
Abstract
Background
Women in deprived socioeconomic situations run a high pain risk. Although number of pain sites (NPS) is considered highly relevant in pain assessment, little is known regarding the relationship between socioeconomic conditions and NPS.
Methods
The study population comprised 653 women; 160 recurrence-free long-term gynecological cancer survivors, and 493 women selected at random from the general population. Demographic characteristics and co-morbidity over the past 12 months were assessed. Socioeconomic conditions were measured by Socioeconomic Condition Index (SCI), comprising education, employment status, income, ability to pay bills, self-perceived health, and satisfaction with number of close friends. Main outcome measure NPS was recorded using a body outline diagram indicating where the respondents had experienced pain during the past week. Chi-square test and forward stepwise logistic regression were applied.
Results and Conclusion
There were only minor differences in SCI scores between women with 0, 1-2 or 3 NPS. Four or more NPS was associated with younger age, higher BMI and low SCI. After adjustment for age, BMI and co-morbidity, we found a strong association between low SCI scores and four or more NPS, indicating that there is a threshold in the NPS count for when socioeconomic determinants are associated to NPS in women.
Similar content being viewed by others


Background
Living in deprived socioeconomic conditions is associated with higher prevalence of health complaints [1, 2], like generalized [3], musculoskeletal [4], chronic non-malignant [5] and complex/frequent/intensive pain [6]. The most frequent measures of self-reported pain are frequency, severity, and specific pain locations. During the recent years number of pain sites (NPS) is regarded as a better parameter in pain assessment [7] and may be more important than actual sites in determining the impact on health [8] and functioning [9]. Females endorse a larger NPS than males [7, 10–12], and high NPS is frequently reported around middle age [7, 12, 13]. Increasing NPS is related to impaired health status [10, 12], and poorer general [9, 14], as well as physical, psychological and social functioning outcomes [15]. However, little is known regarding the association between socioeconomic conditions and NPS. The aim of this study was to explore the relationship between socioeconomic conditions and NPS in women.
Materials and methods
Study population
The study population comprised recurrence-free long-term gynecological cancer survivors and women from the general population. From 1987 through 1996, 1171 primary patients of cervical, corpus and ovarian cancer were treated at St. Olav's Hospital, Trondheim, which represent all gynecological cancer patients from the middle part of Norway. In May 2003 we examined survival and recurrence status. Women aged 30-75 years and without recurrence of disease, were eligible for participation in this cross-sectional study - in total 369 cases. For each survivor we selected four age-matched women as controls, living in the same county, at random from the population census. We failed to reach 50 cases due to invalid mailing addresses. Thus, the final sample comprised 319 gynecological cancer survivors and 1276 women from the general population. After one reminder, 176 survivors (55%) and 521 controls (41%) responded. Some had incomplete responses to most questions and were excluded. In total, 653 responses were included in the analyses; 160 women with and 493 without a history of gynecological cancer. Mean age was 58 and 57, respectively. The mean follow-up time after cancer treatment was 12 years (SD 2.6; range 8-17). More detailed information on the study population is provided elsewhere [16–18].
Socioeconomic condition
The Socioeconomic Condition Index (SCI) [17] is a modification of the Living Condition Index [19], based on the scores on education, employment, income, ability to pay bills, self- perceived health, and satisfaction with the number of close friends. Education: < 10 years = 0;
10-12 years = 2; 13-15 years = 3; > 15 years = 4. Employment status: unemployed = 0; part- time job = 2; full-time job = 4. The unemployed group included homemakers, students, retired, and women with a disability pension. Annual household income: < 12.500 € = 0;
12.500 - 37.500 € = 2; 37.501-62.500 € = 3; > 62.500 € = 4. Ability to pay bills: never problems = 2; problems = 0. Self-perceived health: very poor = 0; poor = 1; moderate = 2; good = 3; very good = 4. Satisfaction with number of close friends: satisfied with number of close friends = 2; not satisfied with number of close friends = 0.
The summary scores of the SCI range from 0 to 20 and were categorized into quartiles; poor (score ≤ 24 percentile), average to poor (score 25-49 percentile), average to good (score 50-74 percentile), and good (score ≥ 75 percentile) SCI.
