
Abstract
Background
Variance of peak bone mass has a substantial genetic component, as has been shown with twin studies examining quantitative measures such as bone mineral density (BMD) and quantitative ultrasound (QUS). Evidence implicating single nucleotide polymorphisms (SNPs) of the transforming growth factor beta-1 (TGFB1) gene is steadily accumulating. However, a comprehensive look at multiple SNPs at this locus for their association with indices of peak bone mass has not been reported.
Methods
A cohort of 653 healthy Caucasian females 18 to 35 years old was genotyped for seven TGFB1 SNPs. Polymorphisms were detected by restriction endonuclease digestion of amplified DNA segments.
Results
The frequencies of the least common allele at G-800A, C-509T, codon 10 (L10P), codon 25 (R25P), codon 263 (T263I), C861-20T, and 713-8 delC loci were 0.07, 0.33, 0.41, 0.08, 0.04, 0.25 and 0.01, respectively. A significant association was seen between QUS Stiffness Index (QUS-SI) and the SNP at codon 10 and the linked promoter SNP, C-509T. This association remained significant after multiple regression was used to incorporate important clinical covariates – age, BMI, level of activity, family history, and caffeine intake – into the model.
Conclusion
The association of QUS-SI with -509T is consistent with a gene-dose effect, while only individuals homozygous for the codon 10P allele showed a significant increase. In this cohort of young healthy Caucasian females, the T allele at position -509 is associated with greater bone mass as measured by calcaneal ultrasound.
Similar content being viewed by others


Background
Osteoporosis is a common disorder of aging characterized by low bone mineral density (BMD), deteriorating bone microarchitecture, and increased fracture rate. Osteoporosis and BMD are both complex traits with a strong genetic component [1, 2]. Among the genes that have been associated with BMD are those encoding the vitamin D receptor [3, 4], the estrogen receptors [5, 6], collagen Iα1 [7], apolipoprotein E [8], and TGFB1 [9].
Abundant in bone matrix [10], secreted TGFB1 is an important regulator of osteoblast proliferation and differentiation and directly affects bone formation in vivo [11]. Activating mutations in humans are associated with Camurati-Engelmann disease, a disorder of progressive diaphyseal dysplasia characterized by increased BMD [12, 13]. Homozygous knock-out of the TGFB1 gene in mice is associated with an osteopenic phenotype [14]. It is not surprising, therefore, that the TGFB1 locus has emerged as a strong candidate gene in the study of osteoporosis genetics.
The TGF-β1 amino acid sequence is highly conserved across mammalian species, indicating a strong selection against variant forms of the protein [15]. Variable expression or activation of TGF-β1 may therefore be associated with altered bone remodeling and different overall BMD [6]. Thus, elevated serum TGF-β1 levels are associated with osteosclerosis, and conversely, decreased serum TGF-β1 with osteopenia.
Nine TGFB1 SNPs have been identified and studied. Three reside in the promoter region (C-988A, G-800A, C-509T). An insertion of a basepair is found in the 5' UTR at n.+72C. Two SNPs are in the signal sequence (L10P or n.T869C, and R25P or n.G915C), one in exon 5 (T263I or c.C788T) [16], and one in each of introns 4 and 5 (713-8delC [17] and C861-20T [18], respectively) (Figure 1).

Polymorphic loci of the TGFB1 gene. Each locus (A to G) is shown in relation to the promoter, transcription start site (arrow), the exons (rectangles), the pre-propeptide (white rectangles), propeptide (black rectangles) and mature sequence (grey rectangles). Synonyms for each SNP (named differently by different researchers depending on annotation of position 1) are given in the shaded boxes.
A number of studies have examined the association of TGFB1 polymorphisms with TGF-β1 levels. In post-menopausal British women, the -509T allele was associated with higher total serum TGF-β1 [19], but this association was not confirmed in post-menopausal Chinese [20] or Japanese cohorts [21]. Similarly, the L allele at codon 10 was found to be associated with higher serum TGF-β1 levels in middle aged European women [22], but these findings were not confirmed in elderly Australian [23] or Chinese [20] women.
