
Abstract
Background
European citizens are increasingly being offered Internet health services. This study investigated patterns of health-related Internet use, its consequences, and citizens' expectations about their doctors' provision of e-health services.
Methods
Representative samples were obtained from the general populations in Norway, Denmark, Germany, Greece, Poland, Portugal and Latvia. The total sample consisted of 7934 respondents. Interviews were conducted by telephone.
Results
44 % of the total sample, 71 % of the Internet users, had used the Internet for health purposes. Factors that positively affected the use of Internet for health purposes were youth, higher education, white-collar or no paid job, visits to the GP during the past year, long-term illness or disabilities, and a subjective assessment of one's own health as good. Women were the most active health users among those who were online. One in four of the respondents used the Internet to prepare for or follow up doctors' appointments. Feeling reassured after using the Internet for health purposes was twice as common as experiencing anxieties. When choosing a new doctor, more than a third of the sample rated the provision of e-health services as important.
Conclusion
The users of Internet health services differ from the general population when it comes to health and demographic variables. The most common way to use the Internet in health matters is to read information, second comes using the net to decide whether to see a doctor and to prepare for and follow up on doctors' appointments. Hence, health-related use of the Internet does affect patients' use of other health services, but it would appear to supplement rather than to replace other health services.
Similar content being viewed by others


Background
There is a considerable demand for health-related information in the population, and the Internet is gaining ground as a central source of such information [1, 2]. In the US, studies have found that between 56 % and 79 % of Internet users seek health information [3–6]. Starting out as a grassroots phenomenon much used by individual patients operating on their own and often offered by idealists as well as by commercial interests, Internet health sites and other electronic communication tools targeting patients are now important policy instruments for both public and private health providers. In recent years, we have seen national health authorities beginning to focus on e-health services such as electronic health cards, electronic patient records and health portals, including the English NHS Direct Online, the German Telematic Platform, and the Danish Sundhed.dk. In the medical community, expectations about the Internet are mixed. On one hand, the Internet has been described as having the potential to empower patients and stimulate patient participation [7–10]. On the other hand, potential dangers such as the dissemination of inaccurate information and inappropriate use have been stressed [11–13]. Earlier European studies have shown that the use of the Internet for health purposes varied in different parts of Europe [14, 15]. As the dissemination of e-health services is growing along with general Internet use, there is a need to improve our knowledge on how these services are used, by whom and with what consequences. Two research questions were pursued in the present study; Do the users of Internet health services differ from the general population with respect to health and demographic variables? And, which health related Internet activities are most common? Further, we investigated citizens' expectations concerning the provision of e-health services by doctors.
Methods
A study group of 20 researchers designed a questionnaire for computer-assisted telephone interviews (CATI). The questionnaire was piloted with 100 individuals to ensure the comprehensibility of the wording and internal validity. It was designed in English and translated into the other languages by means of the dual focus approach [16]. This approach differs from the translation-back translation method in that it focuses on conceptual equivalence as well as on equivalence in wording and grammar. The aim is to reduce potential cultural bias in the questionnaire. The survey was conducted during the period October to November 2005. Random digit dialling in stratas ensured a randomised representative sample of the populations (age group 15 – 80 years) of seven European countries. The telephone penetration was estimated to be close to 100 % in Norway, Denmark, and Germany. In Poland it was estimated to be 63 %, in Latvia 93 %, in Greece 87 %, and in Portugal 65 %. Mobile phone numbers were included in Norway, Denmark, Germany, and Latvia. Sampling continued until we had approximately 1000 completed interviews from all countries, except Portugal where 2000 interviews were conducted as health- related Internet use was expected to be low. Calculating a response rate is difficult when this sampling procedure is used, as a required number of responses is set before sampling starts, and sampling actually continues until the required number is obtained. The polling agencies conducting the interviews were instructed to follow standard procedures relating to contacting a replacement if a person originally selected for interview was unavailable (i.e. because of incorrect phone number, not answering the phone, not at home, or unwilling to participate). Nevertheless, we lack accurate data from all agencies relating to the number of people who were contacted in order to achieve the final number of completed interviews. A population weight was used to correct for differences in the sizes of the countries' populations for total estimates and logistic regression. No variables had more than 5% missing data. National ethics committees from all countries were informed and had no objections to the survey. We analysed the data by performing descriptive statistics and logistic regression analysis. SPSS version 12.0 was used for all analyses.
Results
The total sample consisted of 7934 respondents; out of these 4714 reported that they were Internet users. After weighting for population size, we had a total sample of 7903, of which 4906 were Internet users.