Number of pain sites
A body outline diagram was divided into 30 different areas; 15 on each side of the body, enabling the respondents to locate pain that they had experienced during the past week. As most studies apply an upper limit of 7-10 NPS [8–12, 15, 20, 21], we localized pain to eight body regions: head; neck; chest/stomach; lower abdomen/pelvis/hips; back/buttock; thigh/knees; legs/feet; arms/hands. The marked regions of pain were summarized into NPS (range 0-8).
Variable specification
The questionnaire also contained questions on potential confounding variables, such as age, marital status (single, married/co-habitant), weight and height (calculation of body mass index, BMI; kg/m2), smoking (yes, previous, never), and co-morbidity. Co-morbidity was measured as diseases/conditions over the past 12 months prior study, with yes/no responses. All questions were assessed by the respondent herself.
Statistical analyses
All questionnaires were scanned. Consistency analyses were run and corrected for appropriate variables. All analyses were carried out with SPSS version 17.0, applying Chi-square test and forward stepwise logistic regression to examine determinants associated to NPS. Outcome measures were adjusted odds ratios (aOR) with 95% confidence interval (CI). We have used p ≤ 0.05 as level of statistical significance. All reported p-values are two-sided.
Ethics
The study was approved by the Regional Committee for Medical Research Ethics, Mid- Norway, the Norwegian Data Inspectorate, and The National Department of Health and Social Affairs, Norway. All respondents gave informed written consent.
Results
There were only minor differences in the prevalence of women reporting 0, 1, 2, 3, and 4 or more pain sites (20.2%, 21.1%, 20.2%, 15.8%, and 22.7%, respectively). Pain in the neck was most prevalent (49.9%) followed by pain in the back/buttock (45.2%), lower abdomen/pelvis/hips (35.4%), and thighs/knees (33.8%) (Table 1).
For the remaining analyses, we categorized NPS as 0, 1-2, 3, and 4-7 pain sites. As displayed in Table 2 age, smoking, and satisfaction with number of close friends were equally distributed among the NPS groups. More women reporting 3 NPS had high BMI. However, in all major factors the differences in the distribution within the NPS groups were found between women reporting 4-7 NPS and those reporting 3 or less NPS. Women with 4-7 NPS were more often single, had lower education, were more often unemployed, had lower income, more problems paying their bills, and poorer general health (Table 2). The SCI summarizes the differences in education, employment status, income, ability to pay bills, self-perceived health, and satisfaction with number of close friends. In total, women with the lowest SCI had the highest NPS (p < 0.001).
The SCI quartiles [poor (score ≤ 24 percentile), average to poor (score 25-49 percentile), average to good (score 50-74 percentile), good (score ≥ 75 percentile)] were evenly distributed by BMI and by co-morbidities such as pulmonary, gastrointestinal, kidney/urinary, skin disorders and migraine/headache. Poor/average to poor SCI-score was more frequent in high age, among singles and smokers, as well as among women who had survived gynecological cancer, had cardiovascular disease, hypertension, diabetes, and musculoskeletal, psychiatric and sleeping disorder (Table 3).
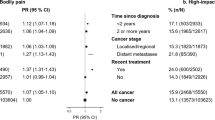
Variables such as SCI (Table 2) and co-factors (Table 3) that were predictors (p < 0.10) of NPS in univariate analyses entered forward stepwise logistic regression analyses. Three models were tested: model A (1-2/0 NPS), model B (3/0 NPS), and model C (4-7/0 NPS), with the no-pain-sites group as reference. In all models we adjusted for co-morbidity. Being a gynecological cancer survivor was not associated with NPS in any model. A significant association was found for increasing BMI and NPS in all three models, with no difference between obese and overweight women. Age below 60 years was associated to 3 or more NPS (models B and C) with no difference between the age-groups 30-49 and 50-59 years. A significant association by decreasing SCI and 4-7 NPS was found in model C, but not in model A or B. Although aOR in the lowest SCI quartiles was 4.2 (95% CI: 1.3-13.5) for the 3/0 NPS group (model B), the strongest association between SCI and NPS was found for the lowest quartile of SCI in model C (aOR 16.9; 95% CI: 4.6-61.7) (Table 4). There was no effect modification between any of the significant variables and co-morbidity in any model.