Other studies have also examined these allelic variants with respect to effects on bone. In 256 postmenopausal Italian women, Bertoldo et al. found strong evidence of association between the 713-8delC SNP and: (i) femoral neck BMD (FN-BMD), (ii) prevalence of hip fractures, and (iii) high bone turnover [24]. In 123 osteoporotic cases and 131 matched normal controls, Langdahl et al. found that the same 713-8delC deletion was associated with low bone mass and increased bone turnover [17]. In 76 pre-menopausal women, Keen et al. reported that the 861-20C allele was associated with higher BMD at the femoral neck, but not at the lumbar spine or with quantitative ultrasound (QUS) at the heel [18]. In a subsequent publication by Langdahl et al. involving 1168 osteoporotic cases and controls, the T allele at T861-20C was associated with significantly higher LS and FN BMD, while the T allele at C-509T was significantly associated with higher FN BMD, and the Pro allele of L10P was associated with greater FN BMD [25]. A study of the L10P variant in 625 Japanese women showed significant association of the 10P allele with higher lumbar spine (LS) BMD and total BMD [21]. This study also examined the -509 site and concluded that -509 T allele, alone or in combination with 10P, is a genetic determinant for osteoprosis. However, the more common allele at codon 10 (leucine) was found to be associated with higher LS BMD and FN BMD in middle-aged European women [22] and with higher FN BMD in Chinese elderly [20]. In 1337 elderly Australian women, the 10P allele associated with lower hip BMD and heel QUS [23]. The codon 10 polymorphism was not seen to have any association to BMD in 3382 elderly Caucasian American females [26]. In 356 healthy Japanese adolescents, however, the -509 CC homozygotes were found to have 5 to 6% greater radial BMD, and higher bone mineral content than the corresponding TT group [27].
In none of these reports were multiple SNP sites examined simultaneously in relation to peak bone mass. We therefore undertook a study of seven TGFB1 polymorphisms in relation to BMD indices as well as clinical covariates in a group of healthy young women with well characterized clinical and laboratory phenotypes to determine their relationship to peak bone mass.
Methods
Subjects
The 653 healthy non-related Caucasian female subjects presented in this report were recruited by advertising for a study of bone and mineral metabolism in the Greater Toronto Area, as described previously [4, 6]. In this study, data on 25 women identified as originating from the Indian sub-continent were excluded.
The study protocol was approved by the Institutional Review Board of the University of Toronto (Toronto, ON) and written consent was obtained from each individual at the onset of the study [4]. Each subject completed a standardized questionnaire about lifestyle factors, menstrual and reproductive history, past history of medical diseases, current and prior medication use, history of fractures, and family history of osteoporosis. Summary clinical characteristics (mean ± SD) include: age, 27.5 ± 4.5 yr (range 18 to 35 yr); weight, 63.3 ± 11.6 kg; height, 1.65 ± 0.06 m; and BMI 23.2 ± 3.9 kg/m2.
Assessment of BMD
BMD was measured at the hip (left femoral neck = FN) and lumbar spine (L2-L4 = LS) by dual-energy X-ray absorptiometry using a DPX-L absorptiometer (Lunar Corp., Madison, WI, U.S.A.). BMD was reported as grams per square centimeter. Quantitative Ultrasound (QUS) measurements were also conducted, consisting of broadband ultrasound attenuation (BUA, dB/MHz), speed of sound (SOS, m/s) and the calculated heel stiffness index (SI, % of age-matched controls), at the right heel (Lunar Achilles; Lunar Corp., Madison WI), as published previously [4]. Summary statistics for our study cohort were: LS-BMD, 1.19 ± 0.13 g/cm2; FN-BMD, 1.00 ± 0.12 g/cm2; and QUS-SI, 97.2 ± 14.1.
DNA isolation and genotyping
DNA was extracted from EDTA-anticoagulated blood as previously described [6]. Gene fragments including the SNPs of interest were amplified by polymerase chain reaction (PCR). Of the nine SNPs known in this region, two were not included in this study. SNPs are named by either nucleotide sequence or amino acid sequence, using the most commonly reported annotation in literature. The SNP +72C was not examined, since previous work [16] revealed it to be in complete linkage with the codon 25 SNP. An additional SNP in the promoter, C-988A, was excluded because the frequency was reported to be only 0.2% [16]. The relative positions of the remaining seven intragenic SNPs are shown in Figure 1. To genotype the C861-20T SNP, previously published methods were used [18]. Methods for genotyping the other six SNPS by PCR amplification and RFLP digestion are similar to those previously published [4]. Given their pairwise proximity, three amplicons were used for genotyping: one for the pair of promoter SNPs, -800 and -509, a second for codon 10 and codon 25, and a third for 713-8delC and codon 263. Primer pairs are given in Table 1. PCR conditions were: 94°C for 1 min (denaturing), 62°C for 40 secs (primer annealing), and 72°C for 1 min + 1 second/cycle (extension) for 35 cycles. Two μl of Q-solution (Qiagen Corp) were added to the codon 10/25 PCR mixture to facilitate amplification of this GC-rich fragment. Also listed in Table 1 are the restriction endonuclease enzymes used to detect one of the two alleles (as specified). Digested DNA products were run on pre-cast Clearose BG wide-mini S-50 gels (Elchrom Scientific, Zurich, Switzerland) and stained with ethidium bromide. All genotypes were sequenced to confirm restriction digestion results.
