
Abstract
Background
The Neck Disability Index (NDI) is the most commonly used outcome measure for neck pain. This study aimed to determine the psychometric properties of a German version of the NDI. Cross-cultural translation and psychometric testing of the NDI were performed.
Methods
The 10-item NDI was translated into German and administered to 558 patients with chronic unspecific neck pain (Mean age 49.9 ± 11.4 years, 76% female). The factor structure and reliability of the NDI were assessed using factor analysis, Cronbach’s alpha, split-half reliability (Spearman-Brown coefficient), and intra-class correlation (ICC2,1). To determine convergent validity, pain intensity (visual analog scale; VAS), pain on movement (VAS), and quality of life (Short Form 36 Health Survey Questionnaire; SF-36) were correlated with the NDI. Correlation with range of motion and sensitivity to change were also assessed in a subsample of 49 patients.
Results
The mean NDI score was 32.75 ± 13.09. Factor analysis revealed a single factor that explained 39.8% of the variance. Cronbach’s alpha was 0.81; Spearman-Brown coefficient was 0.80; and intra-class correlation was 0.81 (95% confidence interval = 0.78, 0.83). Significant correlations were found for pain intensity (r = 0.22, p < 0.01), pain on movement (r = 0.39, p < 0.01), quality of life (r = -0.30 to -0.45, p < 0.01), and range of motion (r = -0.34, p = 0.02). Patients who reported global improvement of health after an exercise or yoga intervention showed a higher decrease on the NDI than patients who reported no global improvement (p < 0.01).
Conclusions
The German version of the NDI has a comparable factor structure as the original version, acceptable psychometric properties, and is sensitive to change after physical activity. Neck disability is associated with other measures of neck pain.
Similar content being viewed by others

Background
With a mean lifetime prevalence of about 50%, neck pain is a major public health problem in all industrialized countries[1]. Despite its often unclear physiological correlates and episodic nature, neck pain is often associated with marked disability: more than 10% of work absenteeism is at least somehow associated with neck pain[2], and about 5% of adults report significantly disabling neck pain[3]. Therefore, the assessment of neck pain and its progression is mostly based on patient-based outcome measures, mainly pain intensity and disability[4]. The Neck Disability Index is probably the most commonly used and best validated instrument for assessing disability in patients with neck pain[5]. Originally based on the Oswestry Low Back Pain Index, the Neck Disability Index assesses neck-related disability on 10 items[6]. The internal consistency generally is reported to be high for both the original[6] and translated versions of the instrument[7–11]. While most validation studies have replicated the original single factor structure[7, 9], other studies found a better fit of the data with a two factor solution[10, 11]. The validity of the Neck Disability Index has also been demonstrated for a number of translations and cross-cultural adaptations including the Japanese, Portuguese, Spanish, and Swedish version[12]. However, the only available German version of the instrument[13] has been criticized for the extremely small sample size in its validation study that strongly limits the usefulness of this version[14].
Therefore, this analysis of 558 patients suffering from chronic non-specific neck pain aimed to determine reliability and validity of a German version of the Neck Disability Index.
Methods
Subjects
Patients from 10 randomized controlled trials on chronic non-specific neck pain were included in psychometric testing. The trials had been conducted at the Department of Complementary and Integrative Medicine, Kliniken Essen-Mitte, Germany[15–22] and at the Immanuel Hospital Berlin, Department of Internal and Integrative Medicine, Berlin, Germany[23, 24]. All studies were conducted in accordance with the ethical standards of the responsible institutional committee on human experimentation and with the Helsinki Declaration of 1975, as revised in 1983. All studies were approved by the institutional ethics committee of the medical institutions at the University of Duisburg-Essen, Germany[15–22] or by the Ethics Committee of the Charité-University Medical Center, Berlin, Germany[23, 24] prior to patient recruitment and all patients gave written informed consent prior to inclusion in the study.
To be included, adult patients of both genders had to suffer from chronic non-specific neck pain for at least 5 days a week for at least 12 consecutive weeks with a mean pain intensity of at least 40 mm on a 100 mm visual analog scale (VAS) from 0 mm (no pain) to 100 mm (worst pain imaginable). Patients with neck pain that was likely to result from specific causes such as neck trauma, disc protrusion, rheumatic diseases, spinal canal stenosis, or neoplasms as well as patients with serious physical or mental comorbidities such as active oncologic diseases, diabetes mellitus, coronary artery disease, affective disorders, addiction, or psychosis were excluded.