Discussion
Major differences in the socioeconomic conditions, measured by SCI, were found between women reporting 4 or more NPS and those reporting 3 or less NPS. The socioeconomic conditions are fairly equal for women reporting 0, 1-2 or 3 NPS (Table 2), with employment status corresponding to women in the general Norwegian population [22]. More women with
4-7 NPS, on the other hand, live under the poorest socioeconomic conditions (Table 2). We did not find a clear socioeconomic gradient in NPS, but a threshold when socioeconomic determinants are associated to NPS. After adjustment for co-factors (Table 3) the strongest association between SCI and NPS was found for women with the lowest SCI scores (Table 4). The association in the other groups is rather modest.
The relationship between low socioeconomic conditions and high NPS could be explained by determinants of social position. Although this relationship has been found for some marginalized groups, there is limited scientific evidence for such associations [23]. On the contrary, components of social position, like material circumstances, lifestyle, and psychosocial factors, have been found to increasingly determine health outcomes. The psychosocial perspective proposes that impaired health is a consequence of long-term stress. Lack of control [24] and relative deprivation [25] may represent the key elements of this association, as both phenomena are related to the lower levels of the social hierarchy in modern societies. Adverse psychosocial environment and low job control [1] as well as experiences of being belittled, lack of social support, and economic hardship [26] is associated with poor self-rated health. Women in deprived socioeconomic positions may experience constant stress due to such unfavorable factors, affecting an imbalance in their hormonal and immune systems [27], leading to pain conditions. Within this context we explain the significant association between low socioeconomic conditions and NPS.
Although a relationship between living in socioeconomic deprived areas and widespread pain has been demonstrated earlier [4], the present study reveals that there is a strong relationship between low socioeconomic status and high NPS. In most studies examining NPS, NPS is treated as a co-factor, with chronic pain [8, 11] or disability [21] as outcome variables. In only one study was NPS treated as the dependent variable [12], indicating an association between three components of socioeconomic condition (education, marital and employment status) and NPS in both sexes. However, in that particular study adjustment for co-morbidity was not performed. After adjustment for co-morbidity, we found a strong association between poor
SCI (lowest quartile) and 4 or more NPS, indicating that there is a threshold for most determinants on NPS. In a wealthy country as Norway, women with an average socioeconomic position (≥ 25 and < 75 percentile of SCI) hardly report any higher NPS than women in the best socioeconomic position (≥ 75 percentile of SCI).
Unfortunately, disadvantaged and less assertive women may lack sufficient resources to perform as a credible patient within a normative, biomedical frame of reference. According to Werner and Malterud [28], Norwegian women with chronic pain exert themselves extensively in order to appear as what they hope is "just right" during medical encounters, i.e. substantial effort from the patient's side is required to get access to health care benefits. Health care professionals should be extra attentive to subtle and unarticulated ill-health symptoms of women living in the lowest socioeconomic position to try and reduce the persistent social inequalities in health outcomes [1, 2].
As reported in other Scandinavian studies [7, 12, 13], we found the highest NPS among women below 60 years of age (Table 4). In accordance with Kamaleri et al. [12], we found a weak association between NPS and overweight, whereas smoking and being a gynecological cancer survivor was not associated with NPS in any model. Traumas as war [20] or frightening accidents [29] have been associated with NPS later in life, but surviving cancer without recurrence seems to be very different from surviving other traumas.
The sample size (N = 653) and the high completeness of reported data, including pain areas on the body chart, are considered strengths of the present study. The prevalence of women reporting no, one, two, three, or 4-7 pain sites (Table 1) is similar to what is reported in another Norwegian study [12], supporting the external validity of the study. We consider the use of SCI as strength of the study, and we avoid the problems of co-linearity in multivariate models applying a single outcome for socioeconomic conditions. One limitation of the present study is the cross-sectional design. We cannot draw strict conclusions on causality as the relationship between socioeconomic conditions and NPS is very complex and interactive. Another limitation is the relatively modest response rate. However, the response-rate among gynecological cancer survivors and their controls selected at random from the general population, 55% and 41%, respectively, is considered high, related to comparable studies [4, 13, 30]. There was no skewed distribution between respondents and non-respondents among survivors and women selected at random from the general population regarding age (quartiles) or marital status (married/single) (data not shown).
