
Abstract
Background
Upon return from space many astronauts experience symptoms of orthostatic intolerance. Research has implicated altered autonomic cardiovascular regulation due to spaceflight with further evidence to suggest that there might be pre-flight autonomic indicators of post-flight orthostatic intolerance. We used heart rate variability (HRV) to determine whether autonomic regulation of the heart in astronauts who did or did not experience post-flight orthostatic intolerance was different pre-flight and/or was differentially affected by short duration (8 – 16 days) spaceflight. HRV data from ten-minute stand tests collected from the 29 astronauts 10 days pre-flight, on landing day and three days post-flight were analysed using coarse graining spectral analysis. From the total power (PTOT), the harmonic component was extracted and divided into high (PHI: >0.15 Hz) and low (PLO: = 0.15 Hz) frequency power regions. Given the distribution of autonomic nervous system activity with frequency at the sinus node, PHI/PTOT was used as an indicator of parasympathetic activity; PLO/PTOT as an indicator of sympathetic activity; and, PLO/PHI as an estimate of sympathovagal balance.
Results
Twenty-one astronauts were classified as finishers, and eight as non-finishers, based on their ability to remain standing for 10 minutes on landing day. Pre-flight, non-finishers had a higher supine PHI/PTOT than finishers. Supine PHI/PTOT was the same pre-flight and on landing day in the finishers; whereas, in the non-finishers it was reduced. The ratio PLO/PHI was lower in non-finishers compared to finishers and was unaffected by spaceflight. Pre-flight, both finishers and non-finishers had similar supine values of PLO/PTOT, which increased from supine to stand. Following spaceflight, only the finishers had an increase in PLO/PTOT from supine to stand.
Conclusions
Both finishers and non-finishers had an increase in sympathetic activity with stand on pre-flight, yet only finishers retained this response on landing day. Non-finishers also had lower sympathovagal balance and higher pre-flight supine parasympathetic activity than finishers. These results suggest pre-flight autonomic status and post-flight impairment in autonomic control of the heart may contribute to orthostatic intolerance. The mechanism by which higher pre-flight parasympathetic activity might contribute to post-flight orthostatic intolerance is not understood and requires further investigation.
Similar content being viewed by others

Background
Upon return from spaceflight many astronauts are unable to tolerate upright posture without experiencing symptoms related to fainting. This high degree of orthostatic intolerance (OI) observed in astronauts after spaceflight indicates probable altered cardiovascular regulation upon return. Early spaceflight data, as well as studies utilizing 6° head-down tilt bed rest (HDBR) to simulate weightlessness, have shown reduced plasma volume and decreased baroreflex response, post-exposure [1–9]. There is evidence of altered autonomic cardiovascular control with a reduction in parasympathetic regulation as well as possible changes in sympathetic cardiovascular regulation following real or simulated spaceflight. However, new evidence indicates that pre-flight physiology may also play an important role [10–12].
Investigations of the cardiovascular differences between astronauts who did, or did not, finish a post-flight stand test have revealed pre-flight differences. Compared to finishers, non-finishers had higher parasympathetic tone [12], lower supine and standing peripheral vascular resistance [11] and systolic blood pressure [10, 11] as well as lower standing diastolic blood pressure [11]. Post-flight, finishers had higher catecholamine levels and vasoconstrictor response to standing compared to non-finishers [10, 11].
Although Fritch-Yelle et al. [11] concluded that post-flight presyncope might be due to centrally mediated hypoadrenergic responsiveness, this has recently been challenged [13]. Based on an investigation into the mechanisms leading to syncope in healthy individuals, Evans et al. [13] suggested that presyncopal astronauts may have had similar or higher rates of norepinephrine release since the accumulation time for norepinephrine was shorter due to termination of the stand test.
It is evidence that the importance of the effect of spaceflight on autonomic responses to post-flight orthostatic stress and the effect pre-flight autonomic status on post-flight OI is not well understood. In the present study, we used HRV analysis to further investigate the relationship between spaceflight and autonomic regulation of the heart on orthostatic intolerance in a group of astronauts for whom measures of catecholamines and total peripheral resistance indicated that post-flight OI was associated with low sympathetic response to standing pre- and post- short duration spaceflights [11].
Due to the nature of the interaction of the parasympathetic and sympathetic nervous systems on the heart, with the parasympathetic decreasing and the sympathetic increasing heart rate, a single measurement of heart rate may be the result of a variety of combinations of parasympathetic and sympathetic activity. On the other hand, heart rate variability (HRV) analyses, in the frequency domain, the dynamic response of the heart rate to these inputs [14]. Two major spectral components have been identified: a low frequency (LF) and a high frequency (HF) component that can be used to provide indicators of sympathetic and parasympathetic modulation of heart rate [14, 15]. Because of this, the use of HRV has proven to be a more powerful tool, than the recording of average heart rate, in the investigation of autonomic control of the heart and is now the most common method used to provide non-invasive indicators of the autonomic nervous system [14]. A number of studies have used spectral analysis of HRV during simulated weightlessness to investigate the effects of spaceflight on autonomic cardiovascular control. A consistent decrease in the parasympathetic nervous system indicator has been observed [16–18], whereas both an increase [17] and no change [16, 18] in the sympathetic nervous system indicator has been reported after head down tilt bed-rest.
