
Abstract
Background
There has been an ongoing debate whether the effects of socioeconomic factors on health are due to absolute poverty and material factors or to relative deprivation and psychosocial factors. In the present analyses, we examined the importance for health of material factors, which may have a direct effect on health, and of those that may affect health indirectly, through psychosocial mechanisms.
Methods
Random national samples of men and women in Hungary (n = 973) and Poland (n = 1141) were interviewed (response rates 58% and 59%, respectively). The subjects reported their self-rated health, socioeconomic circumstances, including ownership of different household items, and perceived control over life. Household items were categorised as "basic needs", "socially oriented", and "luxury". We examined the association between the ownership of different groups of items and self-rated health. Since the lists of household items were different in Hungary and Poland, we conducted parallel identical analyses of the Hungarian and Polish data.
Results
The overall prevalence of poor or very poor health was 13% in Poland and 25% in Hungary. Education, material deprivation and the number of household items were all associated with poor health in bivariate analyses. All three groups of household items were positively related to self-rated health in age-adjusted analyses. The relation of basic needs items to poor health disappeared after controlling for other socioeconomic variables (mainly material deprivation). The relation of socially oriented and luxury items to poor health, however, persisted in multivariate models. The results were similar in both datasets.
Conclusions
These data suggest that health is influenced by both material and psychosocial aspects of socioeconomic factors.
Similar content being viewed by others

Background
Socioeconomic differences in mortality and morbidity are well documented [1–3]. An unresolved issue in understanding the socioeconomic gradient in health is what are the causes of the gradient. A key question is whether the gradient is driven by relative or absolute deprivation [4–8]. One interpretation of the association is that health inequalities result from the direct effects of material conditions [5]. The psychosocial interpretation proposes that relative deprivation (relative to persons higher in the social hierarchy) generates psychosocial processes independent from direct effects of material conditions, and that psychosocial mechanisms account for the link between social status and health [8–11]. Resolving this issue is difficult because material and psychosocial factors are usually strongly correlated. Persons with higher socioeconomic status usually have better housing and better nutrition but they also have less "stressful" psychosocial characteristics.
One way to examine this question is to divide material factors into those that can have a direct effect on health (e.g. via exposure to low temperature, damp housing, infections, chemical contamination or physical factors), and those that cannot affect health directly. For example, it is unlikely that ownership of satellite television has a direct protective effect on health; rather it is a marker of a higher status and higher standing in the social hierarchy. Its effect is more likely to be mediated by psychosocial processes [8]. Life style factors, which undoubtedly account for some of the social gradient in poor health, are also more likely to be associated with psychosocial well-being than with adverse material conditions.
In this report, we used data from national population samples from Hungary and Poland. Self-rated health was used as outcome for two reasons. First, data on self-rated health are easy to collect and we had opportunity to use this outcome in both data sets. Second, it is well documented that self-rated health predicts mortality (all cause mortality or specific cause mortality) in prospective studies [12]. We studied the effects on health of three groups of household items: the "basic needs" items, which may affect physical conditions and functioning (e.g. freezer, washing machine etc.), those that affect social interaction, and items that can be characterised as luxury (markers of high status). If the materialist hypothesis is true, the basic items are powerful predictors of health but the luxurious ones are not. On the other hand, an independent effect of the luxurious items, after controlling for potential confounding variables, would support the psychosocial hypothesis. We also examined the role of perceived control as potential mediator between luxury items and health.
Methods
Population and samples
The data come from cross-sectional surveys in Poland and Hungary in 1998; the surveys were a part of the New Democracies Barometer (NDB, http://www.cspp.strath.ac.uk/index.html), a series of surveys about social and political attitudes in post-communist countries. In both countries, random samples of adult population (aged 18 years and over) were selected in a multi-stage sampling procedure. The dataset consists of 973 face-to-face interviews in Hungary (response rate 58%) and of 1141 interviews in Poland (response rate 59%).
Self-reported health
Self-rated health was assessed by the question "How would you rate your health in the last 12 months?", with five possible answers: "very good", "good", "average", "bad", "very bad". For the present analysis, these responses were dichotomized into two categories, with individuals reporting "bad" or "very bad" health classified as "poor health".