Before weighting, we calculated the proportion of Internet health users in each country (Table 1). Health-related use of the Internet was most frequent in the Northern countries, with Denmark (62 %), and Norway (59 %) topping the list, followed by Germany (49 %). The Eastern countries, Poland and Latvia, reported 42 % and 35 % health-related use of the Internet respectively, while the Southern countries had the lowest proportion of Internet health users with 30 % in Portugal and 23 % in Greece. In the sub-sample of Internet users, the differences between the countries were smaller, but a chi-square test showed that the differences between the Northern (74 % Internet health users), East-European (72 %) and Southern countries (60 %) were significant (χ2 (2,4714) = 88, 5, p < 0.001), despite the high score in Poland (79 %).
In the joint population of the seven countries, a total of 44 % (71 % Internet users) reported having used the Internet for health purposes (Table 2). In the general population, men were the most active health users on the Internet (47 % men, 42 % women). However, when Internet access was controlled for and we concentrated on those who were online, women tended to use the Internet more for health purposes than men (75 % women, 68% men). In the total sample, the youngest age group (15–29 years) was more concerned with looking for health information (63 %). Among the Internet users, the 30–44 age group included the most active health users (74 %). Regression analysis revealed that people with higher education and those working in a white-collar profession or not working at all tended to use the Internet more for health purposes. The same applied to those who had visited a general practitioner during the past year and to those who suffered from long-term illness or disability. Subjective assessment of health status had an opposite impact on health-related Internet use in the total sample; those who reported their health to be poor used the Internet less for health purposes than did other respondents. In the total sample, being next of kin to an ill person also increased the likelihood of using the Internet for health purposes, while this correlation did not prove to be significant in the sub-sample of Internet users.
Table 3 shows that one of the most frequent consequences of use was a feeling of reassurance or relief (19 % of the sample). Feelings of anxiety were reported by 10 %. When asked how important they considered the Internet to be as a source of health information, 3141 of the respondents, 40 % of the total sample (53 % of the Internet users), reported it to be important or very important (Table 4). The corresponding figure for face-to-face interaction with health professionals was 6469 respondents, that is, 82 % of the total sample (81 % of the Internet users). Table 5 presents the importance of different e-health services in the choice of a doctor in the total population and among Internet users.
Discussion
Some aspects of the present study should be improved in a follow up study. As mentioned in the methods section, we were unable to calculate an exact response rate due to lacking data from the polling agencies. Even though the number of respondents was high and even though lacking responses to phone calls may be due to many factors, the response rate is of importance to the assessment of the validity of studies such as the present. The telephone penetration in Poland is quite low, which may be of importance to the calculation of the use of e-health services. A future study should therefore include a proportion of mobile phone users in the Polish sample. Income was not included as a variable in the present study. Although education and profession are variables of importance to socio-economic status, adding an income variable could give an even better understanding of the respondents' socio-economic background.
Use of Internet health services varies with country of residence. The North European countries and Poland topped the list, while we found the South European countries at the bottom. As the differences are significant within the sub-sample of Internet users as well, they may not be associated solely with the degree of general Internet access. Two explanations are possible: first, cultural differences, such as preoccupation with health and illness together with other factors, such as the number of accessible web-sites in local languages and the quality and accessibility of general health services, may be of importance [12]. Second, it may be that the Internet user group in the Southern countries is dominated by early adopters, and that the interest in health issues is lower in this group than it is in the general population. If so, we might assume that geographical differences will even out as access becomes more evenly distributed in the national populations.
In the sub-sample of Internet users, women reported more health-related use. This finding is in line with that reported by some studies from the US [1, 3, 17], that female Internet users are more interested in health-related issues. The youngest age group comprises the most ardent Internet users, but it is the young adults and the middle aged who take most interest in health information once they are online. A plausible explanation is that we find a large proportion of family caregivers in this group. Having completed higher education has previously been found to be associated with higher use of the Internet for health purposes [1, 3], a finding which this study confirms. Having a white-collar position usually means longer education; thus it is not surprising that this group are more active Internet health users. We also found a high level of health-related use of the Internet among people who did not have paid work, a possible explanation for this being that students form an important part of this group.
Those who assessed their own health status as poor tended to use the Internet less than others to get health information. However, medical indicators of health, such as a current diagnosis of long-term illness or disability, and a high number of visits to the GP, indicate a higher level of health-related use of the Internet. Hence, we find that those who suffer from illness but who nevertheless feel that they are in good health use the Internet most for health purposes. Concern has been expressed that there might be some patients who feel they are too ill or who do not have the resources to use the Internet [18]. Our study indicates this might be the case. It is important to keep such differences between patient groups in mind when future e-health services and strategies are developed, in order not to widen the gap between the well off and the less well off in society [19].
