
Abstract
Background
Pulmonary tuberculosis continues to increase due to late patient presentation. The study was conducted at a chest clinic of a general hospital in Lagos, Nigeria, to investigate patterns of delays before treatment amongst tuberculosis patients.
Methods
Longitudinal recruitment using a health worker administered protocol to determine time interval from onset of symptoms to initiation of treatment. Presentation to a health facility after 30 days of the onset of symptoms was classified as patient delay. Doctor delay was when patients stayed for more than 15 days with the referring doctor.
Results
One hundred and forty-one patients were recruited. The mean age was 29.5 ± 11.0 years, 89 (63%) were males and 52 (37%) were females. One hundred and sixteen (82%) had positive smears. One hundred and seventeen (83%) delayed their seeking help from health facilities longer than one month after the onset of symptoms. The median patient delay was eight weeks; median doctor delay was one week, median treatment delay was one week and the median total delay was 10 weeks. Doctor delay was observed in 19 (13%) patients. Patient delay was the most frequent type of delay observed and was the major contributor to the overall total delay. Patient delay was not significantly associated with patients' socio-demographic characteristics such as age, gender and educational level.
Conclusion
Majority of TB patients at this centre did not present early to health facilities and continue to serve as reservoirs of infection. Patient education on the disease may help reduce delays in starting treatment.
Similar content being viewed by others


Background
Tuberculosis (TB) is a problem of global importance. Among communicable diseases, TB is the second leading cause of death worldwide, killing nearly 2 million people each year [1]. In Nigeria, tuberculosis is common; a prevalence of 9.2% has been reported in one study [2] and a case fatality rate of 12% in a second [3].
Delay in the diagnosis of TB and commencement of treatment has been reported to be common in Nigeria and other countries [2, 4–10]. These delays are attributable both to patients and doctors. Delay in diagnosis may worsen the disease, increase the risk of death and enhance tuberculosis transmission in the community. In Tanzania, 15% of patients were found to report to a health facility within 30 days of the onset of symptoms [5]. A study from Nigeria [4] showed that 81% of patients delayed for more than one month before presentation at two chest clinics. The patients had visited local private medical facilities, traditional healers and had a low level of knowledge and awareness about the disease.
Furthermore, Nigeria is one of the few countries worldwide where TB control has been slow [11], partly due to patient delays and inefficiencies in the health system. Thus TB control is one of the major public health challenges facing Nigeria. If the control of tuberculosis must succeed, causes of delay by patients and doctors should be investigated and minimised. This study was conducted to determine the patterns of delay amongst tuberculosis patients seen at a tuberculosis clinic in Lagos, Nigeria.
Methods
Background
The study was conducted at the chest clinic of the General Hospital, Ikeja in Lagos, Nigeria. The hospital offers medical care to about 5 million people and was in the process of being upgraded to a teaching hospital at the time of the study. In Lagos State, tuberculosis is treated at no cost to the patient. The programme is run as recommended by the National Programme on tuberculosis control. A pulmonary TB may either be sputum positive or sputum negative for acid-fast bacilli. A sputum positive case is one who sputum shows acid-fast bacilli on at least two samples. Smear negative cases are diagnosed on clinical findings, Mantoux test and chest X-ray. Both sputum positive and negative cases were recruited into the study.
Study design
The study was conducted as a longitudinal recruitment of all new patients seen at the chest clinic. The study sought to investigate patterns of delay amongst TB patients. The Lagos State Hospital Management Board granted ethical approval for the study. The study was conducted between September 2000 and January 2001. All newly diagnosed cases of pulmonary tuberculosis were included in the study. The patients were interviewed at their first visit to the chest clinic. Informed consent was obtained verbally.
Survey instrument
The staff at the chest clinic administered an interview schedule to patients recruited into the study. Information obtained included patient's socio-demographic characteristics, the onset of symptoms, time interval between the onset of symptoms and the first visit to any source of medical treatment, date of diagnosis and when treatment was commenced. Patients were also asked about the method of referral to the chest clinic, and the results of investigations conducted.