Socioeconomic and psychosocial measures
Marital status was categorized into 2 groups: married and unmarried. Subjects were classified into four categories of achieved education: primary or less, vocational, secondary and university degree. Material deprivation was assessed by three questions about how often subject's household had difficulties buying enough food or clothes and paying housing, heating and electricity bills. The possible answers were "never or almost never", "sometimes", "often"and "always". The responses were coded as 0,1,2,3, and a deprivation score was calculated as the sum.
Data about ownership of household items were available and used in the analysis. The items asked differed in the two countries (21 items in Hungary, 7 items in Poland); the items are listed at the footnote of table 1. An index of household items ownership was constructed by summing up items owned by household. For this analysis, the index was grouped into 5 categories (0–4, 5–7, 8–10, 11–13, 14+ items) in Hungary and into three categories (0–2, 3–4, 5–7 items) in Poland. To evaluate the role of absolute or relative deprivation, we classified household items into three categories: "basic needs", "socially oriented needs", and "luxury". In Hungary, basic needs items included washing machine, fridge, freezer, microwave and phone; socially oriented needs items included colour TV, radio, hi-fi, record player, motorcycle, car and car radio; luxury items included cable TV, satellite, video recorder, video camera, CD, PC, dishwasher, dacha (small or large property in the countryside) and garden. In Poland, washing machine and phone were classified as basic needs, colour TV and car as socially oriented needs, and cable TV, satellite and videorecorder as luxury items.
Scores of perceived control over own health and over own life were constructed from 3 and 6 questions, respectively, adapted from the Whitehall II Study and MacArthur Study on Successful Midlife; the actual items were explicitly described previously elsewhere [13, 14].
Statistical analysis
Since the lists of household items recorded in Hungary and Poland were different, we conducted separate analyses for each country. The associations between self-rated health (poor vs. not poor) and different categories of household items were estimated by logistic regression in several steps. First, the odds ratios were adjusted for age and gender. In a second step, odds ratios were further adjusted for several potential confounders: education, material deprivation and marital status. Finally, perceived control was entered into the model to assess whether it could partly mediate the association between household items ownership and health. All analyses were performed in the STATA statistical package (Stata Corporation, College Station, USA).
Results
Table 1 describes the two samples. There was large difference in the prevalence of poor health (13% in Poland compared to 25% in Hungary). Subjects in Poland were slightly younger than in Hungary (49% of subjects younger than 40 years compared to 36%) but distribution of other variables was similar in the two samples.
Table 2 shows correlations between socioeconomic characteristics and perceived control over health and life. Categories of household items are significantly associated with education and deprivation although correlations between these variables are not extremely high.
In both countries, the overall number of owned household items was strongly related to poor self-rated health; and the relationship persisted after adjustment for sex, age, marital status, education and deprivation, and it was only partly reduced by further adjustment for perceived control over life and health (not shown in table).
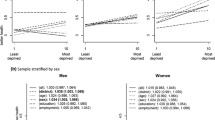
Table 3 shows odds ratios and 95% confidence intervals of poor self-rated health by three categories of items ("basic needs", "socially oriented needs", "luxury") at three levels of adjustment: (1) for age and sex, (2) for age, sex, education, marital status and deprivation, and (3) as previously plus perceived control. In each country, the top three panels present results from the analysis when each of these three variables was included in the analysis separately. The bottom panel shows results from the analysis when three measures of need were mutually adjusted for each other.
In Hungary, there was a significant effect of basic needs items after controlling for age and sex but this effect was explained by adjustment for other socioeconomic variables. The effects of socially oriented needs items and of luxury items were evident at all levels of adjustment. After adjusting for other socioeconomic variables and marital status, the odds ratios between the worst and the best categories were 0.55 for social needs and 0.30 for luxury items (table 3, "Hungary", adjusted 2). Additional adjustment for perceived control led to only a small attenuation of the effect estimates. In Poland, the results showed a similar pattern but the ORs were not statistically significant, perhaps due to smaller number of items measured. Despite the absence of statistical significance, the effect of basic items appeared to be explained by either education and deprivation or the other two categories of household items, and perceived control did not seem to account for the effects of luxury items and socially oriented items.
Discussion
In this study, we examined the effects of absolute and relative deprivation, represented by different categories of household items owned by study subjects. These three categories correspond to material and social aspects of the household items construct. Hence the present study may contribute to the debate on this topic.