The aims of this study were: 1) to assess HRV as an appropriate tool to measure autonomic function pre- and post-spaceflight; 2) to determine whether the effects of spaceflight on the autonomic regulation of the heart were different between astronauts who did or did not experience post-flight OI; and, 3) whether pre-flight HRV was different between astronauts who did or did not experience post-flight OI.
Results
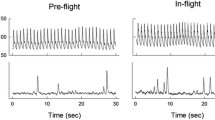
Two of the eight subjects who were unable to complete the 10 minute landing day stand test [11] had insufficient data lengths during the standing portion of the test to perform spectral analysis. Analysis of HRV was therefore limited to six subjects in the stand portion of landing day in the non-finisher group. The RR-interval time series and the corresponding harmonic power spectra for a non-finisher, during the three stand tests, is shown in Figure 1 and that of a finisher in Figure 2. For comparative purposes each of the power spectra were normalized to the total spectral power during the respective pre-flight supine condition.

Data from an astronaut who could not complete the landing day ten-minute stand test (non-finisher). Pre-flight (top figure), landing day (middle figure) and post-flight (bottom figure) RR-interval time series are presented with the onset of standing marked as time 0-minutes. Supine data are on the left (negative times) and stand data on the right (positive times). The gap between -9 and -2 minutes represents the 7-minute carbon-monoxide test for blood volume measurements [11]. Subjects maintained a fixed breathing rate of 15 breaths per minute (0.25 Hz) during the five minutes prior to the carbon monoxide test and during the first five minutes of the stand test. The harmonic spectral power (PHARM) generated from coarse graining spectral analysis of RR-interval in each of the data segments are presented below the supine and above the stand RR-interval data. For comparison over test conditions and with the example finisher astronaut (Figure 2), at each frequency harmonic spectral power was normalized with the pre-flight supine total power (PTOT) and are presented in normalized units (n.u.: PHARM / PTOT).

Data from an astronaut who could complete the landing day ten-minute stand test (finisher). Pre-flight (top figure), landing day (middle figure) and post-flight (bottom figure) RR-interval time series are presented with the onset of standing marked as time 0-minutes. Supine data are on the left (negative times) and stand data on the right (positive times). The gap between -9 and -2 minutes represents the 7-minute carbon-monoxide test for blood volume measurements [11]. Subjects maintained a fixed breathing rate of 15 breaths per minute (0.25 Hz) during the five minutes prior to the carbon monoxide test and during the first five minutes of the stand test. The harmonic spectral power (PHARM) generated from coarse graining spectral analysis of RR-interval in each of the data segments are presented below the supine and above the stand RR-interval data. For comparison over test conditions and with the example non-finisher astronaut (Figure 1), at each frequency harmonic spectral power was normalized with the pre-flight supine total power (PTOT) and are presented in normalized units (n.u.: PHARM / PTOT).
Non-finishers versus finishers
On all test days the ratio PLO/PHI was lower in non-finishers compared to finishers (p = 0.016) and was unaffected by spaceflight (Table 1).
Pre-flight, non-finishers had a higher PHI/PTOT (parasympathetic indicator) than finishers (Figure 4, p < 0.001) and both finishers and non-finishers had similar supine values of PLO/PTOT, which increased from supine to stand (finishers: p < 0.001; non-finishers: p = 0.016, Table 1).
On landing day, compared to pre-flight, only the non-finishers had an overall decrease in PHI/PTOT (Figure 3, p < 0.0001). PHI/PTOT was not different between finishers and non-finishers on landing day (Figure 3, p < 0.0001). Although finishers and non-finishers had similar supine values for PLO/PTOT, only the finishers had an increase in PLO/PTOT from supine to stand on landing day (p < 0.001, Table 1).

The parasympathetic nervous system indicator. The parasympathetic nervous system (PNS) indicator pre-flight, landing day and post-flight with respect to the stand test (3A) and susceptibility to landing day orthostatic intolerance (3B). Symbols denote values different (p < 0.05) from: *, supine or finisher, and #, pre-flight.
Three days after landing, overall PHI/PTOT, was again higher (p = 0.025) in the non-finisher compared to the finisher group (Table 1, Figure 3). Similar to landing day, three days post-flight, only the finishers had an increase in PLO/PTOT from supine to stand (Table 1, p < 0.001).
General effects of spaceflight
When going from supine to standing, RR-interval, PHI, PTOT, and PHI/PTOT decreased and PLO/PHI increased, on all test days (Table 1, all p < 0.015).
Low frequency power, PLO, increased with stand pre-flight but not on landing day or three days post-flight (Table 1). Spaceflight had the effect of reducing mean RR-interval (p < 0.001) on landing day but had recovered to pre-flight values three days after landing (Table 1). Overall, the standing parasympathetic indicator, PHI/PTOT, was also reduced on landing day (p < 0.0001) and three days post-flight (p < 0.01) (Figure 3).