Sample description
The psychometric sample consisted of 558 patients of which 134 (24.0%) were male and 424 (76.0%) were female. Age ranged from 19 to 81 years with a mean age 49.9 ± 11.4 years. The mean pain intensity was 45.7 mm ± 20.8 mm on a VAS; mean pain duration was 7.54 ± 7.52 years (Table 1).
Measures
Neck-specific disability
As a measure of neck-specific functional disability, a translated version of the original 10-item Neck Disability Index (NDI) was used[6]. The NDI covers 10 dimensions of neck-specific disability, namely pain intensity, personal care, lifting, reading, headache, concentration, work, driving, sleeping, and recreation[6]. Each dimension is assessed with 1 item, measured on a 6-point scale from 0 (no disability) to 5 (full disability). The sum score out of all 10 items is multiplied by 2 to obtain a score out of 100%[12]. The instrument was translated into German independently by 2 German native speakers with intensive English language training and knowledge of the English-speaking culture. Both translators were health professionals and experienced in assessing questionnaire and interview data. The translation aimed at a conceptual equivalent of the item rather than a word-for-word translation. Both translations were combined by the translators into a single consensus translation by discussion. The instrument was then back-translated into English by 2 independent professional translators who had no knowledge of the original instrument and had no health back ground. Again, a single back-translation was produced by discussion until consensus was reached. Concordance of the back-translated version and the original NDI was approved by the senior author (AM). The final German version of the NDI is given in Additional file1.
Neck pain intensity
Mean neck pain intensity during the past 7 days was measured on a 100-mm VAS[25].
Pain on movement
Pain on movement was assessed for 6 consecutive head movements (flexion, extension, lateral flexion left/right, rotation left/right). The pain elicited by each of these movements was scored on a 100-mm VAS[18].
Health-related quality of life
Health-related quality of life was assessed using the Short Form 36 Health Survey Questionnaire (SF-36)[26]. This comprehensive 36-item questionnaire yields an 8-scale health profile as well as two component summaries of physical and mental health-related quality of life.
Cervical range of motion
In a subsample of 49 patients, cervical range of motion was measured for 6 cervical movement directions (flexion, extension, lateral flexion left/right, rotation left/right) using an electromagnetic, motion-tracking device (Fastrak, Polhemus, Colchester, USA)[19, 27]. A small sensor was attached to the forehead using a Velcro strap and movements of this sensor were converted to Euler angles. Patients were asked to move their head as far as possible at a comfortable speed. Three trials for each movement direction were performed and averaged.
Statistical analysis
Construct validity
Given that prior cross-cultural adaptations of the NDI had revealed either single factor or two factor solutions, no a priori assumptions about the underlying factor structure of the German NDI were made and an exploratory factor analysis using the principle components extraction and the varimax rotation was performed on the 10 items of the NDI to explore the instrument’s structure. Factors were extracted if their eigenvalue was >1. Domain scores of any resulting factors, or of a total score, were calculated as a sum of the component item scores. A major requirement for factor analysis is a considerably large subject:item ratio. A minimum ratio of 20:1 has been proposed to ensure strong factor structures are replicated reliably[28]. This requirement was met by the subject:item ratio of 1:55.8 in this analysis.
Reliability
To assess internal consistency of the NDI, Cronbach’s α, alpha if item deleted, item-scale correlations, and item difficulty were calculated. Split-half reliability was assessed as the Spearman-Brown coefficient for the first 5 items (pain intensity, personal care, lifting, reading, headache) and the last 5 items (concentration, work, driving, sleeping, and recreation). Two-way random intra-class correlation (ICC2,1) and its 95% confidence interval (CI) was used to assess agreement between measures.
Convergent validity
As a measure of convergent validity, the strength of relationship of the NDI with theoretically related instruments for neck pain patients was assessed. Spearman’s correlation coefficients between the NDI, pain intensity, pain on movement, and the component summaries and subscales of the SF-36 were calculated. Correlation coefficient was further calculated for range of motion in a subsample of 49 patients.