This cross-sectional study has several limitations. First, the possibility that people may be poor because they are ill (reverse causation) cannot be ruled out in cross-sectional study. However, previous research, particularly studies using long-term follow up, has shown that this is probably not an important phenomenon [15, 16]. Second, self-rated health is a subjective measure. Although it has been shown to predict mortality in prospective studies [12], in cross-sectional surveys it can be influenced by other factors, such as dissatisfaction with own life circumstances or life chances. We took advantage of having measured the perceived control over own life and health to address this concern, since this variable would capture some of these negative perceptions. There is little evidence that the results were influenced by negative attitudes. The statistical models did not change substantially after controlling for perceived control – this suggests that this bias did not play an important role in this study. Moreover, one would expect that this would affect similarly both groups of factors – material and psychosocial.
An additional limitation was that we did not have the same household items available in both samples, and we therefore analysed both data sets using available items. However, this shortcoming may be an advantage, because it allowed us to assess whether the observed relationships were specific to one population or whether there is, potentially, a general pattern. The similarity of results in the two countries suggests that there is such a pattern. We are aware that the categorisation of household items was somewhat arbitrary, although it was done a priori, on the basis of hypothesised social participation and relative position. Some of the items, particularly a video recorder and telephone, could be classified to different categories (a video recorder could be in the socially oriented or luxury item group, or telephone could be among the basic or socially oriented needs). When we examined such possible changes in definition of three categories of household items, the results were robust – they did not change materially when one or two of the above mentioned items have been assigned to different category, but the results were sensitive to more substantial movements across categories of items.
Material conditions are certainly an important aspect of socioeconomic status. In this study, they were represented by the material deprivation score and the "basic needs" items. We did not use income, since it is widely believed that people in Central and Eastern Europe would not correctly report their income, and most researchers worry that such questions could decrease the response rates. In addition, in these societies the income (both monetary and non-monetary) from unofficial sources accounts for a substantial proportion of total income. We have therefore asked about difficulties to buy basic necessities, and we calculated the material deprivation score. There has been little research on this construct, but it predicted health well in our previous studies of self-rated health [14, 17]. Hraba et al [18] used a concept of "economic stress" similar to our definition of material deprivation, and like us, they found a significant association between economic hardship and poor self-rated health.
Both the basic item ownership and the deprivation score were strongly associated with poor health in age- and sex-adjusted models, and deprivation score remained a strong predictor in adjusted models. This is consistent with the view that material factors are important determinants of health. The fact that the effect of basic item ownership was eliminated by adjustment for deprivation score confirms that they both measured the same underlying construct – material conditions.
In the Hungarian data, socially oriented and luxury items remained strongly associated with self-rated health even in fully adjusted models. This indicates that their effect does not depend on material deprivation, and it also suggests that the social aspects of household items ownership may be as important as the material ones. Perceived control did not seem to mediate the effect of luxury items on health, contrary to some reports that control may provide the link between socioeconomic status and health [19][20]. The pattern of the results was similar in Polish data but the effects were not statistically significant – we attribute this to the smaller number of items measured and thus a less precise classification of subjects in Poland than in Hungary.
One may speculate, for example, that people compare what they have with what their neighbours, friends or relatives have. Such comparison of "wealth" (in terms of things that are not really important for everyday life) may then be reflected in feelings about their position on the social ladder. This is consistent with the psychosocial factors hypothesis. Apart from the control variables, we did not have the data to assess the mechanism by which these factors influence health. They can include life styles but also biological parameters that are related to psychosocial stress. Nevertheless, the results of this study indicate that – not surprisingly – health in these populations is influenced by both groups of factors: those that affect the material aspects of people's lives, and those that influenced their psychosocial well-being.
References
Phillimore P, Beattie A, Townsend P: Widening inequality of health in northern England, 1981–91. BMJ. 1994, 308: 1125-1128.
Marmot MG, Shipley MJ: Do socioeconomic differences in mortality persist after retirement? 25 year follow up of civil servants from the first Whitehall study. BMJ. 1996, 313: 1177-1180.
Davey Smith G, Bartley M, Blane D: The Black report on socioeconomic inequalities in health 10 years on. BMJ. 1990, 301: 373-377.
Wilkinson RG: Health inequalities: relative or absolute material standards. BMJ. 1997, 314: 591-595.
Lynch JW, Davey Smith G, Kaplan GA, House JS: Income inequality and mortality: importance to health of individual income, psychosocial environment, or material conditions. BMJ. 2000, 320: 1200-1204. 10.1136/bmj.320.7243.1200.
