass pearls (3 mm) and 8 mL of sterile 0.85% saline solution. The bacterial suspension was disaggregated by agitation using a Genie II vortex, and left to stand for 15 min at room temperature. The supernatant was then adjusted, using the 1 McFarland standard, to obtain a bacterial concentration of 3.0 × 108 CFU/mL. The working solution was a 1:25 dilution of this suspension, in Middlebrook 7H9 broth supplemented with 0.2% (v/v) glycerol and 10% (v/v) OADC (oleic acid, albumin, dextrose, and catalase enrichment; Becton Dickinson) for the in vitro anti-mycobacterial activity assay.
In vitro anti-mycobacterial assay
To evaluate the activity of organic extracts, the redox Alamar Blue® (AbD Serotec) microplate assay (MABA) was carried out as described by Franzblau and collaborators [14]. The assay was carried out on 96-well polystyrene flat bottom plates with low evaporation cover lids, in which the M. tuberculosis inoculum was added to supplemented Middlebrook 7H9 broth medium, and mixed with the extracts at different concentrations. In order to prevent excessive evaporation, sterile distilled water was added to the perimetral wells. Rifampicin (Sigma Aldrich) was used as control. Next, 50 μL of fresh Alamar Blue-10% Tween 80 (Sigma Aldrich) mixture (1:1) were added to each well. The microplate was sealed with parafilm and incubated for 48 hours at 37°C. Finally, MIC was calculated and defined as the lowest extract or antibiotic concentration at which no color change of the indicator was evident. Each extract was tested in triplicate.
Screening for sesquiterpene lactones
To search sesquiterpenes lactones in the extracts, the Baljet reaction was used. A 1% picric acid (w/v) solution in ethanol and a 10% sodium hydroxide (w/v) aqueous solution were combined at a 1:1 ratio and added to 2–3 mg of sample. A positive reaction was indicated by an orange to red color change [15, 16].
Results and discussion
Plants used in the present study were selected according to their traditional usage for the treatment of tuberculosis or symptom-related diseases by the Sonoran ethnic groups. Table 1 shows the identification of the studied plants, by scientific and common name, traditional use, parts analyzed, and the ethnic group that uses them as medicinal remedy. The extraction method was chosen based on the consideration that methanolic extracts may contain a wide range of chemical compounds with biological activity such as terpenoids, phenols, flavonoids, saponines, steroids, and others [17–20]. In addition, some studies have reported that methanolic extracts are more active than aqueous extracts in their antibacterial activity [21].
Table 2 shows the MIC values of methanolic extracts of the plants studied. The methanolic extract from Ambrosia confertiflora showed a MIC value of 200 μg/mL against M. tuberculosis H37Rv. Methanolic extracts from Ambrosia ambrosioides and Guaiacum coulteri showed MICs of 790 and 1000 μg/mL, respectively. On the other hand, the extracts from Acalypha californica, Schinus molle, Vallesia glabra, Baccharis glutinosa, Phoradendrom californicum and Acacia farnesiana did not show inhibition even at the highest tested concentration. Guaiacum coulteri, traditionally used against tuberculosis by ethnics groups, resulted less effective in vitro than A. confertiflora (which is not traditionally indicated as anti-TB plant) in the anti-mycobacterial assay. However, as we use only flowers from G. coulteri for the anti-mycobacterial assay, it is important to evaluate other parts of this plant to assess this activity.
Ambrosia confertiflora is used by Sonoran ethnic groups to treat diseases with symptoms closely related to tuberculosis, such as fever and lack of appetite (Table 1), and furthermore, the family to which it belongs (Asteraceae) contains species with a high concentration of sesquiterpene lactones (SQL) identified for their wide variety of biological activities, including their anti-mycobacterial effect [22, 23]. Species of the genus Ambrosia have been previously reported for their anti-tuberculosis activity, associated to SQL [24]. It is likely that the anti-tuberculosis activity observed in A. confertiflora and A. ambrosioides is associated with the presence of such molecules.
Acacia farnesiana, G. coulteri, and S. molle have been referred by Sonoran traditional medicine as anti-tubercular agents, but only G. coulteri resulted active under the conditions tested. In this study we used leaves and fruits of A. farnesiana and S. molle to evaluate the anti-mycobaterial activity which could explain our results, especially in the case of A. farnesiana from which several products (gum, flower, seed, leaves, cortex, root) are used by ethnias as anti-tubercular medicine.
With the exception of Schinus molle, none of the plants studied had been evaluated before in Mexico for their anti-tuberculosis properties [25]. Molina-Salinas et al. [25] reported a MIC of 125 μg/mL for the hexane extract of S. molle; however, for the methanolic extract evaluated in the present study, no activity was detected even at the highest concentration tested (1000 μg/mL). The differences between the results obtained by Molina-Salinas et al. [25] and ours are attributed to the presence of mainly non-polar compounds in the hexane extract, in contrast with the methanolic extract where high polarity compounds are present.