Discussion
We have analysed the data from a group of 29 astronauts who were able to complete a ten minute pre-flight stand tests, eight of which could not complete the same test on landing day [11]. The coarse graining spectral analysis of HRV showed similar differences in sympathetic responses to standing between finishers and non-finishers pre- and post-flight, as was seen with the more elaborate and invasive catecholamine measurements in these same astronauts [11]: PLO/PHI was lower in non-finishers compared to finishers, and, in the non-finishers, PLO/PTOT did not increase with stand post-flight.
We present further evidence that there are specific pre-flight characteristics in autonomic function that distinguish non-finishers from finishers. Both groups had similar reductions in RRI on landing day and due to standing (Table 1), but power spectral analysis of RR-interval during the stand test revealed differences in autonomic function before and after short duration spaceflight, characteristics that may be associated with increased susceptibility to OI following up to 16 days of weightlessness.
There was significantly higher supine parasympathetic activity (PHI/PTOT) in the non-finishers compared to finishers pre-flight; however, this difference disappeared upon standing. Furthermore, the non-finishers also had a decrease in supine PHI/PTOT from pre-flight to landing day three times that of the finishers. Similar results were found between cosmonauts who could or could not finish a 5-minute post-flight stand test following long duration spaceflight (90–198 days) [12]. The mechanism by which higher pre-flight parasympathetic tone might contribute to post-flight OI is not understood [12]. Higher resting parasympathetic control of heart rate is usually associated with reduced sympathetic control. It is possible that parasympathetic activity and its changes to stand and spaceflight is an indicator of a broader difference in autonomic status, both parasympathetic and sympathetic, between non-finishers and finishers.
The indicator associated with the sympathetic nervous system, PLO/PTOT also showed fundamental differences between finishers and non-finishers. However, unlike the parasympathetic indicator these differences were only observed post-flight. Pre-flight, both finishers and non-finishers had similar supine PLO/PTOT, with similar increases in PLO/PTOT from supine to stand (Table 1). With the finishers, the supine and stand values for PLO/PTOT were unchanged from pre-flight to landing day and three days post-flight; however, with the non-finishers, PLO/PTOT did not increase with stand on either landing day or three days post-flight. These data would suggest that cardiac sympathetic activation from supine to stand was impaired post-flight in the non-finishers compared to the finishers and are consistent with a reduced rate of sympathetic response to stand post-flight. This may have contributed to decreased cardiac filling and inadequate stroke volume which ultimately resulted in postural hypotension.
These data support previous reports of landing day hypoadrenergic responsiveness in the non-finishers [11]. However, unlike the previous investigation of this group of astronauts [11] these estimates of autonomic function were performed over the same time period in both finishers and non-finishers and after the first minute of the stand test, not at the end.
Direct measurements of peripheral sympathetic activity during simulated weightlessness through muscle sympathetic nerve activity (MSNA) have produced differing results. In one study with 14 days of HDBR lower MSNA was observed during head-up tilt compared to pre-HDBR [19], while in two others an overall increase in MSNA (supine and orthostatic stress) was observed after three days of dry immersion [20] and after 60 and 120 days of HDBR [21]. Results from MSNA measurements made before and after spaceflight showed an increase in MSNA activation during head-up tilt post-flight compared to pre-flight [22]. Total peripheral resistance and cardiac stroke volume were decreased post-flight whereas heart rate was increased with no change in arterial blood pressure. Unfortunately even though quality signals were collected, none of the six male astronauts tested orthostatically intolerant upon return to Earth and the effects of spaceflight on OI could not be investigated. Our data and those from studies of MSNA show, that in subjects that do not suffer OI, peripheral and cardiac sympathetic activity are sufficient to maintain blood pressure.
In normal subjects, a change from supine to stand causes a shift to greater sympathetic over parasympathetic regulation of cardiac function with a corresponding increase in sypathovagal balance, PLO/PHI. Our data show this change in both groups of astronauts pre-flight, but the non-finishers had lower values than finishers. These were unaffected by spaceflight and suggests that the relationship between sympathetic and parasympathetic modulation of heart rate is preserved in the non-finishers following short duration spaceflight despite the changes observed in parasympathetic and sympathetic activity. In an investigation of HRV in cosmonauts after long duration spaceflight [12], PLO/PHI was found to increase only in the non-finishers both pre-flight and post-flight, however, a low number of finishers during stand in both the pre-flight (n = 5) and post-flight tests (n = 5) may have contributed to the lack of an observed increase in PLO/PHI [12].
Exercise is a physiological perturbation that significantly affects autonomic nervous activity. Research has indicated that long-term endurance training increases heart rate variability, increases parasympathetic activity, and decreases sympathetic activity to the human heart at rest [23–27]. Orthostatic tolerance also appears to be decreased by the improved cardiovascular function associated with physical conditioning [28–31]. As part of the test protocol we did not evaluate individual fitness levels. All astronauts undergo rigorous physical training, including endurance exercise, prior to flight, and variation in pre-flight fitness may have been a contributing factor.
