
Abstract
Background
To date, few studies have assessed the association between the number of children and obesity in couples. We aimed to investigate this association in men and women aged 20–75 years.
Methods
Data from the National Health Survey were considered in this investigation. It included 2728 women and men (1364 couples) aged 20–75 years. Height and weight were actually measured rather than self-reported. A generalized estimating equation model was used to estimate the odds of obesity (body mass index (BMI ≥ 30)) as a function of the number of children adjusted for age, sex, education, economic index, workforce, smoking and place of residence.
Results
We infer that each additional child has at least 5% and at most 34% increase in the odds of obesity in men and at least 4% and at most 29% increase in the odds of obesity in women. Our test of interaction by sex showed that the association between the number of children and obesity was not different among men and women. Among women, factors that increased obesity included age, low education, having more children, being inactive workforce and being nonsmoker. Among men, these factors included high economic index, low education, having more children, and being nonsmoker.
Conclusion
Our results show an association between the number of children and obesity among men. We would recommend interventions to reduce the number of children to prevent obesity in men.
Similar content being viewed by others


Background
Obesity is considered as the disease of the twenty-first century [1]. In the United States, obesity was not considered as an issue of interest in the mid-1980s, but since then, it has become more common: and in 2003–2004, approximately 32.2 percent of the US adult population were obese [2]. Almost one third of adult Canadians are at increased risk of disability, disease, and premature death due to obesity [3]. Obesity is relatively common in Europe, especially in southern and eastern countries, and studies from repeated surveys suggest that the prevalence of obesity has been increasing recent years [1, 4]. Excess body weight has been reported to be a risk factor for cardiovascular diseases, diabetes, some cancers and other diseases [5–12].
BMI (Body Mass Index) increases with the increase in the number of children among women [13–15]. This contribution seems to be, on average, less than 2 kg per pregnancy [14, 16]. Pregnancy-related weight gain is a significant contribution to weight gain for some women (approximately 15%–20%) [17].
Most studies have identified several factors that could be involved in the weight gained after pregnancy [18–20]. The strongest factor for retaining weight after pregnancy seems to be the weight gain during pregnancy [20, 21].
Smoking cessation, which fortunately often occurs once women learn of their pregnancy, will also make women retain more weight [21]. More sedentary lifestyles after pregnancy also appear to be a risk factor [22–24] and socio-economic factors are also associated with higher weight retention after pregnancy [24–26].
In addition, physiological changes can explain the relationship between the number of children and obesity among women, such as hormonal alterations secondary to fewer ovulatory cycles [14], insulin resistance associated with pregnancy [27, 28], and increased glucocorticoid activity [29, 30] during pregnancy.
Some studies have addressed the association between the number of children and obesity among men. A study on 1039 men aged 50–89 years showed that men with five or more biological children were more obese than men without biological children [31]. In the Rancho Bernardo cohort, a positive relationship between the number of children and obesity among men and women has been observed [32]. In this study, participants were men and women 55 to 84 years old. To date, few studies have assessed this association in couples. Weng HH et al. [33] found a positive relationship between the number of children and obesity among couples. This association was higher in women than in men but not significant. In this study, respondents were couples aged 40–70 years.
We aimed to investigate the association between the number of children and obesity in couples by using cross-sectional data from the National Health Survey in Iran.
Methods
Data set examined
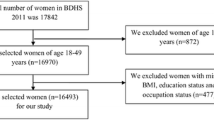
The National Health Survey in Iran is a survey designed to gain comprehensive knowledge and information about health care problems and difficulties throughout the country, 1999–2000. Sampling was conducted on the basis of the cluster method, each cluster comprising of 8 households. The choice of 8 households for the cluster size was based on one-day performance capacity of the data collection group: Four persons (2 physicians, 1 interviewer and 1 lab technician). The statistical framework was based on the household lists available with every Health Department in the provinces, usually updated annually. Where household lists were available, selecting the cluster was made systematically. Data from the National Health Survey were considered in this investigation. These data were collected by the National Research Center of Medical Sciences and are presented partially at the Department of Biostatistics and Epidemiology/Tehran University of Medical Sciences for research. We focused our study on the respondents who lived in Tehran Province only, and the analyzed data included 2728 women and men (1364 couples) aged 20–75 years. We excluded pregnant women from the analyses. This study is approved by the Ethic Committee of the Tehran University of Medical Sciences.
Measurments
BMI (Body Mass Index), our dependent variable, was calculated as weight in kilograms divided by the square of the height in meters (kg/m2), and subjects were classified into obese (BMI ≥ 30 kg/m2) and nonobese (BMI < 30 kg/m2).
