
Abstract
Background
Ruptured renal neoplasms can be a catastrophic clinical presentation. Angiomyolipoma is the commonest renal tumor which presents in this fashion. Renal sarcomas are rare renal neoplasms. Renal leiomyosarcomas are the most common histological subtype of renal sarcomas, accounting for approximately 50–60% of the reported cases. These tumors are usually peripherally located and appear to arise from either the renal capsule or smooth muscle tissue in the renal pelvic wall.
Case presentation
A 70 years old male, with hypertension and ischemic disease, developed acute left flank pain. The general physician evaluated this using ultrasound, which showed a solid left renal mass. Two weeks later, he presented in the emergency room in a state of shock with a palpable flank mass. CT scan of the abdomen showed a large heterogeneous mass lesion in the left perinephric space with minimal post contrast enhancement. Per-operatively, large retroperitoneal hematoma was found within Gerota's fascia along with spleen plastered to the upper limit of hematoma. Nephrectomy and splenectomy were performed. Postoperative course was uneventful and patient was discharged on the 10th post-operative day. Histopathological evaluation of the specimen showed high-grade leiomyosarcoma
Conclusions
Spontaneous rupture of renal neoplasm is a rare clinical presentation. Angiomyolipoma is the commonest cause of spontaneous rupture of the kidney. Presentation of a leimyosarcoma as a ruptured renal neoplasm has not been previously reported in the English literature.
Similar content being viewed by others


Background
Leiomyosarcomas of the kidney make up to 0.5–1.5% of malignant renal tumors in adults [2]. There is no difference in the gender distribution with a mean age at diagnosis in the sixth decade. They typically presents with the classical triad of symptoms i.e. flank pain, hematuria, and abdominal mass mimicking renal cell carcinoma. Radiological findings are nonspecific and diagnosis is usually made postoperatively.
Spontaneous rupture of renal neoplasm is commonly seen for large angiomyolipoma, occasional case report also describes cases of renal cell cancers and Wilm's tumor. Ruptured renal leiomyosarcoma is not previously reported in English literature. In non-English literature, there are two cases [2, 3]. Yoshikawa et al reported a case of a spontaneously ruptured renal leiomyosarcoma, treated by nephrectomy followed by immuno-chemotherapy and radiotherapy [2]. At 18 months, follow up of patient was free of local recurrence and distant metastasis. Kyuno et al reported a case of spontaneous rupture of leiomyosarcoma, who died 2 months after nephrectomy of intestinal perforation.
Case presentation
A 70 years old male, known case of hypertension and ischemic disease, developed acute left flank pain, the general physician evaluated this by an ultrasound that showed a solid left renal mass. He was referred to this hospital for further evaluation, however, he presented in the emergency room with sudden onset of severe central abdominal pain, radiating to left flank increasing with movement and associated with two episodes of non-bilious vomiting. On clinical examination patient was haemodynamically stable, pale looking, with a bi-manually palpable left flank mass, extending to right hypochondrium. Initial laboratory work up showed a low Hemoglobin 6.1 g/dl (13.7–16.3), urinalysis showed microscopic haematuria, and serum creatinine 1.8 mg/dl.
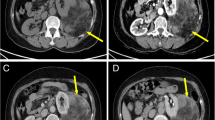
CT scan of abdomen (Figure 1) showed a large heterogeneous mass lesion in the left perinephric space with minimal post contrast enhancement. After adequate resuscitation, nephrectomy was performed. Per-operatively, large retroperitoneal hematoma was found within Gerota's fascia along with spleen plastered to the upper limit of hematoma. Nephrectomy and splenectomy were performed. Postoperative course was uneventful and patient was discharged on 10th post-operative day. Histopathological evaluation of the specimen showed high-grade leiomyosarcoma (figure 2). Sections were stained for a broad panel of immunohistochemical markers using monoclonal antibodies, which was positive for vimentin and α-smooth muscle actin (ASMA) and negative for desmin, S-100 and CD34. Patient refused radiotherapy and died 4 months after surgery.

Post contrast spiral CT showing large retroperitoneal hematoma with minimal contrast uptake by the renal tissue confined to the upper pole of the left kidney.

High power photomicrograph of Leiomyosarcoma exhibiting irregular bundles of spindle and polyhydral cells having pleomorphic vesicular nuclei. An abnormal mitotic figure is present in the center of the picture (H & E × 200).
Conclusions
Spontaneous rupture of renal neoplasm is a rare clinical presentation. Angiomyolipoma are the commonest cause of spontaneous rupture of kidney. Presentation of a leimyosarcoma as a ruptured renal neoplasm has not been previously reported in English literature.
Leiomyosarcomas even when confined to the kidney have a poor prognosis. Radical surgery offers the best chance of cure; role of adjuvant chemo-immunotherapy and/or radiotherapy remains debatable, due to paucity of data on the treatment of this rare renal neoplasm and divergent results from limited experience in literature.
References
Srinivas V, Sogani PC, Hadju SI, Whitmore WF: Sarcomas of the Kidney. J urol. 1984, 132: 13-16.
Yoshikawa M, Hayashi Y, Sanma S, Maruyama Y, Hirao Y, Okajima E: Spontaneous rupture of renal leiomyosarcoma: report of a case. Hinyokika-Kiyo. 1986, 32 (9): 1282-7.
Kyuno H, Iwamura M, Muramoto M, Kou H, Koshiba K: A case of spontaneous rupture of renal leiomyosarcoma. Hinyokika-Kiyo. 1996, 42 (8): 583-6.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2490/2/13/prepub
Acknowledgements
Written consent was obtained from the patient's relative for publication of the patient's details.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contributions
MM carried out the literature search and drafted the manuscript. MHA proposed that the manuscript be drafted, literature search and drafted the manuscripts. ASH conceived of the study, and participated in drafting the pathology aspect of the manuscript.
All authors read and approved the final manuscript.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
{kind=link}
{kind=link}
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Moazzam, M., Ather, M.H. & Hussainy, A.S. Leiomyosarcoma presenting as a spontaneously ruptured renal tumor-case report. BMC Urol 2, 13 (2002). https://doi.org/10.1186/1471-2490-2-13
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2490-2-13