Data analysis
All questionnaires were analysed in a computer using Epi-Info software v6.04c [12]. Standardised definitions of the different types of delays were followed [6]. The interval between the onset of symptoms and the first contact with a health facility was defined as patient delay while the interval from the time of visit to the first facility to the chest clinic was defined as doctor delay if no treatment for tuberculosis had been initiated. Treatment delay was the time interval from diagnosis until treatment was started while total delay was the time from the onset of symptoms until treatment was commenced and was made of these three components. Furthermore, presentation after 30 days of the onset of symptoms was classified as patient delay; doctor delay was when patients stayed for more than 15 days with the referring doctor [8]. Both descriptive and inferential statistics were determined. The level of significance was set at P < 0.05.
Results
Socio-demographic characteristics of patients
One hundred and forty-one patients were recruited into the study. The mean age was 29.5 ± 11.0 years. Eighty-nine (63%) patients were males and 52 (37%) were females. The mean age of females (27.6 ± 11.0 years) was comparable to that of the males (30.7 ± 10.9 years, p = 0.10). Ninety-nine (70%) had at least secondary school education. Thirty (21%) patients were unskilled workers including traders and housewives and 50 (36%) were skilled workers (Table 1).
Diagnosis of TB
Symptoms of tuberculosis experienced by patients include cough (128 patients, 91%), fever (117, 83%), weight loss (103, 73%), chest pain (85, 60%), night sweats (63, 44%) and haemoptysis (42, 30%). Twenty-one (15%) patients gave a history of exposure to someone who had chronic cough at home while 9 (6%) had such an exposure at the place of work. One hundred and thirty-one patients (93%) had a chest X-ray suggestive of tuberculosis and 116 (82%) had sputum positive smears. The association between those who had radiological evidence of the disease and positive sputum smears was slightly below the level of significance (p = 0.053). Seventy-three (52%) patients knew that TB was treated at no cost, 24 (17%) patients thought that fees were charged while 44 (31%) did not know.
Type of facility first visited
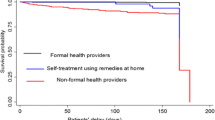
One hundred and four (74%) patients consulted with various types of hospitals as the first place for seeking help while 37 (26%) went to other places such as chemists and prayer houses (Table 2). More patients went to private hospitals than any other type of facility. Prior to presentation at the chest clinic, 19 (14%) patients did not go to any hospital at all while 98 (70%) visited one hospital and 24 (17%) visited between two to four hospitals. Ninety (64%) patients were referred to the chest clinic by doctors, 22 (16%) came by themselves and 29 (21%) were brought by friends and relatives.
Patterns of delays
Patterns of delays are shown on Table 3. The mean total delay was 14.3 ± 9.3 weeks. Patient delay was the most frequent type of delay observed and the greatest contributor to total delay. Patient delay was observed in 117 (83%) patients. The mean time to presentation was significantly longer in patients who delayed (14.0 ± 9.2 weeks) than in those who did not (3.7 ± 0.7 weeks, p < = 0.001). Twenty (17%) patients visited a health facility within 30 days of the onset of symptoms, 63 (45%) did so within 1–3 months, 38 (27%) between 4–6 months and 16 (6%) after 6 months.
Patient delay was not found to be significantly associated with age (p = 0.96) gender (p = 0.87), sputum result (p = 0.43), place of first consultation (p = 0.12), educational level (p = 0.07) or any of the symptoms of disease (p > 0.05). One hundred and twenty-two (87%) patients were referred to the chest clinic within a week of visiting a health facility by the attending doctor or health worker and only 19 (13%) had doctor delay. One hundred and twenty-seven (90%) were commenced on treatment within a week of being seen at the chest clinic. Total delay less than 4 weeks in only four (3%) patients; between one to three months in 69 (49%) patients and longer than 3 months in 68 (48%) patients.