Education was defined as the total number of years of education. The respondents were categorized into three groups: those with low (0–8 years), moderate (9–12 years) or high (more than 12 years) education. The three categories used two dummy variables.
The respondents were grouped according to their place of residence as living in cities (urban) or villages (rural). Information about the respondent's age was based on their self-reported birth year.
We had no information on physical activity and alcohol consumption (the consumption of alcohol is prohibited in Iran).
There wasn't any information on household income, but economic index is a surrogate for household income.
Workforce status: The original questionnaire item included twelve response categories. For this analysis, housewife, student, retired and unemployed were grouped into one category named "nonactive workforce" vs. "active workforce" (others).
Economic index was defined as the area of living place (in square meter) divided by number of people in household.
Smoking status dichotomized into smokers (those who smoke every day and have smoked at least 100 cigarettes in their lives) vs. nonsmokers (others).
Information about the number of children was based on self-reports.
Statistical analysis
Since couples' responses are correlated, the Generalized Estimating Equations (GEE) model, which takes into account the correlated nature of responses, with a logit link and exchangeable correlation structure was used to estimate the odds of a obesity as a function of the number of children adjusted for age, sex, education, economic index, workforce, smoking and place of residence. Economic index, the number of children and age were examined as continuous variables. The other five variables were (0,1) variables. We looked specifically for interactions between sex and all covariates (sex × education, sex × smoking and sex × place of residence were not significant and we excluded these nonsignificant terms). The interaction between sex and number of children was not significant but it is sensible to include a variable that is central to the purpose of the study and report its estimated effect even if it is not statistically significant. A model containing interaction terms implies that both the estimated odds ratios and their corresponding confidence intervals vary as the values of the effect modifiers vary. The results are presented as ORs and their 95 percent CIs. All analyses were carried out by using SAS software Package, version 9.1.
Results
Our data included 2728 women and men (1364 couples) aged 20–75 years with a mean age of 36.9 year. The mean BMI of study members was 26.1 kg/m2(95% CI: 25.9–26.3); 17.5 percent were obese (BMI > 30 kg/m2). The mean number of children and economic index were 2.8 and 21.2 m2, respectively. Altogether, 11.6 percent were active workforce. The mean education was 8 years. Of the respondents, 19.5% were smokers, and 93.2% were urban. Table 1 shows the frequency distributions of all variables for men and women by obesity Category.
We started by fitting a preliminary GEE model including only sex and number of children to observe the influence of the potential confounders on obesity. This model shows that the odds of obesity increased with increasing number of children: unadjusted obesity odds ratios were 1.29(95% CI: 1.21–1.39) and 1.10(95% CI: 1.001–1.20) for women and men, respectively. The unadjusted OR of 1.29 for women was significantly different from the unadjusted OR of 1.10 for men because the interaction between the number of children and sex was statistically significant (p = 0.006).
In GEE model controlling for age, economic index, workforce status, education level, place of residence and smoking status, the odds of obesity increased with increasing number of children: obesity odds ratios were 1.18(95% CI: 1.05–1.34) and 1.16(95% CI: 1.04–1.29) for men and women, respectively. For each additional child, the odds of obesity increased by 18% among men and 16% among women. Our test of interaction by sex showed that the association between the number of children and obesity was not different among men and women (P = 0.79). Comparing two models, we found that the obesity odds ratio in women decreased after adjustment for confounding variables, whereas that for men increased slightly.
Moreover, Table 2 shows that age was directly associated with obesity only among women. Obesity odds ratios were 1.02 (95 percent CI: 1.001–1.05), and 0.98 (95 percent CI: 0.96–1.01) for women and men, respectively. We infer that a 1-year increase in age has 2% increase among women and 2% decrease among men in the odds of obesity.
We found a statistically significant association between economic index level and obesity only among men. Obesity odds ratios were 1.002 (95 percent CI: 0.99–1.01), 1.02 (95 percent CI: 1.01–1.04) for women and men, respectively. A 1-m2 increase in economic index has 0.2% in women and 2% increase in men in the odds of obesity.
An inverse association was observed between workforce level and obesity among women. Obesity odds ratios were 0.25 (95 percent CI: 0.10–0.60) and 0.98 (95 percent CI: 0.46–1.27) for active women and men, respectively.
Overall, subjects with lower education were more obese. Using low education as the reference group, obesity odds ratios were 0.76 (95 percent CI: 0.59–0.69) and 0.60 (95 percent CI: 0.37–0.97) for the moderate and high groups, respectively
An association was observed between place of residence and obesity (but nonsignificant). Obesity odds ratio was 0.70 (95 percent CI: 0.47–1.04) for urban couples.