Responsiveness
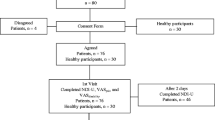
Sensitivity to change was calculated in a subsample of 49 patients. After the first assessment, those patients participated in a 9-week exercise or yoga intervention. The intervention consisted of 15 minutes of self-directed daily home practice based on manualized instructions and (for the yoga intervention) weekly 90-minute classes with a certified instructor[19]. After the intervention, the assessment was repeated. Additionally, global improvement was assessed on a 5-point Likert-type scale ranging from "my health is much better" to "my health is much worse" and patients were divided into two groups comprising those with stable vs. those with improved health. NDI change scores between the two groups were compared using an unpaired t-test.
All statistics were performed using the statistical package IBM SPSS Statistics (Version 20.0; IBM Inc., New York, USA). A p-value of <0.05 (two-tailed) was considered significant in all analyses.
Results
Descriptive scale characteristics
Mean item values ranged from 0.45 to 2.24 (Table 2). For all item but "personal care", the whole 0–5 range of the item was scored by at least 1 patient. For "personal care", the highest score was 3 ("I need some help but can manage most of my personal care"); 99.3% of the patients scored 2 or lower. The total instrument had a mean of 32.75 with a standard deviation of 13.09, values ranged from 8.00 (n = 4, 0.7%) to 82.00 (n = 1; 0.2%).
Factor structure of the NDI
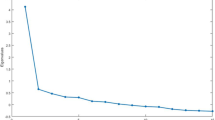
Kaiser-Meyer-Olkin’s measure of sampling adequacy was satisfactory with 0.89, indicating that the sample was suitable for factor analysis. Primary component factor analysis revealed a single factor structure which would explain 39.8% of the variance (Table 2). Factor loadings ranged from 0.484 to 0.755 (Table 2). While the item "headache" had a factor loading < 0.5, the removal of this item from the analysis did not change Cronbach’s α. Therefore, it was decided to retain the item in the instrument to ensure consistency with the original English language instrument.
Reliability
As a measure of internal consistency, Cronbach’s α was 0.81. For all items, deletion of the specific item would have reduced Cronbach’s α except for the item "headache" which deletion would not have changed alpha (Table 2). Corrected item total correlation ranged from 0.38 to 0.63; item difficulty ranged from 0.23 to 0.45 except for "personal care". "Personal care" had an item difficulty of 0.09 reflecting a generally low scoring. As the removal of this item from the analysis would have reduced Cronbach’s Alpha, it was decided to retain the item in the instrument. Testing for split-half reliability revealed a Spearman-Brown coefficient of 0.80. Intra-class correlation was ICC2,1 = 0.81, 95% CI = 0.78 to 0.83.
Convergent validity
Results of the correlation analyses to determine the convergent validity of the NDI are shown in Table 3. NDI was significantly correlated with all measures. Correlations effect sizes were moderate for all measures except for pain intensity and emotional role function whose correlations with NDI had small effect sizes.
Responsiveness
Patients who reported global improvement of health after exercise or yoga showed a decrease of 7.04 ± 6.33 on the NDI; patients who reported no global improvement had a decrease of 0.82 ± 8.25; the group difference was significant (p < 0.01).
Discussion
The German translation of the Neck Disability Index demonstrated a single factor structure with good internal consistency, intra-class correlation, and split-half reliability. The original English version was developed as a one-factor instrument[6]. The single factor solution has been supported in cross-cultural adaptations of Spanish[9], Brazilian/Portuguese[7], Greek[8], Finnish[29], and Turkish[30] translations. However, 2-factor structures were also found in a number of translated versions including the Italian[10], Polish[31], Arabic[32], and Japanese[11] versions. Recently, an alternative German version of the NDI has been validated in a total of 51 neck pain patients and healthy subjects[13]. While this validation study revealed a 2-factor solution, the interpretability of this analysis and hence the usefulness of the instrument is strongly limited by the extremely small sample size[14]. Compared to other versions of the Neck Disability Index, the explained variance of the single factor was relatively low in the German version reported here[12] but comparable to that of the Greek version[8]. Item-difficulty was relatively low for all items, especially for "personal care" that had not been scored higher than 3 out of 5 by any patient. More than a characteristic of the instrument, this might reflect a characteristic of the sample that reported only moderate pain intensity and relatively low disability despite the long duration neck pain. Strong disability in personal care might reflect a higher grade of general disability and have a higher impact on activities of daily living than e.g. disability in lifting. However, patients with Whiplash-associated disorder with more pronounced general disability have been shown to have higher personal care-related disability[33]. Despite the very low item difficulty of "personal care" and the low factor loading of "headache", removing these items would have reduced content validity of the instrument and make cross-cultural comparisons harder. Therefore, it was decided to retain the original 10-item structure.