Discussion
The symptoms of TB are initially similar to those of other diseases and it is not unusual for patients to consider that the problems would be simple to treat or resolve spontaneously. This may be partly responsible for 26% of patients in this study seeking help from non-medical facilities. However, the proportion (74%) of those who sought help from medical facilities is comparable to the 89% found in Malawi [13] but higher than the 58% reported from South Africa [14].
The patterns of delay observed in this study are similar to those seen in other studies [4–8, 13, 14]. The frequency of patient delay is lower than the 29% found in India [15]. With a median patient delay of eight weeks, the proportion of patients (83%) who delayed seeking treatment is similar to the 81% reported from Nigeria [4], though overall there are no differences in the patterns of patient delay. This present study confirms the findings of Enwuru et al [4]. The occurrence of doctor delay (13%) in this study is similar to the 10% observed in Ethiopia [8] while the median total delay of 10% is the same rate reported from South Africa [14]. Furthermore, the median duration of doctor delay was shorter amongst patients at the facility and not as frequently occurring as patient delay, unlike the situation in Ghana [6], Pakistan [16] and Turkey [17]. This may be because doctors in general practice in Lagos refer patients quickly to the chest clinic due to the high cost of treatment, which may not be affordable if the patients were to be managed in private hospitals.
Thus late patient presentation was a more important contributor to total delay in commencing treatment than doctor delay. The delay by patients is probably due to a low level of knowledge and awareness of the disease and lack of information about availability of free treatment. In Zambia, lack of money for treatment was a major contributory factor to patient delay [10]. Factors such as age of patient, educational level and residence of patient, which have been identified to be significant predictors of patient delay, could not be not established in this study [5, 6, 18]. This may be partly because of the cosmopolitan nature of Lagos as people can move from one part of the city to another within a short period.
With such a high number of sputum-positive cases, coupled with lack of information about treatment, the disease is likely to be continuously transmitted within the community, at work and at home making TB control more difficult. In addition, about two thirds of patients seen at the chest clinic were referred from a doctor, which provides a window of opportunity for collaboration in TB control between the private and public sector. This collaboration becomes important as one study from Lagos [19] showed that majority of private hospitals employed short treatment regimes outside the recommendations of the National Tuberculosis/leprosy Control Programme. The non-compliance has implications for continuing transmission in such patients and the development of drug resistance.
Therefore we recommend that health education about symptoms of tuberculosis and the importance of early medical treatment be vigorously mounted by all stakeholders in the health sector to reduce delays so that patients can present early for treatment.
Conclusion
Patients with tuberculosis do not present early to hospital while patient delay was more common than other types of diagnostic delays.
References
Frieden TR, Sterling TR, Munsiff SS, Watt CJ, Dye C: Tuberculosis. Lancet. 2003, 362: 887-899. 10.1016/S0140-6736(03)14333-4.
Salami AK, Oluboyo PO: Hospital prevalence of pulmonary tuberculosis and co-infection with human immunodeficiency virus in Ilorin; a review of nine years (1991–1999). West Afr J Med. 2002, 21: 24-27.
Salami AK, Oluboyo PO: Management outcome of pulmonary tuberculosis; a nine year review in Ilorin. West Afr J Med. 2003, 22: 114-119.
Enwuru CA, Idigbe EO, Ezeobi NV, Otegbeye AF: Care-seeking behavioural patterns, awareness and diagnostic processes in patients with smear- and culture-positive pulmonary tuberculosis in Lagos, Nigeria. Trans R Soc Trop Med Hyg. 2002, 96: 614-616.
Wandwalo ER, Morkve O: Delay in tuberculosis case finding and reatment in Mwanza, Tanzania. Int J Tuber Lung Dis. 2000, 4: 133-8.