An inverse association was observed between smoking status and obesity. Obesity odds ratio was 0.68 (95 percent CI: 0.48–.98) for smokers compared with nonsmokers.
Among subjects with active workforce level, the odds of obesity for men was1.21 times that for women. In contrast, among subjects with nonactive workforce level, the odds of obesity for women was 2.44 times that for men.
Discussion
In this cross-sectional study, we assessed associations between the number of children and obesity in men and women. In the first model (without confounders), unadjusted obesity odds ratios were 1.29(95% CI: 1.21–1.39) and 1.10(95% CI: 1.001–1.20) for women and men, respectively. Unadjusted OR of 1.29 for women was significantly different from the unadjusted OR of 1.10 for men. Furthermore, we were able to adjust for covariates that might be important confounders in these associations. After adjustment for confounding variables, number of children is positively associated with obesity in both sexes. We infer that each additional child has at least 5% and at most 34% increase in the odds of obesity in men. For women, the figures are 4% and 29%, respectively. Although this association was stronger in men than in women, the difference was not statistically significant. Our results are basically in line with the observation by Weng HH et al [33].
Comparing two models, the influence of the potential confounders included in analysis can be observed. Unadjusted ORS of 1.29 and 1.10 are changed to ORS of 1.16 and 1.18 for women and men, respectively. After controlling for potential confounders, the similar associations were seen in both sexes suggest a lifestyle, rather than a biologic, impact of having children in women.
Our findings were consistent with the conclusions of Lawlor et al. [35] and Hardy et al. [36]. Lawlor et. al [35] concluded that "Lifestyle risk factors associated with child-rearing lead to obesity and result in increased CHD in both sexes; biological responses of pregnancy may have additional adverse effects in women". Hardy et al. [36] showed that "Any association between number of children and CHD risk factors is a result of lifestyle and behaviors associated with family life rather than being as result of the biological impact of pregnancy in women".
Our finding may point toward a better understanding of the social and cultural mechanisms of obesity in couples. Most couples seem to be spending more free time with their children. With increasing number of children, couples may have little time to spend on health behaviors. For example, they don't go to the gyms and exercise centers. Children love fast food, and parents have to follow them. Fast food doesn't contain large amounts of fiber, vitamins, minerals, and the like-elements necessary for good nutrition and health. In contrast, these substances can cause or increase obesity. An increased consumption of snacks [37], caloric beverages [38, 39] and fast foods [40] by children and young adults has been shown repeatedly to be associated with obesity and excess weight gain.
There are some limitations of our study. This study is a cross-sectional study, which means that we cannot draw definitive conclusions concerning the direction of causality. However, this should be confirmed by further longitudinal studies. Measures of "the age of children" and "the length of time the children lived in the household" are useful in this regard but they were not available for study members.
Our study had several strengths. It was performed in a nationally representative sample of the Iranian couples. Few studies have assessed the association between the number of children and obesity in couples. To our knowledge, ours is the first study in Iran. Height and weight were actually measured rather than self-reported. It is well known that self-reports underestimate the prevalence of obesity [41, 42]. This study included couples aged 20–75 years who lived in Tehran province but our findings may be generalized to other provinces as well.
Conclusion
Number of children is positively associated with obesity in both women and men. For each additional child, the odds of obesity increased by 18% among men and 16% among women. Since obesity is positively associated with cardiovascular disease, cancer, diabetes, and other important causes of morbidity and mortality, we would recommend interventions to decrease the number of children to prevent obesity in men, too.
Abbreviations
- BMI:
-
body mass index
- OR:
-
odds ratio
- GEE:
-
generalized estimating equation
- CHD:
-
coronary heart disease.
References
Rossner S: Obesity: the disease of the twenty-first century. Int J Obese. 2002, 6 (Suppl 4): S2-S4. 10.1038/sj.ijo.0802209.
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM: Prevalence of overweight and obesity in the United States, 1999–2004. JAMA. 2006, 295 (13): 1549-55. 10.1001/jama.295.13.1549.
Birmingham CL, Muller JL, Palepu A, Spinelli JI, Anis AH: The cost of obesity in Canada. CMAJ. 1999, 160 (4): 483-488.
Seidell JC: Obesity in Europe; Scaling an epidemic. Int J Obes Relat Metab Disord. 1995, 19 (Suppl 3): S1-S4.
Kannel WB, D'Agosting RB, Cobb JL: Effect of weight on cardiovascular disease. Am J Clin Nutr. 1996, 63: 195-225.
