
Abstract
Background
Abdominal surgical site infections are among the most common complications of inpatient admissions and have serious consequences for outcomes and costs. Different risk factors may be involved, including age, sex, nutrition and immunity, prophylactic antibiotics, operation type and duration, type of shaving, and secondary infections. This study aimed to determine the risk factors affecting abdominal surgical site infections and their incidence at Imam Khomeini, a major referral teaching hospital in Iran.
Methods
Patients (n = 802) who had undergone abdominal surgery were studied and the relationships among variables were analyzed by Student's t and Chi-square tests. The subjects were followed for 30 days and by a 20-item questionnaire. Data were collected through pre- and post-operative examinations and telephone follow-ups.
Results
Of the 802 patients, 139 suffered from SSI (17.4%). In 40.8% of the cases, the wound was dirty infected. The average age for the patients was 46.7 years. The operations were elective in 75.7% of the cases and 24.7% were urgent. The average duration of the operation was 2.24 hours, the average duration of pre-operative hospital stay 4.31 days and the average length of (pre- and post-operation) hospital stay 11.2 days. Three quarters of the cases were shaved 12 hours before the operation. The increased operation time, increased bed stay, electivity of the operation, septicity of the wound, type of incision, the administration of prophylactic antibiotic, type of operation, background disease, and the increased time lapse between shaving and operation all significantly associated with SSI with a p-value less than 0.001.
Conclusion
In view of the high rate of SSI reported here (17.4% compared with the 14% quoted in literature), this study suggests that by reducing the average operation time to less than 2 hours, the average preoperative stay to 4 days and the overall stay to less than 11 days, and approximating the timing of shaving to the operation and substituting cefazolin for cefaluthin when prophylactic antibiotic is to be administered, the SSI may be reduced to a more acceptable level.
Similar content being viewed by others

Background
SSIs are among the most common hospital acquired infections comprising 14–16 percent of inpatient infections[1]. SSI is a dangerous condition, a heavy burden on the patient and social health system[2]. Such infections lengthens bed stay for an average of seven days. Potential sources of infection are the patient (especially contamination by alimentary tract bacteria), hospital environment, food, other patients, staff, infected surgical instruments, dressings, and even drugs and injections [3]. The incedence of SSIs with regard to abdominal surgical sites and operating conditions is as follows:
Clean wounds (1.5–3.7%); clean-contaminated wounds (3–4%); contaminated wounds (8.5%); dirty-infected wounds (28–40%); in laparoscopy (10%) umbilical hernia (2–5%); in the cancer of the colon without taking antimicrobial drugs (30–60%); or with antibiotic and proper intestine wash (10%); in colostomy (above 50%); in colon perforation (20%); in stomach cancer and surgery (20%); in hernionite (50%); in adult appendectomy (10–20%); in children's appendicitis (2–5%); in aged appendicitis and in pregnant women (10–50%); and in AIDS victims (above 50%); in liver abscess (20%); in hydatid cyst (2–5%); in acute and chronic cholecystectomy without stones (10%); in acute septic cholangitis (10–20%); in laparoscopic cholecystectomy (2–5%); and in splenectomy (2–5%) [4].
SSI is identified with redness, inflammation, heat, pain, a temperature of 38°C, and septic drainage from the surgical site during the 30 days following operation[4]. Several factors are to be taken into account for SSI, some of which are as follows:
While we could not find any significant correlation between sex and SSI rate, age proved to be an important factor; the rate of wound infection for 15 to 24-year-old patients was only10% but increased significantly for those over 65 years of age. The extent of SSI was doubled for obese patients. The duration of surgical operation also proved to be a significant factor: only 3% of operations lasting 30 minutes or less led to infection, while for operations lasting more than 6 hours this rate leapt to 18%. SSI rate increased with longer durations of preoperative bed stay, but preoperative showers with a disinfecting soap such as chlorhexidine or Betadine decreased the cutaneous bacterial load. According to Kruise, the rate of infection was reduced to 1.3% among patients who showered with disinfecting soap containing hexachlorophene. In those who showered with ordinary soap the corresponding figure was 2.1%, and for patients who did not shower at all it increased to 2.3%. However, another study on 5536 subjects showed no decrease in SSI in patients who showered with chlorhexidine preoperatively; the rate was 4% [4]. Among other factors that delay wound healing or increase the infection rate are cigarette smoking, which increases the postoperative infection rate 5-fold, and the use of steroids, which delays wound healing and increases the infection rate by 9 percentage points from 7% to 16%. Aseptic surgical techniques are claimed to decrease the infection rate, though not to zero [3]. However, the administration of prophylactic antibiotics 30 to 60 minutes before surgery, decreases the incidence of SSI [4–10]. Obviously, remote infections increase SSI. Other contributing factors are the type of surgery and secondary infections. The object of this study was to assess SSI, and the incedence of the factors contributing to such infections at Imam Khomeini Hospital in Iran.
