
Abstract
Background
Whether the increase in vascular disease prevalence and mortality in OA populations is a result of co-occurrence of cardiovascular disease and OA, which are both common in the older population, is due to OA treatments or to the common association with reduced physical activity and/or obesity is unclear. One way to explore this non-invasively is to examine the cross-sectional relationship between changes in retinal microvasculature, which have been shown to be markers of generalized vascular pathology, and knee structural changes in an asymptomatic community-based population.
Methods
A community sample of 289 (61% women) aged 50–79 years with no knee symptoms underwent magnetic resonance imaging (MRI) of their dominant knee in 2003. Cartilage volume and bone marrow lesions (BMLs) were determined. All subjects also had retinal photographs taken from which retinal arteriolar and venular diameters were determined and summarized as the central retinal arteriolar equivalent (CRAE) and the central retinal venular equivalent (CRVE).
Results
Retinal venular diameter was significantly wider in subjects with a BML compared with subjects without a BML (mean (SD) 214.2 (2.8) μm versus 207.5 (1.1) μm respectively independent of age, gender and BMI. A trend for decreased medial tibial cartilage with increasing CRAE was also observed (regression coefficient −2.70 μl, 95%CI-5.74, 0.5, p=0.08).
Conclusion
These findings suggest that vascular pathology, indicative of inflammatory processes, is associated with early structural knee changes. The role of micro-vascular changes in the pathogenesis of OA warrants further investigation.
Similar content being viewed by others


Background
There is growing evidence that vascular disease might have a role in the pathogenesis of osteoarthritis (OA)[1]. People with OA have a higher prevalence of vascular disease and cardiovascular risk factors than those without OA[2]. More recently it was also found patients with OA are at higher risk of death from diabetes and cardiovascular disease compared to the general population[3]. Specific markers of vascular pathology including vessel wall thickness[4] and carotid artery calcification[5] have been also associated with the presence of generalised and hand OA respectively. While the study of vascular changes in hand OA[5] may not adequately represent the identical genetic, inflammatory and degenerative factors seen in knee OA. It still adds to the body of work suggesting vascular mechanism in OA. Whether the increase in vascular disease prevalence and mortality in OA populations is a result of the co-occurrence of cardiovascular disease and OA, which are both common in the older population, is due to OA treatments or to the common association with reduced physical activity and/or obesity is unclear[6].
One way to explore this is to examine asymptomatic people, prior to the onset of clinical knee OA. By using MRI it is possible to assess joint structure non-invasively. Structures such as cartilage volume and bone marrow lesions can be measured. Reduced cartilage volume is associated with increasing severity of OA and is linked to joint replacement[7], a clinically important outcome. Bone marrow lesions(BMLs) are associated with pain and progression of knee OA[8]. A further challenge is the difficulty of directly assessing bone microvasculature in healthy subjects. The retina provides a direct visualization of microvasculature in the body. Retinal microvasculature changes, such as arteriolar narrowing and venular widening, have been shown to be marker of generalized vascular pathology with reported associations with diabetes, hypertension, metabolic syndrome, atherosclerosis and inflammation and micro vascular disease (reviewed in[9]). Recently the relationships between retinal vascular calibre in patients with rheumatoid arthritis(RA) were explored[10]. Patients with RA were shown to have significantly wider retinal venular calibre compared to controls[10].
Therefore the aim of this study was to explore the cross-sectional relationship between changes in retinal microvasculature with BMLs and cartilage volume in a sample of asymptomatic community based adults.
Methods
Subjects
Subjects were recruited from the Melbourne Collaborative Cohort Study(MCCS). Subjects were excluded if they had OA, as defined by the American College of Rheumatology clinical criteria, current or past knee disease, a history of knee pain in the past five years at baseline lasting for > 24 hours; a previous knee injury requiring non-weight bearing treatment for > 24 hours or surgery (including arthroscopy); or a history of any arthritis diagnosed by a medical practitioner or contraindication to MRI. The study was approved by the Human Research Ethics Committee of The Cancer Council of Victoria and Monash University Standing Committee on Ethics in Research Involving Humans. All participants gave written informed consent.
Data collection
Participants completed a questionnaire that captured information on their demographics. Weight was measured to the nearest 0.1 kg (shoes, socks, and bulky clothing removed) using a single pair of electronic scales. Height was measured to the nearest 0.1 cm (shoes and socks removed) using a stadiometer. From these data, BMI (weight/height2 kg m-2) was calculated.