Lynch JW, Due P, Muntaner C, Davey Smith G: Social capital – Is it a good investment strategy for public health?. J Epidemiol Community Health. 2000, 54: 404-408. 10.1136/jech.54.6.404.
Wilkinson RG: Inequality and the social environment: a reply to Lynch et al. J Epidemiol Community Health. 2000, 54: 411-413. 10.1136/jech.54.6.411.
Marmot M, Wilkinson RG: Income and health: material and psychosocial pathways. A reply to Lynch et al. BMJ. 2001, 322: 1233-1236. 10.1136/bmj.322.7296.1233.
Bosma H, Marmot MG, Hemingway H, et al: Low job control and risk of coronary heart disease in the Whitehall II (prospective cohort) study. BMJ. 1997, 314: 558-565.
Marmot M, Bosma H, Hemingway H, et al: Contribution of job control and other risk factors to social variations in coronary heart disease incidence. Lancet. 1997, 350: 235-239. 10.1016/S0140-6736(97)04244-X.
Hemingway H, Marmot M: Psychosocial factors in the aetiology and prognosis of coronary heart disease: systematic review of prospective cohort studies. BMJ. 1999, 318: 1460-1467.
Idler EL, Benyamini Y: Self-rated health and mortality: a review of twenty-seven community studies. J Health Soc Behav. 1997, 38: 21-37.
Pikhart H: Social and psychosocial determinants of self-rated health in seven countries of Central and Eastern Europe. 2002, Norwell: Kluwer Academic Publishers
Bobak M, Pikhart H, Rose R, Hertzman C, Marmot M: Socioeconomic factors, material inequalities, and perceived control in self-rated health: cross-sectional data from seven post-communist countries. Soc Sci Med. 2000, 51 (9): 1343-50. 10.1016/S0277-9536(00)00096-4.
Benzeval M, Judge K: Income and health: The time dimension. Social Science and Medicine. 2001, 52: 1371-1390. 10.1016/S0277-9536(00)00244-6.
Lynch JW, Kaplan GA, Shema SJ: Cumulative impact of sustained economic hardship on physical, cognitive, psychological, and social functioning. N Engl J Med. 1997, 337: 1889-1895. 10.1056/NEJM199712253372606.
Bobak M, Pikhart H, Hertzman C, Marmot M: Socioeconomic factors, perceived control and self reported health in Russia. A cross-sectional survey. Soc Sci Med. 1998, 47 (2): 269-279. 10.1016/S0277-9536(98)00095-1.
Hraba J, Lorenz FO, Pechacova Z, et al: Education and health in the Czech Republic. J Health Soc Behav. 1998, 39: 295-316.
Syme SL: Control and health: a personal perspective. In: Stress, personal control and health. Edited by: Steptoe A, Appels A. 1989, Brussels-Luxembourg: John Wiley & Sons Ltd, 3-18.
Bosma H, Schrijvers C, Mackenbach JP: Socio-economic inequalities in mortality; importance of perceived control. BMJ. 1999, 319: 1469-1470.
Pre-publication history
The pre-publication history for this paper can be accessed here:http://www.biomedcentral.com/1471-2458/3/38/prepub
Acknowledgements
The NDB surveys were funded by grants from Paul Lazarsfeld's Society, Vienna, the European Commission, and by the Centre for the Study of Public Policy, Glasgow. The data analyses were supported by a grant from the MacArthur Foundation and by the project LN00B107 of Ministry of Education of the Czech Republic. MM is a recipient of Medical Research Council Research Professorship. The authors would like to thank the ESF scientific programme Social Variations in Health Expectancy in Europe for support and useful discussions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Competing interests
None declared.
Authors' contributions
HP and MB participated in all phases of preparation of the manuscript. MM was involved in study design, questionnaire development and he commented on all drafts of the manuscript. RR was involved in study design, preparation of questionnaire and he commented on earlier drafts of the paper.
Rights and permissions
This article is published under an open access license. Please check the 'Copyright Information' section either on this page or in the PDF for details of this license and what re-use is permitted. If your intended use exceeds what is permitted by the license or if you are unable to locate the licence and re-use information, please contact the Rights and Permissions team.
About this article
Cite this article
Pikhart, H., Bobak, M., Rose, R. et al. Household item ownership and self-rated health: material and psychosocial explanations. BMC Public Health 3, 38 (2003). https://doi.org/10.1186/1471-2458-3-38
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/1471-2458-3-38