Statistical analysis
Haplotyping of -800 and -509 SNP loci was possible since both SNPs were amplified in one PCR product, and simultaneous digestion by Eco 181 and Tai I produced a unique pattern of fragments for each possible haplotype [28, 29]. Loci were tested for Hardy-Weinberg (HW) equilibrium of the distribution of the genotypes, and pairwise linkage disequilibrium (LD) coefficients calculated and normalized (Δ'), using methods of Weir et al. [30], and improved software as we have described [31]. Bivariate correlations between BMD, QUS-SI, and lifestyle factors, menstrual and reproductive factors, and TGFB1 genotypes were assessed using Spearman rank correlation coefficients, as reported previously [4, 6]. Each TGFB1 SNP was added to the model without any clinical covariates and then with covariates used in our established model [6]. All data analyses were performed with SPSS for Windows 10.0.7 (SPSS Inc., Chicago, Illinois, U.S.A.).
Results
TGFB1 polymorphisms
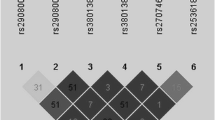
Frequencies of the minor alleles were: codon 10 (41%), -509 (33%), C861-20T (25%), codon 25 (8%), -800 (7%), codon 263 (4%), and 713-8delC (1%). For the -800 and -509 haplotypes, 4.3% (n = 28) of the samples were doubly heterozygous, and all were in trans, as detected by sequential enzyme digestion (data not shown). Shown in Table 2 are the pair-wise standardized LD coefficients (Δ'). In this population the -509 is closely linked to codon 10 (Δ' = 0.88) and is in negative LD with 713-8delC (Δ' = -0.77). Codon 10 is also in negative LD with 713-8delC (Δ' = -0.80).
Clinical characteristics by TGFB1 genotype
In comparing clinical parameters among genotype groups, no significant differences were observed for age, weight, height, calcium intake, caffeine intake, or BMI. Summary data grouped by -509 and codon 10 genotypes are shown in Table 3. Results for other genotypes are not shown, as there are no significant differences, and the other SNPs as explained below were not significant determinants of peak bone mass in this population.
TGFB1 SNPs and clinical characteristics
Correlations of QUS-SI, lumbar spine BMD, and femoral neck BMD with clinical, lifestyle and the TGFB1 genotypes are shown in Table 4. As previously reported for this cohort, LS BMD is positively correlated with age, height, weight, BMI and level of physical activity as an adolescent [4]. At the hip, significant positive correlations of BMD were found with height, weight, BMI, calcium intake, and the amount of physical activity reported at time of study and during adolescent years. Negative correlations were seen with age and the amount of caffeine consumption for the FN BMD. Heel QUS was positively correlated with the same factors as FN BMD, with the exception of calcium intake.
Association of TGFB1 genotypes with BMD and QUS
There was no significant correlation of any TGFB1 SNP with BMD at FN or LS (data not shown). Of the seven loci, only the -509 SNP was significantly correlated with QUS-SI. (r = 0.078, p = 0.038). Since this SNP is in strong linkage disequilibrium with codon 10 (Δ' = 0.88) and 713-8delC (Δ' = -0.77), all three of these SNPs were included in further analysis.
The number of T alleles (0, 1 or 2) at the -509 site shows significant association with QUS-SI (Figure 2). Mean QUS-SI was higher in TT homozygotes (101.2 ± 12.9) than in CT heterozygotes (97.42 ± 10.30, p = 0.04) or CC homozygotes (95.8 ± 9.31, p = 0.006) and in heterozygotes versus CC homozygotes (p < 0.05). A similar allele-dose effect was not observed with the codon10 SNP; homozygotes for the rare allele (PP group) had a significantly higher mean QUS-SI (100.6 ± 13.2) than heterozygotes (96.4 ± 14.1, p = 0.007) or LL homozygotes for the T allele (97.2 ± 14.2, p = 0.041). Adjusted QUS-SI means for the -509 SNP, after correction for age, caffeine intake and BMI (means of 27.5 years, 1.54 cups/day and 23.2 kg/m2, respectively), were: CC 93.6 ± 1.0, CT 95.0 ± 1.0, and TT 98.7 ± 1.9. For codon 10, adjusted means were: LL 94.8 ± 1.1, LP 93.7 ± 1.0 and PP 98.3 ± 1.5. For SNP 713-8delC, only 18 heterozygotes were found and no significant difference in QUS-SI means was observed (data not shown).