Consistent with findings on other versions, the instrument was positively correlated with pain intensity and negatively with quality of life and neck range of motion[33–36]. This might reflect well-known associations between pain intensity, subjective disability, quality of life, and objective range of motion[37–39]. Interestingly, neck disability was associated not only with physical quality of life but also with all dimensions of mental quality of life. This is in line with earlier findings of correlation of the neck disability and mental health[40].
The instrument was sensitive to change after exercise or yoga interventions. Global impression of improved health was associated with improved neck disability. Several randomized trials have shown that exercise can improve global health and neck disability in chronic neck pain patients[41, 42]. This also seems to apply to yoga intervention[19, 23, 43]. The German version of the Neck Disability Index seems to be responsive to these improvements. Responsiveness of a German version of the NDI has also been assessed in another study[44]. This study concluded that responsiveness to change was lower in the NDI than in the Bournemouth Questionnaire for Neck Pain. However, it remains unclear whether a validated or unvalidated version of the NDI was used. Moreover, responsiveness was assessed differently in this study since the analysis was performed in students rather than neck pain patients and participants were not treated between repeated measurements.
This study has several limitations. First, the sample was not recruited specifically for the purpose of validating the Neck Disability Index but was drawn from a number of randomized trials. All available patients from the respective trials were included in the analysis. Thus, no a priori sample size calculation was performed. However, the achieved sample was considerably larger than that of most other cross-cultural adaptations of the NDI[7–9, 11, 32, 36, 40]. Secondly, the sample comprised mainly female patients with low to moderate disability due to chronic non-specific neck pain. The psychometric properties found in this analysis might therefore not be fully applicable to patients with more severe neck pain and/or Whiplash-associated disorder. However, despite its limitations, this study comprises a large homogeneous sample to evaluate the reliability and validity of the German version of the Neck Disability Index.
Conclusions
Comparable to the original English version, the German version of the Neck Disability Index demonstrated a single factor structure. The instrument has acceptable to good psychometric properties and is associated with other measures of health. The instrument further is sensitive to change after physical activity. As the original instrument, the German version of the Neck Disability Index seems to present a useful measure of neck disability in patients with chronic non-specific neck pain.
References
Fejer R, Kyvik KO, Hartvigsen J: The prevalence of neck pain in the world population: a systematic critical review of the literature. Eur Spine J. 2006, 15 (6): 834-848. 10.1007/s00586-004-0864-4.
Cote P, van der Velde G, Cassidy JD, Carroll LJ, Hogg-Johnson S, Holm LW, Carragee EJ, Haldeman S, Nordin M, Hurwitz EL, Guzman J, Peloso PM, Bone and Joint Decade 2000-2010 Task Force on Neck Pain and Its Associated Disorders: The burden and determinants of neck pain in workers: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. Spine (Phila Pa 1976). 2008, 33 (4 Suppl): S60-S74.
Cote P, Cassidy JD, Carroll L: The Saskatchewan Health and Back Pain Survey. The prevalence of neck pain and related disability in Saskatchewan adults. Spine (Phila Pa 1976). 1998, 23 (15): 1689-1698. 10.1097/00007632-199808010-00015.
Deyo RA, Battie M, Beurskens AJ, Bombardier C, Croft P, Koes B, Malmivaara A, Roland M, Von Korff M, Waddell G: Outcome measures for low back pain research. A proposal for standardized use. Spine (Phila Pa 1976). 1998, 23 (18): 2003-2013. 10.1097/00007632-199809150-00018.
Vernon H: The Neck Disability Index: state-of-the-art, 1991–2008. J Manipulative Physiol Ther. 2008, 31 (7): 491-502. 10.1016/j.jmpt.2008.08.006.
Vernon H, Mior S: The Neck Disability Index: a study of reliability and validity. J Manipulative Physiol Ther. 1991, 14 (7): 409-415.