Magnetic resonance imaging
A sagittal MRI of the dominant knee (defined as the lower-limb from which the subject stepped off when initiating gait) for each participant was performed between October 2003 and December 2004 as described on a 1.5-T whole body MR unit (Philips, Medical Systems, Eindhoven, the Netherlands) using a commercial transmit-receive extremity coil. The following sequences and parameters were used: fat suppressed, gradient recall acquisition in the steady state, three dimensional T1-weighted (58 msec/123 msec/55°, repetition time/echo time/ flip angle), 1 signal average, slice thickness 1.5 mm, field of view 16 cm and matrix 512 × 512. In addition a coronal T2-weighted fat-saturated acquisition, repetition time 2200 ms, echo time 20/80 ms, with a slice thickness of 3 mm, a 0.3 interslice gap, 1 excitation, a field of view of 11-12 cm, and a matrix of 256 × 128 pixels was also obtained[11].
Cartilage volume
Knee cartilage volume was determined by image processing on an independent workstation using the Osiris software (Digital Imaging Unit, University Hospital of Geneva, Switzerland). The volumes of individual cartilage plates (medial and lateral tibia) were measured from the total volume by manually drawing disarticulation contours around the cartilage boundaries on each section on a workstation as described from T1 images by 2 independent trained observers unpaired and blinded to subject identification The interclass correlation coefficients (ICC) were 0.94 for medial and 0.96 for lateral tibial cartilage volume measurements. The coefficients of intra-reader variation (CVs) for the medial and lateral tibial cartilage volume measures were 3.4% and 2.0% respectively[11].
Bone area
The cross-sectional areas of medial and lateral tibial plateaus were determined by means of image processing on an independent workstation using the software program OsiriX, by creating an isotropic volume from the input images, which were reformatted in the axial plane. Areas were directly measured from these axial images as previously described from T1 images by two assessors[11]. Using this technique, osteophytes, if present, are not included in the area of interest. The ICC (inter-class) were 0.97 for medial and 0.92 for lateral tibial plateau area measurements. The CVs for the medial and lateral tibial plateau bone areas were 2.3% and 2.4%, respectively[11].
Bone marrow lesions
BMLs were defined as areas of increased signal intensity adjacent to subcortical bone present in either the medial or lateral, distal femur or proximal tibia[12]. Two trained observers, who were blinded to patient characteristics, together assessed the presence of lesions for each subject from T2 coronal images[12]. The presence or absence of a BML was determined. The reproducibility for determination of the BML was assessed using 60 randomly selected knee MRIs (к value 0.88, P < 0.001).
Measurement of retinal vascular calibre
Non-mydriatic retinal photographs of both eyes, centred on the optic disc and the macula, were taken of participants using a digital retinal camera (Canon CR6-45NM; Canon, Lake Success, NY, USA). Retinal vascular calibre was measured using a computer-assisted vessel measurement system (University of Wisconsin, Madison, WI, USA) that uses microdensity to detect the vessel edge[13]. With the assistance of a trained grader, the program identifies all retinal vessels greater than 25 μm in diameter that completely pass through the region between 1/2 and 1 disc diameter from the optic disc margin (zone B) and identifies their edges using a pixel density histogram. The cross-sectional diameter of retinal arterioles and venules is measured repeatedly and summarized using formulae to obtain values representing the average arteriolar and venular caliber of that particular eye. The inter- and intra-grader agreement was examined in randomly selected 90 images. The inter- and intra-grader correlation coefficients for CRAE were 0.95 and 0.96 respectively. The inter- and intra-grader correlation coefficients for CRVE measurements were 0.98 and 0.99 respectively. Figure1 provides a retinal photograph with the arterioles and venules identified from which CRAE and CRVE are determined. Because retinal calibre measures were highly correlated between eyes, vascular calibre measurements of the right eye were used in all analyses.

Retinal photograph with the arterioles and venules identified from which CRAE and CRVE are determined.