In addition to fitness level, astronaut gender may also play a role in susceptibility to post-flight OI. In this data set, five of eight non-finishers were female, while 19 of 21 finishers were male [11]. A compilation of statistics (25 female, 140 male) on incidence of presyncope after short duration spaceflight (5–16 days) showed a similar effect, with presyncope occurring in 28% of the females and 7% in the males [32] and is associated with low vascular resistance [33] There is growing body of evidence to suggest that autonomic cardiovascular control is different between males and females both at rest [34] and when exposed to orthostatic stress [35–37]. At rest the parasympathetic nervous system is a more dominant influence of heat rate variability in women than in men [34]. Women also respond to cardiovascular stress with greater heart rate increases through parasympathetic withdrawal, whereas men respond primarily with greater increases in vascular resistance through sympathetic control of peripheral vasoconstriction [35–38].
Our data clearly show that the non-finishers have higher parasympathetic activity pre-flight than the finishers and have lower pre-flight PLO/PHI. As well this group also had smaller increases in total peripheral resistance during the pre-flight stand test [11]. It could be argued that these data are representative of female subjects since the majority of the non-finishers were female, yet, others [12] have shown a similar pre-flight relationship between non-finishers and PLO/PHI. Given the distribution of sympathetic versus parasympathetic cardiovascular control between genders we could expect there to be representation of both males and females at either end of the PLO/PHI range. However, as one moves to the extremes at either ends of the range (high sympathetic to parasympathetic or low sympathetic to parasympathetic ratio) a specific gender will dominate. It should not be surprising to find male subjects in the region containing mainly female subjects.
As a group, the non-finishers also had a significant reduction in supine parasympathetic and standing sympathetic activity on landing day such that sympathovagal balance was preserved. This suggests an interaction between sympathetic and parasympathetic control of heart rate during spaceflight to maintain PLO/PHI. Given these changes in autonomic function from pre-flight to landing day the non-finishers, mostly women, who normally respond to cardiovascular stress via greater parasympathetic withdrawal than sympathetic activation, would be compromised and more susceptible to OI.
Regardless of the underlying factors that contribute to the autonomic relationship to post-flight OI, high parasympathetic and low sympathetic activity pre-flight was associated with reduced orthostatic tolerance post-flight. A possible effect of reduced parasympathetic control at rest would be the lack of buffering of blood pressure at the beginning of orthostatic stress, thereby leading to reduced orthostatic tolerance. Fadel et al. [39], further indicate that vagal baroreflex control is pivotal to the reflex regulation of heart rate and maintenance of arterial blood pressure during dynamic and transient decreases in systemic blood pressure. The strength of this relationship is most likely related to the relative strength of the parasympathetic and sympathetic control systems during day-to-day activities. In those subjects with higher parasympathetic compared to sympathetic tone, parasympathetic activity would be expected to play a greater role. The reverse would also be true. During weightlessness the arterial baroreceptor system is rarely challenged due to the lack of postural fluctuations in blood pressure. Upon return to Earth, this results in reduced vagal tone. Unless a significant regulatory mechanism remains to compensate for the sudden drop in blood pressure on standing, the subject will be orthostatically intolerant. Those subjects, in whom sympathetic vascular resistance control was high before spaceflight, would not experience as great an effect during orthostatic stress.
When interpreting HRV, care must be taken to ensure that the data segment was obtained during steady state conditions [14]. In this study, care was taken to ensure that data used for HRV analysis was from segments that were closest to being steady state. The subject was supine for at least ten minutes before the baseline HRV analysis. Baseline analysis was also performed prior to the carbon monoxide (CO) rebreathe test for blood volume. During the stand portion of the test, HRV analysis was not performed until at least one minute had passed, allowing for heart rate and blood pressure to stabilize (Figures 1 &2). This was at three minutes after the CO-rebreathe protocol and at least eight minutes after the inhalation of CO for the blood volume test. Analysis of the RR-interval in the two minutes prior to and immediately following the CO test segment indicated that there was no difference in mean RR-interval or the standard deviation of RR-interval (see sample data, Figures 1 &2) which would suggest that the CO-rebreathe test did not affect the heart rate data.
We chose to use CGSA to investigate HRV due to its unique ability to allow for investigation of fractal variability. However, results from the harmonic component of CGSA are compatible with those from a general spectral analysis fast Fourier transform (FFT) using the Task Force [14] guidelines. A standard FFT algorithm with a suitable windowing function (Hanning window) applied to the stand data (Table 2) demonstrates the compatibility of CGSA with HRV guidelines [14]. Although the absolute values determined by each method were different, the significant main effects and interactions for PTOT, PHI and PLO were the same. Not surprisingly, the normalized sympathovagal balance estimate (PLO / PHI ratio) was also similar between the two methods. In the case of the standard FFT analysis, significance main effects were observed for all three conditions (test day, supine/stand, finisher/non-finisher) (Table 2); whereas, CGSA only found significance for test day and supine/stand (Table 1).
With general FFT analysis, there is not a comparable parasympathetic indicator to CGSA's PHI/PTOT, since the latter estimate relies on the extraction of harmonic and fractal components to determine PHI [24, 25]. Similarly, the suggested sympathetic indicator for FFT and autoregressive analysis (PLO/PTOT, 0.04–0.0.40 Hz) [26] will not be the same as CGSA's PLO/PTOT. In fact, we see that due the nature of the calculation of the FFT sympathetic indicator, the results are identical to that found for sympathovagal balance (Table 2). We suggest that our sympathetic indicator (PLO/PTOT) provides important new information on the relationship between low frequency HRV, orthostatic intolerance and spaceflight.