Cook C, Richardson JK, Braga L, Menezes A, Soler X, Kume P, Zaninelli M, Socolows F, Pietrobon R: Cross-cultural adaptation and validation of the Brazilian Portuguese version of the Neck Disability Index and Neck Pain and Disability Scale. Spine (Phila Pa 1976). 2006, 31 (14): 1621-1627. 10.1097/01.brs.0000221989.53069.16.
Trouli MN, Vernon HT, Kakavelakis KN, Antonopoulou MD, Paganas AN, Lionis CD: Translation of the Neck Disability Index and validation of the Greek version in a sample of neck pain patients. BMC Musculoskelet Disord. 2008, 9: 106-10.1186/1471-2474-9-106.
Andrade Ortega JA, Delgado Martinez AD, Almecija Ruiz R: Validation of the Spanish version of the Neck Disability Index. Spine (Phila Pa 1976). 2010, 35 (4): E114-E118. 10.1097/BRS.0b013e3181afea5d.
Marchese C, Cristalli G, Pichi B, Manciocco V, Mercante G, Pellini R, Marchesi P, Sperduti I, Ruscito P, Spriano G: Italian cross-cultural adaptation and validation of three different scales for the evaluation of shoulder pain and dysfunction after neck dissection: University of California - Los Angeles (UCLA) Shoulder Scale, Shoulder Pain and Disability Index (SPADI) and Simple Shoulder Test (SST). Acta Otorhinolaryngol Ital. 2012, 32 (1): 12-17.
Nakamaru K, Vernon H, Aizawa J, Koyama T, Nitta O: Crosscultural adaptation, reliability, and validity of the Japanese version of the neck disability index. Spine (Phila Pa 1976). 2012, 37 (21): E1343-E1347. 10.1097/BRS.0b013e318267f7f5.
MacDermid JC, Walton DM, Avery S, Blanchard A, Etruw E, McAlpine C, Goldsmith CH: Measurement properties of the neck disability index: a systematic review. J Orthop Sports Phys Ther. 2009, 39 (5): 400-417. 10.2519/jospt.2009.2930.
Swanenburg J, Humphreys K, Langenfeld A, Brunner F, Wirth B: Validity and reliability of a German version of the Neck Disability Index (NDI-G). Man Ther. 2014, 19 (1): 52-58. 10.1016/j.math.2013.07.004.
Gabel CP, Cuesta-Vargas A, Osborne JW, Melloh M: Commentary on the article by Swanenburg et al. 'Validity and reliability of a German version of the Neck Disability Index (NDI-G)’. Man Ther. 2014, 19 (1): e1-e2. 10.1016/j.math.2013.10.007.
Schuth M, Schwickert M, Lüdtke R, Lauche R, Choi KE, Musial F, Michalsen A: [Randomized controlled trial of the efficacy of the F.M. Alexander technique for chronic neck pain - a pilot study]. Yearbook of the Karl and Veronica Carstens-Foundation, no 16 (2009). Edited by: Albrecht H, Frühwald M. 2010, Essen: KVC Verlag, 103-118.
Braun M, Schwickert M, Nielsen A, Brunnhuber S, Dobos G, Musial F, Ludtke R, Michalsen A: Effectiveness of traditional Chinese "gua sha" therapy in patients with chronic neck pain: a randomized controlled trial. Pain Med. 2011, 12 (3): 362-369. 10.1111/j.1526-4637.2011.01053.x.
Cramer H, Baumgarten C, Choi KE, Lauche R, Saha F, Musial F, Dobos G: Thermotherapy self-treatment for neck pain relief - a randomized controlled trial. Eur J Integr Med. 2012, 4 (4): e371-e378. 10.1016/j.eujim.2012.04.001.
Cramer H, Lauche R, Hohmann C, Choi KE, Rampp T, Musial F, Langhorst J, Dobos G: Randomized controlled trial of pulsating cupping (pneumatic pulsation therapy) for chronic neck pain. Forsch Komplementmed. 2011, 18 (6): 327-334. 10.1159/000335294.
Cramer H, Lauche R, Hohmann C, Ludtke R, Haller H, Michalsen A, Langhorst J, Dobos G: Randomized-controlled trial comparing yoga and home-based exercise for chronic neck pain. Clin J Pain. 2013, 29 (3): 216-223. 10.1097/AJP.0b013e318251026c.