Conclusion
After adjustment for age, BMI and co-morbidity, we found a strong association between low SCI score and four or more NPS, indicating that there is a threshold in the NPS count for when socioeconomic determinants are associated to NPS in women.
Funding
The study was funded by a grant from SINTEF Health, Trondheim, Norway, and by a grant from the Sør-Trøndelag University College, Faculty of Nursing, Trondheim, Norway.
Abbreviations
- BMI:
-
Body mass index
- SCI:
-
Socioeconomic condition index
- NPS:
-
Number of pain sites
References
Van Lenthe FJ, Schrijvers CTM, Droomers M, Joung IMA, Louwman MJ, Mackenbach JP: Investigating explanations of socio-economic inequalities in health - The Dutch GLOBE study. Eur J Pub Health. 2004, 14: 63-70. 10.1093/eurpub/14.1.63.
Raphael D: Health Promotion and Quality of Life in Canada. 2010, Canadian Scholars' Press: Essential Readings
White KP, Harth M: The occurrence and impact of generalized pain [Review]. Best Pract Res Clin Rheumatol. 1999, 13: 379-389. 10.1053/berh.1999.0027.
Brekke M, Hjortdahl P, Kvien TK: Severity of musculoskeletal pain: relations to socioeconomic inequality. Soc Sci Med. 2002, 54: 221-228. 10.1016/S0277-9536(01)00018-1.
Eriksen J, Jensen MK, Sjogren P, Ekholm O, Rasmussen NK: Epidemiology of chronic non-malignant pain in Denmark. Pain. 2003, 106: 221-228. 10.1016/S0304-3959(03)00225-2.
Jablonska B, Soares JJF, Orjan S: Pain among women: associations with socio- economic and work conditions. Eur J Pain. 2006, 10: 435-447. 10.1016/j.ejpain.2005.06.003.
Ektor-Andersen J, Isacsson SO, Lindgren A, Orbaek P: The experience of pain from the shoulder-neck area related to the total body pain, self-experienced health and mental distress. The Malmo Shoulder-Neck Study group. Pain. 1999, 82: 289-295. 10.1016/S0304-3959(99)00053-6.
Smith BH, Elliott AM, Hannaford PC: Is chronic pain a distinct diagnosis in primary care? Evidence arising from the Royal College of General Practitioners' Oral Contraception study. Fam Pract. 2004, 21: 66-74. 10.1093/fampra/cmh115.
Saastamoinen P, Leino-Arjas P, Laaksonen M, Martikainen P: Pain and health-related functioning among employees. J Epidemiol Community Health. 2006, 60: 793-798. 10.1136/jech.2005.043976.
Fillingim RB, Edwards RR, Powell T: The relationship of sex and clinical pain to experimental pain responses. Pain. 1999, 83: 419-425. 10.1016/S0304-3959(99)00128-1.
Wijnhoven HA, de Vet HC, Picavet HS: Prevalence of musculoskeletal disorders is systematically higher in women than in men. Clin J Pain. 2006, 22: 717-724. 10.1097/01.ajp.0000210912.95664.53.
Kamaleri Y, Natvig B, Ihlebaek CM, Benth JS, Bruusgaard D: Number of pain sites is associated with demographic, lifestyle, and health-related factors in the general population. Eur J Pain. 2008, 12: 742-748. 10.1016/j.ejpain.2007.11.005.
Rustøen T, Wahl AK, Hanestad BR, Lerdal A, Paul S, Miaskowski C: Age and the experience of chronic pain: differences in health and quality of life among younger, middle-aged, and older adults. Clin J Pain. 2005, 21: 513-523. 10.1097/01.ajp.0000146217.31780.ef.
Baune BT, Caniato RN, Garcia-Alcaraz MA, Berger K: Combined effects of major depression, pain and somatic disorders on general functioning in the general adult population. Pain. 2008, 138: 310-317. 10.1016/j.pain.2008.01.002.