Conclusion
In summary, we investigated heart rate variability at rest in the supine position and in response to upright posture in 29 astronauts before and after spaceflights lasting up to 16 days. We separated individuals according to their ability to remain standing without assistance for 10 min on landing day. Although both finishers and non-finishers had an increase in sympathetic activity with stand pre-flight, only finishers retained this response post-flight. We also identified pre-flight autonomic responses that might separate finishers and non-finishers. Both groups of astronauts had the expected shift to greater sympathetic over parasympathetic regulation (increased sympathovagal balance, PLO/PHI) of cardiac function from supine to stand on all test days. However, the non-finishers had lower values than finishers did. That this was unaffected by spaceflight suggests the relationship between sympathetic and parasympathetic modulation of heart rate was preserved in both groups following short duration spaceflight. Compared to finishers, non-finishers had higher parasympathetic activity. The mechanism by which higher pre-flight parasympathetic activity might contribute to post-flight orthostatic intolerance is not understood and needs to be investigated further.
Methods
This protocol was approved by the Johnson Space Center Human Research Policy and Procedures Committee. Forty astronauts were familiarized with the study protocol and data collection procedures 30 days pre-flight. Data used for the study was collected 10 days before launch (baseline, pre-flight), on landing day (1–2 h after landing), and 3 days after landing (post-flight), on shuttle missions lasting 8–16 days. Of the 40 original astronaut subjects, 7 were excluded from analysis because they had taken promethazine or dextroamphetamine within 12 h or caffeine within 4 h preceding the test on landing day [11]. Four more subjects were excluded from HRV analysis because their landing day catecholamine values were not available for analysis in our previous paper [11] due to ruined blood samples. Therefore, only 29 astronauts, whose mean age was 39.8 ± 5.2 yr, were used in our analysis.
The research protocol and cardiovascular data for these astronauts have already been presented [11]. On each test day the subject had abstained from caffeine, alcohol, and any medications for the preceding 12 hours; was at least 2 hours postprandial; and had not exercised heavily in 24 hours. Over a 10-minute period the subject was instrumented for blood pressure (Finapres, Ohmeda, Inglewood, CO), heart rate, and transcranial Doppler (Medasonics, Fremont, CA) measurements [11]. After instrumentation, five minutes of supine data were collected. During this period subjects paced their breathing with an auditory signal at 15 breaths per minute. This was followed by a change to the left lateral position for 7-min to perform echocardiography and carbon monoxide rebreathing [11].
Following the carbon monoxide rebreathe procedure, the subjects were returned to the supine position and after 2-min they were assisted to the standing position by three investigators [11]. To minimize blood pressure changes due to the effort of standing, subjects were lifted from behind both shoulders while their feet were swept off the bed [11]. The subjects remained unassisted in the standing position for up to 10 min and were returned to the supine position. Due to limited space within the crew transport vehicle on landing day the assisted stand test was used to approach as closely as possible the conditions of a tilt test. During the first five minutes of the stand test each subject was again requested to follow an auditory signal to pace their breathing at 15 breaths per minute. If the subjects became presyncopal during the stand they were returned immediately to the supine position. Subjects were deemed to be presyncopal if the subject indicated symptoms such as dizziness or nausea, or if we observed any of the following: i) a decrease in HR of more than 15 beats per minute; ii) a decrease in systolic blood pressure of more than 25 mm Hg/min; iii) a decrease in diastolic BP of more than 15 mm Hg/min; or, iv) a decrease in transcranial Doppler middle cerebral artery mean flow velocity of more than 15 cms-1/min.
Data collection
A standard three lead electrocardiograph was used to collect the ECG signal. The analog signal was recorded simultaneously at 12 kHz using an eight-channel digital tape recorder (TEAC RD-111T, Montebello, CA). Beat-by-beat analysis of these data was performed off-line. The peak of the R wave of the ECG tracings were marked by an automated computer system and manually reviewed for anomalies and electrode movement artefact (due to ventilation or to cable movement) that may have affected this process. These data were then used to generate an RR-interval (RRI) time series.
Heart Rate Variability (HRV) analysis
For all subjects, heart rate variability analysis was performed on 256 beat RRI time series segments obtained during the five minute supine data collection and following one minute of stand.
The heart rate signal has been shown to be fractal [40–42]. That is, a broad-band, non-white signal underlies the (harmonic) variations that are normally taken to indicate parasympathetic and sympathetic regulatory control of the heart. We therefore chose to evaluate the beat-by-beat variability of RR-interval with by coarse graining spectral analysis (CGSA) [43] as this method has the ability to extract the harmonic components from the fractal components [43, 44]. The algorithm has been described in detail, along with a demonstration of its efficiency in extracting harmonic from the fractal component, particularly in the very low frequency region, to achieve better spectral estimates with short data sets [43]. From the total power (PTOT), the fractal (PFRAC) and harmonic (PHARM) components are extracted. Although the recommended standard for the lower limit of the low frequency range of heart rate variability is 0.04 Hz [14], this was based on methods that did not isolate harmonic from fractal and was designed to minimize the effect of the fractal component on low frequency power. However, the CGSA algorithm has been demonstrated to be able to efficiently the extract harmonic from the fractal component over the total frequency range (0.0 – 0.50 Hz) [43].