Lawn SD, Afful B, Acheampong JW: Pulmonary tuberculosis: diagnostic delay in Ghanaian adults. Int J Tuber Lung Dis. 1998, 2: 635-40.
Lawn SD, Acheampong JW: Pulmonary tuberculosis in adults. Factors associated with mortality at a Ghanaian teaching hospital. West Afr Med J. 1999, 18: 270-4.
Demissie M, Lindtjom B, Berhane Y: Patient and health service delay in the diagnosis of pulmonary tuberculosis in Ethiopia. BMC Public Health. 2002, 2 (1): 23-10.1186/1471-2458-2-23.
Auer C, Sarol J, Tanner M, Weiss M: Health seeking and perceived causes of tuberculosis among patients in Manila, Philippines. Trop Med Int Health. 2000, 5: 648-656. 10.1046/j.1365-3156.2000.00615.x.
Needham DM, Godfrey-Faussett P, Foster SD: Barriers to tuberculosis control in urban Zambia: the economic impact and burden on patients prior to diagnosis. Int J Tuberc Lung Dis. 1998, 2: 811-817.
Netto EM, Dye C, Raviglione MC: Progress in global tuberculosis control 1995–1996, with emphasis on 22 high-incidence countries. Global monitoring and surveillance project. Int J Tuberc Lung Dis. 1999, 3: 310-320.
Dean AD, Dean JA, Burton JH, et al: EpiInfo, Version 6: A word processing, database and statistics program for epidemiology on microcomputers. Centres for Disease Control, Atlanta, Georgia, USA. 1994
Salaniponi FM, Harries AD, Banda HT, Kang'ombe C, Mphasa N, Mwale A, Upindi B, Nyirenda TE, Banerjee A, Boeree MJ: Care seeking behaviour and diagnostic processes in patients with smear-positive pulmonary tuberculosis in Malawi. Int J Tuberc Lung Dis. 2000, 4: 327-332.
Pronyk RM, Makhubele MB, Hargreaves JR, Tollman SM, Hausler HP: Assessing health seeking behaviour among tuberculosis patients in South Africa. Int J Tuberc lung Dis. 2001, 5 (7): 619-27.
Rajeswari R, Chandrasekaran V, Suhadev M, Sivasubramaniam S, Sudha G, Renu G: Factors associated with patient and health system delays in the diagnosis of tuberculosis in south India. Int J Tuberc Lung Dis. 2002, 6: 789-795.
Sadiq H, Muynck AD: Health care seeking behaviour of pulmonary tuberculosis patients visiting TB Center Rawalpindi. J Pak Med Assoc. 2001, 51: 10-16.
Guneylioglu D, Yilmaz A, Bilgin S, Bayram U, Akkaya E: Factors affecting delays in diagnosis and treatment of pulmonary tuberculosis in a tertiary care hospital in Istanbul, Turkey. Med Sci Monit. 2004, 10: CR62-67.
Lienhardt C, Rowley J, Manneh K, Lahai G, Needham D, Milligan P, McAdam KP: Factors affecting time delay to treatment in a tuberculosis control programme in a sub-Saharan African country: the experience of The Gambia. Int J Tuberc Lung Dis. 2001, 5: 233-239.
Alakpa GE, Edet EA: Management of pulmonary tuberculosis PTB: regimen employed in Lagos, Nigeria. West Afr J Med. 1999, 18: 119-123.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/4/18/prepub
Acknowledgements
We are grateful to all the health workers who administered the questionnaire as well as the patients who took part in the study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing Interests
None declared.
Authors' contributions
OOO conceived study, designed protocol, participated in data collection, performed data analysis, wrote manuscript. JBO participated in data collection and in writing the manuscript. All authors read and approved the final manuscript
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Odusanya, O.O., Babafemi, J.O. Patterns of delays amongst pulmonary tuberculosis patients in Lagos, Nigeria. BMC Public Health 4, 18 (2004). https://doi.org/10.1186/1471-2458-4-18
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-4-18