Methods
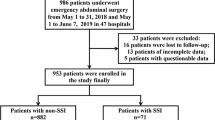
In this study, 802 patients in a teaching hospital during the 15 months from April 2002 to July 2003 underwent abdominal surgery and were studied for SSI and the factors affecting it. Initially, 884 patients were recruited for the study but 82 were excluded on the basis of the following criteria: deficient medical records; patients operated at a different hospital and subsequently transferred to Imam's Hospital: or patients deceased during the operation or within the following 30 days.
The dependent variable in this study was abdominal surgical site infection, defined as redness, swelling, pain, temperature above 38°C, during the 30 days after operation. The independent variables were: age, sex, site operated, body mass index, time of shaving the site of incision, administration of prophylactic antibiotics, type of surgical operation, duration of operation, duration of preoperative bed stay; preoperative shower, type of shaving, and accompanying conditions.
The data were collected through a 20-item questionnaire. The stages for data collection and information completion were as follows: identification of patients; preoperative interview; postoperative interview; record completion; weekly examinations and telephone follow-ups for 30 days following operation; and pre-discharge examinations. The collected data were analyzed by the SPSS 10 package, using Student's t-test for continuous variables and chi-square test.for categorical variables.
To the best of our ability, this study was conducted with due attention to research ethics.however, problems met in the follow-ups the patient's discharge imposed limitations on the study
Results
Of the 802 patients studied who had undergone abdominal surgery 139 (17.4%) suffered from SSI as defined in Table 1. No infections were observed in the other 663 cases (82.7%). So far as wound type was concerned, we found clean wounds in 109 cases (13.6%); clean-contaminated wounds in 214 cases (26.7%); contaminated wounds in 307 cases (45.8%); and dirty infected wounds in 112 cases (14%). While 255 cases (28.1%) did not shower before the operation, the other 577 patients (71.9%) did.
The body mass index for 73 patients (9.1%) was above 30, indicating obesity. Over half the patients (403 cases) suffered from accompanying conditions such as diabetes, high arterial blood pressure, kidney or liver failure, malignancy, febrile condition, cardiac disorders, thyroid disorders, blood disease, chronic obstructive pulmonary disease, convulsion, hyperlipidemia, or immunological disorders; or had previously undergone surgical operations. The rest were free of accompanying conditions (Table 2).
We found no significant correlations between SSI incidence and sex or preoperative shower. However, correlations with duration of operation, duration of preoperative bed stay, electivity of surgery, lengthening of preoperative shaving time, increasing age, wound infection, site of surgery, type of incision, accompanying disorders, and type of prophylactic antibiotic administered before operation were all significant at p < 0.001. Although differences in SSI rates were not significantly related to BMI, a trend was apparent: SSI rate was higher with low and high BMI.
The following prophylactic antibiotics were used: ampicillin, gentamicine, cephalothin, metronidazole, ceftriaxone and cefazoline (table 3).
Discussion
For the 802 participants in this study, the SSI reported was 17.4%, which is well above the 14–16% reported in other studies [1]. There were particularly high values in cases of umbilical hernia (14.3% compared with previously reported 5%) and stomach cancer (39.7%; in previous studies 20%) [4]. Increasing age is correlated with greater likelihood of certain chronic conditions, malnutrition and a fall in the body immunological efficiency, causing more extensive SSI [4]. The present findings supported this argument (p = 0.001).
SSI is not correlated with sex [5], in agreement with previous findings (p = 0.093). The literature shows that SSI increases with obesity, one reason being a decrease in blood circulation in fat tissues [7]. Malnutrition is another factor predisposing to SSI [5]. In this study we considered a BMI of above 30 obese and that of below 20 as malnutrition, found no significant correlations between the two ranges and SSI extensity (p = 0.692). But, the previously reported correlation between SSI and pre-operation bed stay (p = 0.018) [4, 5] was supported by this study. This is one of the factors to be taken into account. Thus by reducing pre-operation bed stay we may decrease SSI. The findings of this study also proved the risk of SSI to be less in elective surgeries than those referred to emergency departments as cases of acute abdomen, which could result from lack of readiness for operation on the patient's side. Here we should reduce risk factors by preparing the patient for the urgent operation as much as possible.