Lauche R, Cramer H, Choi KE, Rampp T, Saha FJ, Dobos GJ, Musial F: The influence of a series of five dry cupping treatments on pain and mechanical thresholds in patients with chronic non-specific neck pain–a randomised controlled pilot study. BMC Complement Altern Med. 2011, 11: 63-10.1186/1472-6882-11-63.
Lauche R, Cramer H, Hohmann C, Choi KE, Rampp T, Saha FJ, Musial F, Langhorst J, Dobos G: The effect of traditional cupping on pain and mechanical thresholds in patients with chronic nonspecific neck pain: a randomised controlled pilot study. Evid Based Complement Alternat Med. 2012, 2012: 429718-
Schumann S, Lauche R, Irmisch G, Hohmann C, Rolke R, Saha F, Cramer H, Choi KE, Langhorst J, Rampp T, Dobos G, Musial F: The effects of 5 sessions of cupping massage on chronic non-specific neck pain: a randomized controlled pilot study. BMC Complement Altern Med. 2012, 12 (Supplement 1): 80-
Michalsen A, Traitteur H, Ludtke R, Brunnhuber S, Meier L, Jeitler M, Bussing A, Kessler C: Yoga for chronic neck pain: a pilot randomized controlled clinical trial. J Pain. 2012, 13 (11): 1122-1130. 10.1016/j.jpain.2012.08.004.
Michalsen A: [Randomized-controlled trial on the effectiveness of meditation for chronic neck pain]. German Clinical Trials Registry. Available:https://drks-neu.uniklinik-freiburg.de/drks_web/navigate.do?navigationId=trial.HTML&TRIAL_ID=DRKS00000460 Assessed: 08 May 2013 2010,
Tiplady B, Jackson SH, Maskrey VM, Swift CG: Validity and sensitivity of visual analogue scales in young and older healthy subjects. Age Ageing. 1998, 27 (1): 63-66. 10.1093/ageing/27.1.63.
Bullinger M, Kirchberger I: SF-36. Health Survey. Manual. 1998, Göttingen, Germany: Hogrefe
Jordan K, Haywood KL, Dziedzic K, Garratt AM, Jones PW, Ong BN, Dawes PT: Assessment of the 3-dimensional Fastrak measurement system in measuring range of motion in ankylosing spondylitis. J Rheumatol. 2004, 31 (11): 2207-2215.
Costello AB, Osborne J: Best practices in exploratory factor analysis: four recommendations for getting the most from your analysis. Pract Assess Res Eval. 2005, 10 (7): 1-9.
Salo P, Ylinen J, Kautiainen H, Arkela-Kautiainen M, Hakkinen A: Reliability and validity of the finnish version of the neck disability index and the modified neck pain and disability scale. Spine (Phila Pa 1976). 2010, 35 (5): 552-556. 10.1097/BRS.0b013e3181b327ff.
Kesiktas N, Ozcan E, Vernon H: Clinimetric properties of the Turkish translation of a modified neck disability index. BMC Musculoskelet Disord. 2012, 13: 25-10.1186/1471-2474-13-25.
Guzy G, Vernon H, Polczyk R, Szpitalak M: Psychometric validation of the authorized Polish version of the Neck Disability Index. Disabil Rehabil. 2013, 35 (25): 2132-2137. 10.3109/09638288.2013.771706.
Shaheen AA, Omar MT, Vernon H: Cross-cultural adaptation, reliability, and validity of the Arabic version of Neck Disability Index in patients with neck pain. Spine (Phila Pa 1976). 2013, 38 (10): E609-615-
Hoving JL, O’Leary EF, Niere KR, Green S, Buchbinder R: Validity of the neck disability index, Northwick Park neck pain questionnaire, and problem elicitation technique for measuring disability associated with whiplash-associated disorders. Pain. 2003, 102 (3): 273-281. 10.1016/S0304-3959(02)00406-2.
Ackelman BH, Lindgren U: Validity and reliability of a modified version of the neck disability index. J Rehabil Med. 2002, 34 (6): 284-287. 10.1080/165019702760390383.