Diverse methods and procedures to assess anti-mycobacterial agents are currently used, resulting in a diversity of cut-off values to define a MIC value as active: MIC ≤100 μg/mL, ≤125 μg/mL, ≤ 200 μg/mL [6, 25–27]. For this reason, no international standard has yet been established to adequately define the level of anti-mycobacterial activity. For the present study we defined as active the extract with a MIC value of ≤ 200 μg/mL, considering the presence of the active component (s) at adequate concentration for their further isolation and purification, such was the case of Ambrosia confertiflora methanolic extract.
References to medicinal plants used by ethnic groups are mainly considered as a relevant guideline in the research of natural products; however, in many cases it is possible to validate the biological activity referred, but in others it is not possible to confirm scientifically their medicinal properties.
The difference in the anti-mycobacterial activity of A. confertiflora, A. ambrosioides and G. coulteri may be attributed to the difference in the relative concentration of the active compound in these plants. However, further research is required to demonstrate this statement.
Several reports correlate the high content of terpenoid compounds and different biological activities for the genus Ambrosia, such as anti-fungal, anti-trypanosomic, and anti-leishmania, as well as an anti-malaria effect [28–31].
From A. confertiflora, SQLs could be responsible for the anti-mycobacterial effect observed in the present study [32, 33]. Cantrell et al. [23], in their review, reported plant-derived terpenoids and some synthetic analogs with variable anti-tubercular activity by the BACTEC 460 system. Particularly, over 50 sesquiterpene are reported [23] in that evaluation, where the most active compounds from A. confertiflora were santamarine and reynosin with a MIC value of 64 μg/mL. The MIC values obtained in our study are higher in comparison with those previously reported for reynosin and santamarine, since these are pure compounds, whereas ours were crude extracts.
Based on the latter and considering that the SQLs isolated by Yoshioka and collaborators are from a chloroform extract [32], we included less polar crude extracts such as chloroform, dichloromethane, and ethyl acetate from A. confertiflora and evaluated the effect on the growth of M. tuberculosis H37Rv. The results evidenced an increase in the activity of these extracts in comparison to the methanolic extract; but the main activity was obtained with chloroform with a MIC value of 90 μg/mL. On the other hand, the dichloromethane and ethyl acetate extracts showed MIC values of 120 and 160 μg/mL, respectively (Table 3). Highly polar molecules exhibit a reduced transport through the outer lipid layer of mycobacteria and, in consequence, lower anti-mycobacterial activity, whereas less polar molecules exhibit higher permeability [34, 35]. These reports are in agreement with our results, where the extracts obtained with less polar solvents showed better activity than those exhibited by the methanolic extracts.
Our findings reveal that the extraction method with intermediate-polarity solvents (e.g. dichloromethane) favors the possibility to obtain active compounds against M. tuberculosis, since it would be quite difficult to obtain them from aqueous extracts (high-polarity) as reported by Camacho-Corona and collaborators [27]; hence, the active compounds against this pathogen must be either less polar or even non-polar [25]. For this reason, the aqueous extraction method would not be the ideal method to obtain anti-mycobacterial compounds.
Based on studies reporting that both A. confertiflora and A. ambrosioides are rich in SQLs [22, 23], we chose to perform a qualitative Baljet reaction to establish the possible presence of these molecules, resulting positive for all the different extracts (chloroform, dichloromethane, ethyl acetate and methanol) of A. confertiflora (Table 3) and the methanolic extract from A. ambrosioides. Although this reaction is also positive for cardiac glycosides and others containing α, β-unsaturated lactones, anti-mycobacterial activity has been attributed to this kind of molecules. Further studies are being performed on A. confertiflora to isolate the active compounds.
Conclusions
Ambrosia confertiflora and A. ambrosioides were included in this study, despite not being used for the treatment of tuberculosis by local ethnic groups, and showed the best anti-mycobacterial in vitro activity.
The anti-mycobacterial activity of Guaiacum coulteri is consistent with the traditional use by Sonoran ethnic groups as anti-tuberculosis agent.
However, in the case of Schinus molle and Acacia farnesiana which are used against tuberculosis by these groups, no anti-mycobacterial activity was found, since only leaves and fruits were evaluated, but not gum, flower, seed, cortex or root as used by ethnias especially in the case of A. farnesiana.
For these reasons it is important to investigate a broader spectrum of medicinal plants in order to find compounds active against Mycobacterium tuberculosis.
References
Jordao L, Vieira OV: Tuberculosis: new aspects of an old disease. Int J Cell Biol. 2011, 2011: 1-13.