Mean right heel ultrasound stiffness for -509 and codon10 genotypes. Error bars represent standard error of means. P-values were obtained by Scheffé correction for multiple testing after routine ANOVA.
Multivariate analysis
Based on the model previously reported by Rubin et al. [4], the seven TGFB1 genotypes were each introduced as single additive variables (variant allele counted as 0, 1 or 2) to the original multivariate analysis to test for significance. The LS BMD model included the following clinical variables: weight, physical activity at time of study, and physical activity during adolescence, age, paternal history of osteoporosis, family history of osteoporosis, and past amenorrhea greater than 3 months. None of the TGFB1 SNPs were significant predictors of LS BMD, nor were results significant for femoral neck (data not shown).
In a previously reported model from our laboratory on this group of Caucasian females the estrogen receptor (ER1) SNPs were examined [6]. ER1 Xba I, Pvu II restriction haplotypes and AIB1 genotypes were interactively significant in that model, which included the following clinical covariates: age, physical activity at the time of the study and physical activity in adolescent years, caffeine consumption, and BMI. When -509 and codon 10 SNPs were added as new variables to the clinical covariates model, they remained significant (Table 5). Thus, the -509 and codon 10 SNPs appear to make significant independent contributions to the explained variance of QUS-SI.
Discussion
TGF-β1 is a secreted factor that plays an important role in bone remodelling. It is a potent stimulator of osteoblastic bone formation, causing chemotaxis, proliferation and differentiation in committed osteoblasts [11]. Although in vitro experiments have led to conflicting reports about the effects of exogenous TGF-β1 in cultured osteoblast systems [32, 33], secreted TGF-β1 leads to matrix growth and osteoblast stimulation in vivo, while it inhibits mineralization, osteoclast differentiation and the resorptive activity of mature osteoclasts [34, 35]. Mouse knockouts for TGFB1 have skeletal defects, including shortened long bones and decreased tibial BMD. In humans, however, mutations found in the pro-peptide of TGFB1 are associated with Camurati-Engelman Disease (CED), an autosomal dominant disorder manifesting as periosteal and endosteal thickening of the long bone diaphyses [12, 13]. Most of these mutations lie in the Latent Associated Peptide (LAP) that is cleaved from the mature TGF-β1 peptide. LAP subsequently binds to mature TGF-β1 to form an inactivated secretory complex. Presumably, mutations that interfere with binding of LAP to the mature peptide would lead to increased TGF-β1 activation, stimulating bone remodelling, net bone deposition, and resulting in a denser skeleton.
In our cohort, allele frequencies for the -800, -509, codon 10, codon 25 and codon 263 SNPs are in agreement with those published by Cambien et al. [16], and Syrris et al. [36], who examined French, Irish and UK populations. Allele frequencies in our cohort for 713-8delC and C861-20T, respectively, are comparable to those in the European Caucasians studied by Langdahl et al. and by Keen et al. [17, 18]. Of the 7 SNPs examined for linkage, 713-8delC was in complete negative LD with codon 25 and codon 263. The 713-8delC SNP was in strong negative LD with -509 (Δ' = -0.77) and codon 10 (Δ' = -0.80), suggesting a single haplotype. Moreover, disequilibrium coefficients in our population were comparable to those reported by Cambien et al [16].
The two SNPs in the promoter, G-800A and C-509T, may theoretically alter the binding of RNA polymerase or other transcription factors. Luedecking et al. found that the transcriptional activity of the -509T variant allele of the TGFB1 gene was slightly greater than that of the common C allele [37]. Serum TGF-β1 concentrations are increased in a gene dose-dependent fashion, with differences in concentrations in TT homozygotes being twice that of TC individuals, when the CC genotype is taken as the referent [19]. Our results for the -509 polymorphism are consistent with this view that the T allele (high TGF-β1 producer) is associated with increased bone formation in young women, since heel QUS-SI is increased in rough proportion to the number of T alleles present. Langdahl reported a similar finding in a healthy Danish middle aged cohort, in whom higher FN BMD was associated with TT genotype [25]. In the Japanese population, however, the -509 CC genotype has been found associated with higher BMD [21]. This difference may be due to background genetic differences in the populations, ascertainment differences affecting the TGF-β1 genotype distribution in the sample set, or environmental factors. Differences in linkage disequilibrium may also contribute to this discordance, and shed light on parallel differences with codon 10 associations. In some studies, the 10Pro allele is associated with increased BMD [21, 25], but not in others [20, 22, 23].