Statistical analysis
Descriptive statistics for the characteristics of the study subjects were tabulated. All variables were assessed for normality. Retinal measures, cartilage volume and bone area were normally distributed. BMLs were dichotomous. The general linear model was used to compare retinal measures between those with and those without a BML. The estimated marginal mean was adjusted for age, gender and body mass index (model 1) and also either CRAE or CRVE (model 2). The relationship between retinal vasculature and cartilage volume was assessed by linear regression. The potential confounder’s age, gender, BMI and respective bone area (model 1) and also BMLs (yes v. No) (model 2) were included in multivariate analyses. A p value of less than 0.05 (two-tailed) was regarded as statistically significant. All analyses were performed using the SPSS statistical package (standard version 14.0, SPSS, Chicago, IL, USA).
Results
Retinal photographs were available for 287(96%) participants. Study participants had a mean age of 58(SD5.5) years and BMI of 25.9(4.3) kg/m2. There were 186 women(61%). The mean CRAE and CRVE were 144.2(13.5) μm and 208.4(17.8) μm, respectively. Two participants(0.7%) had diabetes. Forty two(14%) people had a BML in their knee. People with a BML were not significantly older than those who did not have a BML (p= 0.22). The mean cartilage volume area at baseline was 1700 μl (SD 528) for the medial and 2042 μl (SD631) for the lateral compartment.
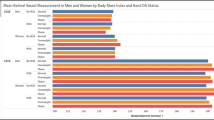
The mean vessel diameters for those with a BML and for those without a BML are presented in Table1. No significant difference in retinal arteriolar diameter was observed between those with and those without a BML. In contrast, venular diameter was significantly wider for subjects with a BML compared with subjects without a BML both before (mean 214.1(SE2.8) μm for those with a BML compared with 207.5(SE1.1) μm, p=0.03) and after adjustment with age, gender and BMI (mean 214.2(SE2.8) μm for those with a BML compared with 207.5 (SE1.1) μm for those without a BML. No significant differences in arteriole diameters were observed. Similar findings were observed when the two subjects with diabetes were excluded from the analyses (data not shown).
The relationship between vessel diameter and medial and lateral tibial cartilage volume is presented in Table2. Increasing arteriolar diameter was significantly associated with less medial tibial cartilage volume (regression coefficient −5.6 μl (95%CI-10.1, -1.1) change in cartilage volume per μm change in CRAE p=0.02) in univariate analyses. After adjustment the association remained the same but was no longer significant (regression coefficient −2.65 μl (95%CI −5.67, 0.38) p=0.09). Additional adjustment with BML presence did not change the association. No significant associations between arteriolar diameter and lateral tibial cartilage volume were observed. Similarly we did not observe any significant associations between venular diameter and either medial or lateral tibial cartilage volume. When the 2 diabetic subjects were excluded no significant differences were observed (data not shown).
Discussion
In our cross-sectional study of asymptomatic community based adults, mean retinal venular diameter was significantly wider in participants with a BML. A trend for reduced cartilage volume within the medial compartment with increasing arteriolar diameter was also observed.
In our study we found that those with BMLs had wider a CRVE. Wider venular calibre has been linked to diabetes, measures of arthrosclerosis, obesity and hypertriglyceridemia[9]. While the mechanisms linking the relationships between these conditions and increased venular diameter are unknown, there is some evidence to suggest that inflammatory processes or endothelial dysfunction underlie these relationships. Increased venular diameter has been associated with systemic markers of inflammation, such as C-reactive protein[14, 15]. Venous occlusion and stasis may result in increased intra-osseous pressure and ischemia. Such changes have been reported in studies of bone marrow oedema in both human and animal models of OA[1, 16, 17]. It is well recognised that BMLs assessed on MRI may represent areas of osteonecrosis, oedema, trabecular abnormalities and bony remodeling[18] and there is evidence that they may be the consequence of episodes of ischemia and inflammation[19]. The findings of this study support a role for vascular changes possibly mediated by inflammatory factors. It is well known that the medial compartment is more susceptible to damage, most likely due to the increased loading through that compartment[20]. Our findings in the medial rather than the lateral compartment suggest a combination of systemic effects with local biomechanical effects.