The harmonic component can then be further divided into two frequency regions; high frequency (HI, >0.15 Hz) and low frequency (0.0 – 0.15 Hz) [43]. The high frequency region is respiratory related and mediated by the parasympathetic nervous system, whereas the low frequency region is a consequence of several factors and is a combination of both parasympathetic and sympathetic nervous system activity. From these the integrated low frequency (0.0 – 0.15 Hz, PLO) and high frequency (0.15 – 0.50 Hz, PHI) power can be determined.
Given the distribution of sympathetic and parasympathetic nervous system activity with frequency at the sinus node, PHI/PTOT can be used as an indicator of parasympathetic activity and PLO/PHI has been used as an indicator of sympathetic activity in control of heart rate [45, 46] or sympathovagal balance [47]. Previously we found that due to the large possible range of values generated by this ratio, especially as PHI decreases with orthostatic stress, this number should be normalized by taking its square root [15]. In effect, this is then the ratio of the amplitudes of the low and high frequency regions [15]. It has been suggested that modulation of sympathetic activity on the heart is best estimated when normalized to total power (PLO/PTOT) rather than PHI [47]. Although the computation of the powers by CGSA is different from the autoregressive technique used in the above research, we have also included PLO/PTOT, as determined by CGSA, in our analyses.
This method relies on the respiratory frequency residing above 0.15 Hz. Although we were not able to measure ventilation in these subjects, an attempt was made to achieve this important criterion [14] by requesting the subjects breathe at 15 breaths per minute (0.25 Hz). Analysis of HRV revealed a frequency peak above 0.15 Hz in all subjects.
Statistics
Subjects were grouped based on presence or absence of presyncope on landing day. All individual data groups (i.e. standing in non-finisher group on landing day) were found to be normally distributed using the 'Kolmogorov-Smirnov' test for normality. A repeated measures analysis of variance of test day (pre-flight, landing day, 3 days post flight), stand test (supine, stand) and group (finishers, non-finishers) factors was used with group nested within subjects. The JMP-IN statistical package (SAS Institute Inc.) was used. Due to the missing data from two of the non-finisher subjects during the stand test on landing day, comparisons of finishers and non-finishers was performed using an estimated mean square error. Post hoc analyses using a Student-Newman-Keuls test were performed on specific comparisons related to our hypotheses. These were considered significant if the probability was less than 0.05 (p < 0.05). All data are quoted as mean ± SEM (standard error of the mean).
Abbreviations
- OI:
-
orthostatic intolerance
- HDBR:
-
6° head-down tilt bed rest
- MSNA:
-
muscle sympathetic nerve activity
- F:
-
finishers of landing day 10 minute stand test
- NF:
-
non- finishers of landing day 10 minute stand test
- HRV:
-
heart rate variability
- LF:
-
low frequency
- HF:
-
high frequency
- CGSA:
-
coarse graining spectral analysis
- PTOT:
-
total power
- PFRAC:
-
fractal power
- PHARM:
-
harmonic power
- PLO:
-
harmonic low frequency power (0.0 – 0.15 Hz)
- PHI:
-
harmonic high frequency power (0.15 – 0.50 Hz)
- PHI/PTOT:
-
indicator of parasympathetic activity
- PLO/PHI:
-
sympathovagal balance
- PLO/PTOT:
-
indicator of sympathetic activity
References
Butler GC, Xing HC, Northey DR, Hughson RL: Reduced orthostatic tolerance following 4 h head-down tilt. Eur J Appl Physiol Occup Physiol. 1991, 62: 26-30.
Convertino VA, Doerr DF, Eckberg DL, Fritsch JM, Vernikos-Danellis J: Head-down bed rest impairs vagal baroreflex responses and provokes orthostatic hypotension. J Appl Physiol. 1990, 68: 1458-1464.
Fritsch JM, Charles JB, Bennett BS, Jones MM, Eckberg DL: Short-duration spaceflight impairs human carotid baroreceptor-cadiac reflex responses. J Appl Physiol. 1992, 73: 664-671.
Fritsch-Yelle JM, Charles JB, Jones MM, Beightol LA, Eckberg DL: Spaceflight alters autonomic regulation of arterial pressure in humans. J Appl Physiol. 1994, 77: 1776-1783.
Gaffney FA, Nixon JV, Karlson ES, Campbell W, Dowdney ABC, Blomqvist CG: Cardiovascular deconditioning produced by 20 hours of bedrest with head-down tilt (-5°) in middle-aged healthy men. Am J Cardiol. 1985, 56: 634-638. 10.1016/0002-9149(85)91025-2.
Hughson RL, Yamamoto Y, Butler GC, Güell A, Gharib C: Evaluation of spontaneous baroreflex response after 28 days head down tilt bedrest. Acta Astronautica. 1993, 8: 601-605. 10.1016/0094-5765(93)90076-9.