Thaiss WM, Thaiss CC, Thaiss CA: Recent developments in the epidemiology and management of tuberculosis –new solutions to old problems?. Infect Drug Resist. 2012, 5: 1-8.
World Health Organization: Global tuberculosis report. 2012,http://apps.who.int/iris/bitstream/10665/75938/1/9789241564502_eng.pdf,
World Health Organization: Global tuberculosis control: WHO Report. 2010,http://reliefweb.int/sites/reliefweb.int/files/resources/F530290AD0279399C12577D8003E9D65-Full_Report.pdf,
Zager EM, McNerney R: Multidrug-resistant tuberculosis. BMC Infect Dis. 2008, 8: 10-10.1186/1471-2334-8-10.
Jiménez A, Meckes M, Ramírez R, Torres J, Luna J: Activity against multidrug-resistant Mycobacterium tuberculosis in Mexican plants used to treat respiratory diseases. Phytother Res. 2003, 17: 903-908. 10.1002/ptr.1377.
Speck A, Scotti MT, de Paulo V: Current pharmaceutical design of Antituberculosis drugs: future perspectives. Curr Pharm Des. 2010, 16: 2656-2665. 10.2174/138161210792389289.
Bermejo MC, Clavera I, Michel RFJ, Marín B: Epidemiology of tuberculosis. An Sist Sanit Navar. 2007, 30: 7-19.
Lauzardo M, Peloquin CA: Antituberculosis therapy for 2012 and beyond. Expert Opin Pharmacother. 2012, 13: 511-526. 10.1517/14656566.2012.657176.
Johnson J, Moreno SF, López R: Compendio fitoquímico de la medicina tradicional herbolaria de Sonora. 1996, Sonora: Universidad de Sonora
López R, Hinojosa A: Catálogo de plantas medicinales sonorenses. 1988, Sonora: Universidad de Sonora
Arizona-Sonora Desert Museum.http://www.desertmuseum.org/images/csds/sonoran_map-lg.jpg,
Robles RE, Velázquez CA, Garibay A, Gálvez JC, Ruíz E: Antimicrobial activity of north-western Mexican plants against helicobacter pylori. J Med Food. 2011, 14: 1280-1283. 10.1089/jmf.2010.0263.
Franzblau SG, Witzig RS, McLaughlin JC, Torres P, Madico G, Hernández A, Degnan MT, Cook MB, Quenzer VK, Ferguson RM, Gilman RH: Rapid, low-technology MIC determination with clinical Mycobacterium tuberculosis isolates by using the microplate Alamar Blue assay. J Clin Microbiol. 1998, 36: 362-366.
Silva GL, Lee IS, Kinghorn AD: Special problems with the extraction of plants. Natural Products Isolation. Methods in Biotechnology. Volume 4. Edited by: Canell JPR. 1998, New Jersey: Humana Press, 343-363. 1
Schneider G, Lachner I: Beitrag zur Analytik und Wirkung von Cnicin [abstract]. Planta Med. 1987, 53: 247-251. 10.1055/s-2006-962693.
Tiwari N, Thakur J, Saikia D, Gupta MM: Antitubercular diterpenoids from Vitex trifolia. Phytomedicine. 2013, 20: 605-610. 10.1016/j.phymed.2013.01.003.
Madaan R, Bansal G, Kumar S, Sharma A: Estimation of total phenols and flavonoids in extracts of Actaea spicata roots and antioxidant activity studies. Indian J Pharm Sci. 2011, 73: 666-669. 10.4103/0250-474X.100242.
Khatuntseva EA, Men’shov VM, Shashkov AS, Tsvetkov YE, Stepanenko RN, Vlasenko RY, Shults EE, Tolstikov GA, Tolstikova TG, Baev DS, Kaledin VA, Popova NA, Nikolin VP, Laktionov PP, Cherepanova AV, Kulakovskaya TV, Kulakovskaya EV, Nifantiev NE: Triterpenoid saponins from the roots of Acanthophyllum gypsophiloides Regel. Beilstein J Org Chem. 2012, 8: 763-775.
Viswanathan MBG, Ananthi JDJ, Kumar PS: Antimicrobial activity of bioactive compounds and leaf extracts in Jatropha tanjorensis. Fitoterapia. 2012, 83: 1153-1159. 10.1016/j.fitote.2012.07.007.
Parekh J, Jadeja D, Chanda S: Efficacy of aqueous and methanol extracts of some medicinal plants for potential antibacterial activity. Turk J Biol. 2005, 29: 203-210.
Seaman FC: Sesquiterpene lactones as taxonomic characters in the Asteraceae. Bot Rev. 1982, 48: 121-595. 10.1007/BF02919190.