The relationship between vascular markers and cartilage has not been previously explored. However, there is some evidence of a relationship with joint replacement, a marker of end stage OA[21]. Among women of the AGES-Reykjavik study, increased aortic calcium was associated with joint replacement (JR) due to OA. A trend towards increased atherosclerosis and JR was also observed[21]. In this study, we showed a trend for increasing arteriolar diameter and reduced medial, but not lateral, tibial cartilage volume. Cartilage is avascular receiving nutrients and oxygen from the underlying bone with more than 50% of the glucose, oxygen and water requirements of cartilage being provided by perfusion from the subchondral vessels[22]. Dilation of arterioles has been associated with markers of inflammation including higher leukocytes counts and higher erythrocyte sedimentation rate[15]. It is possible that inflammatory processes may affect the subchondral vessels resulting in the impaired the supply of nutrients to the overlying cartilage plate and subsequent cartilage loss. There is also evidence that during the degenerative process there is neovascularisation of the deep regions of articular cartilage[23]. It is possible that once early vascularisation of cartilage occurs inflammatory processes may influence cartilage directly. This has the potential to affect the structural integrity of cartilage and in the context of local biomechanical factors influence the progression of disease. Further longitudinal research will be required to assess this.
This study had a number of limitations. We have not examined vasculature in the bones directly. Our finding suggests that systemic factors are associated with knee changes cross-sectionally. It is possible that there are local factors affecting the vasculature that we have not been able to measure, further work will be required to assess this. The association of arterioles with cartilage volume did not reach significance, however given this was an asymptomatic population without evidence of clinical disease, and that a number of factors have been associated with cartilage volume cross-sectionally, it is not surprising that we did not detect a significant association between retinal vessel calibre and cartilage volume above the stronger risk factors. We did not assess femoral cartilage. A major limitation in measuring femoral cartilage volume is that the femoral cartilage articulates with the medial and lateral tibial cartilage and the patellar cartilage. There is no clear anatomical hallmark to separate the subregions of femoral cartilage that form part of each of these compartments so non-anatomical rules have been used to measure the femoral cartilage in different subregions. In addition tibial cartilage volume correlates with femoral cartilage volume in the same compartment[24] and grade of radiographic knee OA[25]. It is for these reasons that we have measured the tibial cartilage volume. This study was cross-sectional, therefore we cannot infer causality, larger longitudinal studies will be required. Finally due to the modest number of BMLs in our cohort, larger studies are needed which include examination of BML volume.
Conclusion
We found that retinal venular diameter was wider in participants with a BML. A trend for reduced cartilage volume within the medial compartment with increasing arteriolar diameter was also observed. These findings were in asymptomatic community based adults who were free of clinical knee OA. These findings suggest a novel hypothesis that micro vascular pathology may be important in the pathogenesis of knee OA and warrants further work.
Key messages
These findings suggest that vascular pathology is associated with early structural knee changes. The role of micro-vascular changes in the pathogenesis of OA warrants further investigation.
References
Findlay DM: Vascular pathology and osteoarthritis. Rheumatology. 2007, 46: 1763-1768. 10.1093/rheumatology/kem191.
Kadam UT, Jordan K, Croft PR: Clinical comorbidity in patients with osteoarthritis: a case–control study of general practice consulters in England and Wales. Ann Rheu Dis. 2004, 63: 408-414. 10.1136/ard.2003.007526.
Nuesch E, et al: All cause and disease specific mortality in patients with knee or hip osteoarthritis: population based cohort study. BMJ. 2011, 342: d1165-10.1136/bmj.d1165.
Kornaat PR, et al: Positive association between increased popliteal artery vessel wall thickness and generalised osteoarthritis: is OA also part of the metabolic syndrome. Skel Radiol. 2009, 38: 1147-1151. 10.1007/s00256-009-0741-7.
Jonsson H, et al: Hand osteoarthritis in older women is associated with carotid and coronary atherosclerosis: the AGES Reykjavic study. Ann Rheum Dis. 2009, 68: 1696-1700. 10.1136/ard.2008.096289.
Conaghan PG, Vanharanta H, Dieppe PA: Is progressive osteoarthritis an atheromatous vascular disease. Ann Rheum Dis. 2005, 64 (11): 1539-1541. 10.1136/ard.2005.039263.
Cicuttini FM, et al: Rate of cartilage loss at two years predicts subsequent total knee arthroscopy: a prospective study. Ann Rheum Dis. 2004, 63: 1124-1127. 10.1136/ard.2004.021253.
Felson DT, et al: Bone Marrow Edema and its relation to progression of knee osteoarthritis. Ann Intern Med. 2003, 139: 330-336.
Nguyen TT, Wong TY: Retinal vascular manifestations of metabolic disorders. Trends Endocrinol Metab. 2006, 17 (7): 262-268. 10.1016/j.tem.2006.07.006.