Murphy TK, Calle EE, Rodriguez C, Kahn HS, Thun MJ: Body mass index and colon cancer mortality in a large prospective study. Am J Epidemiol. 2000, 152: 847-54. 10.1093/aje/152.9.847.
Brandt Van den PA, Spiegelman D, Yaun SS: Pooled analysis of prospective cohort studies on height, weight and breast cancer risk. Am J Epidemiol. 2000, 152: 514-27. 10.1093/aje/152.6.514.
Resnik HE, Valsania P, Halter JB, Lin X: Relations of weight gain and weight loos on subsequent diabetes risk in overweight adults. J Epidemiol Community Health. 2000, 54: 596-602. 10.1136/jech.54.8.596.
Corrada MM, Kawas CH, Mozzafar F, Paganini-Hill A: Association of body mass index and weight change with all-cause mortality in the elderly. Am J Epidemiol. 2005, 163: 938-949. 10.1093/aje/kwj114.
Magnusson PKE, Rasmussen F, Lawlor DA, Tynelius P, Gunnell D: Association of body mass index with suicide mortality: a prospective cohort study of more than one mollion men. Am J Epedimiol. 2006, 163: 1-8. 10.1093/aje/kwj002.
Tikkinen KAO, Auvinen A, Huhtala H, Tammela TL: Nocturia and obesity: a population – based study in Finland. Am J Epidemiol. 2006, 163: 1003-11. 10.1093/aje/kwj139.
Mishra V, Arnold F, Semenov G, Hong R, Mukuria A: Epidemiology of obesity and hypertension and related risk factors in Uzbekistan. Eur J Clin Nutr. 2006, 69: 1355-66. 10.1038/sj.ejcn.1602465.
Bradley PJ: Conditions recalled to have been associated with weight gain in adulthood. Appetite. 1985, 6: 235-241.
Rossner S: Pregnancy, weight cycling and weight gain in obesity. Int J Obes Relat Metab Disord. 1992, 16 (2): 145-7.
Wilsgaard T, Jacobsen BK, Arnesen E: Determining lifestyle correlates of body mass index using multilevel analyses: The Tromso study,1979–2001. Am J Epedimiol. 2005, 162: 1179-88. 10.1093/aje/kwi328.
Brown JE, Kaye SA, Folsom AR: Parity-related weight change in women. Int J Obes Relat Metab Disord. 1992, 16 (9): 627-31.
Gunderson EP, Abrams B: Epidemiology of gestational weight gain and body weight changes after pregnancy. Epidemiol Rev. 2000, 22: 261-
Williamson DF, Madans J, Pamuk E, Flegal KM, Kendrick JS, Serdula MK: A prospective study of childbearing and 10-year weight gain in US white women 25 to 45 years of age. Int J Obes Relat Metab Disord. 1994, 18: 561-9.
Schauberger CW, Rooney BL, Brimer LM: Factors that influence weight loss in the puerperium. Obstet Gynecol. 1992, 79: 424-
Harris HE, Ellison GT, Holliday M, Lucassen E: The impact of pregnancy on the long-term weight gain of primiparous women in England. Int J Obes Rel Metab Disord. 1997, 21: 747-10.1038/sj.ijo.0800466.
Rossner S, Ohlin A: Pregnancy as a risk factor for obesity: lessons from the Stockholm Pregnancy and Weight Development Study. Obes Res. 1995, 3 (Suppl 2): 267s-275s.
Ohlin A, Rossner S: Trends in eating patterns, physical activity and socio-demographic factors in relation to postpartum body weight development. Br J Nutr. 1994, 71: 457-70. 10.1079/BJN19940155.
Walker LO: Predictors of weight gain at 6 and 18 months after childbirth: a pilot study. J Obstet Gynecol Neonatal Nurs. 1996, 25: 39-48. 10.1111/j.1552-6909.1996.tb02511.x.
Harris HE, Ellison GT, Clement S: Do the psychosocial and behavioral changes that accompany motherhood influence the impact of pregnancy on long-term weight gain?. J Psychosom Obstet Gynaecol. 1999, 20: 65-79. 10.3109/01674829909075579.
Potter S, Hannum S, McFarlin B, Essex-Sorlie D, Campbell E, Trupin S: Does infant feeding method influence maternal postpartum weight loss. J Am Diet Assoc. 1991, 91: 441-6.
Harris HE, Ellison GT, Clement S: Relative importance of heritable characteristics and lifestyle in the development of maternal obesity. J Epidemiol Community Health. 1999, 53: 66-74.