The TGFB1 codon 10 and 25 polymorphisms are located in the signal sequence, which is cleaved from the TGF-β1 precursor at codon 29 (Gly29-Leu30 peptide bond). In general, signal sequence mutations affect peptide export efficiency [38]. The replacement of leucine by proline at position 10 would be expected to disrupt the alpha-helical domain, while replacement of arginine by proline at position 25 would change the characteristic polarity of the carboxyl domain of the signal sequence. In either case, altered signal peptide regulation leading to differential trafficking or export would be the likely mechanism underlying genotype-dependent differences in TGF-β1 metabolism.
The physiologic evidence for such differential expression is not extensive. Awad et al. reported a significant correlation between codon 25 genotype and amounts of TGF-β1 secreted by cultured lymphocytes stimulated in vitro [39]. Significant association of the codon 10 genotype with plasma TGF-β1 concentrations, BMD at lumbar spine, and vertebral fracture frequency, has been reported in controls and 2 different Japanese populations of osteoporotic patients [40]. In both control and osteoporotic groups, the association with higher plasma TGF-β1 and the 10P allele was roughly additive [9]. In a study of Japanese adolescents, those homozygous for the 10P genotype had significantly higher BMD than those homozygous for the L10 allele [27]. These results suggest that increased skeletal mineralization during puberty may be related to the presence of a 10P allele. Our study of Caucasian pre-menopausal women found no difference in BMD at either FN or LS, but found a positive association between the Leu10 allele and calcaneal QUS-SI.
Of the remaining SNPs, Langdahl et al. reported that the 713-8delC was more frequent in osteoporotic women (6/123), than controls (2/131) but no correlation to bone mass was demonstrated in the controls [25]. It is possible that linkage of this SNP with other functional sites provides an explanation for variable but genuine association with parameters of bone strength and mineral density. Indeed, we observed that the 713-8delC is in negative disequilibrium with codon 10 and -509 (Δ' = -0.77 and -0.80, respectively) in our population. Thus, previous positive results with this genotype alone may represent association with a haplotype extending across all 3 loci.
None of the TGFB1 SNPs in this study was significantly associated with either spine or hip BMD. Although apparently negative in contrast to other studies, our findings may be explained in part by the demographic characteristics of our cohort. Ours was a population of healthy young adults, whereas previous research showing an association with codon 10 and 713-8delC was based on post-menopausal women diagnosed with osteoporosis [25]. It is generally understood that studies of post-menopausal women are predominantly investigations of the rate of bone loss, whereas those in young adults are identifying genetic determinants of peak bone mass accumulation. While BMD is a measure of the density of the mineralized bone, QUS-SI is a measure of bone architecture as well [41].
The skeletal site examined for bone mass and bone quality is important. Modelling of data in twins has indicated that there are both common and specific genetic factors acting on bone at different skeletal sites and on different aspects on bone quality [42, 43]. Our study suggests that TGFB1 genetic variation does not seem to be a major factor in total bone mineralization per se, at least as measured by BMD at the hip and femur.
Significant linkage disequilibrium exists between -509 and codon10 alleles and the results in our cohort (Δ' = 0.88) are no exception. However, the LD is not complete, and it is therefore no surprise that both -509 and codon 10 show association to QUS-SI, even when entered as independent variables in the multiple regression analysis. When means are compared for each genotype at a single locus, only the -509 genotypes showed a gene dosage effect, much as Yamada et al. described in a cohort of Japanese adolescents [27]. Evidence indicates that the T allele of -509 may be the more important SNP leading to an increase rate of transcription, which in turn affects bone mass. For our cohort, the multiple regression model for QUS-SI, as the dependent variable, adjusted for clinical covariates (age, height, weight, BMI, caffeine and calcium intake) and therefore these factors are likely confounders of the genotype effects seen.
Our findings must be interpreted in the context of several potential limitations. Our Caucasian cohort was recruited from an ethnically diverse urban population and admixture effects cannot be excluded. Only women were recruited, and we cannot say whether a similar association would be observed in men. Recruitment was conducted by public advertisement, and there may be significant bias toward those believing they were at higher risk for a bone related disease, particularly because of family history. However, the parameters for LS and FN BMD and for QUS-SI are comparable to other cohorts of healthy young women [4], and the associations we describe are independent of family history in our multiple regression model.