Van Doornum S, et al: Retinal vascular calibre is altered in patients with rheumatoid arthritis: a biomarker of disease activity and cardiovascular risk?. Rheum. 2010, Epub ahead of print
Wluka AE, et al: The determinants of change in tibial cartilage volume in osteoarthritic knees. Arthritis Rheum. 2002, 26: 2065-2072.
Wluka AE, et al: Bone Marrow Lesions predict increase in knee cartilage defects and loss of cartilage volume in healthy middle-aged women over 2 years. Ann Rheum Dis. 2008, 68 (6): 850-855.
Hubbard LD, et al: Methods for evaluation of retinal microvascular abnormalities associated with hypertension/sclerosis in the Atherosclerosis Risk in Communities Study. Ophthalmology. 1999, 106 (12): 2269-2280. 10.1016/S0161-6420(99)90525-0.
Klein R, et al: Are inflammatory factors related to retinal vessel caliber. Arch Ophthalmol. 2006, 124: 87-94. 10.1001/archopht.124.1.87.
Ikram MK, et al: Are retinal arteriolar or venular diameters associated with markers for cardiovascular disorders? The rotterdam study. Invest Opthalmol Vis Sci. 2004, 45: 2129-2134. 10.1167/iovs.03-1390.
Winet H, Hsieh A, Bao JY: Approaches to study of ischemia in bone. J Biomed Mater Res. 1998, 43: 410-421. 10.1002/(SICI)1097-4636(199824)43:4<410::AID-JBM8>3.0.CO;2-B.
Aaron RK, et al: Perfusion abnormalities in subchondral bone associated with marrow edema, osteoarthritis and avascular necrosis. Ann N Y Acad Sci. 2007, 1117: 124-137. 10.1196/annals.1402.069.
Zanetti M, et al: Bone marrow edema pattern in osteoarthritic knees:correlation between MR imaging and histologic findings. Radiology. 2000, 215: 835-840.
Simkin PA: Bone pain and pressure in osteoarthritic joints. Osteoarthritic joint pain. 2004, Wiley, Chichester, 179-186.
Andriacchi TP: Dynamics of knee malalignment. Orthop Clin North Am. 1994, 25 (3): 395-403.
Jonsson H, et al: The presence of total knee or hip replacements due to osteoarthritis enhances the positive association between hand osteoarthritis and atherosclerosis in women: the AGES-Reykjavic study. Ann Rheu Dis. 2011, Epub ahead of print
Imhof H, et al: Subchondral bone and cartilage disease: a rediscovered functional unit. Invest Radiol. 2000, 35: 581-588. 10.1097/00004424-200010000-00004.
Mapp PI, et al: Angiogenesis in two animal models of osteoarthritis. Osteoarthr Cartil. 2008, 1: 61-69.
Cicuttini FM, Wluka AE, Stuckey SL: Tibial and femoral cartilage changes in knee osteoarthritis. Ann Rheum Dis. 2001, 60: 977-980. 10.1136/ard.60.10.977.
Cicuttini F, et al: Comparison of cartilage volume and radiological assessment of the tibiofemoral joint. Arthritis Rheum. 2003, 48: 682-688. 10.1002/art.10840.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2474/13/255/prepub
Acknowledgements
The Melbourne Collaborative Cohort Study recruitment was funded by VicHealth and The Cancer Council of Victoria. This study was funded by a program grant from the National Health and Medical Research Council (NHMRC; 209057) and was further supported by infrastructure provided by The Cancer Council of Victoria. We would like to acknowledge the NHMRC (project grant 334150) and Colonial Foundation. Drs Wluka and Wang are the recipients of NHMRC Public Health Fellowships (317840 and 465142, respectively). Ms Davies-Tuck is the recipient of a Monash Bridging Fellowship. We would especially like to thank the study participants who made this study possible.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interest
The authors declared that they have no competing interest.
Authors’ contributions
FC, AW, GG and English were involved in study design and inception. MLD-T, AW, FC were involved in subject recruitment, data collection, statistical analyses and interpretations. RK, TW and LH were involved in the retinal measures. All authors were involved in manuscript preparation and revision.
Authors’ original submitted files for images
Below are the links to the authors’ original submitted files for images.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Davies-Tuck, M.L., Kawasaki, R., Wluka, A.E. et al. The relationship between retinal vessel calibre and knee cartilage and BMLs. BMC Musculoskelet Disord 13, 255 (2012). https://doi.org/10.1186/1471-2474-13-255
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2474-13-255