Hughson RL, Yamamoto Y, Maillet A, Fortrat JO, Pavy-Le Traon A, Butler GC, Güell A, Gharib C: Altered autonomic regulation of cardiac function during head-up tilt after 28-day head-down bed-rest with counter-measures. Clin Physiol. 1994, 14: 291-304.
Parker DE, Reschke MF, Gierke HEV, Lessard CH: Effects of proposed preflight adaptation on eye movements, self-motion perception, and motion sickness: a progress report. Aviat Space Environ Med. 1987, 58: A42-A49.
Zhang LF: Vascular adaptation to microgravity: what have we learned. J Appl Physiol. 2001, 91: 2415-2430.
Buckey JCJ, Lane LD, Levine BD, Watenpaugh DE, Wright SJ, Moore WE, Gaffney FA, Blomqvist CG: Orthostatic intolerance after spaceflight. J Appl Physiol. 1996, 81: 7-18.
Fritsch-Yelle JM, Whitson PA, Bondar RL, Brown TE: Subnormal norepinephrine release relates to presyncope in astronauts after spaceflight. J Appl Physiol. 1996, 81: 2134-2141.
Sigaudo-Roussel D, Custaud M, Maillet A, Güell A, Kaspranski R, Hughson RL, Gharib C, Fortrat J-O: Heart rate variability after prolonged spaceflights. Eur J Appl Physiol. 2002, 86: 358-265. 10.1007/s00421-001-0551-7.
Evans JM, Leonelli FM, Ziegler MG, McIntosh CM, Patwardhan AR, Ertl AC, Kim CS, Knapp CF: Epinephrine, vasodilation and hemoconcentration in syncopal, healthy men and women. Autonomic Neuroscience. 2001, 93: 79-90. 10.1016/S1566-0702(01)00323-X.
Task Force, European Society of Cardiology and the North American Society of Pacing and Electrophysiology: Heart rate variability – Standards of measurement, physiological interpretation, and clinical use. Circulation. 1996, 93: 1043-1065.
Blaber AP, Bondar RL, Freeman R: Coarse grained spectral analysis of HR and BP variability in patients with autonomic failure. Am J Physiol. 1996, 271: H1555-H1564.
Crandall CG, Engelki KA, Pawelczyk JA, Raven PB, Convertino VA: Power spectral and time based analysis of heart rate variability following 15 days head-down bed rest. Aviat Space Environ Med. 1994, 65: 1105-1109.
Hughson RL, Yamamoto Y, Blaber AP, Maillet A, Fortrat JO, Pavy-Le Traon A, Marini JF, Güell A, Gharib C: Effect of 28-day head-down bed rest with countermeasures on heart rate variability during LBNP. Aviat Space Environ Med. 1994, 65: 293-300.
Sigaudo D, Fortrat JO, Maillet A, Allevard AM, Pavy-Le Traon A, Hughson RL, Guell A, Gharib C, Gauquelin G: Comparison of a 4-day confinement and head-down tilt on endorcine response and cardiovascular variability in humans. Eur J Appl Physiol Occup Physiol. 1996, 73: 28-37.
Kamiya A, Michikami D, Fu Q, Iwase S, Hayano J, Kawada T, Mano T, Sunagawa K: Pathophysiology of orthostatic hypotension after bed rest: paradoxical sympathetic withdrawal. Am J Physiol Heart arc Physiol. 2003, 285: H1158-H1167.
Iwase S, Sugiyama Y, Miwa C, Kamiya A, Mano T, Ohira Y: Effects of three days of dry immersion on muscle sympathetic nerve activity and arterial blood pressure in humans. J Auton Nerv Syst. 2000, 79: 156-164. 10.1016/S0165-1838(99)00076-4.
Kamiya A, Iwase S, Kitazawa H, Mano T, Vinogradova OL, Kharchenko IB: Baroreflex control of muscle sympathetic nerve activity after 120 days of 6 degree head-down bed rest. Am J Physiol Regul Integr Comp Physiol. 2000, 278: R445-R452.
Levine BD, Pawelczyk JA, Ertl AC, Cox JF, Zuckerman JH, Diedrich A, Biaggioni I, Ray CA: Human muscle sympathetic neural and haemodynamic responses to tilt following spaceflight. J Physiol. 2002, 538: 331-340. 10.1113/jphysiol.2001.012575.
Dixon EM, Kamath MV, McCartney N, Fallen EL: Neural regulation of heart rate variability in endurance athletes and sedentary controls. Cardiovasc Res. 1992, 26: 713-719.
Goldsmith RL, Bloomfeld DM, Rosenwinkel ET: Exercise and autonomic function. Coronary Artery Disease. 2000, 11: 129-135. 10.1097/00019501-200003000-00007.
Gregoire J, Tuck S, Yamamoto Y, Hughson RL: Heart rate variability at rest and exercise: Influence of age, gender, and physical training. Can J Appl Physiol. 1996, 21: 455-470.
Shi X, Stevens G, Foresman B, Stern S, Raven P: Autonomic nervous system control of the heart: endurance exercise training. Med Sci Sports Exerc. 1995, 27: 1406-1413.