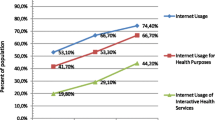
Our study confirms that the main health-related activity on the Internet is information seeking [1, 2]. However, a considerably higher number than previously reported [3] used the Internet as a communication channel. Among Internet users, 27 % had participated in forums or self-help groups and 30 % had interacted with health professionals. This indicates that other health-related activities on the Internet are becoming increasingly important, and that e-health services have already become an important part of health care for many people, as has also been suggested by other studies [20].
The possible relation between health related Internet usage and peoples' use of other health services has been given attention in later years [9, 21, 22]. In our study, three findings are of particular interest with regard to this topic: Only 6 % claim they have made, cancelled or changed a doctor's appointment based on health related Internet activity. Second, we found that people primarily use the Internet for general reading. And third, that approximately a quarter of the respondents actually use the Internet to prepare for or follow up a doctor's appointment. Hence we conclude that the Internet is used as a supplement to the ordinary health services rather than as a replacement. Another finding that supports our conclusion is the relatively low number of respondents (40 %) who claimed that the Internet was an important channel for health information (Table 4). Face-to-face contact with a health professional was considered important by almost twice as many, 79 %. However, even if our study shows the Internet is used as a supplement, we also see indications that health related Internet activity affect the populations' use of traditional medical services. One third of the Internet users have brought with them to their doctor suggestions or queries on diagnosis after surfing the net for health information. And almost half of the Internet users claim they have used the Internet to decide whether they need to see a doctor. As the number of European general practitioners offering e-health services is still low, we are not surprised that only 4 % of respondents reported that they had approached their family doctor via the Internet.
It was twice as common to feel reassured as it was as to feel anxious after using the Internet for health purposes. Hence, our study supports the idea that the populations' use of Internet health information is more likely to have a beneficial than a negative influence on individual health experiences [21].
A sign of the increasing importance of the Internet in citizens' health management is that about a third of the respondents stated that the doctor's provision of e-health services was of importance when choosing a new doctor. The differences between the expectations of Internet users and the general population, as presented in Table 5, support the idea that it is likely there will be an increasing demand for provision of e-health services by primary care and hospital services as more and more Europeans obtain Internet access [23].
Conclusion
The Internet is becoming an important source of health information and a potential e-health channel for European citizens. The users of Internet health services differ from the general population when it comes to health and demographic variables. The most common way to use the Internet in health matters is to read information, second comes using the Internet to decide whether to see a doctor and to prepare for and follow up on doctor's appointments. Hence, health-related use of the Internet does affect patients' use of other health services, but it would appear to supplement rather than to replace ordinary health services. It is twice as common for users to feel reassured after accessing the Internet for health purposes as it is to experience anxiety. Doctors are likely to find that patients expect them to offer e-health services. Future strategies should ensure that e-health services are implemented with care, in order not to consolidate or create new inequalities in health care. It will be of great importance to follow up on studies of European citizens' use of e-health.
References
Baker L, Wagner TH, Singer S, Bundorf MK: Use of the internet and e-mail for health care information. JAMA. 2003, 289: 2400-6. 10.1001/jama.289.18.2400.
Eysenbach G, Kohler C: What is the prevalence of health-related searches on the World Wide Web? Qualitative and quantitative analysis of search engine queries on the internet. AMIA Annu Symp Proc. 2003, : 225-9.
Hesse BW: Trust and sources of health information. Arch Intern Med. 2005, 165: 2618-24. 10.1001/archinte.165.22.2618.
Fox S: Health information online. 2005, Washington, DC: Pew Internet & American Life Project, [http://www.pewinternet.org/PPF/r/156/report_display.asp]
Ybarra ML, Suman M: Help seeking behaviour and the Internet: A national survey. Int J Med Inf. 2006, 75: 29-41. 10.1016/j.ijmedinf.2005.07.029.
Cotten SR, Gupta SS: Characteristics of online and offline health information seekers and factors that discriminate between them. Soc Sci Med. 2004, 59: 1795-806. 10.1016/j.socscimed.2004.02.020.
Street RL: Mediated consumer-provider communication in cancer care: the empowering potential of new technologies. Patient Educ Couns. 2003, 50: 99-104.
Jadad AR: Promoting partnerships: challenges for the internet age. BMJ. 1999, 319: 761-4.
Andreassen HK, Trondsen M, Kummervold PE, Gammon D, Hjortdahl P: Patients Who Use E-Mediated Communication With Their Doctor- New Constructions of Trust in the Patient-Doctor Relationship. Qual Health Res. 2006, 16: 238-248. 10.1177/1049732305284667.