Common variations in DNA sequence are often associated with mild phenotypic effects [44]. Thus even a single SNP could account for a significant variation in bone mass so as to potentially influence subsequent fracture risk. However, the contribution of genotypes determined by all intragenic loci within a gene must be evaluated with environmental factors, in order to generate a balanced picture of gene-environment interactions for a complex quantitative trait like peak bone mass.
References
Pocock NA, Eisman JA, Hopper JL, Yeates MG, Sambrook PN, Eberl S: Genetic determinants of bone mass in adults. A twin study. J Clin Invest. 1987, 80: 706-710.
Patel MS, Rubin LA, Cole DE: Genetic determinants of peak bone mass. The Osteoporosis Primer. Edited by: Henderson JE, Goltzman D. 2000, Cambridge: Cambridge University Press, 131-146.
Morrison NA, Qi JC, Tokita A, Kelly PJ, Crofts L, Nguyen TV, Sambrook PN, Eisman JA: Prediction of bone density from vitamin D receptor alleles. Nature. 1994, 367: 284-287. 10.1038/367284a0.
Rubin LA, Hawker GA, Peltekova VD, Fielding LJ, Ridout R, Cole DE: Determinants of peak bone mass: clinical and genetic analyses in a young female Canadian cohort. J Bone Miner Res. 1999, 14: 633-643.
Kobayashi S, Inoue S, Hosoi T, Ouchi Y, Shiraki M, Orimo H: Association of bone mineral density with polymorphism of the estrogen receptor gene. J Bone Miner Res. 1996, 11: 306-311.
Patel MS, Cole DE, Smith JD, Hawker GA, Wong B, Trang H, Vieth R, Meltzer P, Rubin LA: Alleles of the estrogen receptor alpha-gene and an estrogen receptor cotranscriptional activator gene, amplified in breast cancer-1 (AIB1), are associated with quantitative calcaneal ultrasound. J Bone Miner Res. 2000, 15: 2231-2239.
Grant SF, Reid DM, Blake G, Herd R, Fogelman I, Ralston SH: Reduced bone density and osteoporosis associated with a polymorphic Sp1 binding site in the collagen type I alpha 1 gene. Nat Genet. 1996, 14: 203-205. 10.1038/ng1096-203.
Shiraki M, Shiraki Y, Aoki C, Hosoi T, Inoue S, Kaneki M, Ouchi Y: Association of bone mineral density with apolipoprotein E phenotype. J Bone Miner Res. 1997, 12: 1438-1445.
Yamada Y, Miyauchi A, Goto J, Takagi Y, Okuizumi H, Kanematsu M, Hase M, Takai H, Harada A, Ikeda K: Association of a polymorphism of the transforming growth factor-beta1 gene with genetic susceptibility to osteoporosis in postmenopausal Japanese women. J Bone Miner Res. 1998, 13: 1569-1576.
Seyedin SM, Thompson AY, Bentz H, Rosen DM, McPherson JM, Conti A, Siegel NR, Galluppi GR, Piez KA: Cartilage-inducing factor-A. Apparent identity to transforming growth factor-beta. J Biol Chem. 1986, 261: 5693-5695.
Cohen MM: TGF beta/Smad signaling system and its pathologic correlates. Am J Med Genet A. 2003, 116: 1-10. 10.1002/ajmg.a.10750.
Janssens K, Gershoni-Baruch R, Guanabens N, Migone N, Ralston S, Bonduelle M, Lissens W, Van ML, Vanhoenacker F, Verbruggen L: Mutations in the gene encoding the latency-associated peptide of TGF-beta 1 cause Camurati-Engelmann disease. Nat Genet. 2000, 26: 273-275. 10.1038/81563.
Kinoshita A, Fukumaki Y, Shirahama S, Miyahara A, Nishimura G, Haga N, Namba A, Ueda H, Hayashi H, Ikegawa S: TGFB1 mutations in four new families with Camurati-Engelmann disease: confirmation of independently arising LAP-domain-specific mutations. Am J Med Genet A. 2004, 127: 104-107. 10.1002/ajmg.a.20671.
Dickson MC, Martin JS, Cousins FM, Kulkarni AB, Karlsson S, Akhurst RJ: Defective hematopoiesis and vasculogenesis in transforming growth-factor-beta-1 knock out mice. Development. 1995, 121: 1845-1854.
Derynck R, Jarrett JA, Chen EY, Goeddel DV: The murine transforming growth factor-beta precursor. J Biol Chem. 1986, 261: 4377-4379.