Kamaleri Y, Natvig B, Ihlebaek CM, Bruusgaard D: Localised or widespread musculoskeletal pain: does it matter?. Pain. 2008, 138: 41-46. 10.1016/j.pain.2007.11.002.
Rannestad T, Skjeldestad FE, Platou TF, Hagen B: Quality of life among long-term gynaecological cancer survivors. Scand J Caring Sci. 2008, 22: 472-477. 10.1111/j.1471-6712.2007.00557.x.
Platou TF, Skjeldestad FE, Rannestad T: Socioeconomic conditions among long-term gynaecological cancer survivors - A population-based case-control study. Psycho- Oncology. 2010, 19: 306-312. 10.1002/pon.1575.
Rannestad T, Skjeldestad FE: Pain and quality of life among long-term gynaecological cancer survivors: a population-based case-control study. Acta Obstet Gynecol Scand. 2007, 86: 1510-1516. 10.1080/00016340701743116.
Gudbergsson SB, Fossa SD, Ganz PA, Zebrack BJ, Dahl AA: The associations between living conditions, demography, and the 'impact of cancer' scale in tumor-free cancer survivors: a NOCWO study. Support Care Cancer. 2007, 15: 1309-1318. 10.1007/s00520-007-0251-x.
Yaari A, Eisenberg E, Adler R, Birkhan J: Chronic pain in Holocaust survivors. J Pain Sympt Manage. 1999, 17: 181-187. 10.1016/S0885-3924(98)00122-5.
Turner JA, Franklin G, Fulton-Kehoe D, Sheppard L, Stover B, Wu R, Gluck JV, Wickizer TM: ISSLS Prize Winner: Early predictors of chronic work disability. SPINE. 2008, 33: 2809-2818. 10.1097/BRS.0b013e31817df7a7.
Statistics Norway. 2005, (Assessed April 12, 2008), [http://www.ssb.no]
Elstad JI: Sosioøkonomiske ulikheter i helse - teorier og forklaringer [Socioeconomic inequalities in health - theories and explanations]. 2007, Oslo: Sosial- og helsedirektoratet
Syme SL: To prevent disease - the need for a new approach. Health and social organization. Edited by: Blane D, Brunner E, Wilkinson R. 1996, London and New York: Routledge
Wilkinson R: Unhealthy societies. 1996, London: Routledge
Molarius A, Berglund K, Eriksson C, Lambe M, Norström E, Erikson HG, Feldman I: Socioeconomic conditions, lifestyle factors, and self-rated health among men and women in Sweden. Eur J Publ Health. 2007, 17: 125-133. 10.1093/eurpub/ckl070.
Kristenson M, Eriksen HR, Sluiter JK, Starke D, Ursin H: Psychobiological mechanisms of socioeconomic differences in health. Soc Sci Med. 2004, 58: 1511-1522. 10.1016/S0277-9536(03)00353-8.
Werner A, Malterud K: It is hard work behaving as a credible patient: encounters between women with chronic pain and their doctors. Soc Sci Med. 2003, 57: 1409-1419. 10.1016/S0277-9536(02)00520-8.
Kuch K: Psychological factors and the development of chronic pain. Clin J Pain. 2001, 17: 33-38. 10.1097/00002508-200103000-00006.
Bradley CJ, Bednarek HL: Employment patterns of long-term cancer survivors. Psycho-Oncology. 2002, 11: 188-198. 10.1002/pon.544.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1472-6874/12/7/prepub
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
Non-financial competing interests
Authors' contributions
Toril Rannestad (TR), Finn Egil Skjeldestad (FES). Both authors designed the study, organized the questionnaire. The pilot study was undertaken by TR. Administration of adresses lists, mailing, and reminders were done by a professional market company (Sentio AS, Trondheim, Norway). Consistency analysis of raw data, appropriate corrections, organizing the data file, and analysis were done by FES. Both authors contributed to the interpretation of data and writing of the manuscript. Both authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Rannestad, T., Skjeldestad, F.E. Socioeconomic conditions and number of pain sites in women. BMC Women's Health 12, 7 (2012). https://doi.org/10.1186/1472-6874-12-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6874-12-7