Sadan B: Patient empowerment and the asymmetry of knowledge. Stud Health Technol Inform. 2002, 90: 514-8.
Mitchell KJ, Becker-Blease KA, Finkelhor D: Inventory of Problematic Internet experiences Encountered in Clinical practice. Prof Psychol Res Pr. 2005, 36: 498-509. 10.1037/0735-7028.36.5.498.
Leaffer T: Quality of health information on the internet. JAMA. 2001, 286: 2094-5.
Skinner H, Biscope S, Poland B, Goldberg E: How adolescents use technology for health information: Implications for health professionals from focus group studies. J Med Internet Res. 2003, 5: e32-10.2196/jmir.5.4.e32.
Milicevic I, Gareis K, Korte WB: Making progress towards user-orientation in online public service provision in Europe. Paper presented at echallenges IST 2005. 2005, [http://www.euser-eu.org/SHOWUSERSQL.asp?SQLID=3,2,4&show=LIST&MenuID=108]
Spadaro R: Eurobarometer 58.0. European Union Citizens and sources of information about health. 2003
Erkut S, Alarcón O, Coll C, Tropp LR, Garcia HAV: The dual-focus approach to creating bilingual measures. J Cross Cult Psychol. 1999, 30: 206-18. 10.1177/0022022199030002004.
Houston TK, Allison JJ: Users of Internet health information: Differences by health status. J Med Internet Res. 2002, 4: e7-10.2196/jmir.4.2.e7.
Bessell TL, Silagy CA, Anderson JN, Hiller JE, Sansom LN: Prevalence of South Australian's online health services. Aust N Z J Public Health. 2002, 26: 170-3.
Korp P: Health on the Internet: Implications for health promotion. Health Educ Res. 2006, 21: 78-86. 10.1093/her/cyh043.
Diaz JA, Griffith RA, Ng JJ, Reinert SE, Friedman PD, Moulton AW: Patients' use of the Internet for medical information. J Gen Intern Med. 2002, 17: 180-5. 10.1046/j.1525-1497.2002.10603.x.
Fogel J, Albert SM, Schnabel F, Ditkoff BA, Neugut AI: Internet use and social support in women with breast cancer. J Health Psychol. 2002, 21: 398-404. 10.1037/0278-6133.21.4.398.
Murray E, Lo B, Pollack L, Donelan K, Catania J, Lee K, Zapert K, Turner R: The impact of health information on the physician-patient relationship. J Med Internet Res. 2003, 5: e17-10.2196/jmir.5.3.e17.
Ferguson T: Online patient-helpers and physicians working together: a new partnership for high quality health care. BMJ. 2000, 321: 1129-32. 10.1136/bmj.321.7269.1129.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/7/53/prepub
Acknowledgements
This article forms part of the WHO/European survey on e-health consumer trends, in part financed by the Programme of Community Action in the Field of Public Health E-health (2003–2008) of the Health and consumer protection directorate general, directorate C, EC. The funding source had no involvement in the study design or interpretation of the data. We acknowledge the contributions of the other members of the project group, Laurence Esterle, Per Hjortdahl, Angelina Kouroubali, Per Egil Kummervold, Antònio Sousa Pereira, Ulli Prokosch, Birgitte Lolan Ravn, Andrzej Staniszewski, Tove Sorensen, Manolis Tsiknakis and Silje C. Wangberg.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
The author(s) declare that they have no competing interests.
Authors' contributions
HKA contributed to conception and design, acquisition of data, analysis and interpretation of data, and drafting and revising the manuscript. CEC contributed to conception and design, acquisition of data, analysis and interpretation of data, and drafting and revising the manuscript. SS contributed to conception and design, acquisition of data, analysis and interpretation of data, and drafting and revising the manuscript. HV contributed to conception and design, acquisition of data, analysis and interpretation of data, and drafting and revising the manuscript. RW contributed to conception and design, acquisition of data, analysis and interpretation of data, and drafting and revising the manuscript. MMBF contributed to conception and design, acquisition of data, and drafting and revising the manuscript. RCD contributed to conception and design, acquisition of data, and drafting and revising the manuscript. IP contributed to conception and design, acquisition of data, and drafting and revising the manuscript. All authors read and approved the final manuscript.
Rights and permissions
This article is published under license to BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
About this article
Cite this article
Andreassen, H.K., Bujnowska-Fedak, M.M., Chronaki, C.E. et al. European citizens' use of E-health services: A study of seven countries. BMC Public Health 7, 53 (2007). https://doi.org/10.1186/1471-2458-7-53
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-7-53