Cambien F, Ricard S, Troesch A, Mallet C, Generenaz L, Evans A, Arveiler D, Luc G, Ruidavets JB, Poirier O: Polymorphisms of the transforming growth factor-beta 1 gene in relation to myocardial infarction and blood pressure. The Etude Cas-Temoin de l'Infarctus du Myocarde (ECTIM) Study. Hypertension. 1996, 28: 881-887.
Langdahl BL, Knudsen JY, Jensen HK, Gregersen N, Eriksen EF: A sequence variation: 713-8delC in the transforming growth factor-beta 1 gene has higher prevalence in osteoporotic women than in normal women and is associated with very low bone mass in osteoporotic women and increased bone turnover in both osteoporotic and normal women. Bone. 1997, 20: 289-294. 10.1016/S8756-3282(96)00363-8.
Keen RW, Snieder H, Molloy H, Daniels J, Chiano M, Gibson F, Fairbairn L, Smith P, MacGregor AJ, Gewert D: Evidence of association and linkage disequilibrium between a novel polymorphism in the transforming growth factor beta 1 gene and hip bone mineral density: a study of female twins. Rheumatology (Oxford). 2001, 40: 48-54. 10.1093/rheumatology/40.1.48.
Grainger DJ, Heathcote K, Chiano M, Snieder H, Kemp PR, Metcalfe JC, Carter ND, Spector TD: Genetic control of the circulating concentration of transforming growth factor type beta1. Hum Mol Genet. 1999, 8: 93-97. 10.1093/hmg/8.1.93.
Lau HH, Ho AY, Luk KD, Kung AW: Transforming growth factor-beta1 gene polymorphisms and bone turnover, bone mineral density and fracture risk in southern chinese women. Calcif Tissue Int. 2004, 74: 516-521. 10.1007/s00223-004-0163-4.
Yamada Y, Miyauchi A, Takagi Y, Tanaka M, Mizuno M, Harada A: Association of the C-509-->T polymorphism, alone of in combination with the T869-->C polymorphism, of the transforming growth factor-beta1 gene with bone mineral density and genetic susceptibility to osteoporosis in Japanese women. J Mol Med. 2001, 79: 149-156. 10.1007/s001090100190.
Hinke V, Seck T, Clanget C, Scheidt-Nave C, Ziegler R, Pfeilschifter J: Association of transforming growth factor-beta1 (TGFbeta1) T29 -> C gene polymorphism with bone mineral density (BMD), changes in BMD, and serum concentrations of TGF-beta1 in a population-based sample of postmenopausal german women. Calcif Tissue Int. 2001, 69: 315-320. 10.1007/s002230020024.
Dick IM, Devine A, Li S, Dhaliwal SS, Prince RL: The T869C TGF beta polymorphism is associated with fracture, bone mineral density, and calcaneal quantitative ultrasound in elderly women. Bone. 2003, 33: 335-341. 10.1016/S8756-3282(03)00158-3.
Bertoldo F, D'Agruma L, Furlan F, Colapietro F, Lorenzi MT, Maiorano N, Iolascon A, Zelante L, Locascio V, Gasparini P: Transforming growth factor-beta1 gene polymorphism, bone turnover, and bone mass in Italian postmenopausal women. J Bone Miner Res. 2000, 15: 634-639.
Langdahl BL, Carstens M, Stenkjaer L, Eriksen EF: Polymorphisms in the transforming growth factor beta 1 gene and osteoporosis. Bone. 2003, 32: 297-310. 10.1016/S8756-3282(02)00971-7.
Ziv E, Kahn A, Cauley J, Morin P, Saiz R, Browner W: No association between the TGF-beta 1 Leu10Pro polymorphism and osteoporosis among white women in the United States. Am J Med. 2003, 114: 227-231. 10.1016/S0002-9343(02)01393-1.
Yamada Y, Hosoi T, Makimoto F, Tanaka H, Seino Y, Ikeda K: Transforming growth factor beta-1 gene polymorphism and bone mineral density in Japanese adolescents. Am J Med. 1999, 106: 477-479. 10.1016/S0002-9343(99)00043-1.
Sawitzke AD, Sawitzke AL, Ward RH: HLA-DPB typing using co-digestion of amplified fragments allows efficient identification of heterozygous genotypes. Tissue Antigens. 1992, 40: 175-181.
Peltekova VD, Cole DE, Pavlova A, Rubin LA: Improved method for direct haplotyping at the vitamin D receptor gene locus. Clin Biochem. 1998, 31: 191-194. 10.1016/S0009-9120(98)00005-8.