Kose G, Hepguler S, Atamaz F, Oder G: A comparison of four disability scales for Turkish patients with neck pain. J Rehabil Med. 2007, 39 (5): 358-362. 10.2340/16501977-0060.
Mousavi SJ, Parnianpour M, Montazeri A, Mehdian H, Karimi A, Abedi M, Ashtiani AA, Mobini B, Hadian MR: Translation and validation study of the Iranian versions of the Neck Disability Index and the Neck Pain and Disability Scale. Spine (Phila Pa 1976). 2007, 32 (26): E825-831. 10.1097/BRS.0b013e31815ce6dd.
Daffner SD, Hilibrand AS, Hanscom BS, Brislin BT, Vaccaro AR, Albert TJ: Impact of neck and arm pain on overall health status. Spine (Phila Pa 1976). 2003, 28 (17): 2030-2035. 10.1097/01.BRS.0000083325.27357.39.
Fernandez-Perez AM, Villaverde-Gutierrez C, Mora-Sanchez A, Alonso-Blanco C, Sterling M, Fernandez-de-Las-Penas C: Muscle trigger points, pressure pain threshold, and cervical range of motion in patients with high level of disability related to acute whiplash injury. J Orthop Sports Phys Ther. 2012, 42 (7): 634-641. 10.2519/jospt.2012.4117.
Saavedra-Hernandez M, Castro-Sanchez AM, Cuesta-Vargas AI, Cleland JA, Fernandez-de-las-Penas C, Arroyo-Morales M: The contribution of previous episodes of pain, pain intensity, physical impairment, and pain-related fear to disability in patients with chronic mechanical neck pain. Am J Phys Med Rehabil. 2012, 91 (12): 1070-1076. 10.1097/PHM.0b013e31827449a5.
Wlodyka-Demaille S, Poiraudeau S, Catanzariti JF, Rannou F, Fermanian J, Revel M: French translation and validation of 3 functional disability scales for neck pain. Arch Phys Med Rehabil. 2002, 83 (3): 376-382. 10.1053/apmr.2002.30623.
Philadelphia P: Philadelphia Panel evidence-based clinical practice guidelines on selected rehabilitation interventions for neck pain. Phys Ther. 2001, 81 (10): 1701-1717.
Hurwitz EL, Carragee EJ, van der Velde G, Carroll LJ, Nordin M, Guzman J, Peloso PM, Holm LW, Cote P, Hogg-Johnson S, Cassidy JD, Haldeman S: Treatment of neck pain: noninvasive interventions: results of the Bone and Joint Decade 2000–2010 Task Force on Neck Pain and Its Associated Disorders. J Manipulative Physiol Ther. 2009, 32 (2 Suppl): S141-175.
Cramer H, Lauche R, Hohmann C, Langhorst J, Dobos G: Yoga for chronic neck pain: a 12-month follow-up. Pain Med. 2013, 14 (4): 541-548. 10.1111/pme.12053.
Soklic M, Peterson C, Humphreys BK: Translation and validation of the German version of the Bournemouth questionnaire for neck pain. Chiropr Man Therap. 2012, 20 (1): 2-10.1186/2045-709X-20-2.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/15/91/prepub
Acknowledgments
All trials had been supported by a grant from the Karl and Veronica Carstens-Foundation, Essen, Germany. The Karl and Veronica Carstens-Foundation had no role in the design, data collection, analysis and interpretation of data, in the writing of the manuscript or decision to submit the manuscript for publication. The authors thank the researchers involved in the trials as well as the study participants.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declare that there are no financial or non-financial conflicts of interest.
Authors’ contributions
HC was responsible for conception and design of the study, analysis and interpretation of data, participated in acquisition of data, and drafted the manuscript. RL participated in conception and design of the study, acquisition of data, analysis and interpretation of data, and critically revised the manuscript. JL and GD participated in conception and design of the study, and critically revised the manuscript. AM participated in conception and design of the study, acquisition of data, and critically revised the manuscript. All authors read and approved the final manuscript.
Electronic supplementary material
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited.
About this article
Cite this article
Cramer, H., Lauche, R., Langhorst, J. et al. Validation of the German version of the Neck Disability Index (NDI). BMC Musculoskelet Disord 15, 91 (2014). https://doi.org/10.1186/1471-2474-15-91
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2474-15-91