The findings supported the literature by showing that administration of prophylactic antibiotic half an hour before the operation would bring about the best results and the lowest SSI [10]. This was proved for all antibiotics (p = 0.001) with the exception of cephalothin with (p = 1), which requires a lot more research.
The literature shows that with the duration of above 2 hours, the risk of SSI increases [4]. The average time in this study was 2.24 hours, which must be reduced to below 2 hours although the nature of surgical operations is not always the same.
The time of shaving when it approaches the operation and if done by clippers, reduces the SSI risk. In this study the two times: one hour before surgical operations and 12 hours before that were contrasted which supported previous findings with p = 0.001. This is one area where we can lower the risk by approximating the time of shaving as much as possible to that of operation.
Other such factors quoted in the literature as the conditions of the operating theatre, personal hygiene, acompanying diseases, immunological disorders, smoking, techniques of surgery, the surgeon's expertise, duration of surgical scrub, preoperative skin preparation, poor hemostasis, failure to obliterate dead space, tissue trauma, and inadequate sterilization of instruments, which were not included in this study might be considered as confounding factors.
Conclusion
Considering the relatively higher rate of SSI in this study (17.4% compared with the 14% quoted in the literature), especially in such cases as stomach cancers and umbilical hernia, where the rate is considerablly higher, we should carefully reconsider the whole operation procedure. In general, we should do our best to reduce the average operation duration to less than 2 hours and the average preoperative bed stay to less than 4 days. Thus, the present average of 11.2 days for the total bed stay would be reduced to less than 11 days. The time of shaving should approximate the operation time as much as possible. Finally, when the administration of prophylactic antibiotics is required, cefazoline is recommended to substitute cephalothin.
Razavy: main researcher (design, analysis, report)
Ibrahimpour: (implementation, analysis)
Sabouri Kashani: (report, edit)
Jafarian: (counsult)
References
Skarzynska J, Cienciala A, Madry R, Barucha P, Kwasniak M, Wojewoda T, Sroga J: Hospital infection in general surgery wards. Przegl Epidemiol. 2000, 54 (3–4): 299-304.
Troillet N, Petignant C, Matter M, Eisenring MC, Mosimann F, Francioli P: Surgical site infection surveillance: an effective preventive measure. Rev Med Suisse Romande. 2001, 121 (2): 125-8.
Burkitt Jf: Identification of the sources of staphylococci contaminating the surgical wound during operation. Ann Surg. 1963, 158: 898-904.
Schwartz SI, Comshires G, Spencer FC, Dally GN, Fischer J, Galloway AC: Principles of surgery. 1999, NY: McGraw-Hill companies, 83-7
Habte-Gabr E, Gedebau M, Kronvall G: Hospital-acquired infections among surgical patients in Tikur Anbessa Hospital, Addis Ababa, Ethiopia. Am J Infect Control. 1988, 7-13.
Lecuona M, Torres Lana A, Delgado-Rodriguez M, Llorc J, Sierra A: Risk factors for surgical site infections diagnosed after hospital discharge. J Hosp Infect. 1988, 39 (1): 71-4. 10.1016/S0195-6701(98)90246-8.
Nystrom PO, Jonstam A, Hojer H, Ling L: Incision infection after colorectal surgery in obese patients. Acta chir scand. 1987, 153 (3): 225-7.
Nichols RL: Preventing surgical site infections: A Surgeon's Perspective. Emerg Infect Dis. 2001, 7 (2): 220-4.
Majidpoor A, Jabarzadeh S: Hospital acquired infections, how to control. Emerging, Re-emerging infectious diseases and Employee Health. Edited by: Hatami. 2004, Tehran: Ministry of health and medical education, Center for disease management, 1: 263-321.
Gante JE: Manual of Antibiotics and Infectious Disease Treatment and Prevention. 2002, L.W.W, 630-730. 9
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR: Guidelines for Prevention of surgical site infection 1999. Infect Control Hosp Epidemiol. 1999, 20 (4): 250-78.
Gilbert N, David , Moellering , Robert C, Sande , Merle A: The Sanford Guide to antimicrobial Therapy. 1998, Cambridge: Cambridge University Press. INC
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2482/5/2/prepub
Acknowledgements
Grateful thanks are due to the professors at surgery departments, their personnel, and the staff at medical records department. We should also express our gratitude to the statistics advisors at the dean's office for research at the school of medicine. Finally, we should thank Ms. Bakhshandeh for typing the final version.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Razavi, S.M., Ibrahimpoor, M., Sabouri Kashani, A. et al. Abdominal surgical site infections: incidence and risk factors at an Iranian teaching hospital. BMC Surg 5, 2 (2005). https://doi.org/10.1186/1471-2482-5-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2482-5-2