Godsland IF: The influence of female sex steroids on glucose metabolism and insulin action. J Intern Med. 1996, 738 (Suppl): 1-
Kritz-Silverstein D, Barrett-Connor E, Wingard DL: The effect of parity on the later development of noninsulin-dependent diabetes mellitus or impaired glucose tolerance. N Engl J Med. 1989, 321: 1214-
Heliovaara M, Aromaa A: Parity and obesity. J Epidemiol Community Health. 1981, 35: 197-
Harris HE, Ellison GT, Richter LM, de Wet T, Levin J: Are overweight women at increased risk of obesity following pregnancy?. Br J Nutr. 1998, 79: 489-10.1079/BJN19980086.
Kritz-Silverstein D, Barrett-Connor E, Friedlander NJ: Parenthood and lipid and lipoprotein levels in older men. Ann Epidemiol. 1997, 7: 275-10.1016/S1047-2797(97)00016-1.
Barrett-Connor E: Sex differences in coronary heart disease: Why are women so superior? The Ancel Keys Lecture. Circulation. 1997, 95: 252-
Weng Haoling, Bastian Lori, Taylor Donald, Moser Barry, Ostbye Truls: Number of Children Associated with Obesity in Middle-Aged Women and Men: Results from the Health and Retirement Study. J Women's Health. 2004, 13: 85-10.1089/154099904322836492.
World Health Organisation: Obesity: preventing and managing the global epidemic. Report of a WHO Consultation on obesity. Geneva 3–5 June 1997. 1998, Switzerland: World Health Organisation
Lawlor DA, Emberson JR, Ebrahim S, Whincup PH, Wannamethee SG, Walker M, Davey SG: Is the Association Between Parity and Coronary Heart Disease Due to Biological Effects of Pregnancy or Adverse Lifestyle Risk Factors Associated With Child-Rearing?: Findings From the British Women's Heart and Health Study and the British Regional Heart Study. Circulation. 2003, 107: 1260-4. 10.1161/01.CIR.0000053441.43495.1A.
Hardy R, Lawlor DA, Black S, Wadsworth MEJ, Kuh D: Number of children and coronary heart disease risk factors in men and women from a British birth cohort. BJOG. 2007, 114: 721-730. 10.1111/j.1471-0528.2007.01324.x.
Zizza C, Siega-Riz AM, Popkin BM: Significant increase in young adults snacking between 1977–1978 and 1994–1996 represents a cause for concern. Prev Mec. 2001, 32: 303-10. 10.1006/pmed.2000.0817.
Harnack L, Stang J, Story M: Soft drink consumption among U.S. children and adolescents: nutritional consequences. J Am Diet Assoc. 1999, 99: 436-41. 10.1016/S0002-8223(99)00106-6.
Ludwig DS, Peterson KE, Gortmaker SL: Relation between consumption of suger-sweetened drinks and childhood obesity: a prospective, observational analysis. Lancet. 2001, 357: 505-8. 10.1016/S0140-6736(00)04041-1.
French SA, Story M, Jeffery RW: Environmental influences on eating and physical activity. Annu Rev Public Health. 2001, 22: 309-35. 10.1146/annurev.publhealth.22.1.309.
Bostrom G, Diderichsen F: Socioeconomic differences in misclassification of height, weight and body mass index based on questionnaire data. Int J Epidemiol. 1997, 26: 860-6. 10.1093/ije/26.4.860.
Kuskowska-Wolk A, Bergstrom R, Bostrom G: Relationship between questionnaire data and medical records of height, weight and body mass index. Int J Obes Relat Metab Disord. 1992, 16 (1): 1-9.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/8/213/prepub
Acknowledgements
This study was financed by a grant from Tehran University/Medical Sciences. The authors acknowledge the National Health Survey for their data, coordinated at the Department of Biostatistics, School of Public Health and Institute of Public Health Research, Tehran University/Medical Science, Iran.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The authors declare that they have no competing of interests.
Authors' contributions
EB, MRE and KM originated the idea for this study, did the research proposal, data analysis and prepared the manuscript. ARF and HZ co-ordinated the research project. AF helped and edited the final version as the epidemiology consultant. FS helped and edited the final version as the nutrition consultant. BS helped and edited the final as the physiology consultant. All authors read and approved the final manuscript.
Rights and permissions
Open Access This article is published under license to BioMed Central Ltd. This is an Open Access article is distributed under the terms of the Creative Commons Attribution License ( https://creativecommons.org/licenses/by/2.0 ), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Bakhshi, E., Eshraghian, M.R., Mohammad, K. et al. The positive association between number of children and obesity in Iranian women and men: Results from the National Health Survey. BMC Public Health 8, 213 (2008). https://doi.org/10.1186/1471-2458-8-213
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-8-213