Shin K, Minamitani H, Onishi S, Yamazaki H, Lee M: Autonomic differences between athletes and nonathletes: spectral analysis approach. Med Sci Sports Exerc. 1997, 29: 1482-1490.
Rowell LB: Central circulatory adjustments to dynamic exercise. In: Human Cardiovascular Control. Edited by: Rowell LB. 1993, New York: Oxford University Press, 162-203.
Klein KE, Wegmann HM, Kuklinski P: Athletic endurance training- advantage for space flight?: the significance of physical fitness for selection and training of spacelab crews. Aviat Space Environ Med. 1977, 48: 215-222.
Convertino VA: Aerobic fitness, endurance training, and orthostatic intolerance. Exerc Sport Sci Rev. 1987, 15: 223-259.
Raven PB, Pawelczyk JA: Chronic endurance exercise training: a condition of inadequate blood pressure regulation and reduced tolerance to LBNP. Med Sci Sports Exerc. 1993, 25: 713-721.
Harm DL, Jennings RT, Meck JV, Powell MR, Putcha L, Sams CP, Schneider SM, Shackelford LC, Whitson PA: Genome and Hormones: Gender Differences in Physiology Invited Review: Gender issues related to spaceflight: a NASA perspective. J Appl Physiol. 2001, 91: 2374-2383.
Waters WW, Ziegler MG, Meck JV: Postspaceflight orthostatic hypotension occurs mostly in women and is predicted by low vascular resistance. J Appl Physiol. 2002, 92: 586-594.
Evans JM, Ziegler MG, Patwardhan AR, Ott JB, Kim CS, Leonelli FM, Knapp CF: Gender differences in autonomic cardiovascular regulation: spectral, hormonal, and hemodynamic indexes. J Appl Physiol. 2001, 91: 2611-2618.
Frey MAB, Tomaselli CM, Hoffler WG: Cardiovascular responses to postural changes: differences with age for women and men. J Clin Pharmacol. 1994, 34: 394-402.
Gotshall RW, Tsai PF, Frey MAB: Gender-based differences in the cardiovascular response to standing. Aviat Space Environ Med. 1991, 62: 855-859.
Shoemaker JK, Hogeman CS, Khan M, Kimmerly DS, Sinoway LI: Gender affects sympathetic and hemodynamic response to postural stress. Am J Physiol Heart arc Physiol. 2001, 281: H2028-H2035.
Geelen G, Laitinen T, Hartikainen J, Länsimies E, Bergstrom K, Niskanen L: Gender influence on vasoactive hormones during 70° head up tilt in healthy humans. J Appl Physiol. 2002, 92: 1401-1408.
Fadel PJ, Stromstad M, Wray DW, Smith SA, Raven PB, Secher NH: New insights into differential baroreflex control of heart rate in humans. Am J Physiol Heart Circ Physiol. 2003, 284: H735-H743.
Goldberger AL: Fractal mechanisms in the electrophysiology of the heart. IEEE Eng Med Biol. 1992, 47-52. 10.1109/51.139036. June
Peng CK, Mietus J, Hausdorff JM, Havlin S, Stanley HE, Goldberger AL: Long-range anticorrelations and non-Gaussian behavior of the heartbeat. Phys Rev Let. 1993, 70: 1343-1346. 10.1103/PhysRevLett.70.1343.
Saul JP, Albrecht P, Berger RD, Cohen RJ: Analysis of long term heart rate variability: methods, 1/f scaling and implications. Comput Cardiol. 1988, 14: 419-422.
Yamamoto Y, Hughson RL: Extracting fractal components from time series. Physica D. 1993, 68: 250-264. 10.1016/0167-2789(93)90083-D.
Butler GC, Yamamoto Y, Xing H, Northey DR, Hughson RL: Heart rate variability and fractal dimension during orthostatic challenges. J Appl Physiol. 1993, 75: 2602-2612.
Yamamoto Y, Hughson RL: On the fractal nature of heart rate variability in humans: effects of data length and β-adrenergic blockade. Am J Physiol. 1994, 266: R40-R49.
Yamamoto Y, Hughson RL, Peterson JC: Autonomic control of heart rate during exercise studied by heart rate variability spectral analysis. J Appl Physiol. 1991, 71: 1136-1142.
Pagani M, Malliani A: Interpreting Oscillations of muscle sympathetic nerve activity and heart rate variability. J Hypertension. 2000, 18: 1709-1719. 10.1097/00004872-200018120-00002.
Acknowledgements
We thank all the astronauts who participated in this study. This research was supported by National Aeronautics and Space Administration Contract NAS9-18942 and Natural Sciences and Engineering Research Council, Medical Research Council, Canadian Space Agency Industry University Partnership Grant 669-008/93.
Author information
Authors and Affiliations
Corresponding author
Additional information
Authors' contributions
APB was responsible for the analysis and the interpretation of the heart rate variability. RLB and MSK designed the study and helped recruit the subjects. All participated in the overall interpretation of the data and in the production of the final version of the manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Blaber, A.P., Bondar, R.L. & Kassam, M.S. Heart rate variability and short duration spaceflight: relationship to post-flight orthostatic intolerance. BMC Physiol 4, 6 (2004). https://doi.org/10.1186/1472-6793-4-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1472-6793-4-6