Cantrell CL, Franzblau SG, Fischer NH: Antimycobacterial plant terpenoids. Planta Med. 2001, 67: 685-694. 10.1055/s-2001-18365.
Aponte JC, Yang H, Vaisberg AJ, Castillo D, Málaga E, Verástegui M, Casson LK, Stivers N, Bates PJ, Rojas R, Fernández I, Lewis WH, Sarasara C, Sauvain M, Gilman RH, Hammond GB: Cytotoxic and anti-infective sesquiterpenes present in Plagiochila disticha (Plagiochilaceae) and Ambrosia peruviana (Asteraceae). Planta Med. 2010, 76: 705-707. 10.1055/s-0029-1240681.
Molina GM, Pérez A, Becerril P, Salazar R, Said S, Waksman N: Evaluation of the flora of Northern Mexico for in vitro antimicrobial and antituberculosis activity. J Ethnopharmacol. 2007, 109: 435-441. 10.1016/j.jep.2006.08.014.
Molina GM, Ramos MC, Vargas J, Mata BD, Becerril P, Said S: Bactericidal activity of organic extracts from Flourensia cernua DC against strains of Mycobacterium tuberculosis. Arch Med Res. 2006, 37: 45-49. 10.1016/j.arcmed.2005.04.010.
Camacho MR, Ramírez MA, González O, Garza E, Palacios IP, Luna J: Activity against drug resistant-tuberculosis strains of plants used in Mexican traditional medicine to treat tuberculosis and other respiratory diseases. Phytother Res. 2008, 22: 82-85. 10.1002/ptr.2269.
Tequida M, Cortez M, Rosas EC, López S, Corrales C: Effect of alcoholic extracts of wild plants on the inhibition of growth of Aspergillus flavus, Aspergillus niger, Penicillium chrysogenum, Penicillium expansum, Fusarium moniliforme and Fusarium poae moulds. Rev Iberoam Micol. 2002, 19: 84-88.
Sülsen VP, Frank FM, Cazorla SI, Anesini CA, Malchiodi EL, Freixa B, Vila R, Muschietti LV, Martino VS: Trypanocidal and leishmanicidal activities of sesquiterpene lactones from Ambrosia tenuifolia Sprengel (Asteraceae). Antimicrob Agents Chemother. 2008, 52: 2415-2419. 10.1128/AAC.01630-07.
Klayman DL: Qinghaosu (Artemisinin) – An antimalarial drug from China. Science. 1985, 228: 1049-1055. 10.1126/science.3887571.
Cumming JN, Ploypradith P, Posner GH: Antimalarial activity of artemisinin (Qinghaosu) and related trioxanes: mechanism(s) of action. Adv Pharmacol. 1997, 37: 253-297.
Yoshioka H, Renold W, Fischer NH, Higo A, Mabry TJ: Sesquiterpene lactones from Ambrosia confertiflora (Compositae). Phytochemistry. 1970, 9: 823-832. 10.1016/S0031-9422(00)85188-2.
Renold W, Yoshioka H, Mabry TJ: Chihuahuin, a new germacranolide from Ambrosia confertiflora DC (Compositae). J Org Chem. 1970, 35: 4264-4266. 10.1021/jo00837a640.
Korycka M, Rumijowska A, Dziadek J: The effect of ethambutol on mycobacterial cell wall permeability to hydrophobic compounds. Pol J Microbiol. 2005, 54: 5-11.
Luna J, Costa MC, González HG, Rodrigues AI, Castilho PC: Synergistic antimycobacterial activities of sesquiterpene lactones from Laurus spp. J Antimicrob Chemother. 2007, 59: 548-552. 10.1093/jac/dkl523.
{kind=link}
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6882/13/329/prepub
Acknowledgments
The authors wish to thank the Public Health Laboratory of the state of Sonora for allowing us to work in their BSL-3 laboratory and for all the facilities provided. We thank Professor Jesús Sánchez-Escalante from the Herbarium of the University of Sonora for his support on the authentication of the plants studied in the present work. The present work was supported by the Mexican Council of Science and Technology (CONACyT), Grant numbers 83224 and 83462.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing interests.
Author’s contributions
AGE, RERZ, EWCA, CAVC conceived the study, analyzed data, and drafted the manuscript. EWCA, MNN, ERB were involved in generation of organic extracts. EWCA carried out the biological assay. All authors have read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Robles-Zepeda, R.E., Coronado-Aceves, E.W., Velázquez-Contreras, C.A. et al. In vitro anti-mycobacterial activity of nine medicinal plants used by ethnic groups in Sonora, Mexico. BMC Complement Altern Med 13, 329 (2013). https://doi.org/10.1186/1472-6882-13-329
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6882-13-329