Weir BS: . Genetic Data Analysis II. 1996, Sunderland, Massachusetts: Sinauer Associates, Inc. Publishers
Hamilton DC, Cole DE: Standardizing a composite measure of linkage disequilibrium. Ann Hum Genet. 2004, 68: 234-239. 10.1046/j.1529-8817.2004.00056.x.
Pfeilschifter J, Seyedin SM, Mundy GR: Transforming growth factor beta inhibits bone resorption in fetal rat long bone cultures. J Clin Invest. 1988, 82: 680-685.
Fuller K, Lean JM, Bayley KE, Wani MR, Chambers TJ: A role for TGFbeta(1) in osteoclast differentiation and survival. J Cell Sci. 2000, 113 (Pt 13): 2445-2453.
Antosz ME, Bellows CG, Aubin JE: Effects of transforming growth factor beta and epidermal growth factor on cell proliferation and the formation of bone nodules in isolated fetal rat calvaria cells. J Cell Physiol. 1989, 140: 386-395. 10.1002/jcp.1041400225.
Dieudonne SC, Semeins CM, Goei SW, Vukicevic S, Nulend JK, Sampath TK, Helder M, Burger EH: Opposite effects of osteogenic protein and transforming growth factor beta on chondrogenesis in cultured long bone rudiments. J Bone Miner Res. 1994, 9: 771-780.
Syrris P, Carter ND, Metcalfe JC, Kemp PR, Grainger DJ, Kaski JC, Crossman DC, Francis SE, Gunn J, Jeffery S: Transforming growth factor-beta1 gene polymorphisms and coronary artery disease. Clin Sci. 1998, 95: 659-667. 10.1042/CS19980154.
Luedecking EK, DeKosky ST, Mehdi H, Ganguli M, Kamboh MI: Analysis of genetic polymorphisms in the transforming growth factor-beta1 gene and the risk of Alzheimer's disease. Hum Genet. 2000, 106: 565-569. 10.1007/s004390050026.
Walter P, Johnson AE: Signal sequence recognition and protein targeting to the endoplasmic reticulum membrane. Annu Rev Cell Biol. 1994, 10: 87-119. 10.1146/annurev.cb.10.110194.000511.
Awad MR, El Gamel A, Hasleton P, Turner DM, Sinnott PJ, Hutchinson IV: Genotypic variation in the transforming growth factor-beta1 gene: association with transforming growth factor-beta1 production, fibrotic lung disease, and graft fibrosis after lung transplantation. Transplantation. 1998, 66: 1014-1020. 10.1097/00007890-199810270-00009.
Yamada Y: Association of polymorphisms of the transforming growth factor-beta1 gene with genetic susceptibility to osteoporosis. Pharmacogenetics. 2001, 11: 765-771. 10.1097/00008571-200112000-00004.
Njeh CF, Boivin CM, Langton CM: The role of ultrasound in the assessment of osteoporosis: a review. Osteoporos Int. 1997, 7: 7-22. 10.1007/BF01623454.
Howard GM, Nguyen TV, Harris M, Kelly PJ, Eisman JA: Genetic and environmental contributions to the association between quantitative ultrasound and bone mineral density measurements: a twin study. J Bone Miner Res. 1998, 13: 1318-1327.
Beamer WG, Donahue LR, Rosen CJ, Baylink DJ: Genetic variability in adult bone density among inbred strains of mice. Bone. 1996, 18: 397-403. 10.1016/8756-3282(96)00047-6.
Chakravarti A: Population genetics--making sense out of sequence. Nat Genet. 1999, 21: 56-60. 10.1038/4482.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/6/29/prepub
Acknowledgements
This work was supported by an IOC Partnership Grant from the National Science and Engineering Research Council and Dairy Farmers of Canada.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
PT carried out genetic tests, analysed data and drafted the manuscript.
DC conceived the study, and supervised the study design, statistical analysis, and drafting of manuscript
BW was involved in the design of the genotyping assays and sample preparation
AL was involved in study design and interpretation of the data
LR was involved in recruitment of study population, acquisition of samples, and auditing of the clinical database
All authors read and approved the final manuscript
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Tzakas, P., Wong, B.Y., Logan, A.G. et al. Transforming growth factor beta-1 (TGFB1) and peak bone mass: association between intragenic polymorphisms and quantitative ultrasound of the heel. BMC Musculoskelet Disord 6, 29 (2005). https://doi.org/10.1186/1471-2474-6-29
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2474-6-29